
Abstract

Keywords
My consultant colleague spent all afternoon in the back of an ambulance outside the Emergency Department (ED). Fortunately, she was not in need of medical attention, but the people in the ambulance were. Her task was to identify if anyone waiting in an ambulance could have their care delivered by the hospital at home team instead. By this point, the horse has typically bolted, but she was able to reassure patients and listen to and calm relatives who were anxious, angry and tired.
There were patients in the hospital who would go home that evening, but they hadn’t been discharged yet. It might be 6 pm when their medicines arrive from pharmacy, or 7 pm when their daughter finishes work, or 10 pm when the transport arrives; and then the bed will need to be cleaned before it is ready to use. There is a mismatch between the peak rate of discharge and the peak rate of arrival. If only the hospital could discharge patients in the morning, then beds would be available when needed, resulting in fewer ambulances ‘stacking’ outside.
Before I consider how we could achieve the elusive morning discharge, we must first ask: is discharge before noon (DBN) the solution to the bed and flow crisis? If we want to focus on DBN, then there is one easy, but damaging, solution . . . we keep people in hospital for one more night so that the discharge can occur the following morning. This only serves to increase length of stay (LOS) and reduce flow – precisely the opposite of what we want to achieve.
There is mixed evidence on the benefits of DBN. 1 Advocates of DBN include Wertheimer.2,3 Their group managed to increase DBN from 11 to 38%. 2 They took a whole team approach with education, launch events, feedback and celebration of success. They argue that DBN is achievable and effective and reduced LOS. Shine 4 has questioned the results of Wertheimer,2 stating that there were other initiatives during the study period which influenced positive results, for example, an increase in social care and medical input at weekends.
Others have found that DBN increases LOS for medical admissions.5,6 A large and recent multicentre study of DBN by Kirubarajan et al. 7 looked at 189,781 general internal medical (GIM) admissions in seven hospitals in Canada. Nineteen percent of discharges occurred between 8 am and 12 pm. They found that DBN was not associated with LOS in the ED – that is, patients in the ED requiring a GIM bed did not access one more quickly. There was also no significant association between DBN and GIM LOS. 7
There are some important issues with Kirubarajan et al.’s 7 study which are worth highlighting. Firstly, the study period was 7 years. I would be expecting radical changes in the way that care, and discharge, is delivered during that period, for example, through quality improvement initiatives. The median ED LOS was 14.5 h. 7 While ironically Wertheimer et al. 2 have been criticised4 for implementing other initiatives during their study, what else should the hospitals in Kirubarajan et al.’s 7 study have been doing to reduce LOS during the study period? Secondly, the average number of discharges per day per large hospital was only eight. 7 I work in a 25-bedded frailty ward which is routinely expected to discharge eight patients per day.
So, should we be focusing our efforts on morning discharges? There are benefits to patients who go home in the morning: energy levels are higher and there is more time to settle in and adjust before bedtime. But we also want to increase flow and reduce LOS for two reasons:
to help meet the increasing demand on hospital beds and
to reduce hospital associated harms, for example, delirium, immobility, pressure wounds, falls, deconditioning and loss of independence, which all lead to further increases in LOS – a vicious circle!
Many of the solutions to timely and person-centred discharge are not new. There are some excellent guidelines including ‘The Daily Dynamic Discharge Approach’ 8 and NHS Improvement’s ‘SAFER patient flow bundle’, 9 from 2016 and 2018, respectively. Many of the recommendations in these reports are now embedded widely, such as board rounds and setting a discharge date. But I wonder if we get ‘initiative fatigue’ as postulated by the Red Cross in their report, ‘Home to the unknown: Getting hospital discharge right’. 10 Or the quality improvement project that showed the benefit of discharge rounds on hospital departure times, but then returned to pre-implementation levels in the subsequent 2 months. 11
When considering how we improve timely discharge, it can be useful to consider two groups – short-stay and longer stay admissions. 12 Although this is an arbitrary distinction, and there are some shared solutions, I think that the problems and solutions for each group are different. The 2016 Nuffield Trust report showed that 90% of patients spend ⩽6 days in hospital, with an average LOS of 1.1 days; whereas 10% of patients spend >7 days in hospital and account for 65% of bed days. 11
For short-stay admissions, the priority need not be morning discharge. If someone is fit for discharge at 11 pm and has the desire and means to get home safely, then postponing discharge until 9 am does not benefit anyone. For people who spend a short while in hospital, say 26 h, then it’s all about processes: early access to a senior decision maker, laboratory results, portering, radiology and domestic services. If a blood result is delayed by 2 h, then LOS will increase by nearly 8%. Every minute counts and it requires a whole team approach. Minutes could be saved with, for example, point of care testing and ultrasound, rapid access to other investigations and over-labelled medications. Some short-stay admissions could be avoided entirely with a rise in ambulatory clinics and same day emergency care (SDEC).
For longer stay admissions, if we can reduce LOS, we could have radical reductions in overall bed utilisation. And these are also the people who are most likely to benefit from a planned, morning discharge. Table 1 details some of the areas I think we should focus on to achieve timely discharge in this group.
Potential solutions to achieve timely discharge in longer stay admissions.
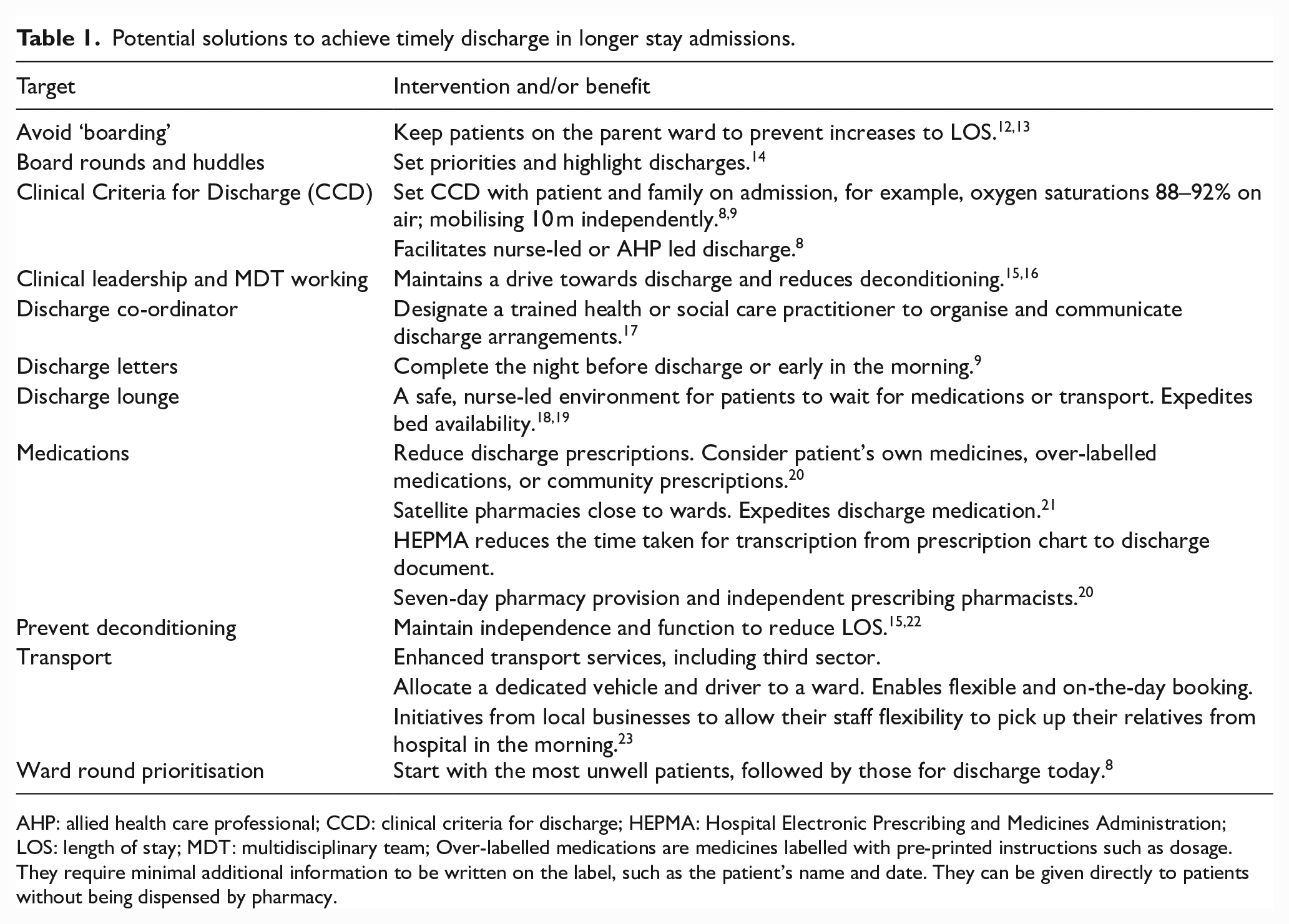
AHP: allied health care professional; CCD: clinical criteria for discharge; HEPMA: Hospital Electronic Prescribing and Medicines Administration; LOS: length of stay; MDT: multidisciplinary team; Over-labelled medications are medicines labelled with pre-printed instructions such as dosage. They require minimal additional information to be written on the label, such as the patient’s name and date. They can be given directly to patients without being dispensed by pharmacy.
In summary, I’d like to share a quote from Zorian: ‘instead of focusing on a particular hour, initiatives should determine the best, earliest discharge time for each patient and align multidisciplinary efforts toward this person-centred goal’. 24 I believe that a key solution sits at the start of the admission, in establishing and sharing individualised clinical criteria for discharge. If we don’t know (and document) what we need to do to get someone home, how will we ever achieve it? And DBN would be a good thing as long as it happens yesterday or today – not tomorrow!
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.