
Abstract
Background:
Influenza vaccination will have added importance this winter given the possibility of further waves of the COVID-19 pandemic. This study examines the impact of an electronic medical record (EMR) reminder on influenza vaccine uptake among eligible hospital inpatients.
Methods:
We included a convenience sample of 750 adults (median age 77 years) who are eligible for influenza vaccination (⩾65 years and/or length of stay >30 days). A live electronic dashboard identified patients eligible for vaccination, prompting reminders sent to the clinical teams via the EMR.
Results:
The EMR reminder was associated with almost a 50% higher likelihood of vaccination after adjusting for other covariates (odds ratio 1.48 (95% confidence interval 1.00–2.20); p = 0.048).
Discussion:
Reminders sent to the clinical team via the EMR appear to be an effective means of increasing vaccine uptake and should be considered as part of this year’s drive to vaccinate eligible patients in hospital.
Background
Influenza remains an important cause of morbidity and mortality among older persons. 1 Over a 30-year period in the United States, approximately 90% of deaths due to influenza occurred in adults aged 65 years or older. 2
Annual vaccination against influenza remains the single best public heath measure available to prevent morbidity and mortality 3 and the World Health Organization emphasises that influenza vaccination programmes should target high-risk groups such as adults aged 65 years and older. 4 As well as being an efficacious tool in preventative medicine for older adults, influenza vaccination has been shown to be cost-effective in this population. 5 The added importance of efforts to reduce circulating levels of seasonal influenza has been highlighted by the COVID-19 pandemic. 6
Influenza vaccination, particularly for vulnerable, older people, will have added importance this winter given the possibility of further waves of the COVID-19 pandemic. 7 Strategies to improve vaccination rates are therefore desirable. While hospital-based interventions in this regard have been shown to be successful, 8 there remains a need for organisational or system-based interventions to increase vaccination uptake. A previous intervention at the study site targeting inpatient influenza vaccination utilised a once-off email-based reminder but on re-audit the influenza vaccination rates for eligible inpatients remained low at 19%. 9
The electronic medical record (EMR) is an ideal model for delivering reminders regarding vaccinations to clinical teams. 10 This study therefore examines the impact of an EMR reminder on influenza vaccine uptake among eligible hospital inpatients.
Methods
Study design
This study examines the impact of an EMR reminder on influenza vaccination rates in a 900-bed university teaching hospital during the influenza season from 1 October 2020 to 12 January 2021. Inpatients were deemed eligible for the intervention if they were aged ⩾65 years and/or had a length of stay (LOS) greater than 30 days.
Intervention
The EMR was utilised to identify patients eligible for the intervention. All eligible inpatients (i.e. any inpatient aged above 65 years and/or admitted 30 days or more to hospital) populated a live electronic dashboard throughout the influenza season. The electronic dashboard was managed by the hospital antimicrobial pharmacist facilitating the generation of clinically relevant email-based reminder prompts to physicians to vaccinate eligible inpatients. Email-based reminders regarding vaccination were completed following review of the inpatient’s clinical notes in the EMR by the antimicrobial pharmacist. This facilitated generation of reminders that had clear clinical context. For instance, if a clinically appropriate reason against vaccination was documented on the inpatient’s notes, then a reminder on influenza vaccination was not generated. Email-based reminders were also supported by standardised pharmacist documentation within the inpatient’s EMR to highlight eligibility for influenza vaccination.
Influenza vaccination history was by self-report. In cases where the patient could not self-report vaccination history, informant history on vaccination status and contact with community general practitioner was completed.
The EMR data enabled automatic rules to update the electronic dashboard and avoid duplication of vaccination within the same influenza season. These rules included the automatic removal of the inpatient from the dashboard once the influenza vaccine was administered on the electronic drug chart. Furthermore, a dropdown field captured vaccination status at the point of admission. If vaccination was indicated as complete, the patient did not populate the dashboard. Clinical governance for the intervention was assigned to a specific Hospital Outbreak Committee of which the antimicrobial pharmacist was a member as well as clinical leads for Medicine, Infectious Diseases and Clinical Microbiology.
Statistical methods
Data were collected retrospectively on a convenience sample of 750 consecutive inpatients during the period of 1 October 2020 to 12 January 2021.
Baseline characteristics of the study sample were analysed descriptively. Logistic regression models with influenza vaccination as the dependant variable, reporting odds ratios with 95% confidence intervals, were used to assess the independent association of the EPR reminder with vaccination status. Covariates were identified a priori based on their likelihood of influencing vaccination rates.
Results
In all, 750 patients were included with a median age of 77 years (95% confidence interval (CI) 76–78); 48% were female. The median LOS was 35 days (95% CI 33–37).
Over 37% of patients were admitted under the care of geriatric medicine (279/750), a further one-third (260/750) were under the care of internal medicine; one-quarter were under the care of a surgical team (180/750), while the remainder (31/750) were under the care of psychiatry.
Over one-third (35%, 264/750) of patients received the influenza vaccine while in hospital, including 40% aged ⩾80 years (see Figure 1).
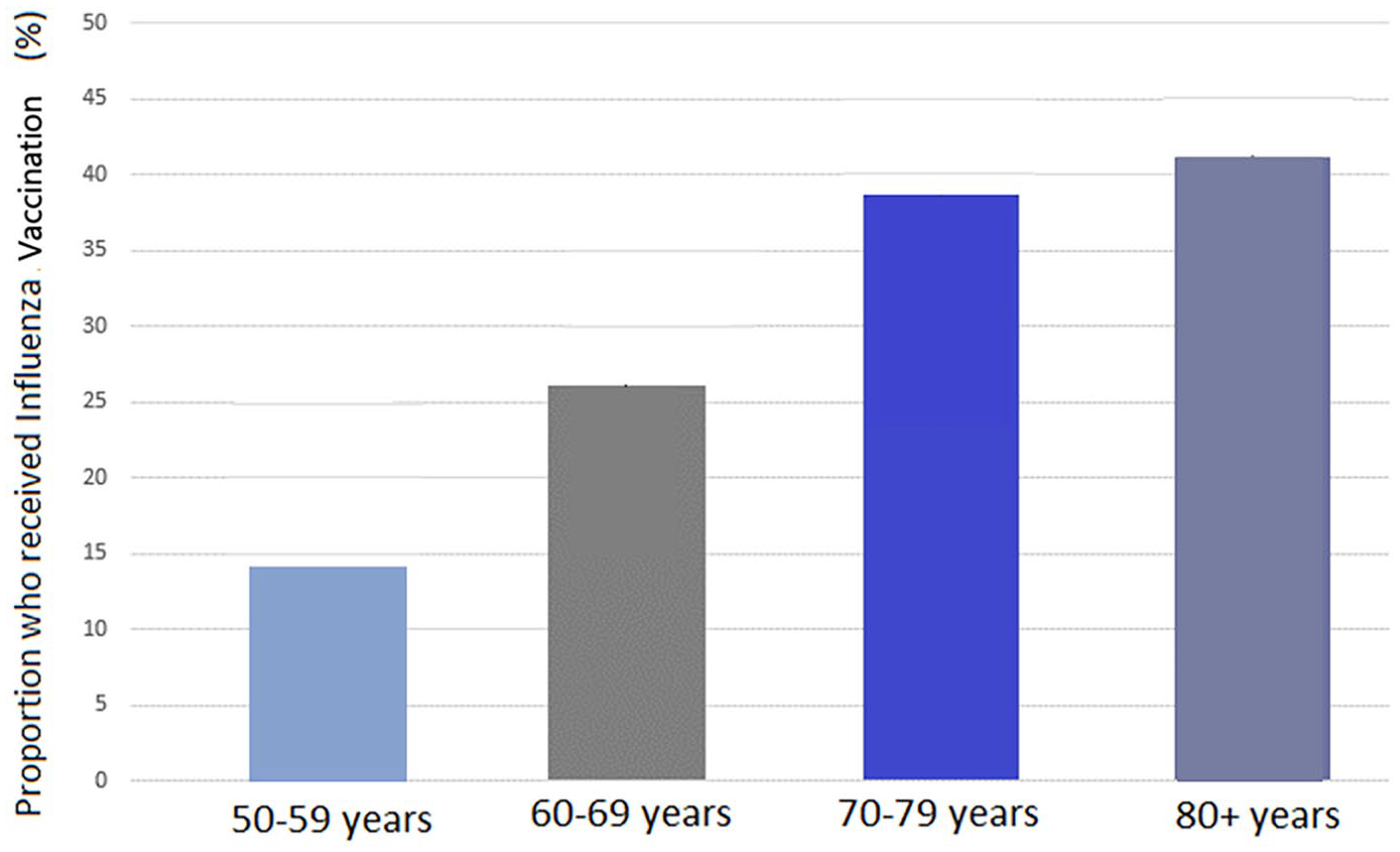
Proportion of patients vaccinated by age category.
An EMR reminder was sent on 41% (305/750) of patients. Logistic regression models demonstrated that this was associated with a significantly higher likelihood of vaccination after adjusting for other covariates (odds ratio 1.48 (95% CI 1.00–2.20); p = 0.048) (see Table 1).
Logistic regression model with influenza vaccination as dependent variable.
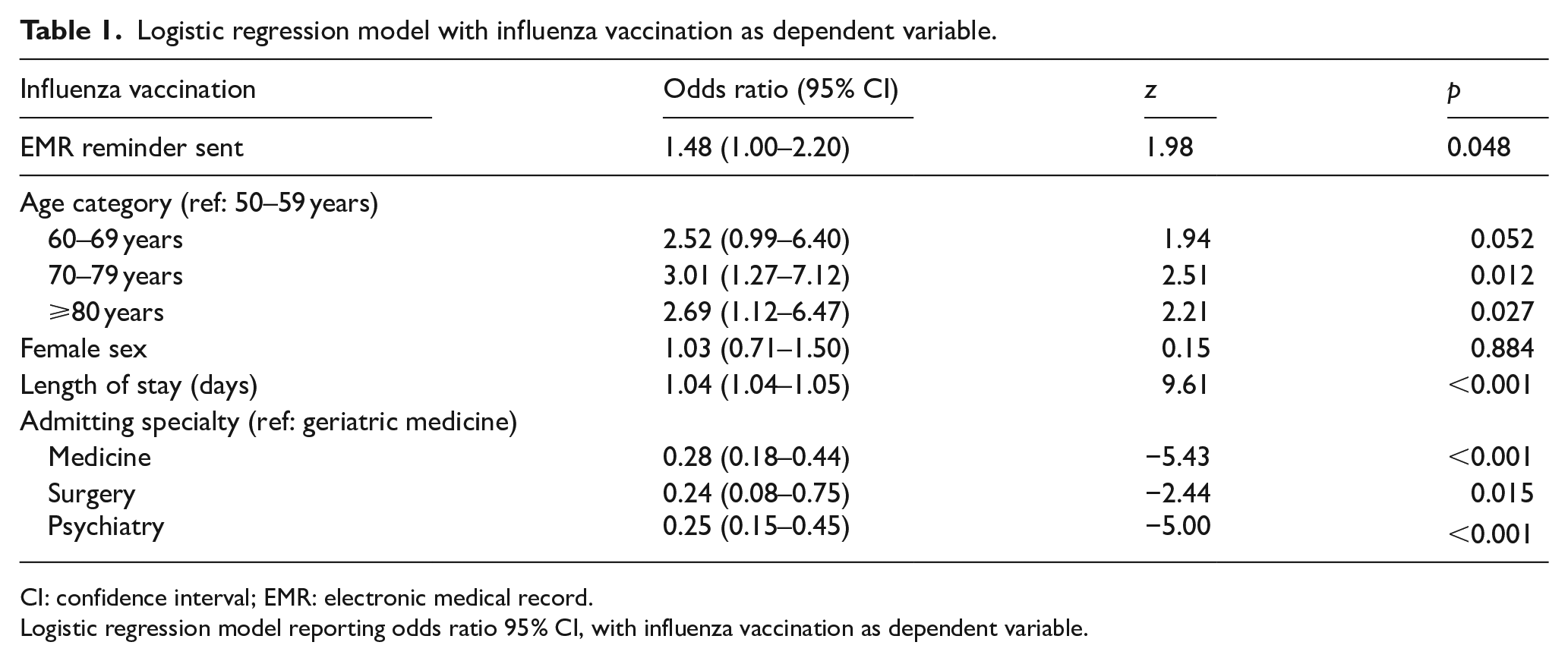
CI: confidence interval; EMR: electronic medical record.
Logistic regression model reporting odds ratio 95% CI, with influenza vaccination as dependent variable.
Other factors independently associated with vaccination were advancing age (odds ratio 2.69 (95% CI 1.12–6.47) for age⩾80 years); increasing LOS (4% higher likelihood of vaccination for every additional day in hospital) and admission under geriatric medicine (odds ratio 3.71 (95% CI 2.45–5.62) when compared to other specialities).
Discussion
This study examined the impact of an EMR-based reminder on influenza vaccination rates among older patients in hospital. We found that the EMR reminder was independently associated with a 50% higher likelihood of vaccination.
Prior studies have shown the benefit of targeted interventions to improve opportunistic influenza vaccination in hospital. 6 These have involved pharmacist-led interventions, 11 an electronic alert system 12 and the provider-level strategies. 7 The intervention in this study is different as it incorporates EMR data within an electronic dashboard to facilitate pharmacist-led review of each clinical step in the vaccination workflow, specifically identification of high-risk inpatients, consent, prescription and administration. It also enables clinically relevant reminders to be targeted at the physician responsible for the current inpatient stay.
It must be noted however that despite the impact of the EMR reminder, the overall inpatient influenza vaccination rate remained low, with only 40% of eligible patients aged ⩾70 years vaccinated in hospital. Several possible reasons have been proposed for generally low influenza vaccine uptake among older people, including demographic and socio-economic factors, as well as other health determinants.13,14 The dynamic and changing clinical environment of an acute hospital may further impact uptake.
In our study, admission under a specialist geriatric medicine service conferred a higher likelihood of vaccination. This is perhaps not surprising when we consider that the greatest benefit of vaccination is likely to be derived by older people with higher levels of frailty and chronic disease, many of whom would be expected to be under the care of geriatric medicine. 15 Furthermore, assessment of vaccination status is likely to form part of the structured comprehensive geriatric assessment. 16 Unsurprisingly, other factors associated with higher vaccination rates were advancing age and longer LOS.
There are some limitations to this study which should be noted. This EMR-based intervention did not involve other potentially important strategies to improve vaccination rates including patient and physician education. Other EMR-based strategies were also not employed including EMR alerts presented to physicians or the use of standing orders. Alert fatigue is acknowledged as a significant challenge within EMR systems.17,18 Our intervention specifically avoided alerts especially interruptive alerts to physician end users to avoid associated alert fatigue. Standing orders are vaccine prescriptions which are automatically produced by the EMR system. They have been shown to be more effective than computerised reminders to physicians for increasing influenza vaccination. 19 Standing orders may represent a future approach for the next iteration of the audit cycle for inpatient influenza vaccination in our site. Secondly, this intervention was conducted as an iteration of the existing hospital audit cycle targeting inpatient influenza vaccination. A control group was not employed and all inpatients deemed eligible for influenza vaccination were included in the intervention to ensure that the maximal inpatient population benefited from the intervention. Additionally, data were not collected on reasons for not vaccinating patients, including refusal, pre-admission community vaccination, contraindications such as active infection. In particular, information regarding vaccination in the community was often not available at the point of admission. These patients met eligibility criteria and populated the dashboard. However, information later gathered from community sources revealed vaccination had been completed already during that influenza season. These patients did not trigger a reminder nor did they get vaccinated which was clinically appropriate. This may be a point for future consideration as COVID-19 vaccination cycles including booster vaccinations will add further complexity when relying on patient-based recall. Strengths of the study include the novel electronic-based system being studied and the robust analysis of association with vaccination status.
In conclusion, we have demonstrated that an EMR reminder system is independently associated with a 50% increase in opportunistic influenza vaccination among older patients. EMR reminders should therefore be considered as part of this year’s drive to vaccinate eligible patients in hospital, but given low vaccination rates overall, may need to be used as part of a multimodal strategy including patient and physician education.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Hospital Outbreak Committee at St James’s Hospital.
Ethical approval
Governance of this clinical intervention was under the remit of the Hospital Outbreak Committee within St James’s Hospital. It formed part of the hospital clinical audit cycle to increase uptake of inpatient influenza vaccination. Given that it falls under the remit of clinical audit/service evaluation, it was approved by the Research and Innovation Office at St James’s Hospital which has oversight of hospital-based research activity.