
Abstract
The article is devoted to the current state of continuing medical education for general practitioners in the city of Moscow and is based on a survey of general practitioners working in Moscow. Results demonstrate a lack of satisfaction with the organisation and content of training in its previous format, the absence of significant changes in the learning objectives following education reform and an ambiguous attitude towards this reform. The minimum continuing education requirements for general practitioners working in the city of Moscow were shown to consist of day release, short-term training, theoretical and practical orientation and the application of contemporary educational technologies. Conceptual approaches to the development of continuing medical education in the field of general medical practice in Moscow were formulated. These comprised organisation of training, setting of learning objectives, selection of forms and methods of training, determination of interactive training content, application of a competency-based approach and individualisation of the educational path.
Keywords
Introduction
The need for the continuing education of doctors is determined by the dynamic development environment and fast pace of medical science, as well as by challenges facing contemporary healthcare in the fields of diagnosis, treatment, prevention and rehabilitation of diseases. The constant increase in and updating of the vast array of relevant information informs the professional need for a systematic increase in the level of theoretical knowledge along with the improvement and expansion of practical skills regardless of age and length of service.
Historically, the first stage in the emergence of continuing medical education (CME) in Russia can be considered as having coincided with the advanced surgical training programme instituted at the St. Petersburg Military Medical Academy in 1851. Later, in 1858, a faculty was created there for improving physician skills in the fields of surgery, therapy and hygiene (Khabriev, 2014). In 1885, under the patronage of Princess Elena Pavlovna, the first Imperial Clinical Institute was established for improving the competency of doctors, renamed as the Leningrad State Institute for the Advanced Training of Physicians in 1924 (Eichwald, 1885). At the beginning of the 20th century, educational institutions for the advanced training of doctors began to open in Moscow, Kazan and other Russian cities (Mikhailov, 2005).
The term ‘continuing education’ was officially introduced into use in 1992 by the law of the Russian Federation of 10/07/1992 No. 3266–1 ‘On Education’.1 However, prior to 2016, the continuing professional education (CPE) model for doctors was only continuous in a limited sense. In essence, it referred to the opportunity to undergo training once every 5 years in order to renew a specialist certificate or training as needed within the framework of advanced thematic training cycles.2
The main characteristic of the ongoing transition to a system of CME since 2016 consists in an accumulative system of advanced training, applying to all types of educational activities and aimed at ensuring the optimal convenience of participating medical workers (Chesnokova, 2019).
In 2017, the present concept of CME development was approved until 2021;3 this has the aim of ensuring the training of highly qualified healthcare professionals, improving the CPE system for medical and pharmaceutical workers and integrating innovative educational technologies in medical and pharmaceutical education in order to ensure the quality of medical care and its accessibility to the population.
In Russian and global practice, the relevance of CME as not only as a practical but also a scientific problem is evidenced by the dynamic growth of publication activity on relevant topics in the RSCI, CyberLeninka, PubMed and Scopus databases (Prirodova & Morgun, 2018).
The main criterion for the effectiveness of CME training consists in the quality and accessibility of medical care. However, in order to provide motivation for CME participation, it is important to monitor the satisfaction of medical practitioners with the emerging system. Expectations, needs and problems associated with training may differ depending on the specialty, as well as on the place of residence and work. Thus, the relevance of developing and optimising CME for general practitioners (GPs) is based on the need to deliver improvements in primary healthcare, defined as one of the current priority areas of the Healthcare Development Strategy in the Russian Federation for the period until 2025.4
The purpose of the present study was to study the basic CME needs of GPs working in the city of Moscow and develop conceptual approaches to its improvement and development based on the obtained results and data from the scientific literature. In order to achieve this goal, the following tasks were specified: investigate the periodicity of GP training at the postgraduate stage in the city of Moscow; carry out a comparative analysis of the main GP training aims in the city of Moscow prior to and following the implementation of the CME system; conduct a comparative assessment of the satisfaction of GPs in the city of Moscow with the organisation and content of the educational process prior to and following the implementation of the CME system; investigate the attitude of Moscow GPs to the implementation of the CME system and the extent to which the results of implementing the CME system met their expectations; assess the opinion of Moscow GPs regarding existing problems and possible approaches to improving the CME programme; summarise the obtained results along with the scientific literature data and formulate proposals for improving the CME system for the CME of GPs in the city of Moscow.
Materials and methods
During the study, sociological, analytical and statistical research methods were applied. A review of domestic and foreign literature on the medical postgraduate education covering a period of 5 years presented in the PubMed and ELibrary databases was carried out alongside an assessment of the relevant legal documents governing additional professional education in the Russian Federation.
A one-time sociological survey of GPs in the city of Moscow was carried out in order to study the frequency of respondents’ answers to questions regarding: the periodicity of training at the postgraduate stage; learning objectives, satisfaction with the organisation and content of postgraduate learning both before and after the introduction of the CME system; to what extent expectations were fulfilled following the introduction of the CME system; principal problems of the existing system of CME and approaches to its improvement and development. The study was carried out using a sampling approach. In order to obtain a representative sample to allow the obtained results to be extrapolated to cover the entire population of GPs in the city of Moscow, we used the methodology proposed for sociological surveys by (Paniotto, 1982). According to this methodology, the sample size should comprise at least 350 units for populations of less than 3000. According to the data of the FSBI Federal Research Institute of Health Organisation and Informatics of the Russian Ministry of Health,5 the total number of GPs in the city of Moscow comprises 2940 individuals. Thus, in order to conform to the stated criterion, it was necessary for at least 350 respondents to take part in the survey.
The questionnaire for conducting a sociological survey was developed by the staff of the Department of General Medical Practice of the Sechenov University Institute of Professional Education to take into account the goals and objectives of the present study. The approbation of the questionnaire was carried out on a pilot group of 17 GPs who were undergoing training at the faculty. In response to the approbation, minor editorial changes were made to the questionnaire.
As well as recording the general characteristics of the respondent, including information about gender, age and general work experience, the questionnaire comprised nine questions. The first, relating to the frequency of training prior to the introduction of the CME system, was presented in multiple-choice form with five possible response options. The second question, which focused on the main goals of training prior to the introduction of the CME system, comprised a selection of nine multiple-choice answers and one detailed response. The third question involved an assessment on a five-point scale of the respondent’s satisfaction with 12 parameters characterising the organisation and content of the educational process, where 5 points were assigned to complete satisfaction: 4 – when the survey participant was more satisfied than not; 3 – in case of difficulty in providing a specific answer; 2 – when the survey participant was rather dissatisfied; 1 point – in the case of unequivocal dissatisfaction. The fourth question in multiple-choice format included five answer options regarding the respondent’s attitude towards the implementation of the CME system. The fifth and sixth questions were identical to the second and third, respectively, but focused on the time period following the introduction of the CME system. The seventh question (multiple-choice) provided information as to the extent to which the transition to the CME system had met the respondents’ expectations (four response options). The eighth question, in which the respondent selected options from the eight proposed answers and/or provided a detailed answer, highlighted the main current problems affecting the CME system. In the ninth question, the respondents were invited to make proposals for the improvement and development of the CME system by choosing ready-made answers and/or formulating their own.
The study participants were selected at random. The questionnaire was sent by e-mail to the managers of general medical practices of the administrative districts of the city of Moscow. In the cover letter, a proposal was formulated to invite these managers to participate in the sociological study by organising a survey of GPs working in public medical organisations of the corresponding administrative district. As a result, a total of 383 GPs were sent an invitation to respond to the questionnaire. Of these, 357 completed questionnaires were sent to the e-mail address of the department, representing a response rate of 93.2%. The analysis was carried out on 357 questionnaires of GPs working in the city of Moscow, which is sufficient to consider the obtained results as representative.
During the statistical processing of the data, the proportion of men and women among the respondents was calculated, along with the average age, work experience and proportion of GPs having a primary specialisation. The response rates of survey participants were analysed in relation to: the frequency of training at the postgraduate stage; learning objectives before and after the introduction of the CME system; the degree of satisfaction with various parameters of the organisation and content of training before and after the introduction of the CME system; attitudes and expectations regarding the implementation of the CME system and existing problems and possible approaches for improving the CME system.
A comparison was made of the respondents’ response rates regarding learning objectives, as well as characterising their satisfaction with various parameters of the organisation and content of the educational process at different stages of postgraduate education development both before and after the introduction of the CME system. For comparison of these relative values, the Student t-test was applied. The differences were considered to be statistically significant (p <0.05).
Results
Among the 357 respondents, men and women comprised 22.4% and 77.6%, respectively. The average age of the survey participants was 47.8 ± 1.0 years, and the average length of practice was to 20.3 ± 0.9 years. Most of the survey participants had passed primary specialisation in therapy (61.5%) or general practice (16.5%).
Prior to the introduction of the CME system, most doctors (49.0 ± 4.1%) underwent training once every 5 years; 21.1 ± 3.4% were trained as needed; 19.9 ± 3.3% had participated in more than 1 training in 5 years; only 6.8 ± 2.1% had trained continuously, while 3.4 ± 1.5% had not received any training in a 5-year period.
The main goals of GP training before and after the introduction of the CME system are presented in Table 1. As can be seen, following the introduction of the CME system, these goals did not significantly change; the following options were the most cited by the respondents (in descending order of the frequency of responses):
Learning objectives for GPs before and after CME implementation.
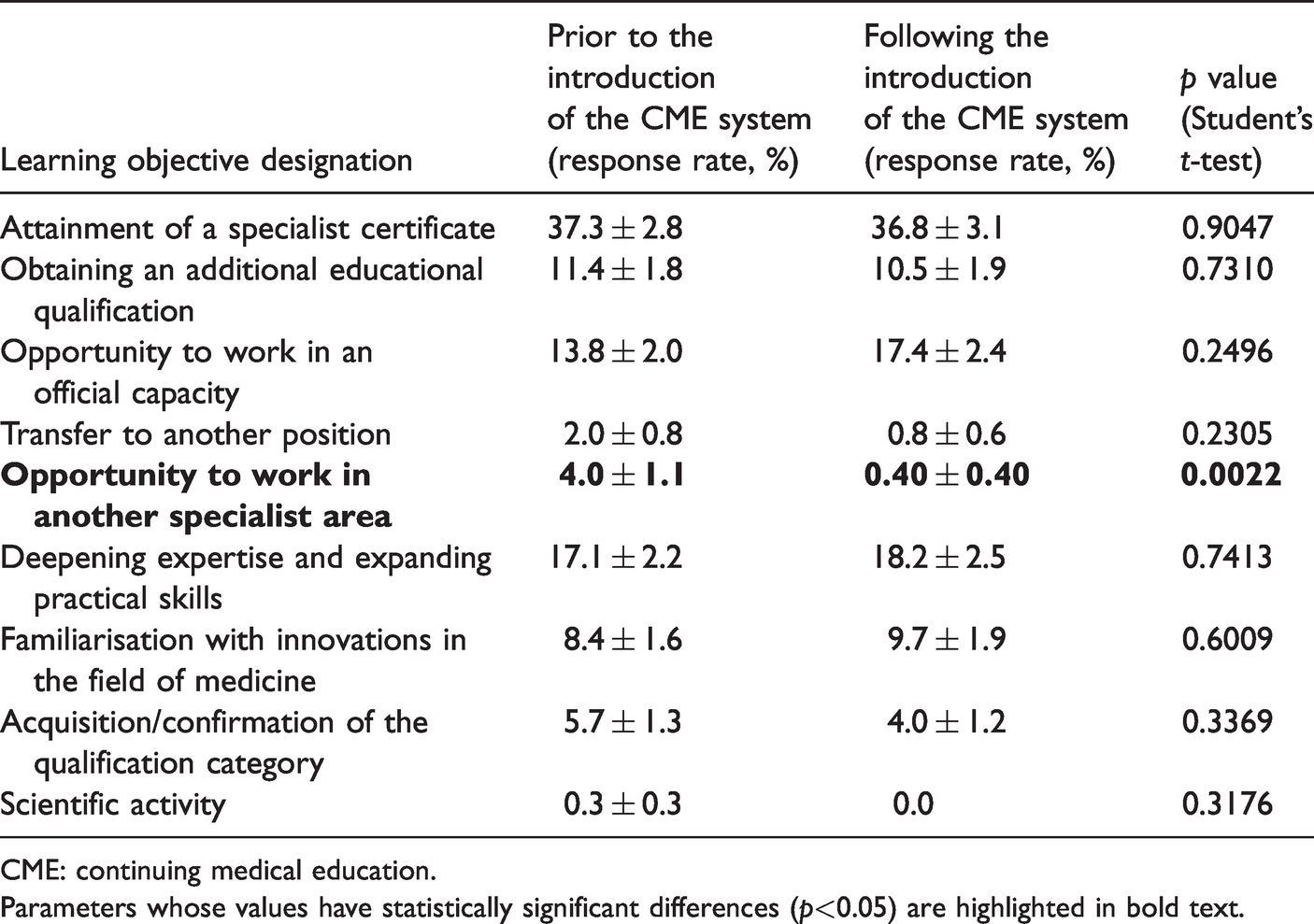
CME: continuing medical education.Parameters whose values have statistically significant differences (p<0.05) are highlighted in bold text.
attainment of a specialist certificate;
deepening expertise and expanding practical skills;
the opportunity to work in an official capacity;
obtaining an additional educational qualification;
familiarisation with innovations in the field of medicine.
Only in relation to the training goal ‘ability to work in another specialty’ were statistically significant differences recorded (the frequency of training for this purpose decreased following the introduction of the CME system). In relation to the training goal ‘scientific activity’, following the introduction of the CME system, no GP who took part in the survey had not received this training.
Table 2 shows the frequency of ‘completely satisfied’ responses in relation to various parameters characterising the organisation and content of the educational process prior to and following the introduction of the CME system. Before the introduction of the CME system, most of the respondents were completely satisfied only with the availability of training, while, with respect to other parameters, complete satisfaction was noted in less than 50% of cases. Following the introduction of the CME system, the frequency of complete satisfaction failed to reach 50% in any of the parameters. In the following parameters, it had a statistically significant negative trend: availability of training and teaching methods, scope of the theoretical part, form of training, schedule of classes and amenity of the training location. For the remaining parameters, the overall dynamics were also negative but did not achieve statistical significance.
Complete satisfaction of GPs with the organisation and content of the educational process prior to and following the introduction of the CME system.
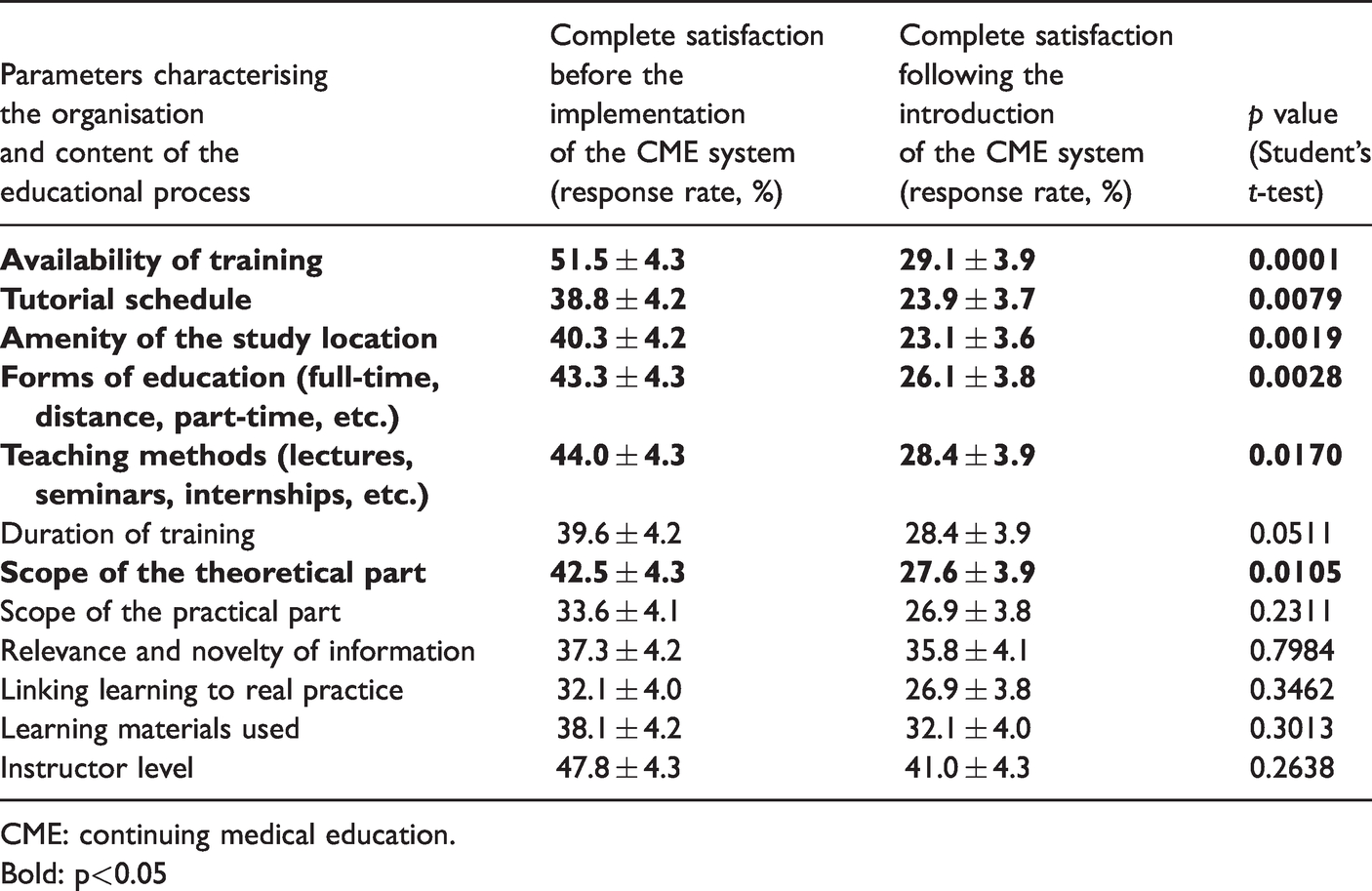
CME: continuing medical education.Bold: p<0.05
The majority of respondents (27.6%) reacted more negatively to the implementation of the CME system, while 23.1% were more positive; 20.9% gave an unambiguously positive assessment or had difficulty in answering; 7.5% expressed an unambiguously negative opinion.
Further, 35.7% of respondents reported that the transition to the CME system did not meet their expectations; for 28.7%, expectations were partially met, while for 20.9%, they were fully met. Also, 14.7% of respondents stated that they did not expect any improvement.
In terms of the main problems associated with participation in CME, the survey participants cited the following (in decreasing order of importance): difficulty of combining work and study (29.8 ± 2.5%); geographical remoteness of the place of study (14.9 ± 1.9%); lack of time to prepare for the exam (14.6 ± 1.9%); tightness of class schedule (13.1 ± 1.8%); increase in the volume of independent work (10.4 ± 1.7%); an increase in personal responsibility (8.9 ± 1.6%); insufficient computer literacy and/or lack of access to a computer/the internet (3.0 ± 0.9%); inconvenient navigation through the CME portal (0.3 ± 0.3%).
For further improvement and development of the CME system in the city of Moscow, the respondents proposed the following approaches (in decreasing order of importance): wider use of training on the premises of a medical organisation/place of work (23.8 ± 2.7%); an increase in the volume of practical training and time for practicing practical skills (20.9 ± 2.6%); full transition to short-term thematic educational courses (14.3 ± 2.2%); broader coverage of the results of research and innovation (13.1 ± 2.2%); wider introduction of digital technologies into the educational process (virtual teaching, video lectures, etc.) (12.3 ± 2.1%); increase in the proportion of distance learning (8.6 ± 1.8%); organisation of on-the-job training (1.2 ± 0.7%); cancellation of the points accumulation system (0.4 ± 0.4%); improvement of the CME portal (0.4 ± 0.4%).
Less than 0.5% of the survey participants suggested a return to the previous practice of postgraduate training.
Discussion
The conducted questionnaire survey of the GPs in the city of Moscow confirmed the formal nature of continuous professional development prior to the introduction of the CME system, which generally consisted of training provided once every five years according to certification cycles. A number of factors testify to the necessity – and even possibly some belatedness – in the reform that took place in the medical education system. First, the results of the questionnaire reveal low levels of satisfaction on the part of doctors with the organisation and the content of training in its previous format, consistent with similar results obtained in a previous study (Pogorelova, 2014), as well as in a survey initiated by the Ministry of Health of the Russian Federation.6 Second, the urgency of the domestic healthcare problem in terms of accessibility and quality can be noted, especially on an outpatient basis. Third, the continuous nature of advanced medical training provided abroad, which is already validated by legal norms and professional medical communities, also emphasises the weakness of the CME system in Russia (Peck, 2000).
At the same time, as evidenced by the heterogeneity of the survey data, the attitude of Moscow GPs towards the introduction of CME is ambiguous. The lack of consensus on this issue is not a specific feature of the doctor population included in the study but is rather characteristic of the Russian medical community as a whole. In other surveys, the preponderance of a positive attitude of doctors to CME varied across a wide range – from 90% (Sokolovskiy et al., 2018) to 34% (Zernova et al., 2018) – while a negative attitude to CME was expressed in up to 42% of cases (Aksenova & Zudin, 2019). There may be several reasons for this. On one hand, one may refer to the conservatism inherent to the medical profession and the insufficient amount of time having elapsed since the introduction of CME and formation of a continuous learning culture. On the other hand, there are specific factors affecting the motivation of Russian medical practitioners to continue with education throughout their working lives. Although for other sectors of professional activity, this implies, first of all, the opportunity to maintain their position, professional development and career growth (which in itself encourages continuous participation in the training process), for doctors, the situation is somewhat different. For medical professionals, while personal responsibility for the welfare of patients, professional self-awareness and the attitude of colleagues come to the fore, as well as the need to conform to formal current legislative requirements connected with their qualification (Moshetova et al., 2019), their connection with the need for continuing education does not appear as immediately obvious. Therefore, a parallel process of evolution should also be expected to occur in the attitudes of doctors to continuous learning.
The above-listed factors can also serve as an explanation for the absence of significant changes in the learning objectives of GPs in the city of Moscow following the introduction of CME. In contrast, in foreign countries, where CME is already characterised as a fairly well-functioning system, the main objectives of GP training include obtaining new information, finding answers to professional questions, putting existing knowledge into practice, solving urgent problems of clinical practice, generalising knowledge, conducting critical assessment of one’s own clinical practice, mastering new practical skills and forming professional relations (VanNieuwenborg et al., 2016).
Thus, the recorded decrease in satisfaction of Moscow GPs with the organisation and content of training following the introduction of CME, as well as the significant proportion of doctors with unfulfilled expectations regarding the reform, should not be misinterpreted. Given the significance of the changes that took place, the results appear to be more characteristic of a reaction to leaving the comfort zone of a formerly well-known education system, rather than a clear signal of a decrease in the quality and effectiveness of education.
However, neither can the results be ignored: the approach to this issue should therefore be constructed both from a subjective point of view and according to underlying objective criteria. On one hand, as was already noted above, this subjective point of view involves innate conservatism, a lack of willingness – and, in some cases, downright reluctance – to switch to a new model of learning and be forced to assimilate its new forms and methods. In support of this point of view, it may be noted that the highest levels of dissatisfaction were recorded among doctors having a length of service of five years or more. At the same time, it is fair to say that less than 0.5% of the survey participants supported a return to the previous training format. Nevertheless, the problems observed for the incipient CME system need to be addressed.
The main barriers to the participation of Moscow doctors in CME can be associated with the time factor and self-organisation. Comparing these results with literature data, they can be construed to comprise key barriers to the continuous training of medical workers not only in Moscow but also in Russia as a whole and abroad (Sokolovskiy et al., 2018; VanNieuwenborg et al., 2016). However, the use of information technology, the internet and navigation through the CME portal caused no significant difficulties for the capital's doctors.
The solution for current CME problems leading to its improvement is seen by Moscow GPs, first of all, in the development of intra-organisational learning, the improvement of scientific and practice-oriented educational processes, the transition to short-term thematic educational courses and the development of distance learning.
Thus, in order for the goals of training GPs in the city of Moscow in the CME system to change to become consistent with leading world practices, increasing the loyalty and motivation of GPs to the process of lifelong learning, as well as their satisfaction with its organisation and content, the following approaches for the improvement and development of the CME system for GPs working in the city of Moscow can be proposed.
According to the results of the study, the following recommendations can be formulated: CME should be carried out in the form of short-term thematic educational programmes structured on a modular basis. Among the organisational forms of training, the following should be primarily used: intra-organisational training; distance learning and e-learning. The choice of topics and the content of educational programmes should be based on the analysis of current practical problems and scientific development in the field of general medical practice. The educational process should be organised in such a way that the majority of time is devoted to the mastery and implementation of practical skills. The theoretical part should highlight current achievements and innovative developments in the field of medicine, as well as the results of clinical trials and clinical recommendations applicable to general medical practice.
On the basis of Russian (Aksenova & Zudin, 2019; Chesnokova, 2018; Churganov, 2018; Denisova & Kurilova, 2019; Fanta et al., 2019; Karas' et al., 2018; Kopylova & Galin, 2018; Popov et al., 2019; Vladimirtsev, 2018; Zernova et al., 2018) and foreign experience (VanNieuwenborg et al., 2016) in the field of CME described in the literature, these recommendations can be supplemented with the following: Each educational programme should have specific learning objectives and practical benefits obtained by the students following its completion. Intra-organisational training should be organised in the form of consultations, audits and clinical reviews. For distance learning and webinars, distance educational modules can be used. Digital support systems for e-learning, educational modules, medical records and learning management should be developed and implemented. The practical part should include simulation-based coursework along with internships at workplaces and in other medical and/or educational organisations. Full-time classes should be held in the form of problem-oriented conferences, seminars, masterclasses and practical workshops. Interactive training should be ensured. For distance learning and e-learning, multimedia solutions, feedback, forums and enquiries should be used. The implementation of educational programmes should be based on a competency-based approach and individualisation of the education trajectory.
Conclusion
The conducted survey of GPs in the city of Moscow confirmed the relevance of CME for this category of medical workers, allowing problems and key areas for further improvement and development to be identified. The main requirements of the metropolitan GP for the educational process were established to consist of minimum day release, short-term training, scientific and practical orientation, as well as the application of modern educational technologies. Based on a generalisation of the questionnaire results and literature data, conceptual approaches to the development of the system CME in the field of general medical practice in the city of Moscow were formulated. It should be noted that, since most of these approaches are universal, they are also suitable for application in other regions of the Russian Federation, as well as in foreign countries.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.