
Abstract
Introduction
Metabolic dysfunction–associated steatotic liver disease (MASLD) is a recognized cardiometabolic risk factor in adults, but its relevance to early vascular remodeling in youth with type 1 diabetes (T1D) remains unclear. We evaluated the independent associations of hepatic fat and body composition with early structural vascular remodeling in youth with T1D.
Methods
This cross-sectional study included 49 late-pubertal youth with T1D (mean age 16.1±2.6 years; duration 7.5±4.3 years). Hepatic fat was quantified using MRI–proton density fat fraction (PDFF), while body composition and estimated insulin sensitivity (eIS) were assessed using dual-energy X-ray absorptiometry and a validated pediatric equation. Carotid intima–media thickness (cIMT), measured by ultrasound, served as the primary outcome. Hierarchical linear regression assessed independent associations after adjustment for age, sex, and diabetes duration.
Results
Mean hepatic fat was 1.87±1.22%, with no participants meeting criteria for steatosis. Hepatic fat, eIS, and diabetes duration were not associated with cIMT. Lean body mass was the primary independent associate of cIMT (β=0.44, p=0.02). Although eIS was strongly associated with waist circumference (r=−0.76, p<0.001), neither variable was associated with cIMT.
Conclusions
In this sub-steatotic cohort, cIMT was primarily associated with lean body mass, reflecting physiologic growth, while central adiposity was associated with metabolic dysfunction but not vascular structure.
Keywords
Key messages
• In youth with type 1 diabetes, hepatic fat is not associated with early vascular structure. • Lean body mass is the primary determinant of carotid intima-media thickness, reflecting physiologic vascular scaling. • Central adiposity is strongly associated with insulin resistance but not vascular remodeling at this stage. • These findings are consistent with a low-hepatic-fat phenotype in this cohort of youth with type 1 diabetes.
1. Introduction
Cardiovascular disease (CVD) is the leading cause of premature mortality in type 1 diabetes (T1D), with structural arterial injury originating as early as adolescence. 1 Longitudinal pediatric cohort data demonstrate that early-onset diabetes confers substantial lifetime cardiovascular risk, underscoring the importance of identifying early determinants of vascular remodeling in youth with T1D.2,3 Carotid intima–media thickness (cIMT) is a well-established surrogate marker of this early remodeling, reflecting the cumulative impact of metabolic stress on the vascular wall. 4 However, in maturing youth, cIMT measurements are also influenced by physiologic growth-related scaling, the proportional expansion of vascular dimensions required to meet the increased metabolic and blood flow demands of developing lean tissue mass (i.e., muscle).5,6 Distinguishing between this healthy scaling and pathologic thickening is essential to accurately characterize early cardiovascular risk in a pediatric population.
In the general population and type 2 diabetes (T2D), metabolic dysfunction–associated steatotic liver disease (MASLD) is strongly associated with cardiovascular disease. 7 This liver-vascular axis appears to extend to adults with T1D, in whom hepatic steatosis is linked to higher cardiovascular risk independent of traditional factors.8,9 Whether this liver-vascular axis is established as early as adolescence in T1D remains unknown. While MASLD is prevalent in pediatric obesity, recent evidence suggests a potential “hepatic-sparing” phenotype in youth with T1D, possibly driven by the peripheral route of insulin delivery and relative portal hypoinsulinemia. 10 However, data characterizing the actual prevalence of MASLD and its subsequent association with cIMT in youth with T1D remain scarce.11,12
In addition, identifying metabolic contributors to cIMT in a growing population requires distinguishing pathologic adiposity from physiologic growth-related vascular scaling. Because BMI does not differentiate between fat and lean mass, direct measures of body composition are essential for accurately evaluating early vascular risk.13,14
Accordingly, this study aimed to quantify hepatic fat and evaluate its association with cIMT relative to systemic body composition in youth with T1D. The primary objectives were to determine the prevalence of MASLD using magnetic resonance imaging and to assess the independent relationships between hepatic lipid, body composition, and metabolic markers with early structural vascular remodeling.
2. Methods
2.1. Study population
This cross-sectional study included 49 adolescents and young adults with type 1 diabetes (T1D), recruited via convenience sampling from outpatient diabetes clinics at UPMC Children’s Hospital of Pittsburgh between March 2024 and February 2025. Eligibility criteria included T1D duration ≥2 years and late-pubertal maturation (Tanner stage IV or higher) determined by physical examination. Restricting the cohort to late puberty minimized the confounding effects of rapid growth and hormonal variability on vascular structure and body composition.
Exclusion criteria included a history of hypertension, chronic liver disease (e.g., viral or autoimmune hepatitis), contraindications to MRI, or use of medications affecting blood pressure or hepatic lipid metabolism. Participants were not excluded based on suspected MASLD; hepatic fat was assessed de novo to determine its prevalence. Recruitment was structured to include representation across BMI categories (normal weight, overweight, and obese), ensuring a broad distribution of adiposity and lean body mass.
The study protocol was approved by the University of Pittsburgh Institutional Review Board. Written informed consent or parental consent with participant assent was obtained from all participants.
2.2. Clinical, imaging, and laboratory assessments
All participants underwent metabolic, hepatic, body composition, and vascular assessments within 12 weeks of study enrollment.
2.3. Statistical analysis
Statistical analyses were descriptive and hypothesis-generating given the cross-sectional design and sample size (N=49). The primary outcome was mean cIMT (mm). Participant characteristics were summarized as means and standard deviations. Pearson correlation coefficients were used to examine bivariate associations between cIMT and variables related to body composition, metabolic status, glycemic control, and hepatic fat.
Hierarchical multivariable linear regression was used to assess associations with cIMT while accounting for physiologic growth. Model 1 included age, sex, diabetes duration, and DEXA-derived lean body mass (kg). Model 2 introduced adiposity measures (MRI-PDFF, BMIz, percent body fat, or waist circumference) in separate models to assess their associations after adjustment for lean body mass. This approach reduced multicollinearity across adiposity measures. Variance inflation factors were evaluated to confirm the absence of significant multicollinearity (VIF<2).
With a sample size of 49, the study was powered to detect moderate-to-large correlations (r≥0.39) with 80% power. All findings were interpreted as exploratory. Statistical tests were two-tailed with a significance level of α=0.05 and were performed using IBM SPSS Statistics, version 29.
3. Results
Demographic and clinical characteristics of youth and young adults with type 1 diabetes (N = 49).
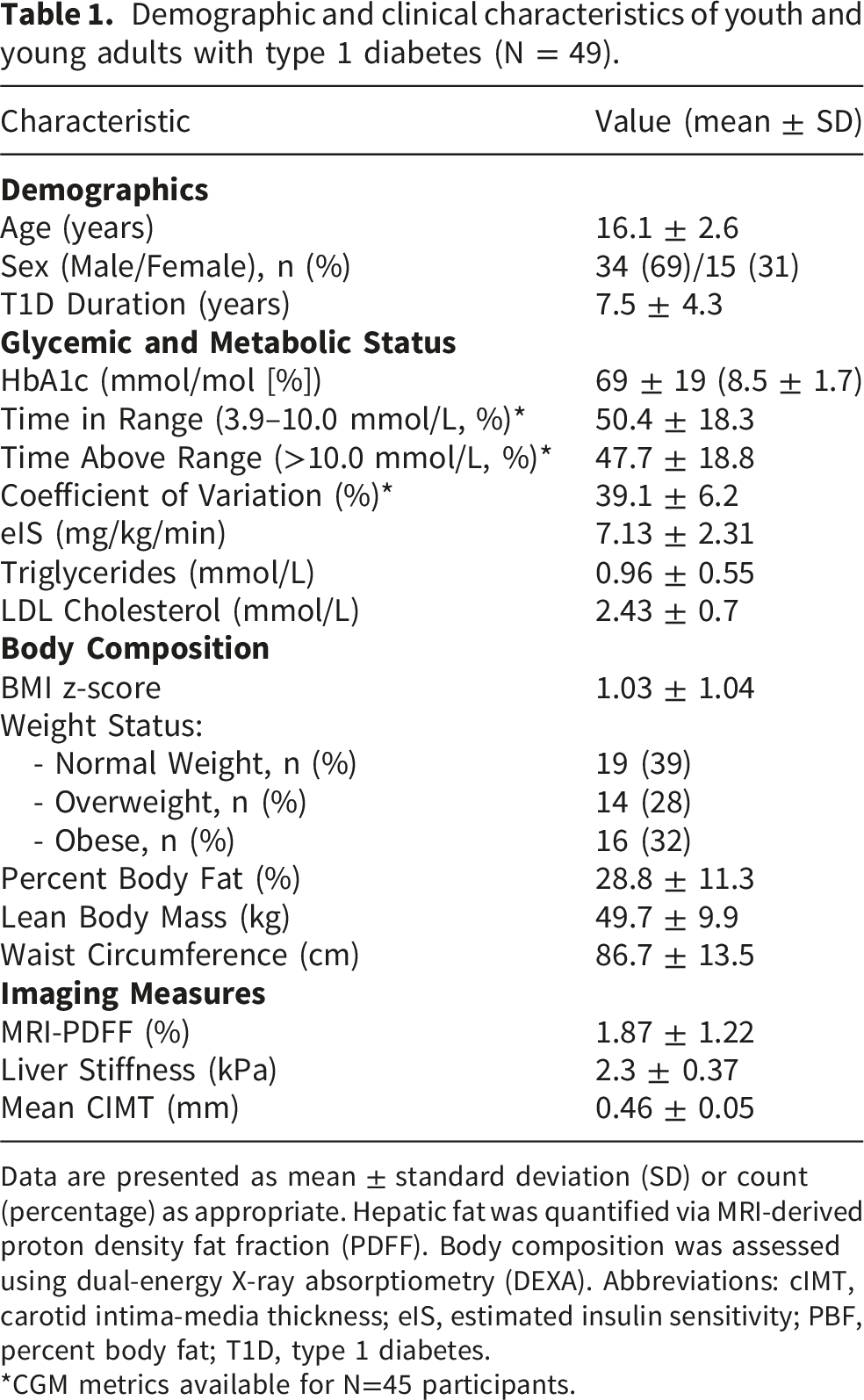
Data are presented as mean ± standard deviation (SD) or count (percentage) as appropriate. Hepatic fat was quantified via MRI-derived proton density fat fraction (PDFF). Body composition was assessed using dual-energy X-ray absorptiometry (DEXA). Abbreviations: cIMT, carotid intima-media thickness; eIS, estimated insulin sensitivity; PBF, percent body fat; T1D, type 1 diabetes.
*CGM metrics available for N=45 participants.
Bivariate pearson correlations between cardiometabolic predictors and primary outcomes.
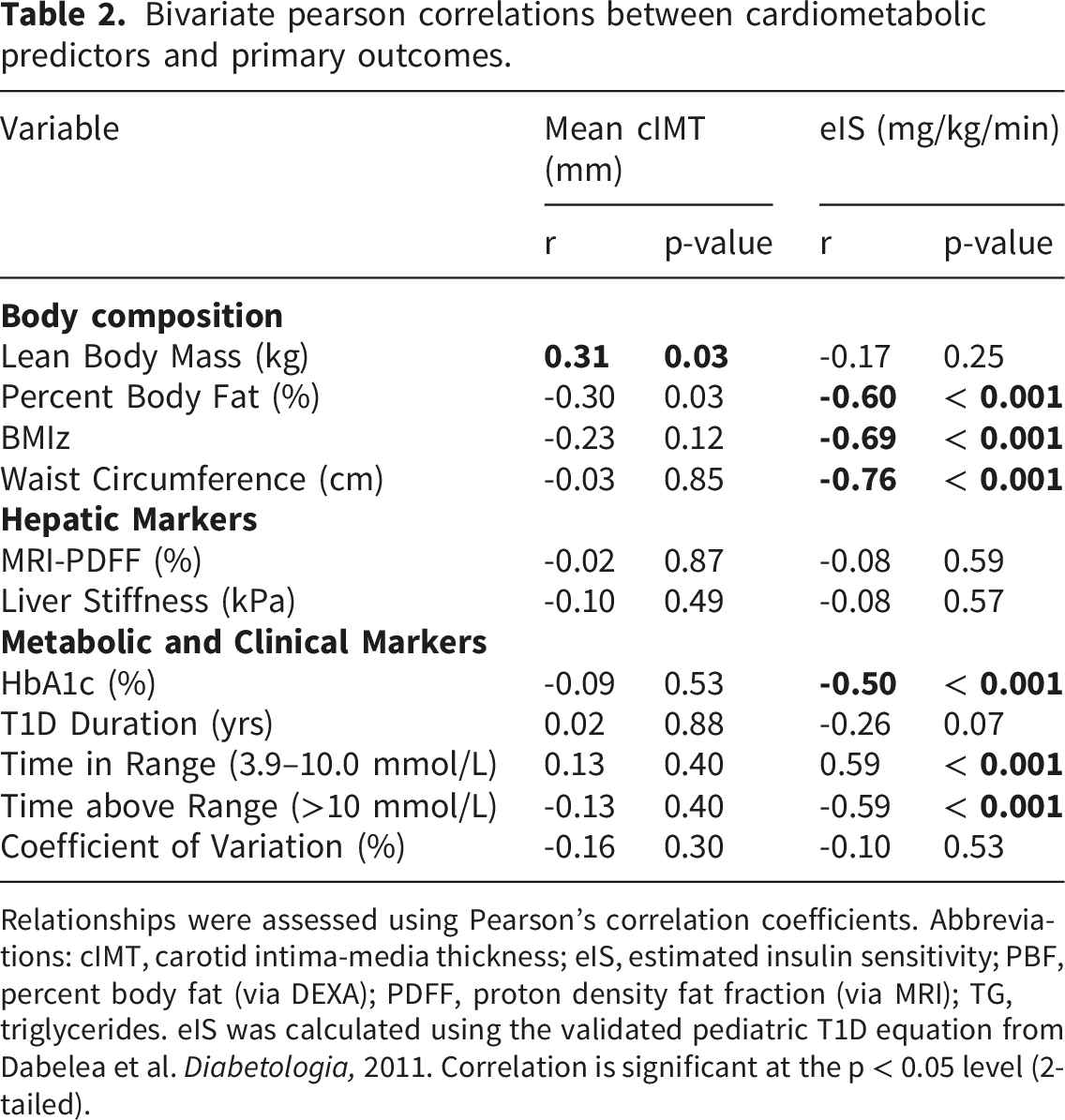
Relationships were assessed using Pearson’s correlation coefficients. Abbreviations: cIMT, carotid intima-media thickness; eIS, estimated insulin sensitivity; PBF, percent body fat (via DEXA); PDFF, proton density fat fraction (via MRI); TG, triglycerides. eIS was calculated using the validated pediatric T1D equation from Dabelea et al. Diabetologia, 2011. Correlation is significant at the p < 0.05 level (2-tailed).
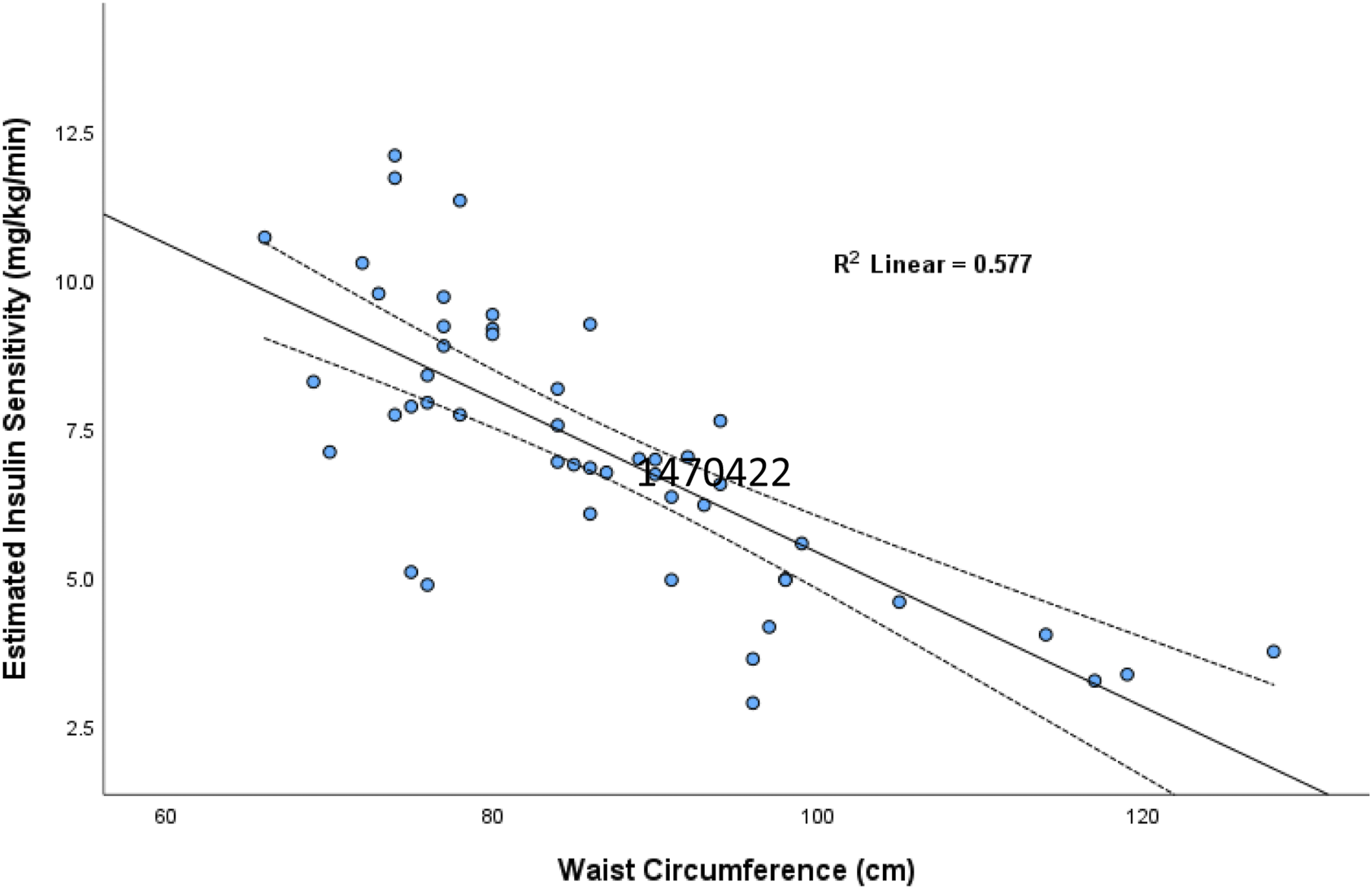
Relationship Between Central Adiposity and Insulin Sensitivity. Scatter plot showing the relationship between waist circumference and estimated insulin sensitivity (eIS) (r=−0.76, R2=0.577, p<0.001). The solid line represents the linear regression fit, and dashed lines indicate the 95% confidence interval.
Hierarchical Linear Regression Models for Mean cIMT.
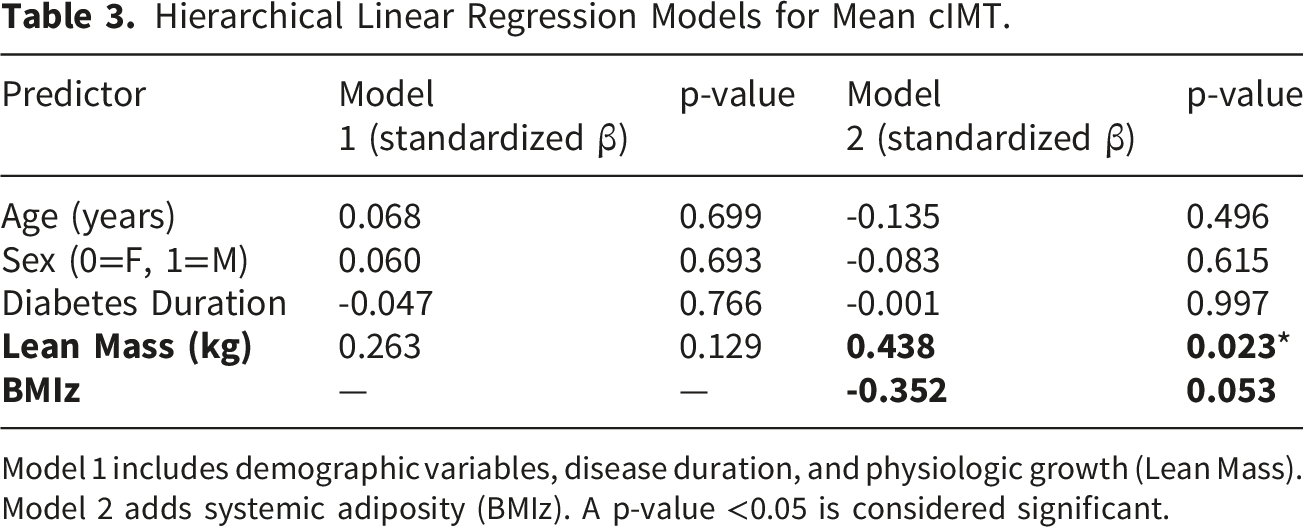
Model 1 includes demographic variables, disease duration, and physiologic growth (Lean Mass). Model 2 adds systemic adiposity (BMIz). A p-value <0.05 is considered significant.
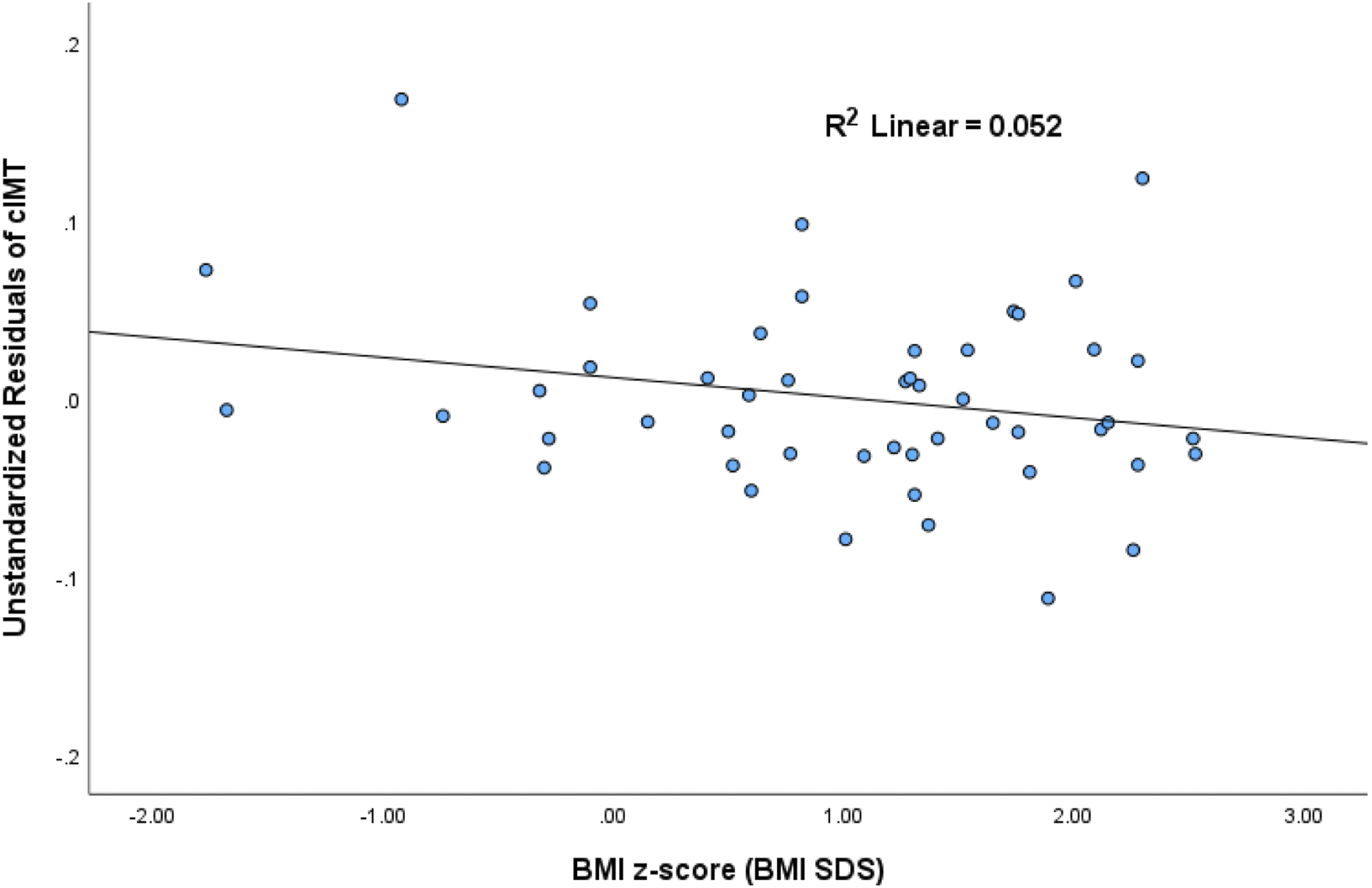
Partial Regression Plot of BMI z-score and Carotid Intima–Media Thickness. Partial regression plot showing the relationship between BMI z-score and the residuals of carotid intima–media thickness (cIMT) after adjustment for age, sex, diabetes duration, and lean body mass (R2=0.052, p=0.053).
Diabetes duration was not associated with cIMT in any multivariable model (all p>0.75). MRI-PDFF, percent body fat, and waist circumference were also not associated with cIMT in multivariable analyses (Supplementary Tables S1–S3). Categorical analysis by hepatic fat tertiles showed similar results, with mean cIMT nearly identical in the lowest (0.46 ± 0.05 mm) and highest (0.46 ± 0.05 mm) tertiles (p = 0.74; Figure 3). Carotid Intima–Media Thickness Across Hepatic Fat Tertiles. Mean carotid intima–media thickness (cIMT) categorized by MRI-derived hepatic proton density fat fraction (PDFF) tertiles: Tertile 1 (low), Tertile 2 (mid), and Tertile 3 (high). Error bars represent 95% confidence intervals (p=0.74).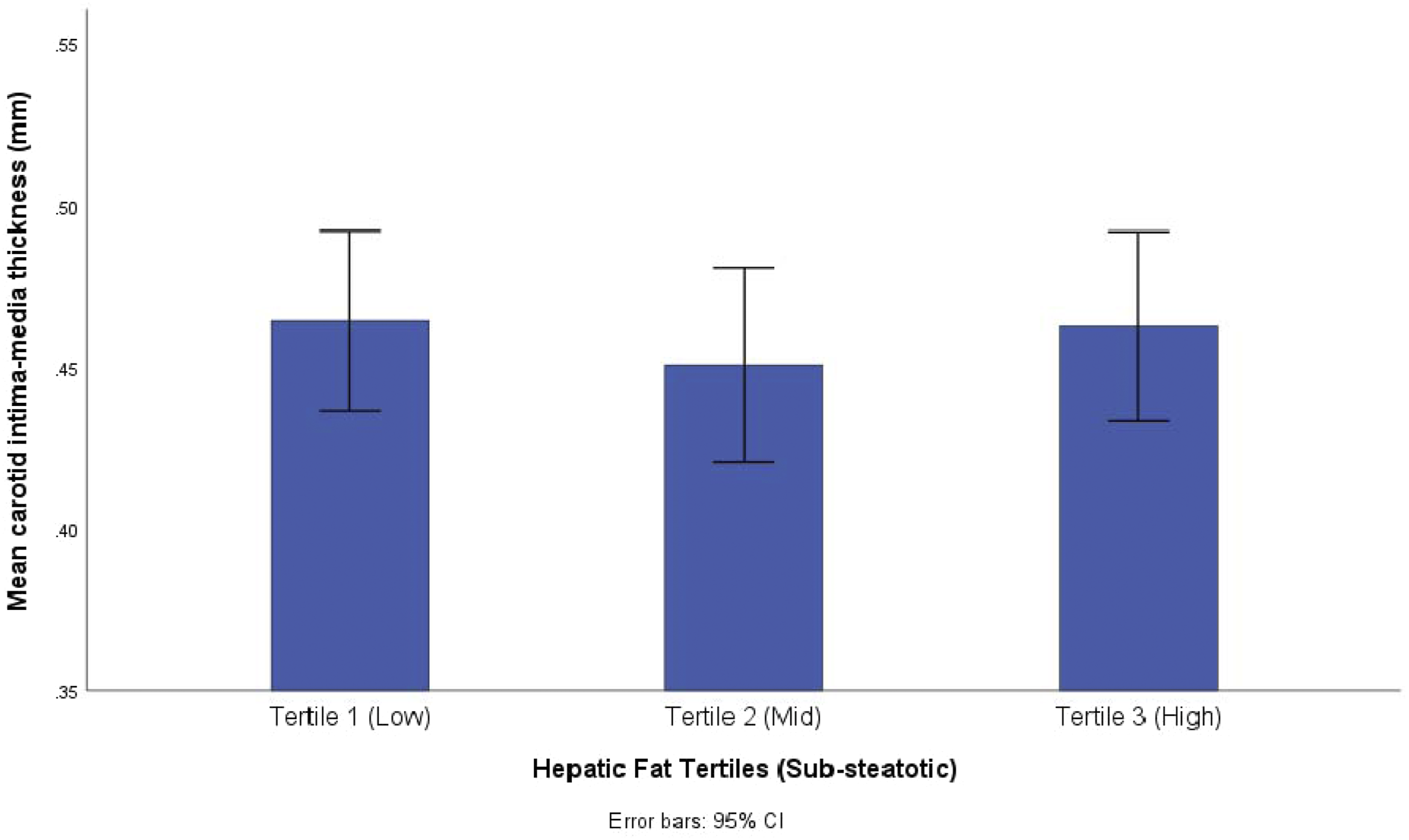
4. Discussion
In this study of youth and young adults with T1D, we identified a dissociation between hepatic lipid accumulation and early markers of cardiovascular and metabolic risk. While the relationship between MASLD and cardiovascular injury is well established in T2D and adult populations, our findings address whether this axis is present in youth with T1D. In this cohort, intrahepatic fat and liver stiffness were within a sub-steatotic range and were not associated with vascular structure (cIMT) or insulin sensitivity (eIS).
Instead, vascular dimensions were primarily associated with lean body mass (i.e., physiologic growth), whereas central adiposity, measured by waist circumference, was the strongest correlate of metabolic dysfunction. After accounting for body size in hierarchical models, lean mass remained the sole independent associate of cIMT, while BMIz demonstrated an inverse trend. These findings suggest that, in early T1D, vascular structure reflects physiologic growth-related scaling rather than pathologic thickening driven by adiposity, insulin resistance, or hepatic lipid accumulation.
Several considerations are essential for contextualizing these findings. In this cohort, hepatic fat content was uniformly below the established 5% threshold for steatosis, with a mean PDFF of only 1.87%. Rather than contradicting the well-characterized liver–cardiovascular axis observed in adult or T2D populations, 7 our data suggest this pathological axis may not yet be prominent in youth with T1D until a greater degree of hepatic lipid accumulation or systemic metabolic dysfunction is reached.
The low liver fat burden observed in our cohort should be interpreted in the context of previous pediatric T1D studies reporting higher rates of steatotic liver disease. In a prior study from our group using vibration-controlled transient elastography, obesity rather than T1D status was the primary determinant of hepatic steatosis, and obese youth with T1D demonstrated imaging and clinical profiles similar to BMI-matched obese youth without diabetes. 20 Similarly, Maffeis et al. reported a MASLD prevalence of 27.5% in a large cohort of youth with T1D and identified long-term glycemic exposure and adverse cardiometabolic profiles as independent predictors of MASLD. 21 Differences in participant characteristics, imaging methodology, and underlying liver fat burden may explain the markedly lower hepatic fat content observed in the present MRI-PDFF cohort. Collectively, these findings suggest that hepatic steatosis is not an inevitable feature of youth-onset T1D and may be influenced more strongly by obesity and broader cardiometabolic risk factors than by diabetes status alone.
The relatively low intrahepatic lipid content observed despite a broad range of adiposity is consistent with the hypothesis that peripheral insulin delivery and relative portal hypoinsulinemia in T1D may limit hepatic de novo lipogenesis.10,22,23 As a result, the liver may be relatively protected from early lipotoxic pathways implicated in vascular injury in obesity and T2D. 24 In our cohort, central adiposity was strongly associated with insulin resistance, whereas neither hepatic fat nor insulin resistance was associated with cIMT. Together, these findings suggest that central adiposity may be more closely related to metabolic dysfunction than hepatic lipid accumulation during this stage of disease.25,26
Beyond hepatic factors, our study highlights the importance of distinguishing physiologic growth from pathologic adiposity when interpreting vascular structure in youth. After accounting for body size via hierarchical modeling, lean body mass emerged as the primary independent correlate of cIMT (β = 0.44, p = 0.02), while BMIz demonstrated a paradoxical inverse trend. This pattern aligns with the arterial scaling hypothesis, which posits that vascular dimensions in growing children primarily reflect the expansion of lean tissue (i.e., muscle) to meet increased metabolic and blood flow demands.5,27 Metabolic effects of adiposity are likely to superimpose on this structure later in the disease course. Failure to account for physiologic growth-related scaling may obscure true relationships between body composition and vascular structure, potentially leading to misclassification of normal arterial growth as early atherosclerotic disease.19,27
Our results offer a meaningful context when compared to the SEARCH CVD Study, the largest evaluation of cIMT in youth with T1D. 28 While SEARCH CVD reported significantly thicker carotid bulb IMT in youth with T1D (cases) compared to healthy controls (0.461 vs. 0.445 mm, p = 0.01), the mean common cIMT in our cohort (0.46 ± 0.05 mm) aligns more closely with their healthy control mean for the common segment (0.450 ± 0.067 mm). This result is also identical to the mean reported in a large, population-based study of 314 youth with T1D, which found a mean common segment cIMT of 0.46 ± 0.06 mm in boys with T1D and 0.43 ± 0.05 mm in girls with T1D. 29 In that cohort, despite a relatively short disease duration (mean 5.5 years), cIMT in 13.1% of participants already exceeded the 95th percentile threshold of healthy controls (p <0.001). This supports the presence of an early remodeling phenotype in youth with T1D.
Furthermore, the mean eIS in our cohort (7.13 ± 2.31 mg/kg/min) reflects a state of diminished insulin sensitivity compared to healthy controls in other studies.30,31 This level of metabolic strain is comparable to the mid-to-lower ranges observed in the SEARCH study, particularly among youth with increasing central adiposity. 15 The robust inverse correlation between waist circumference and eIS (r = -0.76, p <0.001) underscores that visceral fat accretion is a major contributor to metabolic dysfunction in this population. However, neither eIS nor waist circumference was associated with cIMT, suggesting that metabolic abnormalities may precede detectable structural vascular changes in this relatively young cohort. This observation is consistent with the concept that insulin resistance and excess adiposity may emerge before measurable arterial remodeling becomes evident in youth with T1D.
A major strength of this study is the use of multi-modal phenotyping, including MRI-PDFF and DEXA, enabling precise differentiation between hepatic lipid, lean mass, and adiposity. The inclusion of CGM-derived metrics and estimated insulin sensitivity (eIS) provides a more comprehensive assessment of metabolic status than HbA1c alone.
However, several limitations must be acknowledged. First, the cross-sectional design precludes causal inference regarding the temporal progression of vascular remodeling. Second, the limited range of hepatic fat prevented evaluation of clinically significant MASLD. Third, while our modest sample size (N = 49) was sufficient to identify robust associations with lean mass and waist circumference, it may have lacked the power to detect subtle associations between minor hepatic lipid variation and vascular structure. Fourth, the absence of a comparison group without diabetes limits our ability to determine whether the low hepatic fat burden and vascular findings observed in this cohort represent a T1D-specific phenotype or reflect broader physiologic patterns during adolescence. Finally, while traditional cIMT measurements reflect cumulative structural remodeling influenced by growth,6,19 emerging ultra-high-frequency ultrasound techniques suggest that intima-specific changes may be more sensitive to short-term glycemic variability in youth with T1D than the mean cIMT values reported here. 32
Future research should utilize longitudinal designs to determine when the low hepatic fat burden observed in this cohort may be superseded by chronic overnutrition and whether a hepatic fat “tipping point” exists in youth with T1D. Overall, our findings support a metabolic–vascular architecture in this cohort of youth with T1D in which early vascular structure appears to be shaped primarily by physiologic growth and body composition rather than hepatic lipid accumulation or disease duration. These findings suggest that early cardiovascular risk reduction in T1D should prioritize healthy body composition and prevention of central adiposity.
5. Conclusion
In youth with T1D and sub-steatotic hepatic fat levels, intrahepatic lipid content is not associated with arterial structure or insulin sensitivity. Instead, body composition follows two distinct pathways: lean body mass governs structural vascular dimensions (i.e., cIMT) via physiological growth scaling, while central adiposity serves as the primary associate of metabolic strain. Notably, central adiposity was associated with diminished insulin sensitivity but remained independent of vascular structure.
These findings are consistent with a low-hepatic-fat phenotype in youth with T1D in which vascular structure appears more closely related to physiologic growth than to ectopic liver fat accumulation. Longitudinal studies are needed to determine whether increasing hepatic fat burden contributes to cardiovascular risk as cardiometabolic dysfunction evolves over time.
Supplemental material
Supplemental material - Body composition rather than liver fat associates with carotid Intima–Media thickness in youth with type 1 diabetes
Supplemental material for Body composition rather than liver fat associates with carotid Intima–Media thickness in youth with type 1 diabetes by Emir Tas, Memduha Gumus, Swetha Movva, Brenda Mendizabal, Emma Barinas-Mitchell, Zhenwei Gong, Jonathan A. Dranoff, Radhika Muzumdar and Ingrid Libman in Diabetes & Vascular Disease Research.
Footnotes
Acknowledgments
The authors thank the participants and their families for their involvement in this study.
Ethical considerations
The study protocol was approved by the University of Pittsburgh Institutional Review Board.
Consent to participate
Written informed consent or parental consent/participant assent was obtained from all participants.
Author Contributions
Emir Tas: Conceptualization; Methodology; Formal analysis; Data curation; Writing – original draft; Project administration. Memduha Gumus: Investigation; Writing – review & editing. Swetha Movva: Investigation; Data curation; Writing – review & editing. Brenda Mendizabal: Investigation; Writing – review & editing. Zhenwei Gong: Investigation; Data curation; Writing – review & editing. Emma Barinas-Mitchell: Methodology; Supervision; Writing – review & editing. Jonathan A. Dranoff: Methodology; Writing – review & editing. Radhika Muzumdar: Conceptualization; Supervision; Writing – review & editing. Ingrid Libman: Conceptualization; Supervision; Writing – review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the institutional Children's Hospital of Pittsburgh of the UPMC Health System awarded to Dr. Emir Tas.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.