
Abstract
Hyperammonaemia is a life-threatening condition with numerous aetiologies and a variable presentation. It is increasingly associated with bariatric weight-loss procedures and significant mortality despite treatment. Symptoms often occur long after surgery and at times in association with other trigger illnesses. Patients can present to general medicine, general practice and intensive care as well as surgical and anaesthetic teams. We present the case of a male patient who underwent a sleeve gastrectomy with subsequent weight loss and suffered from hyperammonaemic encephalopathy on multiple occasions. His delayed postoperative complication was likely to be multifactorial in nature, and this is outlined in the case. We discuss presentation, investigation, management and patient outcomes.
Case presentation
A 39-year-old man presented to hospital complaining of lethargy, leg oedema, nausea and vomiting over 6 weeks and feeling generally unwell over 6 months. His medical history included a laparoscopic sleeve gastrectomy 2 years beforehand, when he weighed 180 kg. A cirrhotic liver was noted at the time of surgery with normal serum albumin and bilirubin and no ascites. He had a large anterior abdominal wall hernia, originating from a repaired childhood hernia. Other medical history included well-controlled gastro-oesophageal reflux disease, asthma, psoriasis, anxiety and obstructive sleep apnoea. Regular medication included lansoprazole, ranitidine, paracetamol, codeine, vitamins with minerals and trace elements, colecalciferol with calcium carbonate and ferrous fumarate. His self-reported functional capacity was reasonable, with breathlessness on vigorous exertion. He had never smoked and drank no alcohol.
On initial presentation, he had mild general abdominal tenderness, absent bowel sounds and pitting oedema to the knees. He was hypotensive (101/70 mmHg) and tachycardic (105 bpm), with grade 2 hepatic encephalopathy Further results are listed in (Table 1). Estimated dry weight was 92 kg. A working diagnosis of nonalcoholic steatohepatitis cirrhosis was made. Initial management was in accordance with the decompensated cirrhosis care bundle, with lactulose, spironolactone, intravenous albumin and electrolyte replacement. 1 He was discharged on day five with outpatient fibroscan, physiotherapy, occupational therapy and dietician input.
A summary of investigations.
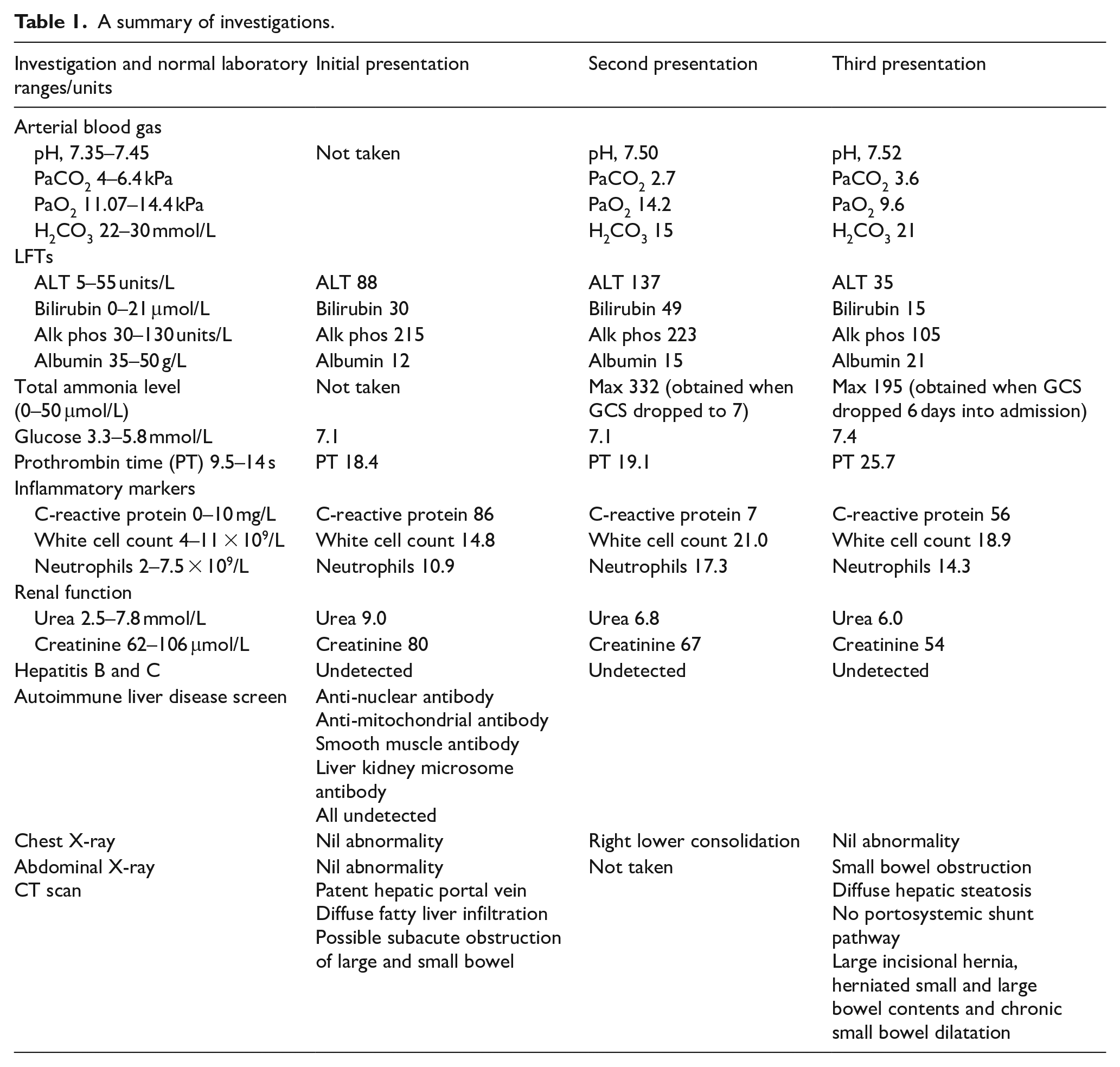
He re-presented 2 days later with confusion. Examination demonstrated reduced consciousness (Glasgow Coma Scale, GCS E4V1M5) and pitting oedema to umbilicus. He continued to deteriorate with tachypnoea (30 rpm), tachycardia (140 bpm), prolonged peripheral capillary refill time (4 s) and reduced consciousness (E4V1M2), requiring intubation. Serum total ammonia level was 332 μmol/L (normal: 0–50 μmol/L). He was treated with sustained low-efficiency dialysis. Eighteen hours after initial sampling, serum ammonia fell to 119 μmol/L, and his conscious level improved to allow successful extubation within 24 h. In addition to previous therapies, he received rifaximin, vitamin B and ascorbic acid and a high carbohydrate diet. Plasma and urinary amino acid and urinary organic acid analysis were normal. He was discharged home after 28 days.
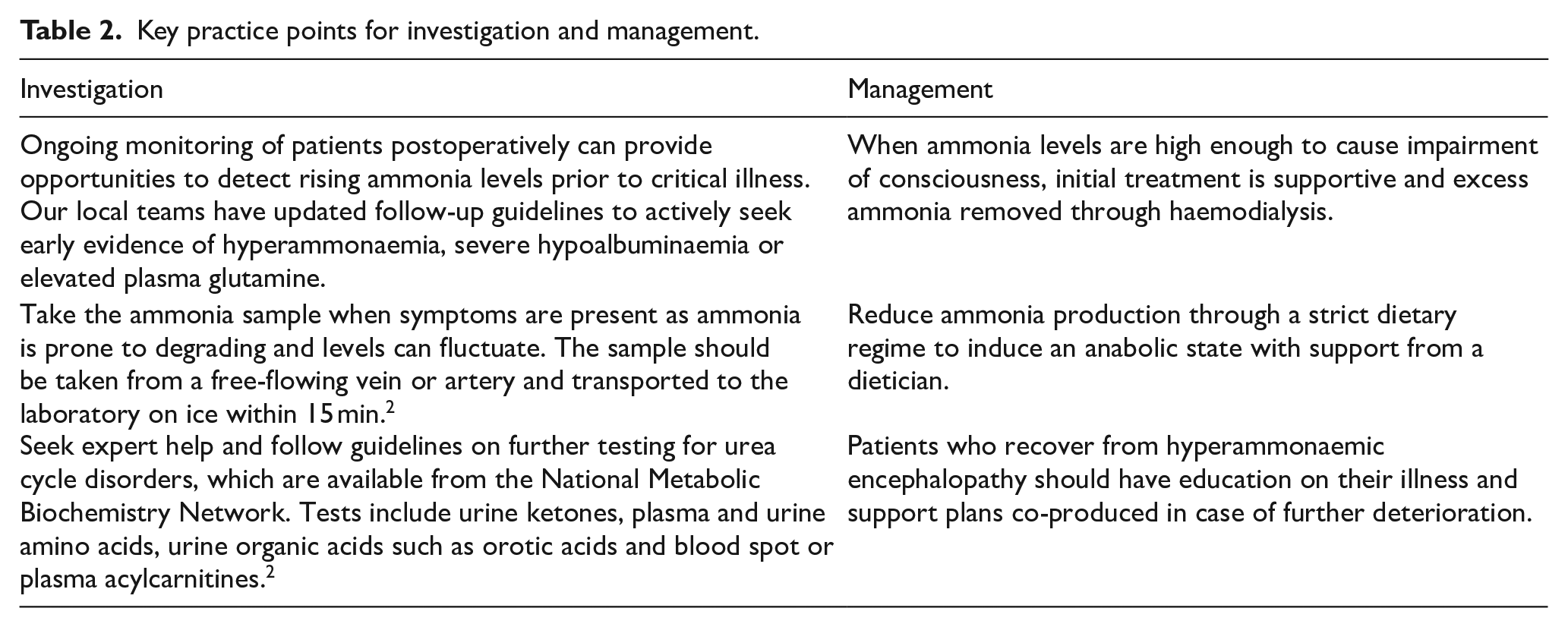
Three months later, he presented with fluctuating consciousness, diarrhoea, feculent vomiting and peripheral oedema. On day six of admission, his consciousness level fell rapidly (E1V1M2), requiring intubation. His serum ammonia level was 195 μmol/L, and he received successful dialysis again. He required significant input from physiotherapy and occupational therapy and was referred to a tertiary centre for abdominal wall repair, which was successful, and assessment for liver transplantation, which was not required. He continues on rifaximin, bumetanide, lactulose, thiamine, vitamin B12 and ferrous fumarate, (Table 2). Two years on, he has not had any further presentations with encephalopathy or decompensated cirrhosis. However, he suffers with forgetfulness, confusion, fatigue, peripheral oedema and the need for walking aids.
Key practice points for investigation and management.
Discussion
Ammonia is a product of protein catabolism via deamination in liver, muscles and kidneys as well as by the action of gut bacteria. In order to be excreted, it is converted to urea via the urea cycle in the liver. In a physiologically normal state, almost 95% of total ammonia measured is in the form of ammonium (NH4+), which is less toxic to the body. As pH increases, there is a greater proportion of ammonia (NH3), which can cross the blood–brain barrier causing clinical signs such as tachypnoea, convulsions and coma. Gradual increases in total ammonia can present with variable symptoms such as lethargy, vomiting and ataxia. A rule of thumb is that a raised serum total ammonia level under 200 μmol/L suggests an acquired cause (e.g. liver failure, valproate therapy), whereas higher levels may indicate underlying metabolic disorders (e.g. inherited urea cycle disorders). 2 Although inherited metabolic disorders are more commonly seen in childhood, these can present in adulthood.3,4 Triggers of adult presentations of metabolic disorders can include catabolic events (e.g. gastrointestinal bleeding), protein overload and pharmacotherapy (e.g. chemotherapy). 5
Hyperammonaemia is a rare complication of common bariatric weight-loss procedures.7,9 There are four main forms of bariatric surgery that enable significant rapid weight loss by reducing the size of the stomach and modifying nutrient and mineral absorption. 6 In the UK, there are approximately 7,000 bariatric surgical procedures per annum. 7 A survey of 3,908 critically ill patients with hyperammonaemia across the USA identified 167 patients with hyperammonaemia and no liver disease; 3.6% had undergone an unspecified form of gastric bypass. 8
One case series of 20 patients (5% male) with hyperammonaemic encephalopathy following Roux-en-Y gastric bypass reported 50% mortality. This is the most common type of bariatric surgery in England. 7 Eleven patients had glutamine levels measured; nine were elevated, in keeping with underlying urea cycle impairment. Four mechanisms were suggested to link gastric surgery and hyperammonaemia: (i) induction of a catabolic state resulting from a significant decline in nutritive intake, (ii) reduction in the urea cycle components through mechanisms such as interruption of citrulline synthesis in intestinal wall, (iii) a favourable environment for a more ureolytic gut microbiome that increases portal system re-circulation of ammonia and (iv) hyperacetylation of urea cycle enzymes, and corresponding loss of function, due to postoperative nutrition deficiencies. 9
Our patient had no prior evidence of liver cirrhosis, but it was found during his operation. In a survey completed in 1998 by 128 bariatric surgeons looking at a collective total of 86,500 bariatric procedures, 39% reported they had found unexpected cirrhosis during an operation, of which 73% were completed. 10 At that time, patients with known cirrhosis were not usually accepted for bariatric surgical procedures. A more recent analysis of 10 studies, looking at patients with cirrhosis who have undergone bariatric procedures, concluded that one can carry out bariatric surgery in patients with ‘well compensated cirrhosis’, indeed some of the studies suggest that following gastric surgery there can be improvement in steatosis, steatohepatitis and fibrosis. 11
Conclusion
We present a case report of a man who underwent a sleeve gastrectomy and suffered from hyperammonaemic encephalopathy on multiple occasions. This rare, delayed, postoperative complication was likely to be multifactorial, with underlying gastrointestinal and nutritional alterations, a degree of nonalcoholic steatohepatitis cirrhosis and evidence of bowel obstruction as a triggering event. We demonstrate the clear need for all physicians, surgeons and intensivists to have an understanding of how bariatric surgery can affect ammonia, its clinical presentation and the initial investigation and management required.
Footnotes
Acknowledgements
We would like to thank the patient who kindly agreed to this case report and took the time to review our write up and add their own input. We would like to thank Dr Monica Doyle, Dr Judith Joss for their clinical input to the case and Dr Michael Miller and Dr Alison Cozens for their input into the write up.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent for the paper to be published was obtained from the patient for publication of the paper.