
Abstract
Background:
The British Thoracic Society recommend that pulmonary embolism (PE) patients with low-risk Pulmonary Embolism Severity Index (PESI) scores are considered for outpatient (OP) management, in settings where robust pathways for follow-up and monitoring exist.
Methods:
Retrospective cohort study. We reviewed the electronic records of 109 consecutive PE patients considered appropriate for OP management. Primary outcomes were the incidence of recurrent venous thromboembolism, major bleeding, mortality at 1 year and evidence of chronic thromboembolic pulmonary hypertension (CTEPH).
Results:
Low-risk PESI scores (I–II) were recorded in 78 (72%) patients, with higher scores a consequence of age and comorbidity rather than haemodynamic instability. There was a low rate of adverse outcomes despite a lack of formal follow up for most patients. There was no evidence of CTEPH in 34 patients who underwent echocardiography.
Conclusion:
Our analysis challenges the need for robust follow-up pathways for all patients with pulmonary embolism.
Keywords
Introduction
Pulmonary embolism (PE) is a potentially life-threatening condition and a leading cause of morbidity and mortality worldwide. 1 Over 69,064 hospital episodes of PE were reported in the UK between 2021 and 2022, resulting in 36,757 admissions. 2 While traditionally managed as inpatients, the move from warfarin to direct acting oral anticoagulants in recent years 3 has prompted a paradigm shift towards outpatient (OP) care.
The British Thoracic Society (BTS) recommends that patients with a confirmed diagnosis of PE are risk stratified using a validated clinical tool such as the Pulmonary Embolism Severity Index (PESI) score, with those designated low-risk considered for OP management. 4 PESI takes into account the patient’s age, gender, history of cancer, heart failure or chronic lung disease, respiratory rate, heart rate, systolic blood pressure, temperature, oxygen saturations and mental state to assign the patient a risk category from I to V. Furthermore, the BTS recommends that for suitable patients, OP follow-up should be offered in a setting where robust pathways for monitoring exist. Specifically, it is recommended that patients have a formal review (either telephone or face to face) within the first week after discharge to assess for the presence of complications and check therapeutic compliance. Additionally, it is proposed that hospitals should have local pathways for the assessment of ongoing symptoms, with further directed investigations if appropriate, and consideration of the duration of anticoagulation. Ideally this follow-up should be performed by clinicians with a special interest in venous thromboembolism (VTE). 4
NICE guidelines are broadly similar. 5 People aged 18 and over having OP treatment for suspected or confirmed low-risk PE should have an agreed plan for monitoring and follow-up. They should be given an anticoagulant alert card that they should carry at all times; written information on symptoms and signs to look for, including the potential complications of thrombosis and of treatment; direct contact details of a healthcare professional or team with expertise in thrombosis who can discuss any new symptoms or signs, or other concerns; and information about out-of-hours services they can contact when their healthcare team is not available. 5
The European Society of Cardiology (ESC) also recommend OP management for low-risk patients who have a PE, 6 but go further than the BTS and NICE in recommendations for optimal follow-up. The ESC advocates a holistic approach covering a spectrum of serious adverse events and challenges that patients with PE may encounter at four distinct time points: at diagnosis, in the first weeks, at 3 months and in the long term. These include cancer screening, thrombophilia screening, advice on returning to sport, lifestyle and travel, cardiovascular risk management and detection of post PE-syndromes including chronic thromboembolic pulmonary hypertension (CTEPH). 7
Against this background, the aim of the current study was to assess the outcomes of patients managed in a health board where robust pathways for follow-up have not existed.
Methods
This was a retrospective cohort study of patients presenting to Dumfries and Galloway Royal Infirmary and the Galloway Community Hospital in south-west Scotland. We searched the electronic patient record for patients who had undergone CT pulmonary angiography (CTPA) between January 2014 and December 2021. This enabled us to identify a consecutive series of patients with PE who were managed as OPs, following first review by a senior decision maker. None of these had chronic kidney disease stage 4/5 or severe liver disease.
We used the pulmonary embolism severity index (PESI) to categorise patients from class I (very low risk of morbidity and mortality) to class V (very high risk of morbidity and mortality). PESI scores were derived from each patient’s known co-morbidities together with the initial set of observations obtained on presentation to the medical assessment unit/emergency department. We accessed clinic letters, general practitioner coded diagnoses and imaging reports to determine adverse outcomes in the period from the index PE to present. Primary outcomes were recurrent PE, anticoagulant related major bleeding, evidence of CTEPH and all-cause mortality at 1 year.
Our study was conducted to define and measure current care and involved routine interventions already in common use. We did not randomize or allocate patients to treatment groups. Our study met the criteria for service evaluation and therefore we did not seek approval from our Research Ethics Committee, in keeping with our health board policy.
Results
We identified 4384 CTPA scans between January 2014 and December 2021. Of these, 848 (19%) were positive for PE, 121 (14%) of which were managed as OPs. We excluded eight patients due to incomplete medical records. Four patients had two CTPAs leaving a total of 109 patients for analysis. The average age of the cohort was 59 years, with age range 20–93 years, and 51% were female. Patients were followed for a minimum of 2 years and an average of 4 years. Although some patients within the cohort had been diagnosed with an earlier PE, our analysis focused only on the presentation and outcomes of the PE that occurred between 2014 and 2021.
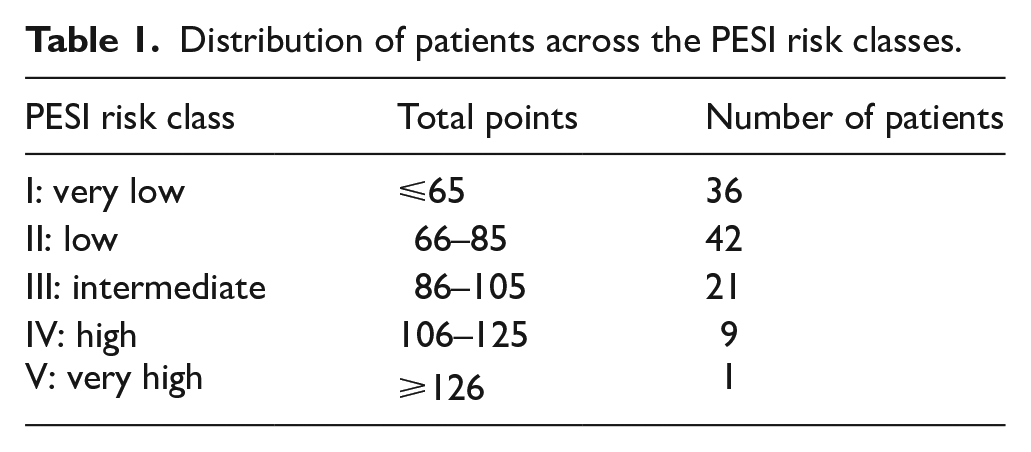
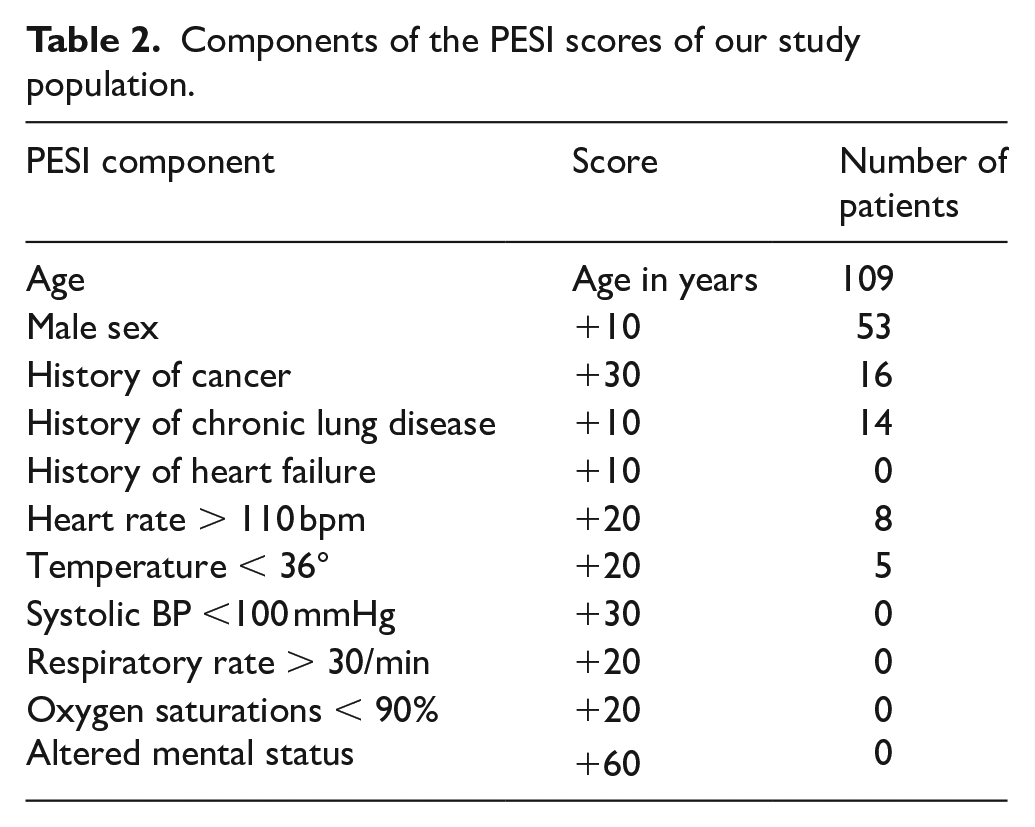
The distribution of patients across the PESI risk classes is shown in Table 1, while a breakdown of the components of their PESI scores can be seen in Table 2. Of note, none of the patients we judged fit enough to be managed as OPs had systolic BP <100 mmHg, respiratory rate >30/min, oxygen saturation <90% or altered mental status.
Distribution of patients across the PESI risk classes.
Components of the PESI scores of our study population.
Only 11 patients (10%) received some form of follow up in the first week following discharge. For five of these, this was for daily clotting screens or dalteparin injections. These patients had a set of observations and a discussion with a clinician during their attendance. Eight patients (7%) were seen in a respiratory, haematology or oncology clinic as a direct result of their PE diagnosis. No patients were reviewed at a dedicated PE or VTE clinic as these do not exist locally.
Recurrent VTE occurred in 9 (8%) patients by one year and 19 (17%) patients by 3 years. Seventeen of the 19 recurrences were PE and two were DVT. These occurred during treatment in three patients, two of whom were anti-coagulated with dalteparin and one with warfarin. Poor compliance was a factor in two of these patients. One patient had a cerebral haemorrhage while taking warfarin when his INR was 3.4. Six patients (5%) died in the 12 months following diagnosis of PE. All were known to have an active cancer diagnosis. There was no suggestion that the primary cause of death in these patients was PE or the associated complications of PE.
We requested echocardiography for 34 patients during follow-up. Requests were submitted by a range of specialties including cardiology, respiratory, acute medicine and general practice for various reasons, and not always because of the PE. The average length of time between the index PE and first echocardiography was 1.6 years. Only one of these showed evidence of pulmonary hypertension. This was a patient whose CTPA showed mild to moderate clot load on a background of diffuse centrilobular lung emphysema with peripheral bronchiectasis. This individual died 1 year later from end-stage COPD leading us to conclude he did not have CTEPH. The absence of features of CTEPH on the remaining 33 echocardiograms meant that no further directed investigations (ventilation perfusion scanning ± catheter-based pulmonary angiography) were requested.
Discussion
The main findings of our study were as follows: 14% of a consecutive series of PE cases were managed as OPs; PESI scores ranged from I to V with higher scores a consequence of age and comorbidity rather than haemodynamic instability; only 10% of patients had some form of contact with a healthcare professional in the first week and no patients were reviewed at a dedicated PE clinic; one patient had an anticoagulant related bleed and three patients had recurrent PE while on treatment; there was no evidence of CTEPH in the 34 patients who underwent echocardiography following their PE; and all six patients (5%) who died during the first year of follow-up had active cancer. None of the deaths were related to PE or to the complications of PE.
Our mortality data contrast with a 1 year case fatality of 29% in a large Canadian cohort of 33,447 PE cases, confirming that our patients were indeed a low-risk group. 8 Contrary to the conventional approach that emphasises structured and sometimes intensive follow-up, our results suggest that such rigorous monitoring may not always be necessary for ensuring favourable patient outcomes. This challenges existing paradigms and suggests a potential shift towards a more streamlined, resource-efficient management strategy for low-risk patients who have a PE. We should emphasise that our study was concerned only with those who were treated as OPs, a management approach made possible as a consequence of the switch from warfarin to direct acting oral anticoagulants such as apixaban, which avoids the time-consuming task of titrating warfarin. 9
Most of the patients in our study (72%) had PESI scores I–II. The PESI score was originally developed to predict 30-day mortality, but has since been used to identify low-risk patients. The BTS recommend patients with PESI scores I–II as suitable for OP management, and suggest that those with intermediate to high-risk PESI scores III–V be admitted to hospital. 4 It has also been shown that an improvement in PESI scores during the first 48 h of admission identifies patients with a very low risk of dying within the first month 10 though we did not examine this possibility in our study.
We did, however, manage 28% of patients who were PESI classes III–V as OPs. Higher PESI scores tended to reflect older age and the presence of co-morbidities rather than derangement of vital signs. All six patients who died within 1 year of their PE diagnosis were PESI class III–V, though none of these deaths were due to a pulmonary embolism or PE complications. Eight PESI class III–V patients were tachycardic at triage, but none were hypotensive and none had a high respiratory rate, oxygen requirement or altered mental status. We would therefore argue that despite the assigned PESI scores, our study population represented a low-risk group in terms of their clinical condition at the time of presentation. Reschen et al also found that clinicians place emphasis on vital signs when deciding on ambulation, 11 as did Lutsey et al who have shown that patients managed as OPs have fewer bleeding events and utilise less healthcare resources in the follow-up period, because a healthier population of patients are initially selected for OP management. 12
VTE recurred in 8% of our patients by 1 year and 17% patients by 3 years. These rates are in keeping with those quoted in the literature. The likelihood of recurrent VTE among 162 Austrian patients with symptomatic PE at 24 months was 19%. 13 Five-year cumulative incidence of recurrent VTE events in a series of 662 Korean patients diagnosed with PE was 22% for all cases of PE, 17% if provoked and 27% after unprovoked PE. 14 In a meta-analysis of 18 studies involving 7515 patients with a first unprovoked VTE, the risk of recurrent VTE after discontinuing anticoagulation was 10% in the first year, 16% at 2 years, 25% at 5 years, and 36% at 10 years. 15 Thus, a lack of structured follow-up does not appear to have been associated with a higher rate of VTE recurrence than expected in our patients.
Our finding that no patients were diagnosed with CTEPH fits with the low observed incidence (0.56%) seen in clinical practice 16 and challenges the recommendations of the ESC 7 and others 17 that early screening for CTEPH should be routine. The Sheffield group reported a CTEPH incidence of 2% when patients were followed up in a dedicated PE clinic, 17 leading Howard and Price to recommend structured follow-up for all PE. 18 However, only 59% of Sheffield patients diagnosed with PE were referred to their PE clinic 17 and no attempt was made to describe the CTEPH incidence in low-risk patients, namely those deemed fit enough not to be admitted to hospital. It seems likely to us that CTEPH would have been considerably less common in the 41% patients who did not attend the PE clinic. We are aware, incidentally, that persistent breathlessness following PE can occur in the absence of CTEPH, 19 an observation that may be a result, at least in part, of deconditioning.20,21 We do not have a local pathway in place to detect ongoing dyspnoea in Dumfries, but the fact that none of our low-risk patients were tachypnoeic or hypoxaemic at the time of diagnosis suggests that persistent breathlessness is unlikely to have been a problem in our study.
We feel it is worth considering the potential implications of our findings on healthcare systems. A relatively small percentage of our cohort (14%) were treated as OPs. The percentage of patients diagnosed with PE treated as OPs reported by others has varied from 4% 22 to 18%. 12 The Directory for Emergency Ambulatory Care suggests that between 60% and 90% of patients with a PE are potential candidates for OP management 23 which, if realised, would have a significant impact on resource allocation were ESC guidelines to be followed. Although the results from a large cohort study in Germany suggest that ambulatory post-PE care is only a minor contributor to the overall chronic costs following diagnosis, 24 we would suggest that the potential gains from the structured follow-up model of care would be minimal for low-risk patients with a PE and therefore that this may not represent the most efficient use of resources. We are not alone in taking this view. A recent paper, with a design similar to ours, explored post-PE follow-up at a large Australian regional city hospital health service. Agwan and colleagues reported a very low incidence of CTEPH along with a small risk of acute PE recurrence, and concluded that in certain circumstances, for example, patients with a first-episode PE that is low risk, provoked and lacking CTEPH risk factors, it may be reasonable to follow-up in primary care rather than at a thrombosis clinic. 25 In a real world setting, our findings imply that we may be able to reduce the overuse of monitoring. This translates into cost savings and would allow resources to be allocated to those higher risk patients who are more likely to benefit. Additionally there may be an improvement in the quality of life for those low-risk patients with the avoidance of frequent and unnecessary hospital visits.
Our study has strengths and limitations. Our observations were based on examination of individual patient data and are therefore likely to be more accurate than those derived from administrative codes. Limitations were as follows: We did not include the rate of re-admission in our primary outcomes, nor did we gather patients’ opinions on the perceived need for follow-up. The decision to ambulate patients lay solely with the senior decision-maker based on their clinical judgement. We were unable to identify patients who remained symptomatic and did not seek help. We assumed that those with ongoing dyspnoea would discuss this with a healthcare professional and that appropriate onwards referrals would be made, with related diagnoses captured in their records, though we did not identify any evidence of this. It is possible nevertheless that a subgroup of patients with post-PE syndromes existed but were never formally diagnosed.
We believe that our findings are generalizable. The resources available within different hospital settings is not a limiting factor given that we are advocating for a reduction in resource utilisation, and in particular we are suggesting that no further imaging such as repeat CTPA or echocardiography is required. Furthermore, as PESI is a widely recognised and validated tool for identifying low-risk patients, this reinforces our belief that our findings would apply broadly. We are not aware of varying rates of adverse outcomes in different ethnic groups which would contra-indicate the streamlining of follow-up for patients in other countries.
Conclusion
In conclusion, the low rates of adverse outcomes identified in our study support both the notion that appropriate patients were ambulated and that these patients did not suffer because of a lack of formal follow-up. We feel our findings support a more nuanced approach to post-PE care. By adopting such an approach, healthcare systems can optimise resource allocation and enhance patient care. Further research is warranted to establish clear guidelines for post-PE management tailored to individual patient risk profiles. It may also be of interest to investigate whether any subgroups within the low-risk population might benefit from closer follow-up. Notwithstanding, we conclude that for low-risk patients who do not have an oxygen requirement and are not hypotensive when first seen, a follow-up call at 1 week with worsening advice given, may be all that is required.
Footnotes
Author contributions
LA and CI had the idea for the project, LA and SB collected the data, LA wrote the first draft, all authors contributed to the final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our study was conducted to define and measure current care and involved routine interventions already in common use. We did not randomize or allocate patients to treatment groups. As our study met the criteria for service evaluation, we did not seek approval from our research Ethics Committee, in keeping with our health board policy.