
Abstract
Grey Matter Heterotopia is a rare clinical entity and its presentation can vary with age. While it usually presents with seizures or behavioural problems, it can seldom present as a stroke mimic. We aim to highlight this rare condition as a differential diagnosis in patients presenting with stroke-like symptoms.
A 64-year-old previously healthy lady presented to our accident and emergency department with the complaints of sudden onset slurred speech, confusion and left-sided weakness and paraesthesia for 1 day. There was no history of tonic-clonic seizures, photophobia or neck stiffness. She had no prior background of epilepsy and/or psychiatric conditions.
On examination, power in the left upper limb was 4/5 on the Medical Research Council power scale and 3/5 in the left lower limb, with no other neurological signs. The rest of the systemic examination was unremarkable. Clinically, an impression of acute stroke was made and a computed tomography (CT) head scan was done which revealed no evidence of acute haemorrhage or ischaemic infarct. However, there was a small 6.3-mm intermediate-density nodule in periventricular deep white matter in the right frontal region, and another nodule located adjacent to the frontal horn of the lateral ventricle on the same side. These incidental small nodules in the right periventricular deep white matter had appearances of grey matter heterotopia (GMH), and this was further confirmed on magnetic resonance imaging (MRI) of the head (Figures 1 and 2).
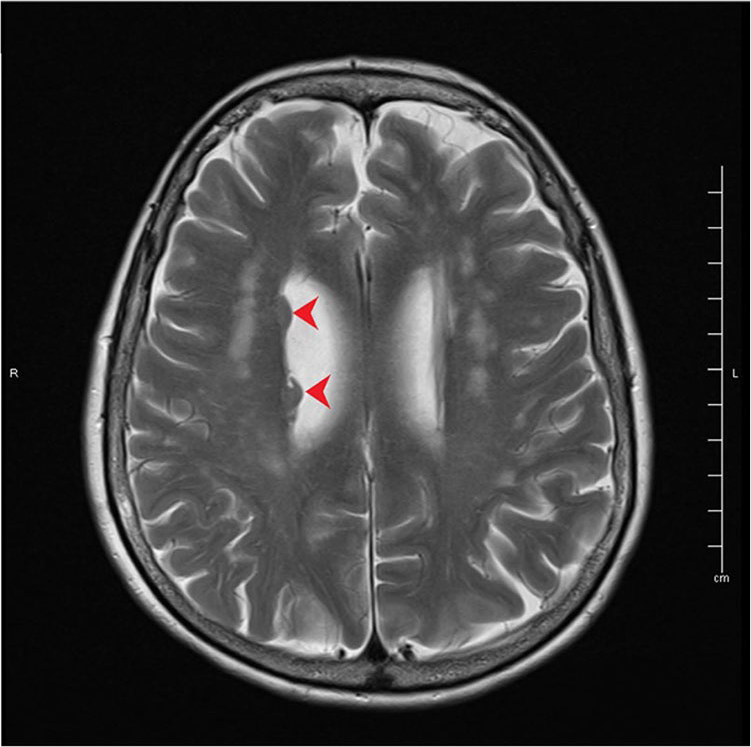
Axial section (at the level of lateral ventricles) of T2-weighted MRI head image shows sub ependymal nodules (red arrows).
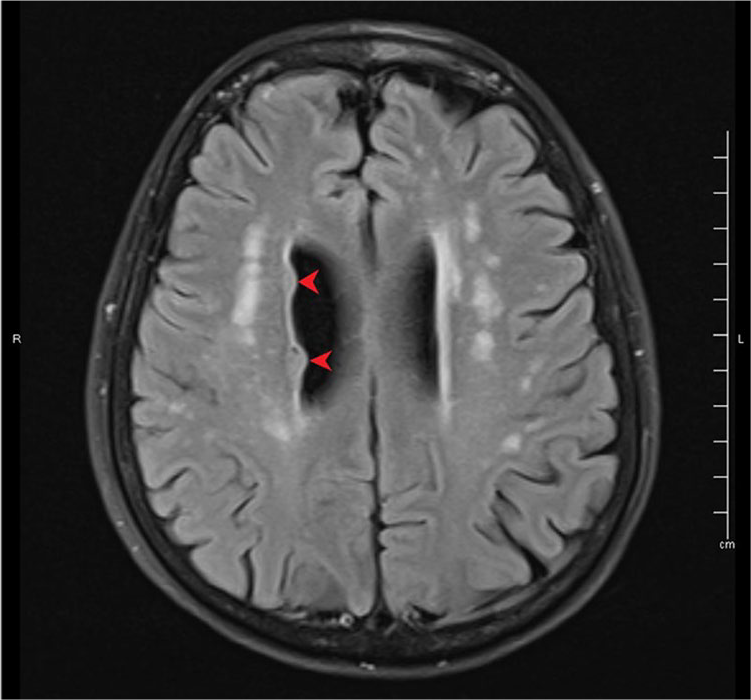
Axial section (at the level of lateral ventricles) of T2 FLAIR MRI head image shows sub ependymal nodules (red arrows).
Grey matter heterotopia are developmental disorders characterised by areas within white matter that have signal characteristics identical to grey matter on T1, T2 and spin echo sequences on magnetic resonance (MR). 1 They are classified as periventricular nodular heterotopia, subcortical heterotopia, subcortical band heterotopia and mixed type. 2 Their aetiology is attributed to both genetic and epigenetic factors. 3 The likely cause is abnormal migration of neuronal cells, during the developmental stage. 4
Across the literature, there is neither an established gender preponderance, nor a consensus on the most common type of GMH. Grey matter heterotopia commonly presents with either epilepsy or a range of psychiatric manifestations, which include delirium, cognitive decline and schizophrenia to name a few. 1 Grey matter heterotopia can present early with mental retardation, epilepsy and speech disorder. Adult-onset GMH usually presents with mild cognitive decline, 2 and neurological manifestations are exceedingly rare. Raza and colleagues reported a case series of 15 patients, out of whom only three had focal neurological symptoms – two with hemiplegia similar to our patient, and one with speech dysfunction. 2 Although a CT head scan might be able to pick up GMH, the sensitivity is less and an MRI remains the gold standard for diagnosing and characterising such lesions. 1
There is no specific treatment for patients with GMH. Grey matter heterotopia needs to be identified by a physician and differentiated from other lesions, as due to its rare presentation it may be missed, and diagnosis and management delayed.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent for the paper to be published (including images, case history and data) was obtained from the patient for publication of this paper, including accompanying images.