
Abstract
This article explores the prominent medical theories in Western Europe, paying attention to how these theoretical frameworks changed perceptions of consuming food. It discusses the idea of moderation of food and drink and how it connected to the practice of Protestantism in the household. Finally, the article explores Scottish domestic papers dating from the seventeenth and eighteenth centuries, focusing on recipe books. Through these sources, this article will highlight the historical ties between food and medicine and how it was understood in the upper-class Scottish households.
The seventeenth century proto-ethnographer, Martin (d.1718) 1 noted that when the people of the Isle of Lewis had a cough: ‘they drink brochan plentifully, which is oatmeal and water boiled together, to which they sometimes add butter. This drink used at going to bed, disposeth one to sleep and sweat, and is very diuretic if it hath no salt in it’ (p. 17). Here is a clear example when food, in this case porridge, was used as a treatment for an illness. And while Martin discussed rural parts of Scotland, most of Western Europe used items that today would be categorised exclusively as food to cure their ailments.
Historians have puzzled over the connection between food and medicine in the early modern period – roughly between 1500 and 1800. In most cases, they have homed in on the domestic sphere as the site of both culinary and some medical production. To explore this location, scholars2–4 have used recipe books and domestic papers to understand how people viewed food within their household. These domestic papers include letters, account books and inventories of private libraries. While these are the set of sources used by many historians studying the connection between food and medicine, some scholars 5 have explored printed diet manuals written by members of the triumvirate – physicians, surgeons and apothecaries. These sources might not centre the domestic sphere, but certainly cannot avoid it. This article uses both sets of sources with emphasis on the former.
As will be discussed, socioeconomic class was inextricably linked with culinary and medical provision for households. The gentry had greater access to a variety of medical care, able to pay the high fees required by the triumvirate and to purchase printed treatises. But wealth also meant greater access to a variety of food and medical ingredients. Whittle and Elizabeth Griffiths 6 have argued that food was one of the ways in which the gentry differentiated themselves from the common folk because their wealth allowed foods to become fashionable rather than purely necessity (p. 104–5). Importantly, the sources used in this article direct the view towards the upper classes. Thus, it must be remembered that what is detailed may not have been accessible to all people.
The first two sections of this article explore the prominent medical theories in Western Europe, paying attention to how these theoretical frameworks changed perceptions of consuming food. It will then discuss the idea of moderation of food and drink and how it connected to the practice of Protestantism in the household. Finally, the article explores Scottish domestic papers dating from the seventeenth and eighteenth centuries with a focus on recipe books. Through these sources, this article will highlight the historical ties between food and medicine and how it was understood in the Scottish upper-class household.
Galenic theory of food
The first important figure to be discussed is Galen of Pergamum (d. 200 BCE) who was a Greek physician. During the Renaissance, his works saw a resurgence along with other classical Greek texts. His theory espoused that the body consisted of four humours: black bile (melancholy), phlegm, yellow bile (choler), and blood. Throughout the sixteenth and seventeenth centuries, these humours became increasingly understood as fluids. Each person had a unique mix of these humours, often referred as his or her complexion, which could be indicated through the temperament of the person or even their skin: so, for example, according to Nicholas Culpeper, 7 a famous English writer of vernacular medical treatises in the seventeenth century, a person with a sanguine complexion was expected to be hairy with ‘a redness intermingled with white in their Cheeks’ (ch. 59). The elevated blood humour in a sanguine complexion could be seen literally in the skin of the person’s face. These humours were also endowed with certain properties: hot, cold, wet, and dry: so, phlegm was composed of the wet and cold, blood of the wet and hot, yellow bile of the dry and hot, and black bile of the dry and cold.
Illness resulted from an imbalance of humours. To rebalance them, practitioners used emetics, diuretics or phlebotomy to expel the excess fluids. These were often harsh methods that left a patient weakened, especially with repeated treatments. But medical treatment was not considered effective unless the patient experienced this elimination.
According to Galenic theory, prevention of disease involved the six ‘non-naturals’: air, food and drink, sleep, exercise and rest, evacuations and obstructions and passions. The non-naturals affected the body from the outside and could misalign the humours through sudden change or disagreement with the person’s complexion.
Importantly, Galenic theory endowed food with the same properties as the humours. For example, it characterised red wine as hot and moist, and the consumable closest to blood, making it more nourishing than white wine. A person’s complexion also dictated what food suited best: older people, who had become colder and drier with age, may have been prescribed red wine because it was hot and moist and thus would restore a balance. Or perhaps, a physician might blame red wine for an older person’s ailments because it did not align with his or her complexion. Therefore, food could ameliorate or cause illness because of its coordination with the person’s complexion. It should be noted that assigning such characteristics to food is not unique to Galen; indeed, some non-Western traditions interpret food as hot or cold. Unfortunately, the inclusion of such practices is outside the scope of this study. What can be emphasised in this article is the idea of food as essential to health, in both maintaining and restoring it, has been entrenched in Western European society and professional medicine for centuries.
Paracelsus’s influence
The second figure who influenced early modern conceptions of food and medicine was Theophrastus von Hohenheim (c. 1493–1541) known as Paracelsus, a Swiss alchemist and physician who disavowed many Galenic teachings and created his own theories of the body and disease. He espoused that all materials consisted of salt, mercury and sulphur, which should be understood as principles rather than materials. Salt was the solidity of things; sulphur was the combustibility and mercury the volatility (p. 202–3). 8 Paracelsus influenced the triumvirate by understanding bodily functions as chemical processes and emphasising distillation as a preferred process for making treatments. His followers became known as iatrochemists, or healer chemists.
Paracelsus’s theory had important consequences for how early modern members of the triumvirate understood digestion. Followers of Galenic theory believed that heat was the driving force behind the process; but one of Paracelsus’s most famous followers, Jan Baptista van Helmont (1579–1644) sought to understand this process chemically and is credited for discovering that the digestive agent was an acid. This discovery and the influence of Paracelsus on the triumvirate should not be understood as a movement towards modern medicine: Paracelsus also famously believed that by eating certain animals, one could obtain their characteristics (p. 302). 9
Adjacent to the iatrochemists were the iatromechanists and iatrophysicists who also sought to reduce the body into matter in motion (p. 220). 8 Iatromathematics can be understood through its most ardent follower, Santario Santario (1561–1636) who set up a series of experiments, perhaps the first ‘scientific’ experiments, during which he weighed his food and then himself before and after eating food, and then once he had evacuated. Since the weight of the food could not be accounted for in these measurements, he believed that some of the food was expired through a form of perspiration. Emblematic of the iatromechanists, Hermann Boerhaave (1668–1738) viewed the body as a system of hydraulics. As professor of medicine at the University of Leiden, he taught many Edinburgh physicians, thus influencing medical practice in Scotland.
Lynette Hunter 10 argues that the influence of Paracelsus – viewing the body as chemical rather than humoral – is visible in printed recipe texts. Increasingly through the seventeenth century, printed recipe collections differentiate between medicine and cookery: the former connected to chemical preparations and the latter used herbs (p. 96). This is perhaps true for printed texts in England, but as will be discussed later in this article, manuscript recipe books are not so easily divided. But medical manuals written by the triumvirate do differentiate these genres. In his book on regimen entitled An Essay on Health and Long Life (1724), 11 Dr George Cheyne (1672–1743), an iatromechanist, distinguished between ‘cookery’ and ‘physick’, indicating that he saw them as separate, but related, genres (p. 29). He thought that people should understand the roles of both in maintaining a healthy life; but they were separate. The influence of Paracelsus, as discussed previously, may account for this separation. As would perhaps the desire to distinguish between the feminine task of cooking and the masculine pursuit of physick, an idea discussed further in another part of this article.
Moderation
Despite the appearance of various theories of the human body throughout the sixteenth and seventeenth centuries, Galenic theory consistently remained the framework through which the triumvirate and, to some extent, the common folk viewed the functioning of the body. Despite being largely an iatromechanist, George Cheyne’s An Essay on Health relied on Galen’s ‘non-naturals’ for guidance and structure. Each chapter dealt with a non-natural and he expounded his own opinions on how and why they mattered to healthy living. The relevant chapter for this discussion, ‘Meat and Drink’, provided general maxims including eat and drink in moderation: ‘To have our Food, that is, our Meat and Drink, as to Quantity and Quality, duly regulated, and precisely adjusted to our concoctive [digestive] Powers, would be of the utmost Consequence to Health and Long Life’ (p. 12). 11
But to Cheyne, what constituted as moderation changed depending on the patient. Some required more rules and restriction to achieve health. His text can be understood as part of his movement towards restrictive diets to cure disease. He wrote: to cut off our Days by Intemperance, Indiscretion, and guilty Passions, to live miserably for the sake of gratifying a sweet Tooth, or a brutal Itch; to die Martyrs to our Luxury and Wantonness, is equally beneath the Dignity of human Nature, and contrary to the homage we owe to the Author of our Being [p4].
11
Indeed, early modern people and texts emphasised the necessity of moderation in a diet to prolong life and health.
What is also striking about this passage is the moral imperative placed on moderation. Early modern Protestant Christianity believed that a healthy body indicated a healthy soul. Thus, moderation in food maintained health, pleasing God. The link between piety, food consumption and health can be seen in ecclesiastical texts as well as dietetic manuals. The Scottish episcopalian clergyman, James Kirkwood (c1650–c1708) wrote a guide to raise proper pious children entitled The true interest of families (1690).
12
According to his manual, when Children are fit for stronger Food, Parents are not to indulge them too much in gratifying the curiosity and daintiness of their Palate, which not only is apt to make them too soft and tender; but likewise disposeth them to gluttony and sensuality; to make their Belly their God. It is fit to accustom them to a plain and simple Diet; which is generally more wholsom than that sort of Food which is very artificially prepared [p58-9].
Moderation battled both ends of the consumption spectrum: eating too much (gluttony) at one end and too little (what he called daintiness) at the other. He also claimed that moderation includes a plain diet. Immoderate eating led to un-healthiness but importantly also drove people to worship their stomach, taking attention away from the real God. For Kirkwood, part of the duty of a parent raising pious children involved teaching them a good relationship with food leading to health.
It is important to stress that early modern period Britain saw different modes of thinking about food and medical treatment, much of which was viewed through the framework of Christianity. Through piety and production, the household became the site of food and medicine, including how people learned to use food to maintain health.
Recipe books
Up until this point in the article, I have spoken generally about Western Europe and Britain, but I would like to narrow this further to Scotland. Perhaps the most emblematic material item of the connection between food and medicine is the early modern recipe book. Manuscript collections of household, culinary and medical recipes were kept in bound notebooks of varying sizes. Usually, they were small though to enable easy access and quick referencing. The recipes themselves were often written in several hands, indicating that these documents were collaborative, either across generations or family networks. Most early modern Scottish manuscript recipe books date from the seventeenth century and the eighteenth century. Scottish printed recipe books become increasingly common in the eighteenth century, but English printed recipe books had been available in the country since at least the seventeenth century and appear in inventories of Scottish libraries.
Briefly, it is important to discuss some of the differences between Scottish and English recipe books because there is more scholarship on the latter sources. During the period, there was increasing cross-cultural communication: the union of the crowns when James VI took over the monarchy of England after the death of Elizabeth I occurred in 1603, enticing many of the upper classes to London for part of the year. In 1707, the parliaments were united, meaning that arguably, the upper classes spent more time south of the border than before or, at least, had political interest there. Because the upper classes of Scotland and England mingled, they exchanged knowledge. But there were some differences. For one, Scottish people were still speaking Scots, even if just employing Scots vocabulary within English. They were also using Scottish measurements such as the chopin (at one time, about a half of a Scots pint, when a Scots pint equated to about two to three Imperial Pints) and the mutchkin (about a quarter of a Scots pint), only the latter has been evidenced in England, and only in the northern regions. 13 Thus, there were fundamental differences in these sources, solidifying the necessity to study Scottish recipe books as their own set of texts but also alongside their English counterparts and the scholarship that has risen around them.
While collections often remain anonymous, we can assume that British collections were written mostly by upper class women. In this period, a wife controlled proportionately more of the care of the household than a husband. The collector also needed to be able to read and write as well as have access to paper, a trifecta only really available for the wealthy. These sources direct scholars to a specific portion of society, therefore, not all of Scotland will be represented in this section.
Understanding recipe books as a feminine enterprise allows scholars to begin to unpack how women operated within a patriarchal society. Scholars have used recipe books and material culture to understand the role of the kitchen in early modern British society. Because of its links to food preparation, early modern people viewed the kitchen as mainly a feminine space; although this did not prevent men from operating within it. 14 The triumvirate actively sought to separate themselves from the medical preparation occurring in the kitchen – or ‘kitchen physick’ – because of its feminine characteristic. But the kitchen is a symbol of the quiet power that women held. Women used their recipe books to concoct medical preparations, regaining the health of a member of the household. But also, Sara Pennell 15 has emphasised the kitchen was a place of ‘transformation and transgression’ because ingredients became meals, which could be poisoned (p. 208). Thus, by operating within the kitchen, women gained power over food and medicine.
These manuscript recipe books share many characteristics and features with modern cooking books. They were often passed down through generations, most often from mother to daughter. In the inscription for her recipe book, 16 Jean Wemyss, Countess of Sutherland (1629–1715) wrote ‘This Book was my mothers in which are many Receipts [Recipes] which she had from the most famous Physitians that Lived in her tyme, she dyed in November 1649 J W Southerland’ [fol. ir] (For quotations from manuscripts, I have silently expanded abbreviations, which I will continue to do throughout this article. Thus, ‘ye’ is written as ‘the’ and ‘wch’ as ‘which’, et cetera.). Collectors also attributed recipes to the friend or family member who gave it to them. This has led the historian Elaine Leong 2 to understand recipe collections as social ledgers (p. 21). In Jean Wemyss’s text, 16 there is ‘A Receipt for the Cancer which I had from the Countess of Lawderdale’, which includes a postscript ‘my mother in law’ written in a lighter ink, indicating it was written later than the recipe (fol. 73v-74r). This postscript indicates the connection between the Sutherlands and Lauderdales and that Jean’s granddaughter possessed the book – also called Jean (c1692–1747) who married the son of the fifth Earl of Lauderdale. Thus, indicating that the book passed through at least four generations.
In some ways, early modern recipe books are also analogous to the modern medicine cabinet, more of a ‘just-in-case’ measure than an everyday necessity. It cannot automatically assume that the households who owned these collections used or made all the recipes. For example, in a portion of Grisell Baillie’s (1665–1746) recipe book 17 dated after 1712, there is ‘A cordial Water against the Plague’ (p. 256), which can be assumed to refer to the Black Death because of the definite article, otherwise perhaps it would be for plagues. Grisell spent much of her life in England, which experienced an epidemic of the Black Death later than Scotland – the last for both respectively were 1665-6 and 1645-7. Certainly, there were later instances of the Black Death in Great Britain, but these were not on the scale of previous periods; arguably, the disease was certainly dying down as a major concern by the early eighteenth century. 18 Thus, there is a high probability that Grisell never used this recipe. Even if some of the recipes were not implemented, recipe collections illuminate the medical concerns of the period. While Grisell arguably never made the treatment for the Plague, the existence of the recipe in her collection highlights the continued fear of its reoccurrence. They can also provide information on how practitioners would have treated a patient if they were to suffer from the ailment.
Importantly, they are usually both a cookbook and a medicine cabinet, with little if any distinction between the two genres. It is tempting to understand food and medicine as separate entities, but as has been evidenced, they were closely linked in early modern thought. As discussed earlier, Lynette Hunter 10 has argued that printed recipe books indicate a distinction between the medicine and culinary food because of the flexibility of manuscript collections – most collectors wrote recipes as and when they were needed – it is not so clear cut. It was not usually a priority to ensure that recipes were written in any sort of order, even by ailment, and thus it is difficult and, in some ways not relevant, to attempt to understand the influence of medical theories on manuscript recipe books. That is not to imply that collectors were not influenced by medical theories – they did obtain these recipes from members of the triumvirate who studied them – but perhaps it is more interesting to study these documents as illustrative of the plethora of treatments available to members of the public. Now that the source has been thoroughly explored, this next section will discuss the blurred delineation between food and medicine.
‘Food’ in medicinal recipes
One of the first notes for modern scholars in studying medical recipes in collections is the abundance of ingredients that are now associated with solely culinary endeavours. The two largest sections of culinary ingredients in these recipes are spices and herbs. In closely studying five Scottish recipe books16,17,19–21 and separating out the medical recipes, the top twenty ingredients used in these recipes are represented in the Table 1 below:
Top 20 ingredients.
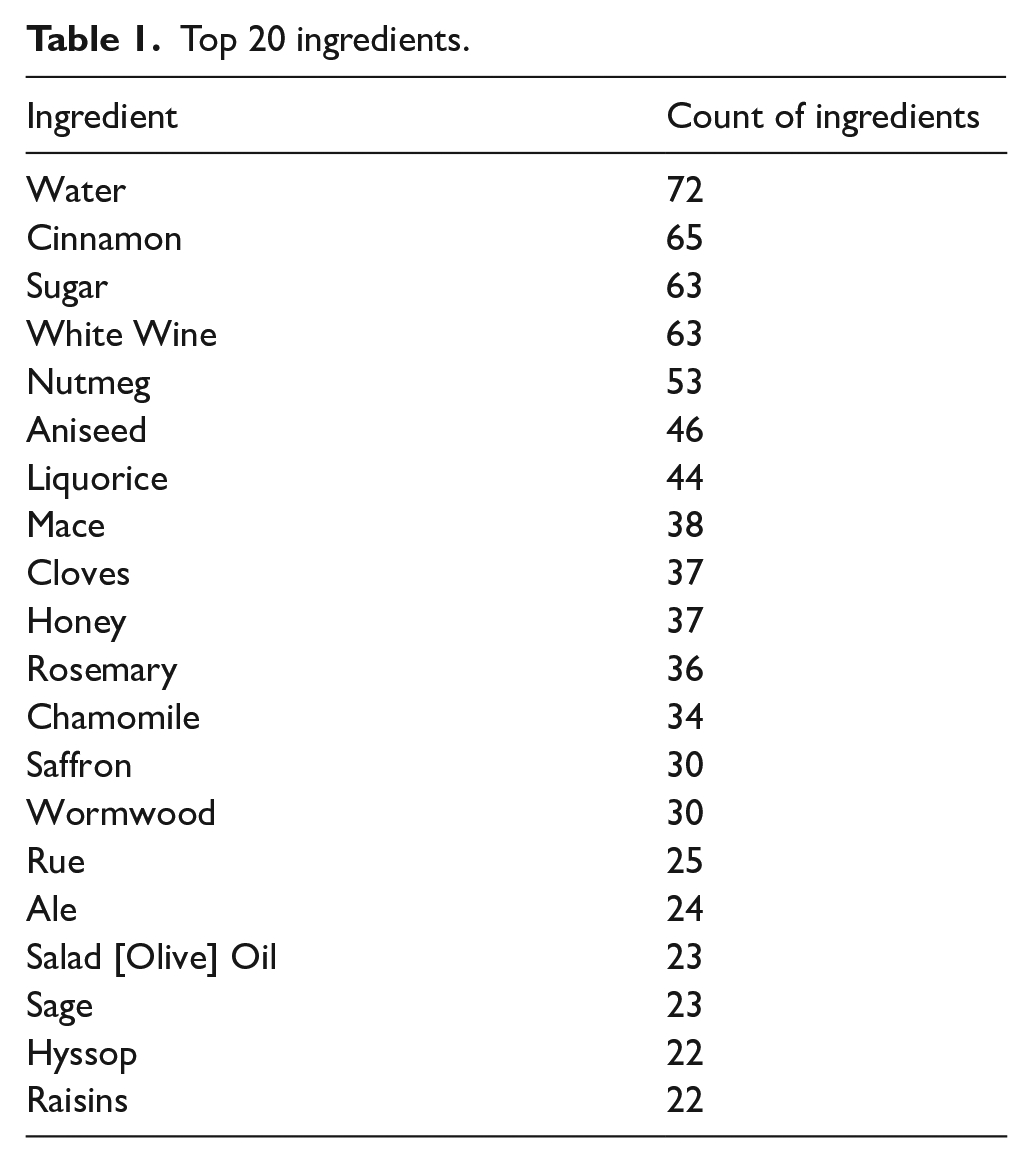
Each of the ingredients produce a strong reaction from one of the senses: e.g. cloves certainly have a strong flavour and smell. This is certainly the reason they are used in culinary recipes. Gabrielle Hatfield 22 posits this characteristic could distract the sufferer from their symptoms, creating a perceived benefit (p. 317). But equally probable was the mystique ascribed to imported ingredients, which increased medical efficacy. The top three on the list are all imported ingredients, acquired from different parts of the world. Many of the top twenty are associated with the East Indies – cinnamon, nutmeg, mace, cloves and saffron – some with the Continent – white wine, salad oil, rosemary and hyssop – and one with the growing trade in the West Indies – sugar. The only ingredients in the top twenty listed as native to Scotland by James Sutherland, first gardener of the Royal College of Physicians Edinburgh physic garden, are camomile, liquorice, wormwood, rue, and sage. Even then, only specific species of these plants were named, like mayweed, which is part of the camomile family. Without studying the import documents and apothecary sales, it is difficult to determine whether people gave preference to the native mayweed or imported camomile. Certainly, the amount of foreign ingredients suggests that by the end of the seventeenth century, the professional and upper classes did not subscribe to the view that God planted cures where disease arose.
The number of imported ingredients highlights both the availability of the items in Scotland and the ability for the wealthy to purchase and use them. The first point reiterates that Scotland participated in international trade prior to the union of the parliaments. Scholars once held the belief that Scotland’s trade prospects increased significantly post-union, but this idea has been tempered within the last couple of decades. 23 Indeed, Scotland had access to ingredients from its trading relationship with England prior to the union but also through its relationship with the Dutch East India Company. The second point is connected to the first because imported ingredients were more expensive and thus more readily available to those who could afford them. Recipe books, therefore, illuminate the privilege provided to the upper classes in Scotland: they had more disposable income, therefore they could purchase more expensive ingredients with perceived medical and demonstrative culinary benefits.
The crossover in culinary and medical ingredients poses difficulties for historians of medicine studying household account books. Lady Jean Wemyss kept an account book 24 from 1650 to 1654, detailing her household’s consumption of goods and services. On 3 September 1653, she spent 10s on 2 ounces of green ginger, the intention of which is not explicitly noted [fol. 28r]. (It is assumed that this entry is in Scottish money, but Jean did not explicitly state this in the text.) Helpfully, Lady Jean was not usually so opaque. One explicit example of food items used for their medicinal properties is on 3 November 1651, when money was spent on ‘wine and spices when I had the cholchik and gravell’ [fol. 25v]. Even without the stated intention, wine and spices purchased together could be assumed to be medicinal, particularly since Jean employed a cook and thus did not control the minutiae of the household culinary accounting.
Recipe books include ‘sick dishes’, which were used for convalescence (p. 421). 25 These dishes were easily ingested and digested, such as pottages, gruel, soup and diet drinks. Often these recipes include both culinary and medicinal language. The example at the beginning of this article may be considered a ‘sick dish’, used more to nourish and comfort the body than to provide medical help.
There are some defining features of these recipes. They are often light in colour and humorally neutral, meaning they could be used on any complexion (p. 324). 26 In an anonymous recipe book with the initials ‘MIM’ written on the inside cover, 21 there is a recipe ‘To make a good colling [cooling] broath for anybody [emphasis added]’, which goes against the Galenic idea that treatments must be individualised (p. 35–6). The recipe also creates a thin chicken soup, which contrasts with a thicker, darker stew made with beef. The use of chicken, however, aligns with Galenic theory because it was seen as an almost universally easily digestible food.
Recipe books also illustrate the prevalence of digestive issues in early modern Scotland. These ailments include kidney and gallbladder stones and indigestion caused by an overindulgence in food or drink, known as surfeit. Foodstuffs held the intriguing position of being able to cause diseases and cure them on an almost equal level. In Jean Wemyss’s collection,
16
there is a recipe for ‘A receit for the paine in the stomack or Cholick’ take a scots pynt of good nanze [Nantes] Brandie, in which infuse of ride [red] Rose Leavis, of Clove giliflours Leaves, of Corn Rose Leaves, of March violot flowres, of each ane handfull also of Balm Leaves, of Rosmarie flours of Mairgilen, of agremonie, and tops of Rosmarie, of each half ane handfull, add to all thes a pound of Beaten sugarcandie, and take of this Brandie so prepared one spoonfull or two when yow fear a Cholick [fol. 55r].
This recipe also highlights some of the emotions that accompanied digestive issues, using ‘fear’ as a method of premonition. In the account book of John Clerk of Penicuik, 27 he recorded the purchase of ‘sum pouders for the gravel’ in March 1663 but was apparently still suffering from the ailment a few months later because he purchased ‘halff a mutchkin off sueit [sweet] oyll for the gravel’ in June (p. 46, 62). It is possible that these treatments were for a member of his household but in either case, the change in treatment indicates the same patient trying different methods to ease his or her discomfort.
Because of the incidence in recipe books, a digestive ailment that appears to have been common in children is stomach worms. Due to the nature of the recipe books, it is difficult to determine if these worms were truly parasites, but they certainly were a digestive issue understood to be incident to children. Alun Withey
28
has highlighted that these ‘worms’ could have been transferred to children through improperly cooked meat (p. 22). Passing such organisms to children would have had a greater effect than if passed to an adult and the recipes indicate that it was prevalent and worrying. While a digestive issue, stomach worms were often treated through plasters laid across the stomach. For example: a plaster for childrine That hath stomack wormes Take a quantitie of nuttmege, of methridate asse much, of conserve of roses a spoonfull, of whyte wyne winegar halfe a spoonfull of the juyce of wormwood a groats worth, of safrone a penne worth, also manie crumes of broune bread as will thicken It so spread it upon a piece of Leather and Lay it upon stomack reaching to the navill [p90-1]
21
This type of treatment avoids the unpleasant effects of other early modern medicines, which would be harmful to the relatively weaker body of a child. It is not clear if parents saw these plasters as effective for treating the problem, but it does illustrate that early modern people adjusted treatments based on the patient.
Conclusion
In summation, this article has provided an overview of connections between food and medicine in early modern Western Europe. Galenic and Paracelsian frameworks helped the triumvirate to understand how the human body worked including how it ingested, digested, and even excreted food. But in narrowing medical practice to recipe books, the dichotomies between Galenic and Paracelsian and between food and medicine blur. In the everyday, people gathered information and attempted treatments which did not leave room for such delineations. Recipe books illustrate the availability of knowledge beyond the triumvirate, but also people’s ability to try things until something worked.
I hope to end by highlighting some key points from this discussion of the historical ties between food and medicine. One, the influence of wealth on access to food and medicine has been present for centuries in Scotland. The National Health Service has certainly ameliorated the gap, but it is beneficial to keep this in mind when thinking about food and medicine. The second point is that practitioners’ advice to maintain a healthy life consistently has included moderation. Though the definition may have changed slightly, George Cheyne and James Kirkwood’s ideas ring true to modern ears, even if we do not want to hear it. The final point is that women were instrumental in providing food and medicine to their households. While male historical actors have figured prominently in this article, sources like recipe books indicate that early modern women had a quiet but powerful role in maintaining and regaining the health of those around them.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.