
Abstract
A 92 year old female with multiple co-morbidities was admitted following a fall at home. She was found to be suffering from ongoing loose stool with intermittent rectal bleeding during hospitalisation. An inpatient flexible sigmoidoscopy identified a large well-demarcated, superficial, non-bleeding ulcer in the rectum. Histology of biopsies of the rectal ulcer showed inflammation and ulceration with crypt distortions in the ulcer base. Immunohistochemistry for cytomegalovirus (CMV) confirmed presence of inclusion bodies which was suggestive of CMV proctitis. Her CMV IgG serology was positive with a high DNA level of 15,861 IU/mL. Oral valganciclovir was started and patient responded well to the anti-viral treatment with resolving bowel symptoms.
Keywords
Introduction
Cytomegalovirus (CMV) colitis has been well recognised as an opportunistic infection in immunocompromised patients and often results in significant morbidity and mortality in hospitalised patients. Immunocompetent patients are rarely affected. Below we present an interesting case of an unusual presentation of CMV proctitis in an elderly patient.
Case presentation
A 92-year-old lady was brought into hospital following an unwitnessed fall at home. Her past medical history included hypothyroidism, ischaemic heart disease, type 2 diabetes mellitus with a recent HbA1C of 6.7%, osteoarthritis and a previous ischaemic stroke. Her observations were stable and she remained afebrile. Blood results including inflammatory markers on admission were unremarkable. She was admitted to a geriatric ward for further management and found to be suffering from ongoing loose stool with intermittent fresh rectal bleeding. Multiple stool samples were sent without any microorganisms identified. She had had a recent hospital admission with rectal bleeding, which was thought to be related to haemorrhoids.
No medications including non-steroidal anti-inflammatory drugs were identified to be the possible cause of her diarrhoea. An in-patient flexible sigmoidoscopy was performed for further evaluation. Endoscopic examination to proximal descending colon revealed scattered uncomplicated diverticulae in the sigmoid colon and a well-demarcated, superficial, non-bleeding ulcer of approximately 4 cm in diameter in the rectum (Figure 1). Multiple biopsies were taken from the ulcer and histology showed inflammation and ulceration with some crypt distortions in the ulcer base. Immunohistochemistry for CMV reviewed presence of inclusion bodies which was suggestive of CMV proctitis (Figure 2). Subsequent blood test was sent to look for CMV viraemia which was not detected. She was then treated with acyclovir and her diarrhoea gradually subsided. Given the resolution of her symptoms, a repeat sigmoidoscopy to assess her rectal ulcer was not arranged after discussions with patient and her family before discharge.
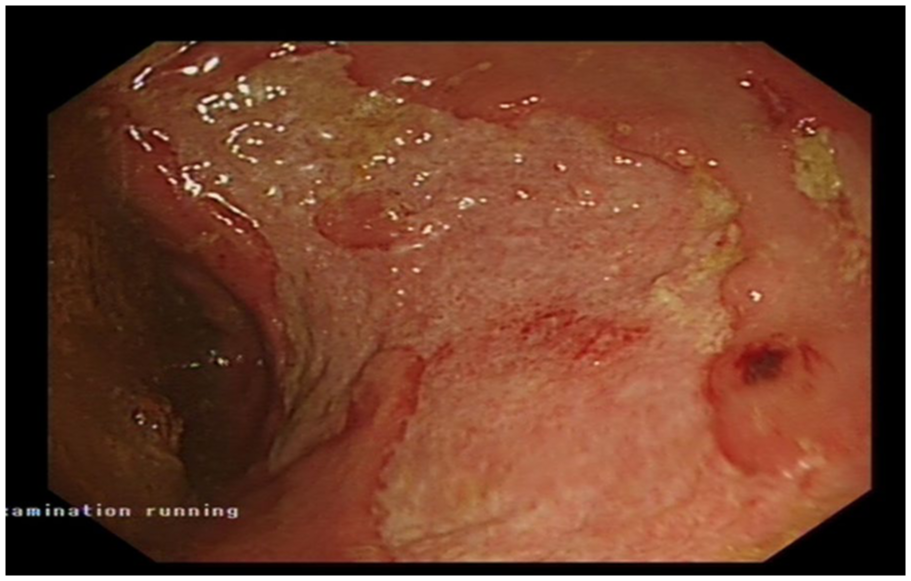
Flexible sigmoidoscopy revealed a large, well-demarcated superficial ulcer in rectum.
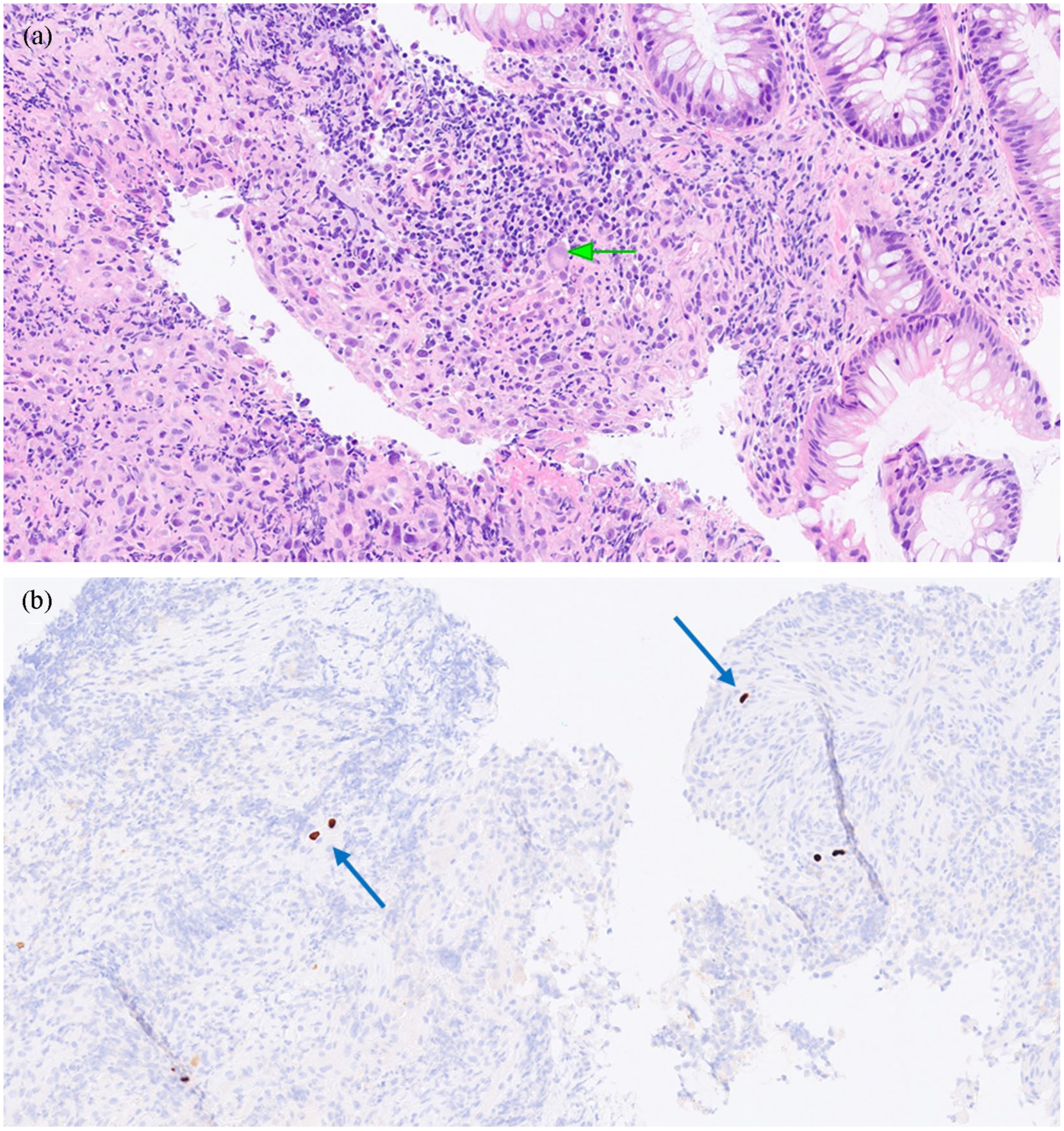
Microscopic examination of rectal ulcer biopsy. (a) Hematoxylin and eosin staining revealed inflammation and ulceration with crypt distortions and an CMV inclusion body (green arrow) in the ulcer base. (b) Immunohistochemical staining for CMV demonstrated positive uptake in inclusion bodies (blue arrows).
Discussion
There are many differentials for a rectal ulcer, and many conditions can manifest pathologically in the rectum. Solitary rectal ulcer syndrome, ulcerative proctitis, radiation proctopathy, non-steroidal anti-inflammatory drugs-induced ulcer are some of the examples. CMV colitis can present as a primary infection or reactivation. Given the positive status of our patient’s IgG with a negative IgM, this was a case of reactivated CMV infection in the form of a rectal ulcer. Although a full colonoscopic assessment was not performed to rule out coexisting proximal colitis, it was unlikely to be the case given the patients sigmoid and descending colon were unaffected at the sigmoidoscopy. Reactivation of CMV colitis in immunocompetent patients is uncommon and only a limited number of cases have been reported. This makes reactivation of latent CMV infection in the form of a solitary rectal ulcer in an immunocompetent patient extremely rare. We performed a literature search on PubMed online database using the term ‘CMV proctitis’ and indeed only one similar case in Taiwan has been reported. 1 Studies revealed that CMV colitis in immunocompetent patients tends to present in elderly patients and those with immunomodulating conditions such as diabetes mellitus.2–4 There is strong evidence that ageing is associated with immune system dysregulation within the gastrointestinal tract.5,6 It is also believed that latent infections further impair age-related immunodeficiency and hence elderly patients are more susceptible to reactivation of latent infections. 7
CMV colitis in immunocompetent is often associated with diarrhoea, abdominal pain, and occasionally haematochezia/melaena and fever.1,2 CMV proctitis and rectal ulcers, however, can potentially cause life-threatening complications such as heavy rectal bleeding, intestinal perforation and even death. 8 Furthermore, a majority of cases of reactivation of CMV colitis in immunocompetent patients during hospitalisation have been noticed to be preceded by an adverse event such as septic shock and infection, which resulted in a disruption to bowel mucosal surface.1,9,10 CMV colitis should therefore be routinely considered as a differential condition in hospitalised elderly patients who developed nosocomial diarrhoea.
Patients who are clinically symptomatic with persistent bowel symptoms and CMV viraemia are often initiated on anti-viral treatment. However, most studies have not been able to establish a conclusive clinical benefit in treating CMV colitis, which is often self-limiting with a proportion of patients achieving complete clinical resolution without medical intervention.1–3 Anti-viral therapies such as ganciclovir and valganciclovir are known to be associated with potential toxicities such as myelosuppression and nephrotoxicity. Clinicians should always cautiously weigh clinical benefit of anti-viral therapies against potential side-effects and toxicities before initiating treatment on a case-by-case basis.
Conclusion
In conclusion, CMV colitis in an immunocompetent individual is rare but should not be overlooked. Early recognition and diagnosis of the disease can improve patients’ survival. 4 Clinicians should remain vigilant and consider reactivation of CMV colitis in hospitalised elderly patients with multiple co-morbidities who develop nosocomial diarrhoea.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Consent for publication
Verbal and written consent have been obtained from the patient involved for this case to be published.