
Abstract
Primary hyperparathyroidism (PHPT) is the leading cause of incidentally detected hypercalcaemia in asymptomatic individuals. Rarely, PHPT may present with severe hypercalcaemia or even hypercalcaemic crisis. We describe a case of a 53-year-old male who presented with acute severe hypercalcaemia as the index manifestation. Complete clinical, biochemical and radiological evaluation led to an eventual diagnosis of PHPT. He had a challenging clinical course as hypercalcaemia did not improve significantly despite undergoing multiple sessions of haemodialysis and other supportive measures. Furthermore, the presence of acute kidney injury precluded the use of bisphosphonates. In the end, he received subcutaneous denosumab injection and his serum calcium levels improved dramatically afterwards. Subsequently, he underwent successful parathyroidectomy. Denosumab therapy can play a critical role in managing such patients especially when other therapeutic modalities cannot adequately control hypercalcaemia.
Keywords
Introduction
Primary hyperparathyroidism (PHPT) is a common endocrine disorder. When PHPT is caused due to parathyroid adenoma, it is usually associated with a smouldering clinical course due to the effects of chronic hypercalcaemia. In contrast to it, malignancy-related hypercalcaemia (often seen in advanced stage of malignant disease) and parathyroid carcinoma are associated with life-threatening severe hypercalcaemia and carry a poor prognosis. 1 However, in rare instances, hypercalcaemic crisis may be the sole presenting feature of PHPT and may pose a diagnostic dilemma. Severe hypercalcaemia is a life-threatening entity and is often accompanied by various degree of renal dysfunction. Management of such cases is therefore challenging and necessitates prompt therapy. The role and utility of denosumab therapy in such scenarios holds good promise. We describe the clinical presentation of an interesting case of PHPT presenting with acute severe hypercalcaemia as the index presentation and also describe utility of denosumab therapy.
Case report
A 53-year-old male patient presented with symptoms of nausea, vomiting and constipation for last 2 weeks. There was no history of abdominal pain, renal stones, pancreatitis, kidney disease, gall stone disease, bony fractures and peptic ulcer disease in past. The patient was diagnosed with type 2 diabetes mellitus for last 2 years and was continuing tablet glimepiride 1 mg and metformin 1,000 mg/day. On evaluation, the patient was conscious and cooperative. He appeared dehydrated and lethargic. His vitals at presentation were fairly stable. Evaluation of chest, cardiovascular and abdominal system was grossly normal. He underwent abdominal and pelvic ultrasonography and upper gastrointestinal endoscopy. Significant positive findings from imaging included features of acute kidney injury. Blood investigations revealed presence of severe hypercalcemia (serum calcium level – 5.11 mmol/L) and elevated serum creatinine levels (274 µmol/L). The relevant blood investigations have been summarised in Table 1.
Summary of important blood investigations of our index case.
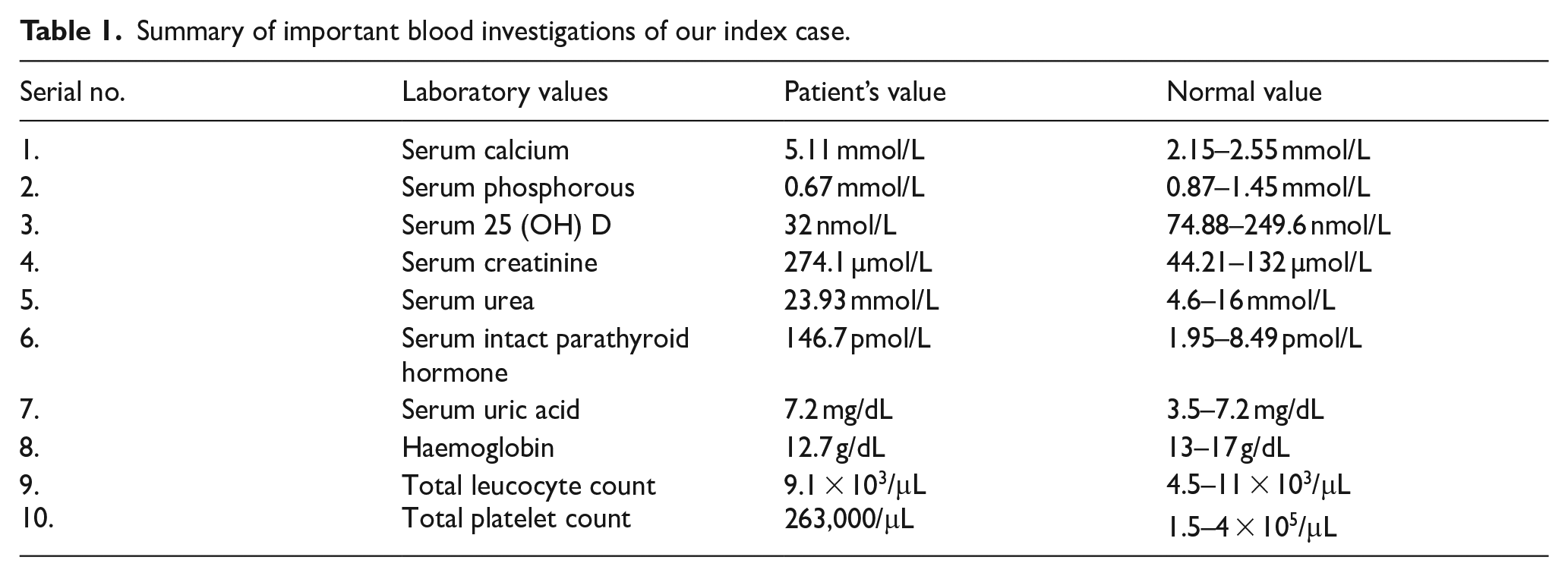
A review of past medical records showed normal serum creatinine level (79.58 µmol/L) assessed 2 months ago. A detailed work up for cause of underlying hypercalcaemia was done. Serum parathyroid hormone (PTH) levels were found to be significantly elevated (146.7 pmol/L). Based on above clinical and supportive biochemical findings, a presumptive diagnosis of PHPT induced severe hypercalcaemia with acute kidney injury was made.
The patient was initially started with intravenous normal saline rehydration followed by diuretic therapy (intravenous furosemide 20 mg was given two times daily) and subcutaneous calcitonin administration. However, no significant response was seen after 24 h. In view of his deteriorating renal function and severe hypercalcaemia, immediate haemodialysis was planned in consultation with nephrologist. Despite three sessions of haemodialysis, his serum calcium and creatinine levels reduced to 4.42 mmol/L and 185 µmol/L, respectively. Owing to refractory and persistent hypercalcaemia along with deranged renal status, injection denosumab (60 mg subcutaneous) was administered to him (received 3 days after admission). Subcutaneous insulin therapy was initiated for control of glycaemic status. Following administration of denosumab, serum calcium levels showed a declining trend and it came down to 2.69 mmol/L (by end of third day after denosumab). Ultrasonography of neck revealed a large mildly lobulated, well encapsulated and homogenously hypoechoic lesion of size 2.8 × 1.0 cm2. The lesion was located posterior to the lower pole of the right lobe of thyroid gland and showed presence of internal vascularity (Figure 1). This lesion was highly suggestive of right inferior parathyroid adenoma. Furthermore, parathyroid scintigraphy showed focal abnormal persistent tracer localisation in the inferior aspect of the lower pole of right lobe of thyroid gland. The above said finding was indicative of right inferior parathyroid adenoma (Figure 2). Dual Energy X ray Absorptiometry ( DXA) scan revealed normal bone mass with T score of −0.6 at lumbar vertebrae, T score of −0.6 at neck of femur and T score of −1.0 at distal radius. After stabilisation of his clinical status, he underwent successful focused parathyroidectomy with rapid improvement in clinical parameters. Serum PTH level declined to 0.56 pmol/L. Serum creatinine levels returned to normal (124.6 µmol/L) on postoperative day four. Following surgery, serum calcium level dropped to 1.99 mmol/L. He was initially managed with intravenous calcium supplementation in early postoperative period followed by oral calcium and calcitriol supplementation (elemental calcium 1500 mg and calcitriol 0.75 mcg in divided doses) to achieve normocalcaemia. The histopathological evaluation of excised tumour confirmed presence of parathyroid adenoma. The patient is on periodic follow up for last 1 year and currently remains normocalcaemic.
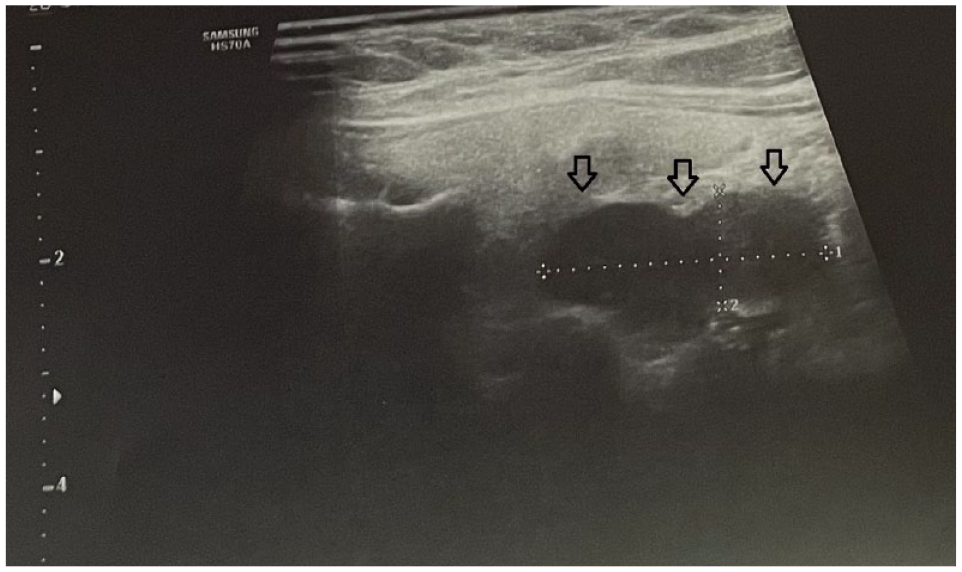
Ultrasonography of neck showing homogenous and well-encapsulated hypoechoic lesion (black arrow) located posterior to lower pole of right lobe of thyroid with internal vascularity measuring around 2.8 × 1.0 cm2.
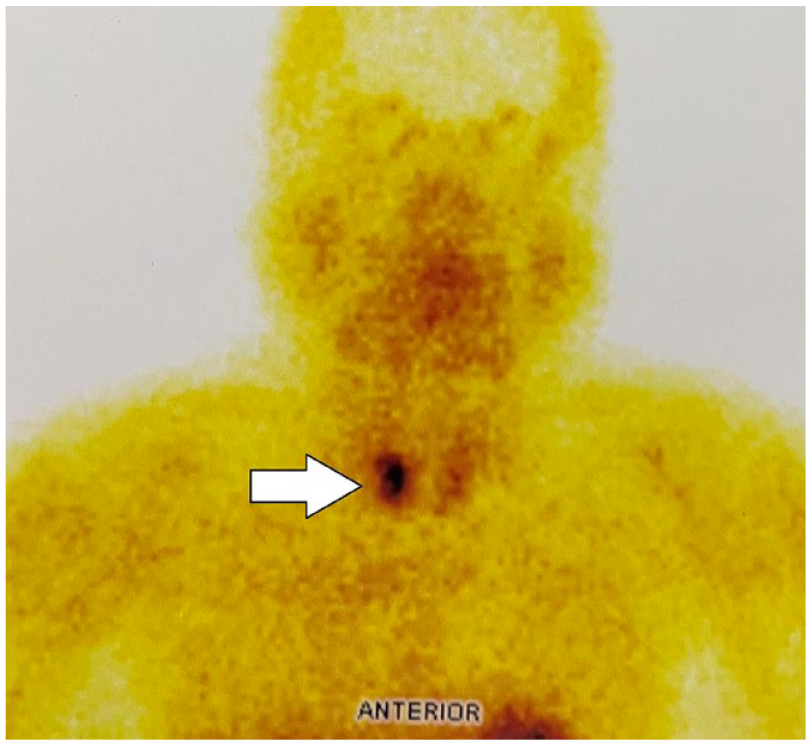
Tc-99m sestamibi parathyroid scan showing abnormal focal tracer localisation in inferior aspect of lower pole of right lobe of thyroid gland suggestive of right inferior parathyroid adenoma (white arrow).
Discussion
Hypercalcaemia is one of the most common electrolyte abnormalities seen in clinical practice especially in emergency and intensive care services. Severe hypercalcaemia (serum calcium level >14 mg/dL) is usually symptomatic and represents a medical emergency. Aggressive treatment in such cases is mandatory (irrespective of symptomatology) as severe hypercalcaemia is associated with multi-organ dysfunction. 2 The underlying aetiology in majority of these cases is either malignancy-associated hypercalcaemia or PHPT. Together, they account for around 90% of all hypercalcaemic patients. Humoral hypercalcaemia of malignancy is most commonly associated with solid tumours and generally has a more acute presentation with severe hypercalcaemia. Manifestations of acute hypercalcaemia can be gastrointestinal (nausea and vomiting), renal (polyuria and polydipsia), neuromuscular (depression, confusion, stupor and coma) and cardiac (bradycardia or heart block). Chronic hypercalcaemia may present with dyspepsia, pancreatitis, nephrolithiasis/nephrocalcinosis, hypertension and neuromuscular weakness. By the time hypercalcaemia is detected in these patients, the diagnosis of malignancy is often apparent.
On the other hand, PHPT is the leading cause of incidentally detected hypercalcaemia in asymptomatic individuals. It is characterised by mild-to-moderate degree of hypercalcaemia along with elevated PTH levels. 3 It is worthwhile to remember that PTH levels may be inappropriately normal (that is not appropriately suppressed in view of prevalent hypercalcaemia). 3 Clinical manifestations for this disorder have evolved from severely symptomatic disease (in resource poor healthcare settings) to asymptomatic disease (in developed countries). Normocalcaemic PHPT is also identified during evaluation of patients with osteopenia or osteoporosis in affluent setting. 4 Symptomatic patients often have bone pain due to fractures or colicky abdominal pain due to renal stones. Severe neurological or neuromuscular symptoms are very rarely seen in PHPT, except in cases of large adenomas or carcinomas. However, an Indian study revealed incidence of hyperparathyroidism induced hypercalcaemic crisis to be 21%. 5 This could be due to the fact that diagnosis may be often delayed leading to presentation with more severe symptomatic disease.
Severe hypercalacemia or hypercalcaemic crisis requires urgent management in order to prevent mortality. 2 Surgical management is the definitive approach for PHPT. In case of hypercalcaemic crisis, patients are usually dehydrated and require immediate hydration with saline infusion (after assessing the cardiac and renal status). Medical management for hypercalcaemia includes use of loop diuretics (after hydration), bisphosphonates, denosumab, calcitonin, cinacalcet, corticosteroids and haemodialysis depending on the prevailing clinical condition. These agents are often used as a bridge therapy in cases of PHPT before a curative surgery is undertaken. Less frequently, few of these agents may be tried as chronic palliative therapy especially in cases where surgery cannot be undertaken or is not curative. Bisphosphonates are very effective in lowering calcium levels in cases of malignancy although their efficacy for the same in PHPT is not consistent. In addition, bisphosphonates are also contraindicated in acutely ill patients with renal failure. Haemodialysis is the preferred modality in cases of severe hypercalcaemia with renal compromise. However, surprisingly our index patient underwent three sessions of haemodialysis but the serum calcium levels did not improve significantly. In such clinical settings, denosumab can be used as a bridge therapy before eventual surgery. Denosumab is a monoclonal antibody binding to the RANK ligand (RANKL) which inactivates the osteoclastic bone resorption and is helpful in lowering the serum calcium levels. It is particularly useful in the setting of severe renal disease where bisphosphonates cannot be used. Denosumab can be safely administered in case of renal dysfunction. In our case, the serum calcium levels normalised after 3 days of denosumab therapy. We have summarised all reported cases describing utility of denosumab therapy in PHPT associated hypercalcaemia (Table 2).
Summary of clinical and biochemical findings in cases where denosumab therapy has been tried for hypercalcaemia management.
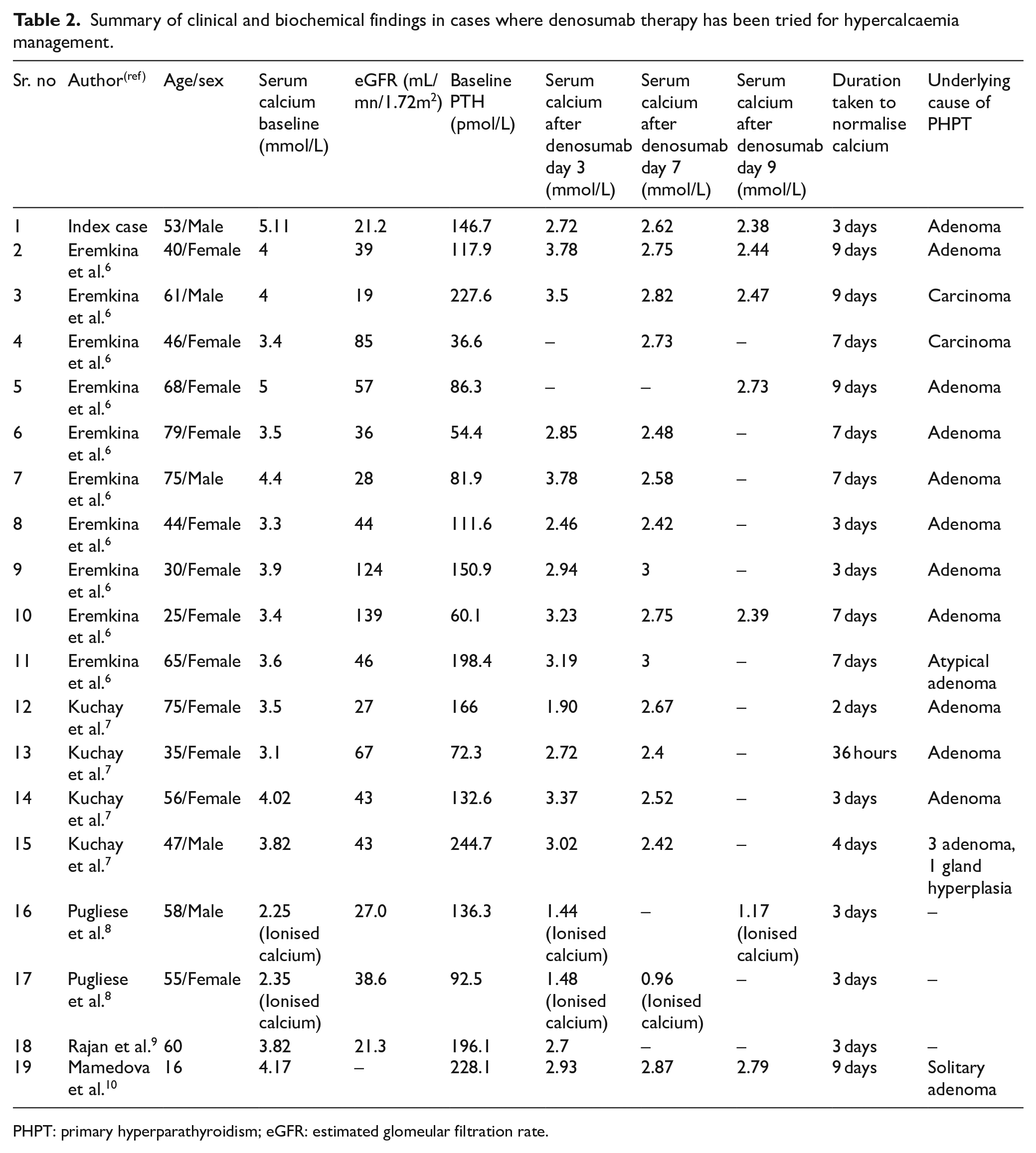
PHPT: primary hyperparathyroidism; eGFR: estimated glomeular filtration rate.
The reported duration to lower serum calcium levels in various studies also averaged around 3vdays6–9 or even earlier around 36 h after denosumab administration. 10 The patients should be meticulously observed for the occurrence of post-operative hypocalcaemia. Thus, denosumab can be used successfully for management of hyperparathyroidism (due to parathyroid adenoma) induced hypercalcemia in addition to its approved use in the setting of hypercalcaemia of malignancy, especially in cases of refractory hypercalcaemia.
Conclusion
Hypercalcaemic crisis may be rarely a presenting feature of PHPT. Hypercalcaemic crisis is often accompanied by renal dysfunction and can be challenging to manage. In such scenarios, denosumab therapy can play a critical role in managing such patients especially when other therapeutic modalities cannot adequately control hypercalcaemia. Hence, denosumab may act as a beneficial bridging therapy in such patients till curative surgery can be performed.
Footnotes
Authors’ note
This case study was presented as poster presentation at ENDO 2022.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent for the paper to be published (including images, case history and data) was obtained from the patient for publication of this paper, including accompanying images.