
Abstract
Background:
Resident doctors require professional development through conference attendance yet there are major challenges to the ways in which attendance is impacted. The COVID-19 pandemic created a shift in education delivery, including medical conferences moving towards online setting. The aim of the study was to explore the factors influencing conference attendance and the post-COVID-19 implications for the future of conference delivery and professional development.
Methods:
A mixed-methods approach comprising of an online questionnaire and semi-structured interviews was used. Theoretical sampling was performed to invite UK-based resident doctors to complete the questionnaire. Individuals were then invited to a semi-structured interview to explore their experiences further. Content analysis was performed for questionnaire data and thematic analysis for interview data.
Results:
Seventy-four doctors completed the questionnaire, of these 15 participated in semi-structured interviews. During the COVID-19 pandemic most trainees attended online events, but with the abolition of travel restrictions all were keen to return to the face-to-face format. Motivational learning promoted the drive for conference attendance. Other factors included networking and the attainment of continuous professional development points.
Discussion:
The findings demonstrate how professional development can be successfully enacted through changes to the delivery of conferences. Virtual conferences promote inclusivity and accessibility for doctors in training. However, the lack of opportunities to network is their main drawback. Whilst face-to-face conferences are considered the most attractive; concerns regarding cost, leave, sustainability and work–life balance affect motivation to attend. The findings have implications for educators, resident doctors and conference organisers.
Keywords
Introduction
Medical conference attendance provides a host of advantages for resident doctors including continuous professional development (CPD), networking and presentation of original research. 1 Within current UK training schemes, credit is awarded for conference attendance and presentations, thus also providing advantages for career progression. Furthermore, attendance certificates are sought-out by training programme directors at e-portfolio assessments. 2
During the COVID-19 pandemic, all forms of communication were moved to the virtual platform. Now, five years down the line, the medical and academic world are returning to their pre-COVID-19 educational calendars. Conferences are now being held in numerous forms including face to face, online or hybrid. 3
Virtual meetings facilitated ongoing communication between doctors and scientists, ultimately paving the way for the creation of vaccinations which ultimately decreased the morbidity and mortality associated with COVID-19. It is indisputable that the online platform has many advantages. With regards to conferences specifically, digital events can help tackle inequality. Accessibility is increased by minimal travel and the associated cost, in addition to cheaper registration fees. This is particularly important for graduate students, post-doctoral researchers and female academics who are identified as having lesser economic means (compared to tenured professors and male colleagues).4,5 They also allow individuals with family responsibilities, physical needs and visa requirements, who may not have otherwise been able to attend an in-person event, to participate.4,5 Such flexibility can be beneficial for resident doctors who are usually subject to busy on-call rotas with limited study budget and leave allowance.
As concerns about the environment continue to mount, online conferences also have the benefit of reducing an individual’s carbon footprint. Prior to the COVID-19 pandemic an in-person global conference could produce 1.3–1.8 tonnes of carbon dioxide per attendee which would exceed the two-thirds of the total annual per capita emissions of several countries, including the United States and United Kingdom. 6
Numerous teams have described their experiences of transferring their conferences to the online setting, suggesting that attendee numbers more than doubled. However, these trends do not appear to reflect attendance from low- and middle-income societies, who have been reported to have attended more in-person conferences, compared to the online events (since this move to digitalisation).6,7 This reflects a digital divide, raising the question of how inclusive the online environment is. Other drawbacks included; time zones restrictions, no parallel sessions, hence, a shorter scientific programme. 6
CPD points are compulsory elements of conference attendance. In-person conferences can offer subject delivery in a variety of methods including workshops, round table discussions and traditional lectures. 8 Within the virtual world however, variety can be more difficult to produce, hence, providing challenges in engaging prospective participants both behaviourally and cognitively. One limitation of video conferencing, ‘zoom fatigue’ could be due to prolonged direct eye gaze (a phenomenon not present during in-person interactions) and screen size (affecting brain activity and biochemical changes). The ‘chat’ function can also lead to distractions and processing overload, as well as emotions of self-consciousness.9,10 Distractions within the home environment are also thought to contribute. Delegates of digital conferencing admitted to undertaking multitasking behaviours, which have been linked to lower engagement. 11
Another benefit of in-person conferences is the social events offered. For resident doctors especially, conferences can be a satisfying way to meet and catch-up with colleagues, meet experts in the field who they otherwise would not have had the opportunity to meet, and perhaps most importantly, identify opportunities for future practice. All this whilst exploring new cities and cultures. 12 Despite a reported increase in trainees joining virtual conferences, a decrease in the participation of social events within the online platform, compared to in-person has been reported. Unfortunately, with the current state of technology little can be done to change the opportunities available.8,9 Whilst specific reasoning for this has not been elicited, in a questionnaire-based study by Bolander et al. comparing the two conference formats, digital conferences were described as ‘less real and fulfilling’. Virtual participants approached them with a stance of ‘ambivalence . . . apathy . . . and resignation’. 4 Conference organisers therefore have many factors to consider when planning their annual events.
To our knowledge, there is no published literature reviewing how post-COVID-19 educational events are perceived by doctors in training. The aim of this study was to explore resident doctors’ current perceptions on factors affecting online and in-person conference attendance to events, hence identifying key themes regarding the decision-making process of attending medical conferences. This can provide the foundations for conference organisers to plan their events according to what is most beneficial for doctors in training.
Methods
This work was performed by using a mixed-methods approach comprising of a two-phase study design. Phase 1 comprised a questionnaire and phase 2, semi-structured interviews.
A questionnaire was chosen for phase 1 as an efficient method to assemble context on which to base the interviews and hence produce theory. This comprised 21 original questions subdivided into 3 sections demographic information, experience of online conference attendance, and perceptions of skills acquired at conferences. (A copy of the questionnaire can be found in Supplemental appendix 1). Furthermore, given the intended study group of resident doctors within the United Kingdom can be very large (currently estimated at over 60,000 individuals), the questionnaire provided an opportunity to create a volunteer pool keen to be interviewed. 13 At the end of the questionnaire participants were asked to provide their email address if they had attended both in-person and virtual conferences and were happy to be contacted regarding phase 2 of the study. Phase 1 therefore directly informed phase 2. Approval was granted from the Hull York Medical School Ethics Committee in May 2022.
Resident doctors (any grade before consultant level) working in the United Kingdom who had attended a medical conference (from medical school until the present-day) were eligible. This ensured that participants were subject to the same training criteria and opportunities.
Purposive sampling was used to approach participants. Once a cohort of participants was established, theoretical sampling was undertaken through semi-structured interviews. Grounded theory methodology was subsequently followed allowing the researcher to be guided by emerging theory. The use of analysis and coding at the end of each interview further facilitated this procedure. 14
Sample size was not explicitly predetermined, as per Glaser and Strauss’ data saturation principles, and concerns that numbers within qualitative research are valuable but should be used with caution and only in specific circumstances as per Monrouxe et al. However, a review of the previous literature suggested that saturation could be reached with 4–40 interviewees. 13 The researchers therefore aimed to recruit 20 participants.
Doctors were recruited to phase 1 of the study through advertisements on social media. Word of mouth, led to snowball recruitment. The online questionnaire was implemented on Google Docs™. It comprised 20 multiple choice questions. Question generation and design were undertaken via consensus discussion amongst the authors, abiding by previously described successful formats.15,16 Pilot testing was undertaken amongst five relevant doctors in training. Participating volunteers completed the questions anonymously, with implied consent. In May 2022, the questionnaire was released into the public domain, remaining live for 6 weeks. At this time, all UK COVID-19 restrictions had been lifted. Many medical conferences had reverted to an in-person format, with few adopting a hybrid setup. For phase 2, all participants who provided an email address expressing interest in being interviewed were contacted and provided further information. Participants who consented to be interviewed provided their written consent prior to interview.
Interviews were performed with pre-prepared interview stems for effective qualitative inquiry. All were anonymised and recorded via Microsoft Teams™, using the application’s automatic software for the production of interview transcripts. The average interview duration was 28 min. Each transcript was then reviewed by the lead investigator. Data collection (including both the survey and interviews) was undertaken over a 12 week period.
Questionnaire data analysis was conducted via content analysis. Interview data were subject to constant comparison thematic analysis. Open coding was used to generate initial codes, axial coding led to category creation, which contributed to the creation of selective coding and theme creation. 17
Reflexivity
Personal reflexivity was undertaken by the lead author prior to conducting the interviews, to reflect on how their own experiences, values and cultural background might shape the research process. 18 The lead author is a junior resident doctor with first-hand experience of attending and organising medical conferences. This shared professional background helped facilitate rapport with participants, particularly in building trust and shared understanding around the topic.
The interviews were also shaped by an ethics of care approach. This involved actively fostering psychological safety by reassuring participants of the anonymity of their responses, giving them as much time as needed to answer questions, and allowing them to skip any questions they found distressing. Given the sensitive nature of recalling experiences during the pandemic, the interviewer was attentive to verbal and non-verbal cues that might suggest discomfort. For remote interviews, the camera was kept on, to allow visual observation of participant wellbeing, and participants were regularly checked in with during the conversation.
The lead author conducted and transcribed the interviews, whilst all three authors were involved in the thematic analysis. The co-authors are experienced qualitative researchers in medical education and brought a critical, outsider perspective to the data, which complemented the insider positionality of the interviewer. Regular team discussions were used to reflect on how each ’researcher’s background influenced data interpretation, ensuring that multiple viewpoints were considered during analysis.
Whilst participant quotes are presented largely in verbatim form, minor adjustments were made to remove colloquialisms for clarity and readability.
Results
The results that follow combine those from phases 1 and 2. However, the focus of this section will be on the results of the semi-structured interviews (phase 2).
Study population
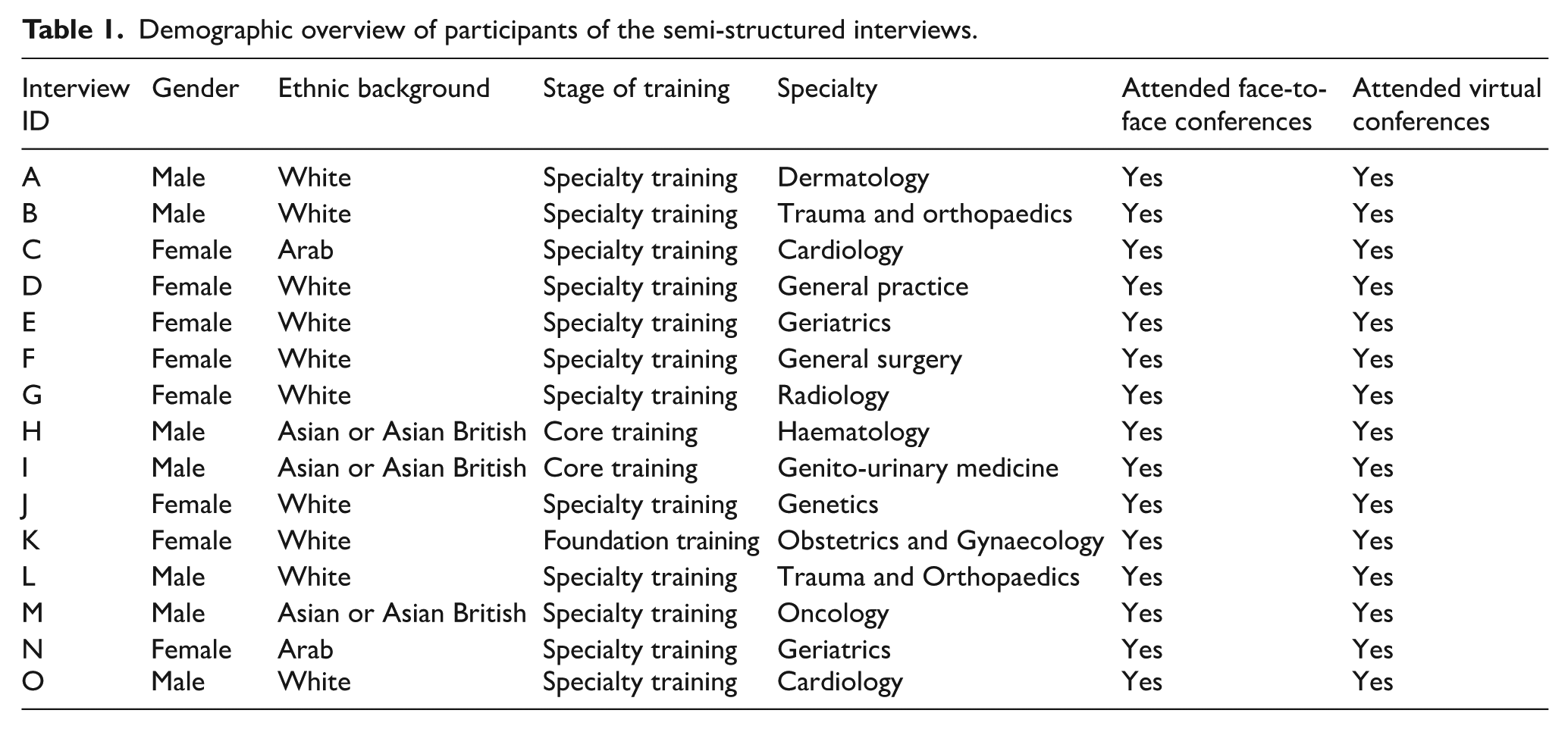
A total number of 74 resident doctor completed the online questionnaire. Of the respondents, 61% were female, over half were aged 25–30 (54%), and 60% were in specialty training. Thirty-one questionnaire participants provided their contact details to submit their interest in phase 2 of the study. Of these, 15 resident doctors provided their written informed consent for interview participations. Table 1 depicts their demographics.
Demographic overview of participants of the semi-structured interviews.
Conference attendance
Most questionnaire participants had only attended virtual conferences since the COVID-19 pandemic (n = 66, 89%). Four main themes were discussed, comprising of social interaction, work–life balance, multiple modalities and the future. Each of the themes and subthemes will be discussed below.
Theme: Social interaction
The in-person setting appeared to facilitate networking better than virtual equivalents. Sixty percent of questionnaire respondents admitted that they had effectively networked at in-person events, but fewer than 10% agreed to this in the virtual setting.
Interviewee A stated that it is possible to network online, ‘but only through constructed means for example, speed dating style events’. They added, ‘many people you might like to speak to won’t attend this.’ Other methods were also described, but there was universal agreement that no virtual format was better than in-person contact.
Feelings of awkwardness, intimidation were described when discussing online events. Furthermore, during online events participants noted that they may be quiet and not interact with other conference delegates through choice. Interviewee B said, I don’t find it easy to network online. I think you need to have that personal interaction with somebody, be able to have the opportunity to maybe grab a drink after the conference, etc., and also get to know them on a personal level rather than just on a workplace level.
Theme: Work–life balance
Organising themes contributing to work–life balance included: travel, time, personal-life and career aspirations. The interviewees suggested that whilst enjoying travelling for an in-person conference and the benefits associated with this of exploring the host city, such an act must be balanced with carer responsibilities, study leave and cost.
Travel
Trainees enjoyed not having to travel during the pandemic and being able to participate in conferences from their own home. Furthermore, all participants suggested an increasing awareness of their carbon footprint and the need to be more environmentally friendly.
Cost
One of the recurring comments was that of cost. Doctors in training, regularly expressed concerns, or recalled prior issues of having conference costs paid for by their deaneries. When this was not the case, there was great concern of having to facilitate the cost of the event out of one’s own pocket in order to await reimbursement further down the line. Interviewee J described this through the following: Cost is definitely a factor to consider, I think because of the way the study budget works. We only get reimbursed after the event. So it’s quite a risky process to organize a face to face conference if you don’t know 100%, you’re going to get reimbursed for that.
Study leave
Ascertaining study leave, was frequently described as a possible issue for conference attendance by all interviewees. Some specialities tend to be particularly strict with their allowance, as described by Interviewee J;
We only get study allowance for one international conference or meeting over your training program. So I’m going to have to really select that, whereas if it’s a virtual meeting, they’re slightly more lenient with the study leave policy with regard to that.
Family life
Doctors with a young family were less likely to consider travelling for an in-person conference. Parents were reluctant to leave all childcare responsibilities to their spouse so that they could attend an in-person conference, this was particularly the case for those with young children, as Interviewee O describes, ‘I’ve got a young baby at the moment . . . if there is something that I want to go to, I’ll try to go to that online rather than in person’.
Career aspirations
Doctors at different stages of training had differing priorities for attending conferences. More junior trainees, chased career progression opportunities such as oral and poster presentations, given that this would provide points for job applications in the future, whereas specialty trainees attended for knowledge acquisition and networking.
The two quotes below sum up the progression of seniority and how the differences in conference attendance varies.
Interviewee I said, As an SHO [senior house officer] my main reason [to attend conferences] is to a. gain further experience of what it would be like to work as a senior in that specialty. I’ve seen the registrars and consultants in clinics, but it’s very different to see them in the more academic side of things, and also to gain further experiences of poster presentations. I attend the conference in general, a. for CV and b. to be a more well-rounded physician.
By contrast, Interviewee M, who is a speciality registrar disclosed the following: I certainly know some of my colleagues are involved with setting up clinical trials where they need to work closely with drug companies in setting up those trials will specifically go to these conferences. . . for the sole purpose of networking with the drug companies for a trial that they’re setting up, so I imagine that’s something that will become more important for me in the future.
Theme: Multiple modalities
Differences in conference execution were also discussed during the semi-structured interviews. Participants disclosed their opinions on the presence of industry, and how the online environment has a different feel to that of in-person as well as many other advantages and disadvantages.
Industry
The presence of pharmaceutical companies at conferences, was met with varying opinions. Surgical trainees placed great emphasis on their presence and need for interaction, whereas medical trainees did not see such need. Interviewee F identified, ‘I enjoy face-to-face conferences [because of] the ability to interact with industry. It’s quite useful to see instruments you might be using. . . to get the actual industry description of how to use it. . .I would never get that online’.
Technology
All interviewees suggested that they did not have issues with accessing online content based on their ability to use an online system. The difficulties tended to arise when the speakers were not ‘au fait’ with the technological aspects of presenting. Emotions of frustration surfaced in situations where the virtual environment was trying to mimic the live environment. Interviewee L recalled their experience, I went to one [a conference] and it just felt quite rude. They went to their AGM bit, and it just cut us all off. Obviously in a regular conference that would be a separate room, and they’d all go off and do it, whereas we just got binned but not really pre warned.
Most interviewees were unaware of all the opportunities that virtual conferences offer, including play-back of recorded sessions, especially those in surgery. However, many trainees admitted that time, was a limiting factor. The time they had allocated to attend a conference did not account for the ability to re-watch sessions.
Virtual fatigue
Fatigue of talking to people online, was raised as a disadvantage of virtual conferences on numerous occasions. Interviewee M recalled, ‘It’s just another thing that you’re doing via screen. . . like all these other aspects of our life and work that are now done digitally. So that makes it less unique’.
This was accompanied by numerous descriptions of the online platform not providing the same experience of communicating with individuals that the in-person environment offers, Interviewee H suggested that There’s an element of communication that you lose out on when you’re doing it online. . . human interactions are very important. . . there’s aspects of communication that you just can’t convey on a screen. Also seeing things live and in person. For example, if there’s a practical demonstration of something, it’s easier to appreciate than on a screen or on a on a textbook.
Multitasking
Many participants described the multitude of distractions which affected their concentration whilst attending online conferences. For example, Interviewee O suggested that For whatever reason people feel the compulsion to try to multitask. . .. if it’s online you feel as though I should probably be doing a bit of something productive at the same time and it is quite easy to get distracted with emails or things like that.
Theme: The future
Finally, at the end of each interview, participants shared their insights regarding the future of medical conferences. Most participants suggested that going forward they would prefer for conferencing to return to the face-to-face format. Reasons for this included maximising networking opportunities and concentration within lectures. There was a growing awareness amongst respondents regarding the benefits of increased accessibility and flexibility that virtual conferences offered.
Interviewee D summarised this effectively by stating, I think lots of people have got used to attending online conferences. If they have dependents at home, they’ve not had to sort out childcare. . . or travel. So I think in terms of ease and flexibility, it’s a lot better.
The overwhelming majority of participants however, suggested that hybrid events could be the future. An example of this was Interviewee K expressing, I think hybrid makes it a lot more accessible for a wider variety of people who wouldn’t be able to go. You’ve got all your environmental sustainability boxes ticked, if [participants] are worried about carbon footprint, or the travel, they can go virtually. If you want to attend in-person you can . . . It’s also a lot more accessible from a diversity point of view, if you have got childcare responsibilities, or you’re ill, or disabled. You can attend the conferences from an environment that’s better for you.
Discussion
This research is the first to explore UK resident doctors’ experiences of attending medical conferences pre- and post-COVID-19 pandemic and disclose their opinions regarding the optimal method of attending a conference in the future.
What type of conferences are resident doctor attending?
The recurring motivations for conference attendance included compulsory training events and personal career progression. McClelland’s theory of the three key motives for learners: power, achievement or affiliation depicts the results of our study population. 19 Achievement as obtained by the presentations of original work, power (the ability to have choice in which event to attend) and affiliation (the importance of networking).
The current data suggest that resident doctors attended virtual conferences at a time where no other options were available. In the era of ‘choice’, the aforementioned motivations will guide conference attendance decisions. An almost unanimous preference towards an in-person event was displayed by the doctors in the cohort, but practicalities may affect this long term.
CPD – Face-to-face vs virtual
Requirement and desire for CPD were a recurring motivation theme for conference attendance both within the study population and literature.1,15 The most traditional learning theory associated with acquisition of new knowledge is Bloom’s developmental taxonomy. 20 This six-level structure highlights that one cannot progress to high levels of intellectual development, without first understanding and applying the knowledge. 16 Medical conferences provide an opportunity for classroom education, in a world of post-graduate medicine, where most learning is undertaken experientially. As such, Bloom’s taxonomy is only the start of a complex inter-relation of learning theories. Dewey recognised the ‘intimate’ relationship between processes of experience and education. 20 Active engagement and interactions of one’s surroundings are considered to help learners gain applied, rather than abstract, knowledge. 21 To facilitate this effectively, our results support that this can only be done within the in-person environment. Socialisation, simulation and opportunities to engage with speakers were the main driving forces behind this.
The problems surrounding CPD attainment at virtual medical conferences included altered concentration due to distractions and multi-tasking behaviours. Is it therefore participating via a screen which causes distraction, or is it the environment in which you do this? The interview respondents suggested that they would often multitask when participating in virtual conferences with household chores or other personal commitments. If such tasks were not performed, would their concentration increase? John Hattie’s concept of visible learning suggests that teaching is visible when the learner knows what to do and how to do it, but perhaps more importantly, when the teacher knows whether learning is happening or not. 22 In the majority of online conferences, most attendees participate with their screen turned off. One could pose a policy of live screen sharing implementation to all attendees, and review if engagement alters.
The issue of quantity was also posed by interviewees. In-person attendance was more likely to mean less flexibility in attending multiple sessions. Sousa et al. proposed that to get the most out of an academic conference one must plan their participation and have self-awareness of preferences and learning needs. 23 By mentally preparing for an event’s attendance, one is already committed and more likely to engage with the educational content available. Online events lack parallel sessions, such absence of choice, could lead to a lack of commitment and preparation, hence reflecting the perceived inferiority of academic engagement.
Implications for CPD
The lack of travel and lower costs makes CPD opportunities easier for online conference attendance. However, improvements need to be made to encourage audience participation, hence increasing concentration and consequent satisfaction. The compulsory use of an attendee’s camera and interactions with live questions and polls could facilitate this. Alternatively, running parallel sessions to mimic an in-person scientific program could be the answer. Both options however, would require technical support and additional funding, which could limit their implementation. 24
Networking – Face-to-face vs virtual
Our study suggests that given the choice, resident doctors prefer in-person conference attendance. The importance of socialisation at events, both with regards to networking and meeting experts in the field has been described. 25 Such opportunities not only aid potential career opportunities through making contacts but also influence the knowledge acquired at a conference. Vygotsky’s learning theory of the ‘Zone of Proximal Development’ (ZPD) suggests that students learn from the ‘Most Knowledgeable Others’ (MKO), a construct built through social interaction with family, teachers and colleagues. 20 Vygotsky suggested that once an individual was in the ZPD, they developed a level of understanding of a subject which had previously been above their ability level. To facilitate this, ‘scaffolding’ can be undertaken, by building interest in the subject and engaging the learners, and using MKOs to support them. 20 Conferences allow attendees to listen to the experience of experts in the field whilst providing a platform for all participants to contribute with their own experiences. Interestingly, our work suggests that the ZPD cannot be reached within the virtual platform, due to a lack of life-like networking opportunities and the absence of prospects of meeting someone ‘naturally’. Furthermore, Petty has suggested that leaders of a field can provide a creative element to teaching. He suggests that through the process of inspiration, clarification, distillation and evaluation, one can develop their skills in self-expression. 26 This highlights that benefits of conferences are all intertwined, and one cannot be achieved without another.
When considering networking, without the additional need for learning, conferences present a unique opportunity to regularly meet certain colleagues one interacts with, only within the conference circuit. Other individuals use such opportunities to meet new people and build relationships. Bryk and Schneider’s notion of relational trust describes such social exchanges. 20 Difficulties of engaging in such ‘trust’ online has been described. It is unclear whether it is the specific virtual environment that creates this, or the method of advertising. Social media platforms have been used to improve networking at conferences. Ebner et al. described the use of Twitter to facilitate networking at an international conference. 27 At their face-to-face event, tweeting facilitated exchange of resources, documentation of social activities, opportunities for feedback and discussions and the organisation of short meetings between online users. 28
Such views appear to be held worldwide. In a study conducted by Englebrecht et al. from authors in South Africa, South Korea, Brazil and the US with a very similar design to the one presented here, but aimed at mathematics education researchers, the participants also agreed that the face-to-face environment better addressed all forms of academic interaction. This included all aspects of learning (particularly when considering workshops), interaction with colleagues and forging new collaborations. 29 The concerns regarding the absence of social interaction at virtual conferences was unanimous from all participants. They suggested that an ordinary activity such as sharing food or partaking in small talk with other conference attendees create social interactions which can help people feel part of a community. 29 Similarly in work performed by Chan’s team in Canada where they explored students’ views from an internal medicine conference between attendees participating online compared to in-person. Those attending on the virtual platform described a limited potential for interaction with other participants. 30
Implications for networking
Human contact cannot currently be adequately replicated in the virtual environment. However, a move towards face-to-face conferences only, does not seem sustainable. Moreover, one must question how we forget how technology helped nurture a feeling of ‘togetherness’ during the COVID-19 pandemic. At a time of social isolation, video conferencing allowed the world to come together. Instead of forgetting virtual networking, work is needed to facilitate its execution in a more natural method. The answer may lie in the increasing use of social media. Platforms such as Twitter™ and Facebook™ are widely used by medical professionals and have facilitated networking outside of conferences for years. Their ease and accessibility could allow virtual attendees to feel less awkward and discouraged.
Is the hybrid model the future?
Whilst most interviewees reported that they would prefer to go back to in-person conferences, the same participants suggested that if this was not possible, they would settle for a hybrid format. Hybrid conferences have been considered the future. Interestingly, they are considered favourable due to the advantages the online platform offers; increased inclusivity, accessibility, and choice were the main reasons behind this favourable option to the resident doctor interviewees. This helped to dismiss concerns regarding travel budget and study leave allowance, as well as the opportunity to balance family life, and minimise one’s carbon footprint.
The limitation to the widespread use of this format in the future, however, is its sustainability. Hybrid conferences are more expensive to fund and more time-consuming, as organising bodies are ultimately running two conferences. There are concerns that choice will lead to fewer in-person attendees. 31 Virtual events are typically less expensive than their in-person counterparts. Certainly, the cheapest option would be to record a live event for playback at a later time.
In a publication of their real-world experience of setting-up a hybrid conference, Devaraj et al. report that of the 1,150 attendees registered, only 155 were physically present. 20 However, this may not be representative of current practice given that their conference was performed in 2021 where travelling was much more limited. Ongoing research is therefore needed.
At the time of writing, the world is now significantly less affected by the COVID-19 pandemic (outside of the walls of hospitals). A drive towards face-to-face meetings is welcomed by trainees as they increase their opportunities to network, engage in simulation activities (particularly for those in surgical specialties), and present original work. However, these is a strong desire for choice. Resident doctors want to balance CPD and networking with family life, carbon footprint and expenses. Whilst hybrid conferencing may be an option in the future, the current literature suggests that their limitations outweigh their benefits.
Limitations
There are a number of limitations of the study. First, the nature of recruitment meant that the study was advertised to individuals known to the researcher. Ultimately, this resulted in interviews being conducted with volunteers that knew the researcher in a working or social capacity. Study volunteers are more likely to participate in research if they have had such social interactions in the past. However, such interactions could have had an impact on the power dynamics of the interview processes, which are known to affect interview responses. 32
The validity could have also been impacted due to the lack of triangulation, in particular the constructivism values of triangulation. 33 Only one researcher undertook the coding of the interview transcripts. It is possible that by including others in the process, different codes could have been generated, hence producing different theories.
Finally, there are many aspects of attending conferences that were beyond the scope of this work including gender balance, reflective practice and role modelling.
Considerations for future work
The current work suggests that the needs of doctors in different medical specialties differ. As such it is prudent to consider further work within surgical, and other medical specialties to relay their experiences and perceptions of medical conferences within their field. Additional work is also needed to investigate if stages of training, affect doctors’ conference attendance decisions.
Finally, this research has focused on resident doctors within the United Kingdom. Access to technology, ease of travel and study budget allowance will vary between this participant population and doctors in other areas of the world. Differences should particularly be considered to those in developing countries, where resources are fewer. An expansion of this study could therefore be rolled out internationally to address this gap.
Recommendations for conference organisers in 2025
Conduct a comprehensive needs assessment prior to determining the conference format
The optimal mode of delivery should be determined by the characteristics of the target audience and the intended learning objectives. For events where the primary goal is the dissemination of knowledge, a fully online format may be adequate and more inclusive for a geographically and demographically diverse audience. Conversely, when fostering professional networks and facilitating informal exchanges are central objectives, an in-person format is likely to be more effective.
Prioritise hybrid models to maximise accessibility
Although hybrid events may entail greater financial investment, they provide the broadest access for potential participants. To ensure equitable engagement across modalities, organisers should implement robust technological infrastructure and technical support, thereby delivering a seamless and high-quality experience for both virtual and in-person attendees.
Strengthen networking opportunities in face-to-face settings
In-person conferences are particularly effective in facilitating the development of sustained professional relationships. Organisers should integrate dedicated networking spaces, structured interaction sessions, and informal social events into the programme. Such initiatives are likely to be valued by participants seeking to expand professional networks and collaborations.
Incorporate environmental impact and cost transparency into planning
Sustainability and affordability have become salient considerations in the post-COVID-19 era, particularly among doctors. Organisers are encouraged to publish estimates of the event’s carbon footprint and to offer incentives for environmentally responsible participation. Additionally, implementing tiered pricing structures – based on factors such as attendance mode (online vs in-person) and duration (single-day vs multi-day) – should be considered standard practice.
Conclusion
This mixed-methods study has demonstrated the perceptions of factors affecting conference attendance of UK resident doctors. Whilst virtual conferences helped to plug a gap in medical education throughout the COVID-19 pandemic, trainees are ready to re-enter auditoriums and interact in person. However, this must be balanced with accessibility and inclusivity of training opportunities. Funding of events and concerns regarding global warming are also expected to pose strain on in-person conference attendance. More work is therefore required to compare the face-to-face and virtual platforms whilst industry continues to optimise the hybrid format.
Supplemental Material
sj-docx-1-rcp-10.1177_14782715251389277 – Supplemental material for Junior doctor medical conferences in the post-Covid era: A mixed-methods study
Supplemental material, sj-docx-1-rcp-10.1177_14782715251389277 for Junior doctor medical conferences in the post-Covid era: A mixed-methods study by Marilena Giannoudi, Paul Crampton and Amaya Ellawala in Journal of the Royal College of Physicians of Edinburgh
Footnotes
Data availability statement
A copy of all interview transcripts can be provided upon request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was granted from the HYMS Ethics Committee in May 2022 (ref no.21 – 22 46).
Consent to participant
All interviewees signed a participant consent form which can be provided on request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.