
Abstract
Background
Cardiovascular complications are the leading cause of mortality in patients with diabetes mellitus (DM) undergoing percutaneous coronary intervention (PCI). This systematic review aims to evaluate the association between HbA1c levels and major adverse cardiovascular events (MACE) in patients with DM post-PCI.
Methods
A comprehensive literature search was conducted following PRISMA guidelines. Eligible studies included randomized controlled trials, cohort studies, and observational analyses assessing the impact of strict, moderate, and poor glycaemic control on cardiovascular outcomes. Data extraction focused on HbA1c levels, MACE incidence, cardiovascular mortality, and cardiovascular complications.
Results
Nine studies with 24,978 participants were included. U-shaped and J-shaped relationships were found between HbA1c levels and cardiovascular outcomes. Moderate glycaemic control (HbA1c 6.5%–7.5%) was associated with the lowest risk of MACE and mortality. In contrast, strict glycaemic control (HbA1c <6.5%) and poor control (HbA1c >7.5%) were linked to increased cardiovascular risk. Patients with HbA1c below 5.5% exhibited a significantly higher risk of cardiovascular mortality, while HbA1c above 8% was also associated with poor outcomes.
Conclusion
Maintaining HbA1c levels in the moderate range (6.5%–7.5%) appears to provide optimal cardiovascular protection for patients with DM post-PCI. Strict or poor glycaemic control increases the risk of adverse outcomes.
Keywords
Introduction
Cardiovascular diseases (CVDs) encompass a spectrum of disorders affecting the heart and blood vessels, including peripheral arterial disease and ischemic heart disease, also referred to as coronary heart disease, constitute the foremost cause of mortality worldwide and significantly contribute to the burden of non-communicable diseases.1,2 Diabetes Mellitus (DM) is a chronic metabolic disorder characterized by persistent hyperglycemia. The Global Burden of Disease Study, indicates approximately 32.2% of all patients with DM have coronary heart disesase (CHD). 3 It has a significant global impact, with 463 million individuals affected in 2019, with that number expected to rise to 578 million by 2030 and 700 million by 2045. 4
DM, with traits of impaired insulin secretion, facilitates the development of atherosclerosis, a pathological mechanism strongly linked to CVDs. The long-term hyperglycemia plays a crucial role in promoting endothelial dysfunction, oxidative stress, and chronic inflammation.5,6 Prior to the discovery of glycosylated haemoglobin (HbA1c), researchers lacked a reliable marker to evaluate an individual’s long-term blood glucose level. In 1976, HbA1c was identified as a clinical indicator for evaluating glycaemic control in patients with DM. 7 HbA1c is now widely recognized as a gold standard biomarker to assess glycaemic control over 2-3 months, and it serves as a robust predictor of long-term prognosis and complications. 8 Recent experimental evidence shows that HbA1c not only reflects glucose exposure but may also directly contribute to vascular inflammation and oxidative stress. 9
Percutaneous coronary intervention (PCI) is a minimally invasive revascularization technique for coronary artery disease, typically involving balloon angioplasty with or without stent placement. The literature shows that patients with DM are more susceptible to PCI-related complications. 10 While acute hyperglycemia is associated with adverse post-PCI outcomes, 11 intensive diabetes treatment has demonstrated benefits in reducing cardiovascular risks. 12 More recent registry studies confirm that baseline HbA1c remains an independent predictor of major cardiovascular adverse events (MACE) and mortality following PCI in patients with DM. 13
These clinical findings can be better understood by examining the underlying pathophysiological mechanism. Chronic hyperglycemia drives macrovascular complications through several interconnected pathways. It includes oxidative stress and inflammation that damage the endothelium and reduce nitric oxide, leading to narrowed vessels, impaired repair, and faster atherosclerosis. 10 Second, advanced glycation end products cross-link vascular proteins, resulting in arterial stiffening and reduced compliance. Third, a thrombotic shift occurs due to increasing platelet activity and reduced fibrinolysis, raising the risk of stent thrombosis and heart events10,14
Insulin resistance and chronic inflammation worsen these effects by weakening insulin’s protective role in the vessels and speeding up plaque buildup after PCI. 14 Importantly, recent studies highlight that HbA1c variability, not just baseline level, is a significant determinant of adverse outcomes after PCI. 15
It is still debatable whether strict or lenient glycaemic control lowers cardiovascular complications. Several studies have reported the association between pre-procedural HbA1c and MACE in patients with DM undergoing PCI.12,16 A randomized controlled trial showed a U-shaped relationship, where both lower (HbA1c <6.5%) and higher (HbA1c >8%) values of HbA1c were linked to increased adverse outcomes. 17 However, most analytical approaches assess HbA1c either categorically or linearly, potentially overlooking more complex nonlinear associations.15,18
A 2023 systematic review confirmed a curvilinear (U- or J-shaped) relationship between HbA1c and outcomes, with both very low and high levels associated with adverse events. 19 Recent registry evidence further reinforces the prognostic role of HbA1c, demonstrating its predictive value for target vessel revascularisation, nonfatal Myocardial Infraction, and long-term mortality in patients with DM after PCI. 13 Optimizing preoperative glycaemic management presents a critical therapeutic challenge, particularly given that patients with DM make up <25% of all PCI patients and experience poor outcomes compared to the patients without DM. 20 Establishing evidence-based glycaemic targets before PCI carries substantial implications for reducing post-procedural complications and improving long-term prognosis.
Given these findings, the present review aims to clarify the association between HbA1c levels and cardiovascular outcomes, including mortality rates, particularly among patients with DM following PCI. Specifically, this review addresses whether moderate glycaemic control (HbA1c 6.5%–7.5%) is associated with superior cardiovascular outcomes in patients with DM following PCI, compared to both strict glycaemic control (HbA1c <6.5%) and poor glycaemic control (HbA1c >7.5%), reflecting a U-shaped relationship in which both extremes of glycaemic control are linked to significantly poorer cardiovascular outcomes. Additionally, this review investigates whether moderate glycaemic control is associated with reduced mortality rates and whether it provides better protection against post-PCI complications in patients with DM compared to strict or poor glycaemic control.
Methodology
This systematic review was conducted to evaluate the association between glycaemic control and cardiovascular outcomes in patients with DM undergoing PCI. This systematic review was not prospectively registered in PROSPERO, as the study protocol was developed retrospectively; however, to ensure transparency and reproducibility, the review was conducted in accordance with the PRISMA 2020 guidelines for literature search, screening, selection, and inclusion.
Search strategy
A comprehensive literature search was performed using the following electronic databases: PubMed, Google Scholar, Cochrane, and Science Direct to ensure comprehensive coverage of clinical medicine research, capture grey literature, conference proceedings, specialized collection of systematic reviews, controlled trials registry, and provide access to full-text scientific articles. The review focused on studies from January 2019-June 2025, as this period represents the emergence of research analyzing non-linear (U-shaped and J-shaped) association with cardiovascular outcomes. Earlier studies have focused more on a linear relationship. Search terms were formulated based on the PICO framework and refined using Boolean operators (AND/OR) to ensure a comprehensive yet focused retrieval of relevant studies (Figure 1). Development of search terms using the PICO framework and Boolean operators (AND/OR) to refine search results.
Study selection and eligibility criteria
This systematic review included studies involving adult patients (≥18 years) diagnosed with type 1 or type 2 DM (T2DM) who underwent PCI. Eligible studies reported pre-PCI or post-PCI HbA1c levels and their association with cardiovascular outcomes. Research comparing strict glycaemic control (HbA1c <6.5%), moderate control (HbA1c 6.5%–7.5%), and poor control (HbA1c >7.5%) with respect to cardiovascular events was considered. Only randomized controlled trials (RCTs), prospective and retrospective cohort studies, case-control studies, and large observational studies with statistical analyses were included. Additionally, only original research articles were considered for inclusion.
Studies were excluded if they focused on prediabetes, gestational diabetes, or pediatric patients (<18 years), lacked clear HbA1c stratification or cardiovascular outcome data, or evaluated non-PCI treatments such as coronary artery bypass grafting or medical therapy alone. Systematic reviews, meta-analyses, case reports, editorials, opinion pieces, and conference abstracts without full data availability were also excluded.
Two independent reviewers (AHK and ZB) screened the titles and abstracts to assess relevance. Studies deemed potentially eligible underwent full-text assessment, and any disagreements were resolved through discussion.
Literature search
The literature search identified 118 studies, of which 16 duplicate records were removed. After screening the titles and abstracts of 102 studies, 41 full-text articles were assessed for eligibility. Studies were excluded due to lack of comparative analysis, a non-PCI focus, or irrelevance to glycaemic control outcomes. Finally, 9 studies fulfilled the inclusion criteria and were included in this systematic review. The study selection process was documented using the PRISMA flow diagram (Figure 2). PRISMA flow diagram depicting the screening, eligibility, and inclusion of studies.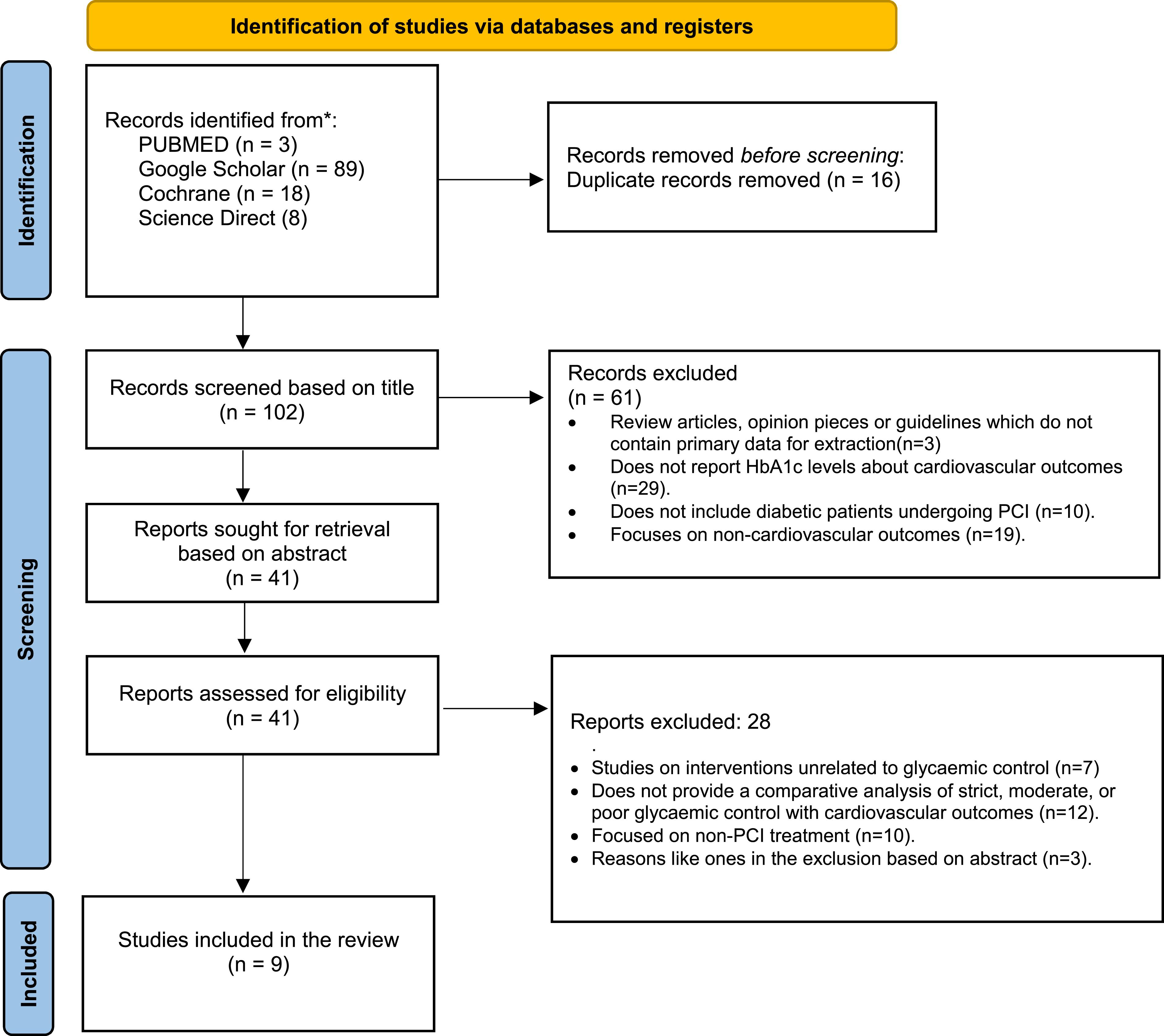
Data extraction
Data extraction was performed using a Microsoft Excel file to systematically collect the following information. The extracted variables included the author(s), publication year, study design (RCT, cohort, case-control, or observational study), sample size, and key patient characteristics such as age, gender, diabetes type, and comorbidities. Information on glycaemic control was categorized into strict, moderate, or poor, with HbA1c targets defined consistently as <6.5%, 6.5%–7.5%, and >7.5%. Details of interventions, including medication use, insulin therapy, and lifestyle modifications, were also collected. The duration of follow-up (e.g., 6months, 1year, and 2year) was noted, along with primary cardiovascular outcomes such as MACE, Myocardial Infarction, stroke, heart failure, and stent thrombosis. Mortality rates, including all-cause and cardiovascular mortality, were recorded. Statistical measures such as hazard ratios, relative risks, odds ratios, confidence intervals, and p-values were extracted, along with any confounding variables that were controlled for in the analysis (e.g., age, hypertension, and kidney disease). The overall characteristics of the included studies are given in Supplement S1. It contains two sheets: Sheet 1 summarizes basic study characteristics (title, authors, outcomes, mortality rate, and main findings), while Sheet 2 provides detailed data on study design, follow-up, glycaemic control groups, and cardiovascular outcomes (e.g., HRs, CIs, p-values for MACE, Myocardial Infarction, stroke). ROBINS-I (Risk of Bias in Non-Randomized Studies of Interventions) tool was used for quality assessment of the included studies given in Supplement S2.
Data synthesis
A narrative synthesis approach was employed following the guidelines proposed by Popay 2006, 21 to assess the role of moderate glycaemic control in improving PCI outcomes in patients with DM. This method was chosen due to the heterogeneity in HbA1c categorizations, outcome measures, and follow-up durations, which made a formal meta-analysis inappropriate. First, a preliminary framework was developed based on existing literature, which suggests better cardiovascular outcomes with a U-shaped relationship between HbA1c and post-PCI, where both hypo and hyperglycemia increase cardiovascular risk. The findings were then grouped thematically into three predefined glycaemic control categories, i.e., strict, moderate, and poor, and types of relationships, such as U-shaped, J-shaped, linear, or threshold-based, on the basis of HbA1c ranges reported across studies. This categorization allowed for pattern recognition and comparative analysis. A tabular format was used to summarize the ranges of HbA1c linked with the lowest and highest risk of adverse outcomes, and narrative commentary on consistent or conflicting evidence was used to synthesize these results across different subgroups and curve types. Subgroup comparisons were also discussed (e.g., differences in outcomes by age, sex, and duration of diabetes) where data permitted. Certainty of evidence, assessment of reporting bias, and sensitivity analyses were not conducted due to the descriptive, narrative nature of the synthesis.
Results
Characteristics of included studies
This systematic review included 9 studies, most published in 2021 (n = 4) and followed by 2023 (n = 2). The number of participants varied across different studies, ranging from 411 to 13,543, with follow-up durations varying from 0.5 to 9 years. The total number of participants for this systematic review was 24,978 across various study designs, including retrospective cohort studies, prospective cohort studies, registry-based analyses, and case-cohort studies.
The patient populations primarily consisted of individuals with T2DM undergoing PCI, often with additional comorbidities such as acute coronary syndrome (ACS) or CHD. Glycaemic control groups were categorized based on HbA1c levels where studies stratified HbA1c levels into narrower ranges (e.g., ≤5.5%, 5.5%-6.0%, 6.0%-6.5%, 7.0%-7.5%, etc.), where we defined strict, moderate, and poor control as <6.5%, 6.6%-7.5%, and >7.5% to identify which type of control is associated with better cardiovascular outcomes.
The primary outcomes measured across studies included MACE, cardiovascular mortality, all-cause mortality, Myocardial Infarction, target vessel revascularization, and ischemic stroke. A few studies also evaluated the impact of HbA1c variability on other outcomes such as bleeding events, In-stent restenosis, and peripheral artery disease. Lastly, most of the studies revealed a U-shaped association between HbA1c and cardiovascular outcomes (n = 5), followed by a J-shaped association (n = 1) there were two studies available for threshold curve analysis and one for inverse linear association.
Impact of glycaemic control on cardiovascular outcomes
This review evaluated the impact of strict, moderate, and poor glycaemic control on cardiovascular outcomes. The findings regarding the association of HbA1c ranges with cardiovascular outcomes and mortality were extracted from various studies and presented in Supplement S1.
Strict glycaemic control (HbA1c <6.5%)
Most studies consistently reported poor outcomes and an increased risk of adverse events with strict control. A retrospective study elucidated that patients with HbA1c <6.5% had a significantly higher risk of cardiovascular mortality compared to the reference group (HbA1c 7.0%–7.5%) (HR: 2.97; 95% CI: 1.33–7.25; p = 0.007). The cardiovascular mortality rate was 14.6% in the strict control group, compared to 7.0% in the reference group (moderate control). 16 Similarly, in another retrospective cohort study of 13,543 patients with diabetes, those with HbA1c ≤ 5.5% had a higher risk of all-cause death (HR: 1.57; 95% CI: 1.06–2.32, p <0.05) compared to the reference group (HbA1c 6.1%–7.0%). 18 Further, in a prospective observational cohort study of 2877 patients with T2DM and ACS undergoing PCI. A study showed that patients with HbA1c <6.5% at 2 year post-PCI had a higher incidence of MACE (19.2%) compared to those with HbA1c between 6.5% and 7.0% (10.9%) (p = 0.044). 20 Similarly, in a large multicenter registry of patients with diabetes with acute myocardial infarction undergoing PCI, strict control (HbA1c <6.5%) was associated with significantly higher long-term mortality compared with moderate control (HbA1c 6.5%–7.5%), confirming a J-shaped relationship. 22 In another case-cohort study of 1621 T2DM patients post-PCI, HbA1c <6.5% independently predicted higher MACE risk compared to moderate HbA1c (HR: 1.92; 95% CI: 1.10–3.34; p = 0.021). 13
Moderate glycaemic control (HbA1c 6.5%–7.5%)
Most of the studies consistently reported moderate glycaemic control to be associated with the lowest risk of MACE. For instance, in a prospective study of 2576 patients with DM undergoing PCI, the lowest MACE rates (16.8%) were observed among patients with DM with moderate glycaemic control (HbA1c 6.5%–7.5%) compared to those with tight control (<6.5%: 22.4%) or poor control (>7.5%: 30.2%) (p <0.01). 12 Cardiovascular mortality was also lowest in the moderate control group. Patients with HbA1c between 6.5% and 7.0% had the lowest incidence of MACE (10.9%) compared to those with HbA1c <6.5% (19.2%) or >7.5% (18.4%). 20 Similarly, HbA1c 7.0%–7.5% had the lowest cardiovascular mortality rate (7.0%) compared to both stricter (<6.5%) and poorer (≥8.5%) control groups. 16 In another prospective registry, patients maintaining HbA1c in the moderate range post-PCI had significantly lower long-term MACE and mortality, supporting the J-curve association. 22 Likewise, in a single-centre prospective study, patients maintaining HbA1c between 6.5 and 7.5% had significantly reduced 2year MACE compared with those under strict (<6.5%) or poor (>7.5%) control. 20 Furthermore, in the case-cohort analysis, HbA1c 6.5%–7.5% was associated with the lowest adjusted risk of MACE compared with both lower and higher HbA1c categories. 13
Poor glycaemic control (HbA1c >7.5%)
Poor glycaemic control (HbA1c >7.5%) was consistently linked to increased risks of adverse cardiovascular outcomes, including higher rates of MACE and mortality in the included studies. Patients with poor glycaemic control (HbA1c >7.5%) had the highest MACE rates (30.2%) and cardiovascular mortality compared to those with moderate or strict control. 12 Further, patients with HbA1c ≥8.5% had a higher risk of cardiovascular mortality (HR: 2.15; 95% CI: 0.92–5.27; p = 0.077) compared to the reference group (HbA1c 7.0%–7.5%). 16 Similarly, patients with HbA1c ≥ 8.0% had a higher incidence of MACE (17.1%) compared to those with HbA1c between 6.5% and 7.0% (10.9%). 20 Similarly, in a registry-based study, persistently elevated mean HbA1c levels (>7.5%) following PCI were associated with a progressive increase in long-term mortality and MACE risk. 24 In a prospective cohort, HbA1c >7.5% was significantly associated with higher 2years MACE compared with moderate control. 20 Furthermore, in a mechanistic study of 675 patients undergoing drug-eluting stent implantation, higher HbA1c was associated with increased platelet reactivity, which translated into higher risks of stent thrombosis and adverse cardiovascular events. 15
Key studies demonstrating the U-shaped/J-shaped and other relationship
U-shaped and J-shaped studies
HbA1c ranges for the lowest and highest risk of adverse cardiovascular outcomes and mortality (U-shaped and J-shaped curve).

Abbreviations: HbA1c, glycated haemoglobin; MACE, major adverse cardiovascular events.
Other relationships
HbA1c ranges for the lowest and highest risk of adverse cardiovascular outcomes and mortality (Linear and Threshold relations).

Abbreviations: HbA1c, glycated haemoglobin; MACE, major adverse cardiovascular events.
Discussion
This systematic review evaluated the association between HbA1c levels and risk of MACE among patients with DM. The existing literature reviewed in this study focused on the in-depth and narrow grading of the HbA1c, which is ≤5.5%, 5.6%-6%, 6.1%-7%, 7.1%-8%, and ≥8% 18 rather than published literature from the last decade that divided HbA1c levels in two categories only i.e. <7% and >7% of HbA1c levels.14,25,26 The stratification of HbA1c levels significantly impacted the interpretation of cardiovascular outcomes because broad ranges (<7% and >7% mean HbA1c) do not allow researchers to precisely observe the U-shape or J-shape association among study parameters.27–29 An evaluation of these associations between studies showed that higher risk prevails on both ends of the spectrum, such that HbA1c above 7.5% is linked with the elevation of mortality rates, and low HbA1c levels of around <6.5% can also lead to Myocardial Infarction and high mortality rates in cardiovascular patients undergoing PCI. 30 Literature shows that a median HbA1c value of 6.1% to 7.0% is linked with reduced MACE, mortality, and other cardiac complications. 18
Risk of overly strict glycaemic control
The findings from included studies suggest that strict control may be as harmful as poor control; patients with strict control had a 2.97-fold higher risk of cardiovascular mortality compared to those with moderate control. 16 Similarly, patients with HbA1c <6.5% had a MACE incidence of 19.2%, nearly double that of the moderate control group (10.9%). 20 Further studies showed that overly strict glycaemic control, particularly at the lower end of the spectrum (≤5.3%), is associated with poorer cardiovascular outcomes as compared to strict control (HbA1c 5.3%–5.9%). 31 These findings align with the pre-2019 ACCORD trial, where intensive glycaemic control increased mortality, likely due to hypoglycemia-related events, impaired vascular repair, and increased autonomic instability, especially in patients with pre-existing cardiovascular disease. 32 In contrast, the pre-2019 ADVANCE and its extended follow-up (ADVANCE-ON) trials showed no such increase in mortality, suggesting that the relationship between strict control and outcomes may depend on patient-specific factors, such as age, diabetes duration, and comorbidities. 33 The contrasting results may be attributed to a key difference between the two trials was the rate and intensity of glucose lowering such that ACCORD used aggressive strategies that rapidly reduced glucose levels, while ADVANCE implemented a more gradual, patient-centered approach. Additionally, differences in baseline patient characteristics, such as older age and a higher prevalence of prior cardiovascular disease in ACCORD, also explained the divergent outcomes. These findings suggest that patient factors such as age, diabetes duration, comorbidities, and risk of hypoglycemia also need to be considered when determining glycaemic targets post-PCI.
The consequences of poor glycaemic control
Poor glycaemic control (HbA1c >7.5%) consistently correlated with worse outcomes across recent studies, as presented in the results. High HbA1c levels (>7.5%). Recent evidence corroborates these findings; a large cohort study demonstrated that HbA1c levels above 8.5% were linked to significantly higher mortality and MACE compared with mid-range HbA1c (6.8%-7.5%), reinforcing the harmful impact of chronic hyperglycemia. 34 This review further supports these findings that poor control significantly elevates risks of MACE and mortality, reinforcing that overly lenient targets are detrimental in this population.
Benefits of moderate glycaemic control
The most favorable outcomes were associated with moderate HbA1c levels (6.5%–7.5%), which balance the risks of both hypoglycemia and chronic hyperglycemia (Figure 3). This target range aligns with American Diabetes Association recommendations for individualized HbA1c goals around 7%.
35
Most of the published studies consistently support this range for optimal cardiovascular protection post-PCI.12,18,20,34 Only one study showed contrasting results with a linear inverse relationship, where patients with HbA1c <6.5% had the lowest risk of MACE, and the risk increased with age.
24
This might be due to the difference in patient population, as this study included patients with a history of long-standing diabetes over 10 years. Nevertheless, heterogeneity in how HbA1c categories were defined across studies limits the comparability of findings, and inconsistent cutoffs may have masked or exaggerated observed U- or J-shaped relationships. Optimal HbA1c range linked to the lowest risk of cardiovascular events
Influence of patient characteristics on the target HbA1c range
The relationship between HbA1c and cardiovascular outcomes may vary based on patient-specific variables such as the duration of diabetes, comorbidity status, patient’s age, and sex factors. Incidence of MACE is higher in older patients with strict glycaemic control or higher HbA1c variability than similar conditions implied in younger individuals.20,36 Similarly, longer diabetes duration (>10 years) and comorbidity independently lead to a higher risk of MACE. 36 A study reported that females are at a higher risk of MACE as compared to males. 37 It is recommended that patients monitor their glycaemic levels, especially if they are facing cardiovascular disease, to overcome the subsequent major cardiovascular adverse effects. 28
These findings emphasize that caregivers should set individualized glycaemic targets in clinical practice rather than adopting a “one-size-fits-all” HbA1c goal. Clinicians should consider less aggressive glycaemic targets (e.g., 7%–8%) for older adults, individuals with long-standing diabetes, or those with significant comorbidities. This approach can minimize the risks of hypoglycemia and cardiovascular stress. Conversely, younger and healthier patients may benefit from a more stringent control, provided they can tolerate it without adverse effects. HbA1c variability should be closely monitored, not just the average value, as large fluctuations can be predictive of poor outcomes. Personalized management of patients with DM can improve cardiovascular outcomes, patient safety, and overall quality of life.
Comparison with previous systematic review and meta-analysis
A 2023 systematic review identified a curvilinear (U- or J-shaped) relationship between HbA1c levels and the effectiveness of intensified glycaemic control in patients with type 2 diabetes and coronary heart disease, highlighting that both very low and high HbA1c are associated with adverse outcomes and emphasizing the need for tailored targets taking into account biological profiles and cardiovascular characteristics. 38 Similarly, a prior meta-analysis demonstrated a U-shaped relationship between HbA1c and cardiovascular outcomes post-PCI, with the lowest risk observed at 6.5%–7.0%, although the authors noted their findings were hypothesis-generating and required prospective validation. 39 Our systematic review aligns with both these studies by suggesting a comparable U-shaped association between pre-procedural HbA1c and post-PCI cardiovascular outcomes. However, our review differs by incorporating more recent studies (January 2019 to Jun 2025), applying stricter inclusion criteria focused exclusively on post-PCI populations suffering from DM, and evaluating narrower HbA1c categories. These improvements in the present review expand the available evidence, give a clearer picture of the U- and J-shaped relationships in modern patient groups, and focus specifically on outcomes after PCI, making the findings more useful for clinical practice.
Guideline perspectives and clinical implications
The recent American College of Physicians guidelines prefer less aggressive goals that balance risks and benefits35,40 and recommend relaxing HbA1c targets for patients with DM, which aim to maintain HbA1c levels between 7% and 8% for most individuals to achieve positive clinical outcomes. 41 These recommendations contrast with all the other guidelines of the American Diabetes Association, American College of Endocrinology, National Institute of Health and Care Excellence , and Institute of Clinical System Improvement, which prefer individualized HbA1c levels under 7% for glycaemic management and aim to reduce the risk of cardiac complications.42,43 Endorsing American College of Physicians recommendations, this literature review suggests that HbA1c levels should be maintained under the moderate range, which is around a mean HbA1c of 7%-7.5%, to achieve better clinical outcomes and reduce the MACE among patients with DM after PCI. 16
Limitations
The systematic review has several methodological and evidence-based limitations. Most of the studies were retrospective, thereby having potential selection bias and limiting causal inferences. The consistency of findings was limited due to heterogeneity in HbA1c measurement methods and follow-up duration. Additionally, the lack of RCTs\ further weakens the evidence, as observational studies cannot establish causality.
This analysis was limited to studies published in English between January 2019 to Jun 2025, which may have led to language and time-based publication bias. We also did not perform a meta-analysis due to high data heterogeneity, and as such, quantitative effect size estimation was not possible. Additionally, data from low-income or non-Western regions were underrepresented due to unavailability, which may affect the generalizability of findings. Discrepancies in HbA1c groupings across publications highlight the need for more standardized reporting in future research.
Recommendations
Future research should address the current evidence gaps through well-designed, prospective randomized controlled trials that compare outcomes of strict, moderate, and poor glycaemic control in patients with DM undergoing PCI, ideally stratified by diabetes duration, age groups, sex, and comorbidity status. These trials should avoid rapid glucose lowering, as seen in the ACCORD trial, and instead focus on individualized, patient-centered glycaemic targets.
Further, studies should incorporate advanced glycaemic metrics such as HbA1c variability, time-in-range, and glycaemic burden, preferably through continuous glucose monitoring, to provide a nuanced understanding of long-term glycaemic exposure. There is also a need to explore the impact of sex differences, especially given findings that females may be at greater cardiovascular risk post-PCI. Research should examine whether ethnic and regional variations influence the optimal HbA1c target to support global clinical applicability. Lastly, future reviews should include non-English literature and attempt meta-analysis where feasible, with standardized outcome definitions.
Conclusion
To summarize the above review and discussion, it can be concluded that these studies provide considerable evidence suggesting a non-linear relationship between HbA1c and cardiovascular events, as both lower and higher HbA1c values are associated with an increased risk of major adverse cardiovascular events among patients with DM undergoing PCI. MACE and relevant adverse effects, even in patients with high comorbidity risk, may be mitigated if HbA1c levels are maintained in the optimal or moderate range. This comprehensive approach emphasizes the importance of glycaemic control, highlighting the need for intensive treatment to achieve optimal HbA1c levels, which can contribute to secondary prevention of cardiovascular events and has the potential to enhance treatment outcomes and improve patient care. However, given the heterogeneity of the included studies and the narrative synthesis approach, these findings should be interpreted with caution, and further prospective studies are warranted to confirm these associations.
Supplemental Material
Supplemental material - Hemoglobin A1c Association Patterns with Cardiovascular Outcomes among Patients with Diabetes mellitus Following Percutaneous Coronary Intervention: A Systematic Review
Supplemental material for Hemoglobin A1c Association Patterns with Cardiovascular Outcomes among Patients with Diabetes mellitus Following Percutaneous Coronary Intervention: A Systematic Review by Ayesha Tariq, Zohra Bhatti, Muhammad Nabeel Akbar Chaudary, Madeeha Laghari, Amer Hayat Khan, Nor Ilyani Binti Mohamed Nazar, Bandeh Ali Talpur in Antiviral Therapy.
Supplemental Material
Supplemental material - Hemoglobin A1c Association Patterns with Cardiovascular Outcomes among Patients with Diabetes mellitus Following Percutaneous Coronary Intervention: A Systematic Review
Supplemental material for Hemoglobin A1c Association Patterns with Cardiovascular Outcomes among Patients with Diabetes mellitus Following Percutaneous Coronary Intervention: A Systematic Review by Ayesha Tariq, Zohra Bhatti, Muhammad Nabeel Akbar Chaudary, Madeeha Laghari, Amer Hayat Khan, Nor Ilyani Binti Mohamed Nazar, Bandeh Ali Talpur in Antiviral Therapy.
Footnotes
Ethical considerations
This study is a systematic review of previously published literature and does not involve the collection of new data from human participants or animals. Therefore, ethical approval and informed consent were not required. The review was conducted using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. All sources of data used in this review are publicly available, and appropriate citations have been provided.
Author contributions
Ayesha Tariq led Conceptualization, Methodology, and Writing original draft. Zohra Bhatti and Muhammad Nabeel Akbar Chaudary contributed to literature search, Data curation, and Writing review & editing. Madeeha Laghari and Bandeh Ali Talpur supported literature search, Data curation, and Formal analysis. Nor Ilyani Binti Mohamed Nazar was responsible for Quality assurance and ensuring adherence to PRISMA guidelines throughout the review process. Zohra Bhatti and Amer Hayat Khan provided Supervision and were responsible for the final review and critical editing of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Supplemental Material
Supplemental material is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.