
Abstract
Acanthamoeba is a rare cause of granulomatous amoebic encephalitis (GAE) associated with high mortality. There have been few case reports of Acanthamoeba meningoencephalitis worldwide. Hemophagocytic lymphohistiocytosis (HLH) is a severe hyperinflammatory condition caused by abnormally active macrophages and cytotoxic T lymphocytes; its secondary form is due to infections or malignancies. However, HLH is rather an unknown complication of GAE. We describe an unusual and previously unreported case of Acanthamoeba meningoencephalitis in a young immunocompetent female culminating in secondary HLH.
Introduction
Acanthamoeba spp., Balamuthia mandrillaris and Naegleria fowleri are a few pathogenic and opportunistic free-living amoebae which could perhaps potentially infect humans and other animals. They are aerobic, mitochondriate protists that are found all over the globe. All three amoebae elicit central nervous system (CNS) infections. There are many species of Acanthamoeba that are known to cause disease, including Acanthamoeba castellanii, Acanthamoeba culbertsoni, Acanthamoeba hatchetti, Acanthamoeba healyi, Acanthamoeba polyphaga, Acanthamoeba rhysodes, Acanthamoeba astronyxis and Acanthamoeba divionensis. Granulomatous amoebic encephalitis (GAE), caused by Acanthamoeba, is an insidious, persistent and largely catastrophic illness, especially in immunocompromised individuals. 1 More than 150 cases of GAE have been reported yet, of which only 11 (7%) were immunocompetent. GAE associated with Acanthamoeba often manifests as a nonspecific or subclinical illness and has a high mortality rate of 44–90% if not identified at an early stage. 2 The pathophysiology of GAE is not completely understood, although complications might include infiltration of blood–brain barrier, brain parenchymal damage and CNS neurovascular compromise. 3 However, hemophagocytic lymphohistiocytosis (HLH) is rather an unknown complication of GAE.
HLH is a severe hyperinflammatory condition caused by abnormally active macrophages and cytotoxic T lymphocytes; its secondary form is often driven by infections or malignancies. The syndrome is marked by fever, hepatosplenomegaly, cytopenias, liver dysfunction, hyperferritinaemia, hypertriglyceridemia or hypofibrinogenemia. 4 Predominant infectious causes of HLH include viral infections like epstein-barr virus (EBV) and cytomegalovirus (CMV), as well as bacterial infections such Staphylococcus aureus and Mycobacterium tuberculosis. 5 Parasite triggered HLH has been most commonly reported with Leishmania spp. although malaria (Plasmodium falciparum and Plasmodium vivax), toxoplasma, babesiosis and strongyloidiasis have also been described with hemophagocytic syndrome. 6 We describe an unusual and previously unreported case of Acanthamoeba meningoencephalitis in a young immunocompetent female culminating in secondary HLH.
Case presentation
A 19-year-old female from the southern part of India who was residing in Uzbekistan for her medical education was admitted to the All India Institute of Medical Sciences, New Delhi, India. She presented with low-grade fever for 20 days and reduced cognitive function for 8 days. She had no concomitant comorbidities and on physical examination, she had pallor and was irritable with a Glasgow Coma Scale of 12 out of 15. She also presented with a stiff neck in conjunction to positive Kernig’s sign and Brudzinski’s sign. Her blood pressure was 108/72 mmHg with a pulse rate of 103/min and body temperature of 100.8 F. Abdomen and chest examination was unremarkable. A provisional diagnosis of acute meningoencephalitis was made, and she was started on intravenous ceftriaxone (2.4 g), acyclovir (1.5 g) and doxycycline (200 mg). A contrast-enhanced CT head was performed, which revealed no abnormalities. Cerebrospinal fluid (CSF) examination revealed lymphocytic pleocytosis with hyper-proteinoracchia and hypo-glycoracchia (Table 1). No tuberculous, viral, fungal or bacterial pathogens were identified using direct staining, nucleic acid amplification test or additional biomarkers. CSF wet mount for free-living amoeba exhibited sluggishly motile organisms with spiny projections morphologically resembling Acanthamoeba spp. trophozoites. The finding was confirmed by CSF polymerase chain reaction (PCR) for Acanthamoeba, which was strongly positive. Once the diagnosis of Acanthamoeba meningoencephalitis was established, patient was started on combination therapy of Oral Fluconazole (800 mg), Rifampicin (450 mg), Azithromycin (500 mg) and Miltefosine (50 mg). In addition, since Acanthamoeba is sometimes referred to as a ‘Trojan horse’ for several other microorganisms, such as viral, bacterial, protist and yeast pathogens, we continued additional antimicrobial therapy until CSF culture was sterile and viral and bacterial PCR were negative. MRI brain was also done which showed multiple T2 FLAIR hyperintensities in grey white matter junction of right cerebral hemisphere and cerebellum with no diffusion restriction/contrast enhancement/blooming on susceptibility weighted imaging (SWI), suggestive of lepto-meningitis.
Cerebrospinal fluid analysis.
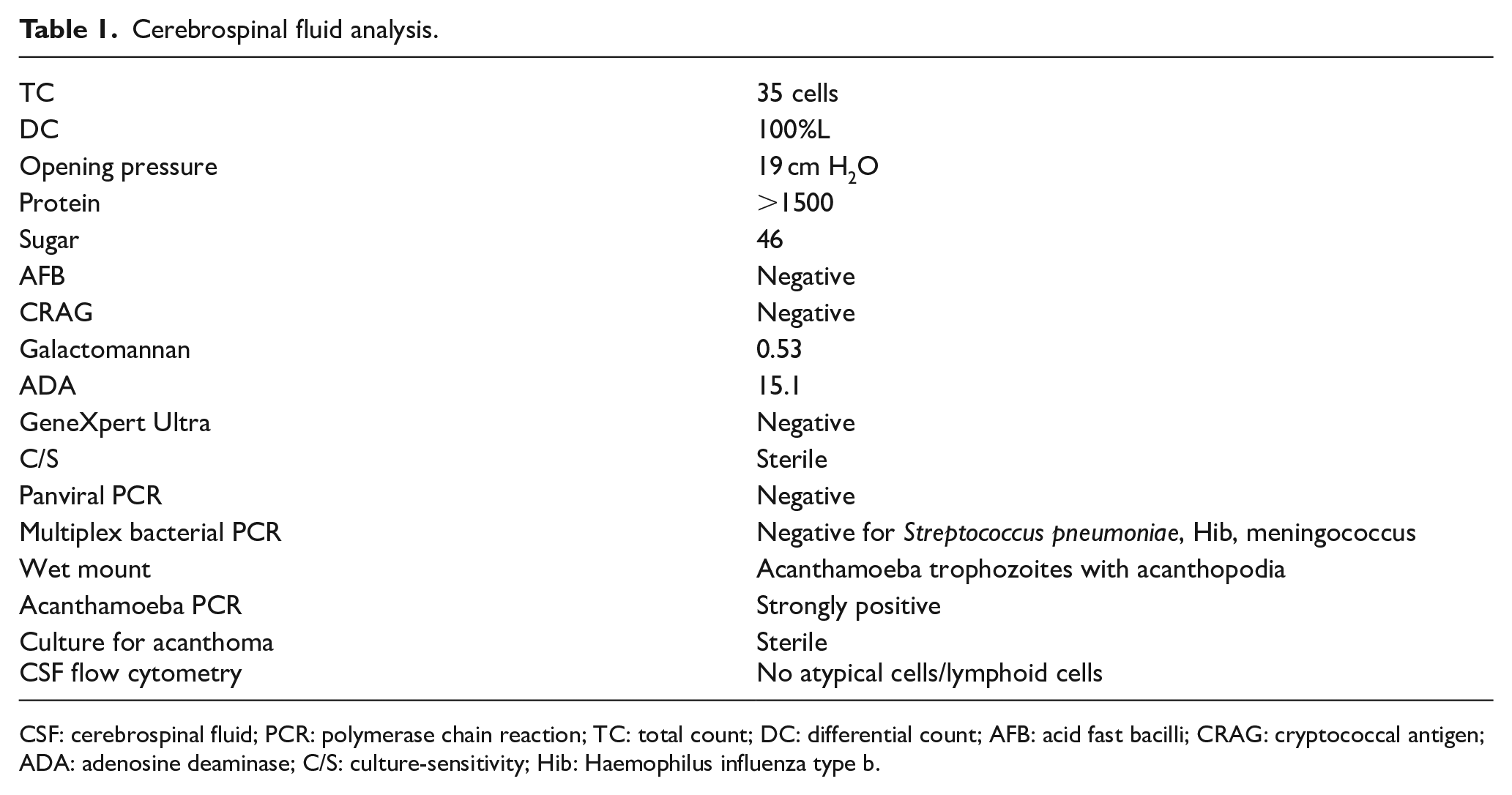
CSF: cerebrospinal fluid; PCR: polymerase chain reaction; TC: total count; DC: differential count; AFB: acid fast bacilli; CRAG: cryptococcal antigen; ADA: adenosine deaminase; C/S: culture-sensitivity; Hib: Haemophilus influenza type b.
On routine investigations at admission, she also had anaemia and thrombocytopenia, which progressed to pancytopenia the following day (Table 2). With worsening pancytopenia and no evidence of haemolysis or any other evident cause and significantly raised ferritin, triglycerides and transaminitis (>2 times), she underwent a bone marrow examination. The examination revealed a hypocellular marrow with myeloid preponderance and normal maturation, megakaryocytes and erythroid precursors were adequate with no evidence of any atypical cells. With worsening clinical and laboratory parameters, she was started on dexamethasone (16 mg) on day 4 based on the clinical judgement of treating team in view of secondary HLH. Unfortunately, her clinical parameters kept on worsening and she was shifted to ICU on day 8. Her decreased consciousness necessitated intubation and mechanical ventilation. She succumbed to her illness with multiorgan dysfunction on day 10.
Laboratory parameters from Day 1 to 10.
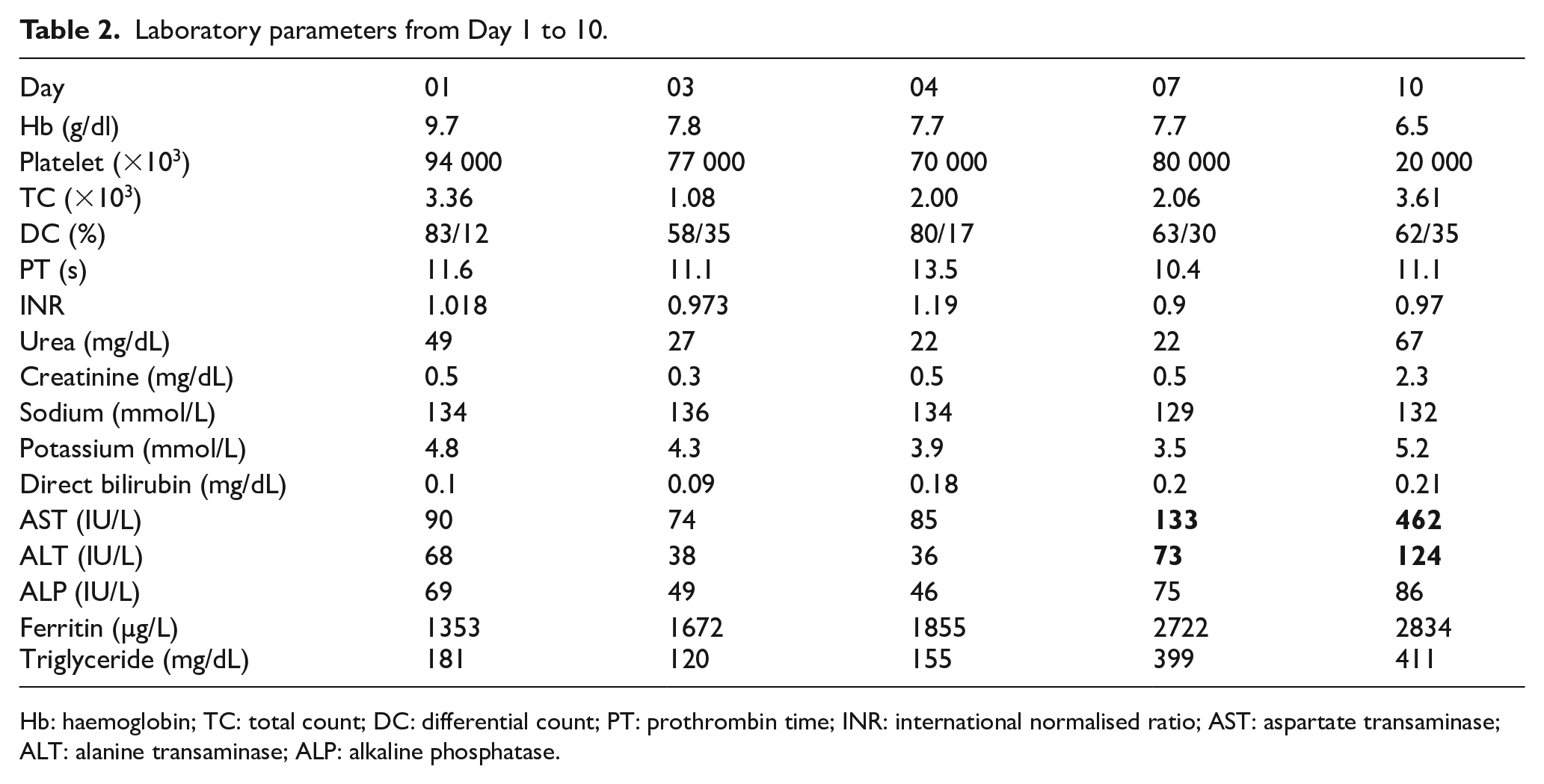
Hb: haemoglobin; TC: total count; DC: differential count; PT: prothrombin time; INR: international normalised ratio; AST: aspartate transaminase; ALT: alanine transaminase; ALP: alkaline phosphatase.
Postmortem minimally invasive tissue sampling (MITS) was done to collect specimens from brain, lung, liver and spleen for histopathological examination. Brain specimen revealed mild chronic inflammatory infiltrates in the meninges. Splenic specimen showed congestion of red pulp with collection of macrophages and hemophagocytes with areas of micro-abscess. The final impression from MITS of all organs was septicaemia-induced changes with hemophagocytosis (Figure 1(a) and (b)).
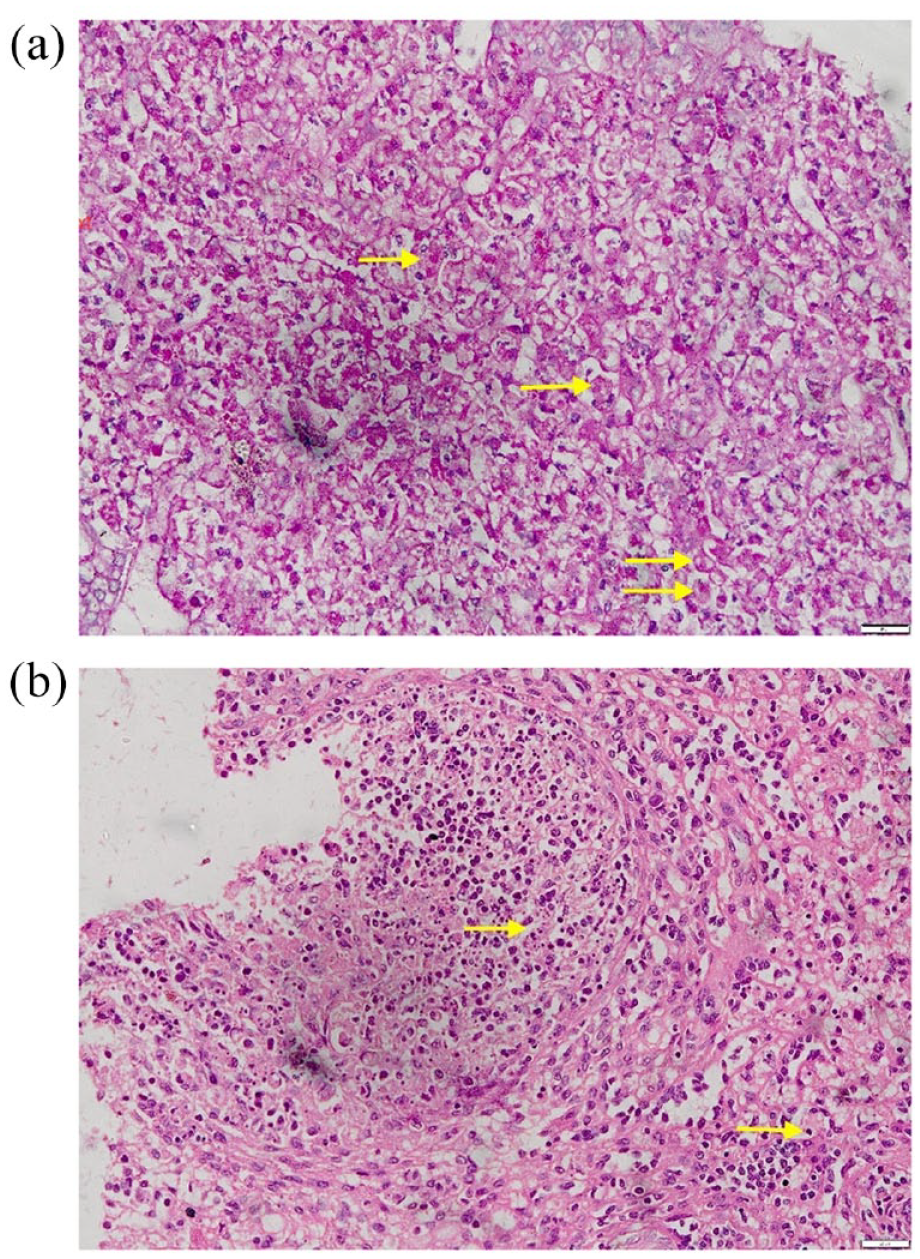
(a) Liver biopsy: H&E staining 40× magnification – evidence of hemophagocytosis – erythrocytes engulfed by macrophages (yellow arrows) and (b) splenic biopsy: H&E staining 40× magnification – evidence of hemophagocytosis – lymphocytes engulfed by macrophages (yellow arrows). H&E: haematoxylin and eosin.
Discussion
To the best of our knowledge, we report the first case of Acanthamoeba meningoencephalitis causing secondary HLH. Acanthamoeba is a free-living organism present ubiquitously but commonly present in water sources like lakes, ponds, rivers and so on. 7 Most of the case reports of GAE have been reported from North America and Indian Subcontinent. 3 Our patient was immunocompetent and didn’t have any history of water body exposure. At the time of symptom onset, our patient was residing at Uzbekistan, only few cases have been reported from the region so far. 3
Early diagnosis and treatment initiation is critical for preventing complications and improving survival of the patient. Diagnosis is critical and can be made using CSF, histopathology examination of biopsy from skin lesions, sinus, lungs or brain, which is mostly obtained postmortem. 8 CSF can be analysed for direct wet mount examination which is a rapid, simple cost-effective diagnostic tool 9 and by polymerase chain reaction (PCR) or real-time PCR. CSF PCR has sensitivity and specificity of 100 and 99.28%, respectively, with culture as the gold standard and had high positive predictive value (90.9%) in the diagnosis of Acanthamoeba meningoencephalitis. 10 Histopathological samples can be stained with hematoxylin and eosin, Grocott’s Gomori Methenamine-Silver, Trichrome, Wright, Calcofluor white and so on for the visualisation of cysts or trophozoites. Acanthamoeba can also be cultured using axenic media, xenic media and tissue culture. 3
HLH can mimic an infection and can blur its presence. Therefore, its diagnosis requires high clinical suspicion along with presence of at least five diagnostic criteria out of the eight proposed in 1991 and revised in 2004. 5 Ante-mortem, our patient had persistent fever, pancytopenia, hyperferritinemia, hypertriglyceridemia and liver dysfunction. The patient was started on anti-microbials and dexamethasone (10 mg/m2 BSA) based on high clinical suspicion of HLH. Diagnosis of HLH was confirmed in our patient postmortem with the presence of hemophagocytes in spleen.
There is no general consensus regarding the treatment regimen for Acanthamoeba meningoencephalitis. Treatment can be given with a combination therapy of trimethoprim-sulfamethoxazole, fluconazole, miltefosine, flucytosine, rifampicin or sulfadiazine-pyrimethamine. 3 Das et al. 11 has reported successful outcomes in two immunocompetent patients with combination anti-microbial therapy. However, Reddy et al. 12 has reported a case of GAE in a 38-year-old immunocompetent male who succumbed to the illness in spite of treatment. Our case is the first confirmed case of Acanthamoeba meningoencephalitis causing secondary HLH.
Conclusion
Our case highlights the rare association of HLH with Acanthamoeba meningoencephalitis and the need for extensive clinical and laboratory evaluation of suspected patients by a multidisciplinary team.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient’s parents for publication of this case report and any accompanying images.