
Abstract
Introduction
The American Thoracic Society (ATS) six-minute walk test (6MWT) guidelines recommend repeat testing at the same time of day to minimise intraday variability. Whether diurnal or seasonal factors affect the 6MWT in pulmonary hypertension (PH) is unclear. We investigated associations between six-minute walk distance (6MWD) and secondary 6MWT parameters with time of day and season using cross sectional and longitudinal analyses.
Methods
This single-centre retrospective study (2019–2025) included PH patients undergoing 6MWT as per ATS guidelines. Cross-sectional analyses compared morning (AM, 07:00–12:00) vs afternoon (PM, 12:01–18:00) and seasonal effects on 6MWD using adjusted linear models. Longitudinal effects were examined with adjusted linear mixed effects models.
Results
The cross-sectional cohort included 1,665 patients (AM n=734, PM n=931). Estimated marginal mean (EMM) 6MWD was higher in the morning than afternoon (354m vs 339m; p=0.005), with no seasonal variation (Winter 338m, Spring 354m, Summer 345m, Autumn 343m; p=0.20). The longitudinal cohort included 554 patients. EMM 6MWD was similar between AM and PM (396m vs 400m; p=0.16) and across seasons (Winter 395m, Spring 395m, Summer 399m, Autumn 398m; p=0.43). Maximal heart rate (MHR) was higher in the afternoon (115 vs 113 bpm; p=0.002) and lower in Summer/Autumn (113 bpm) vs Winter (116 bpm) and Spring (115 bpm; p=0.017).
Conclusion
6MWD was stable across time of day and season, supporting greater flexibility in scheduling 6MWTs than suggested by guidelines. Small variations in MHR were associated with circadian and seasonal influences but did not affect 6MWD. Prospective studies are needed to confirm these findings.
Introduction
The six-minute walk test (6MWT) is a widely used across chronic respiratory disease populations, including chronic obstructive pulmonary disease (COPD) and interstitial lung disease (ILD) to evaluate functional capacity and track clinical change over time. Understanding extrinsic sources of variability such as time of day and seasonal effects is important to support interpretation of longitudinal follow up and research outcomes. Specifically in pulmonary hypertension (PH) is important in assessment of treatment response. 1 The primary outcome, six-minute walk distance (6MWD), correlates with prognosis, haemodynamics, and World Health Organisation (WHO) functional class.2–4 It is recommended as both a primary endpoint in clinical trials and as a key parameter in clinical follow-up of patients in international PH guidelines.1,5,6
Although the 6MWT is simple and reproducible, its performance can be influenced by patient and environmental factors, including motivation, comorbidities, and testing conditions.4,7 Recognising this, the 2002 American Thoracic Society (ATS) guidelines advise performing repeat tests at the same time of day to minimise intraday variability. 8 In healthy populations, exercise capacity and ventilatory function often follow a circadian pattern, with superior performance in the afternoon compared with the morning,9–11 attributed to diurnal changes in muscle function, lung mechanics, body temperature, and hormonal fluctuations. This has not always seen with 6MWD, where in contrast, studies in elderly or chronically ill patients have reported inconsistent findings, with some showing no clear time of day effect on 6MWD.12–14
In PH, the potential influence of diurnal variation on 6MWD has not been directly investigated Given that fatigue a hallmark of PH15–17 tends to worsen throughout the day. This could negatively impact afternoon 6MWD performance and introduce confounding in longitudinal follow up and assessment in clinical trials, relative to prior morning tests. While ATS guidelines already recommend same-time testing, 8 the evidence base supporting this practice in PH remains limited.
Another potential but overlooked source of variability in 6MWT performance is seasonal variation. Several studies in PH, COPD and heart failure have shown that physical activity levels are generally lower during colder months, which may translate into reduced exercise capacity18–21 and therefore supports the need for direct studies on 6MWT performance across seasons. There is evidence from a study using implantable technology that suggests that passive actigraphy data may be affected by seasonality in PH cohorts. 18 Given the evidence that daily activity levels vary across seasons, further studies are needed to confirm whether 6MWD remains stable throughout the year. Establishing this would help inform future 6MWT guidelines, which currently do not address seasonal effects, and would be important to determine accurate longitudinal follow-up in PH patients.
Therefore, the aim of this study is to examine, in a PH cohort, both cross-sectional and longitudinal effects of time of day and season on 6MWD, as well as the impact on secondary 6MWT parameters including heart rate.
Method
Study design
This was a retrospective real-world study at Royal Papworth Hospital (Cambridge, UK), a tertiary PH specialist centre. The study was approved by the Papworth Cardiorespiratory Physiology Research Database (PCRPRD) data access committee (Reference: PCRPRD0006, IRAS: 346834).
Data was collected between 2019-2025 for patients diagnosed with PH who had completed a routine clinical 6MWT. Clinical data collected for the analysis included demographics (age and sex), body mass index (BMI), World health organisation (WHO) PH group, WHO functional class and for those with chronic thromboembolic pulmonary hypertension (CTEPH), a history of pulmonary endarterectomy (PEA) surgery or balloon pulmonary angioplasty (BPA). To ensure inclusion of patients with persistent pulmonary hypertension, only post-PEA/BPA individuals with a mean pulmonary artery pressure > 20 mmHg were included in the analyses. Study design was as follows. Time of day was classified as morning (AM, 07:00–12:00) and afternoon (PM, 12:01–18:00). Seasons were defined according to UK meteorological convention: Winter (December–February), Spring (March–May), Summer (June–August), and Autumn (September–November). The longitudinal analysis included patients who had completed repeated 6MWTs over time and had at least one AM and one PM measurements.
6MWT method
The 6MWT was performed on a 30-metre indoor corridor, with patients instructed to walk as far as possible in six minutes, in accordance with American Thoracic Society/European Respiratory Society technical standards.8,22 Standardised instructions and encouragement were provided. Patients were permitted to slow or stop and rest as required. All tests were conducted in the same corridor environment, with ambient temperature maintained between 21–22°C. In routine clinical practice, a single 6MWT was performed at each visit. From 2019 to 2022, oxygen saturation (SpO2) and heart rate (HR) were measured using the Masimo Rad-5® (Masimo Corporation, Irvine, California, USA). From 2022 to 2025, measurements were captured using the Nonin PalmSAT® 2500 (Nonin Medical, Inc., Plymouth, Minnesota, USA) with a reusable forehead reflectance sensor. Values were recorded every 30 seconds during the test. Perceived breathlessness was assessed pre and post-test using the Borg Category-Ratio 0–10 Scale (CR10). 23
Statistical analysis
Statistical significance was set at p<0.05. Statistical analyses were performed using Jamovi version 2.6.44 and STATA version 18.0. Data was presented as either mean ± standard deviation (SD) or median and interquartile range (IQR). Data normality was tested by using histograms, Q-Q plots and Shapiro-Wilk test.
For cross-sectional analyses, cohort characteristics were compared between AM and PM tests, as well as across seasons. Age and BMI were analysed using independent-samples t-tests, while categorical variables (sex, WHO functional class, PH diagnosis, and intervention status (PEA or BPA)) were compared using chi-squared tests. The effect of time of day (AM vs PM) on 6MWD was examined using linear regression model, adjusting for age, sex, BMI, WHO functional class, and WHO PH disease classification and mechanical intervention (BPA/PEA) status. Similarly, an adjusted linear regression model was conducted to evaluate the effect of season on 6MWD. Given significant main effects for time of day, separate interaction terms were further explored (AM vs PM × PH subtype; AM vs PM × WHO class). To assess subgroup effects, two-way ANOVAs were performed to evaluate the impact of time of day on 6MWD across PH subtypes and across WHO functional classes (mild [FC I], moderate [FC II], and severe [FC III–IV]). Post-hoc pairwise comparisons were conducted following significant ANOVA results to identify specific group differences.
For longitudinal analyses, linear mixed-effects models were used to examine the effects of time of day and season on 6MWD and secondary 6MWT parameters. Separate models were constructed for time of day and for season. Each model included a random intercept for patients and a random slope for the variable of interest (AM vs PM or season) to account for within-subject variability across repeated measures. Models were adjusted for demographic variables (age, sex, BMI), PH diagnosis, and WHO functional class (mild [FC I], moderate [FC II], severe [FC III–IV]). An interaction term (WHO functional class × time of day) was also included. Since BPA or PEA could act as potential confounders of the association between time of day or season and 6MWD, intervention status was included in the model as a time-varying covariate. An interaction term between time of day and intervention status was also applied to test to assess whether the effect of time of day on 6MWD differed according to intervention status. Time from 1st 6MWT visit was included to control for potential effects of disease progression over the follow-up period. Season and time of day (AM vs PM) were included as fixed covariates in the models.
Results
Cross sectional analysis
Demographics of the cross-sectional cohort AM vs PM.
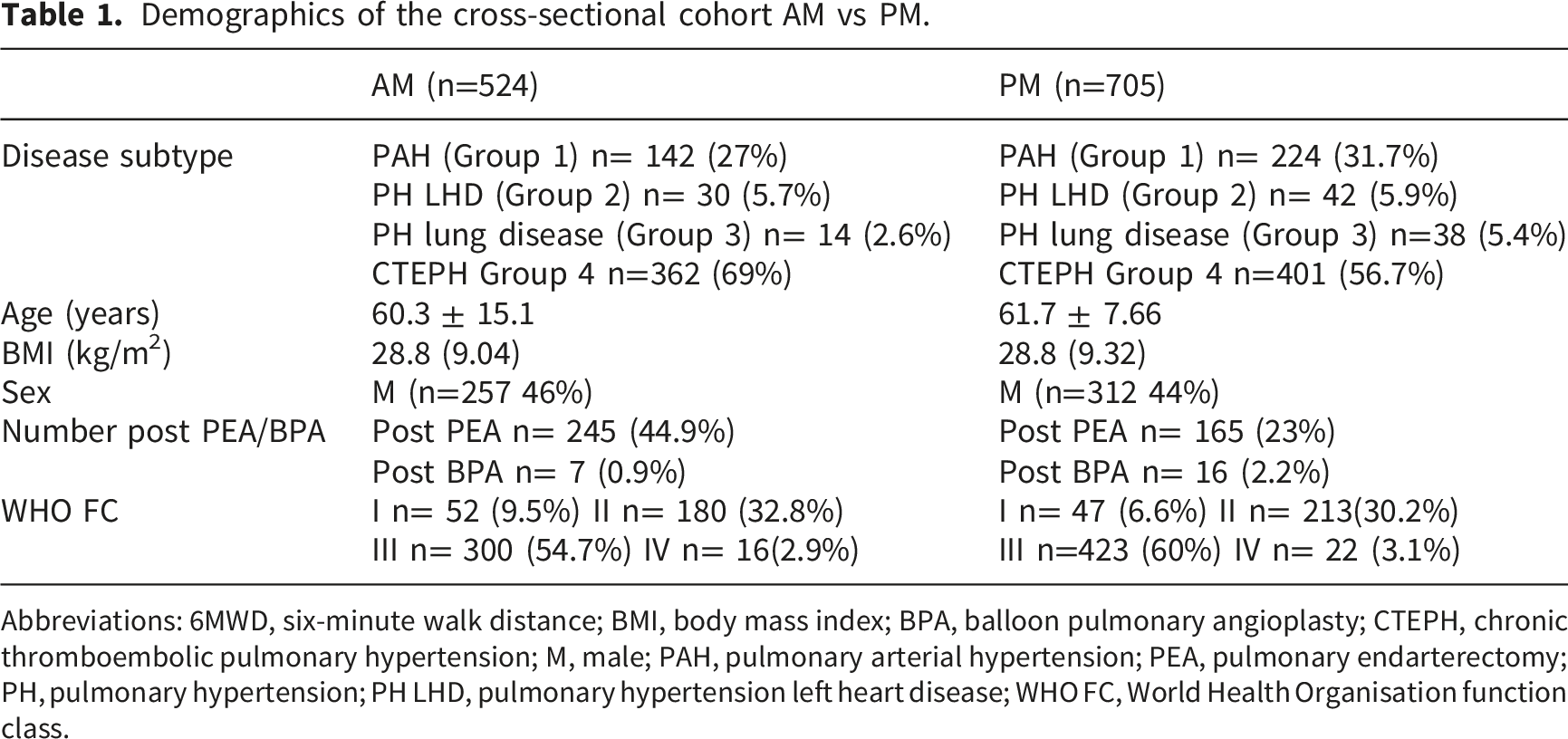
Abbreviations: 6MWD, six-minute walk distance; BMI, body mass index; BPA, balloon pulmonary angioplasty; CTEPH, chronic thromboembolic pulmonary hypertension; M, male; PAH, pulmonary arterial hypertension; PEA, pulmonary endarterectomy; PH, pulmonary hypertension; PH LHD, pulmonary hypertension left heart disease; WHO FC, World Health Organisation function class.
6MWD difference between AM vs PM for whole cross-sectional cohort
There was a significant effect for time of day with patients walking further in the morning compared with the afternoon (p=0.005) which corresponded to a small effect size (partial η2 = 0.004). The adjusted mean 6MWD was 339 m (95% CI: 331-348) for the AM cohort and 322 m (95% CI: 314-330) for the PM cohort, a 17-m difference (see Figure 1). (a). Estimated marginal means (95% CI) AM vs PM cross sectionally for whole PH cohort. (b): Estimated marginal means (95% CI) for seasonal effects cross sectionally for the whole PH cohort.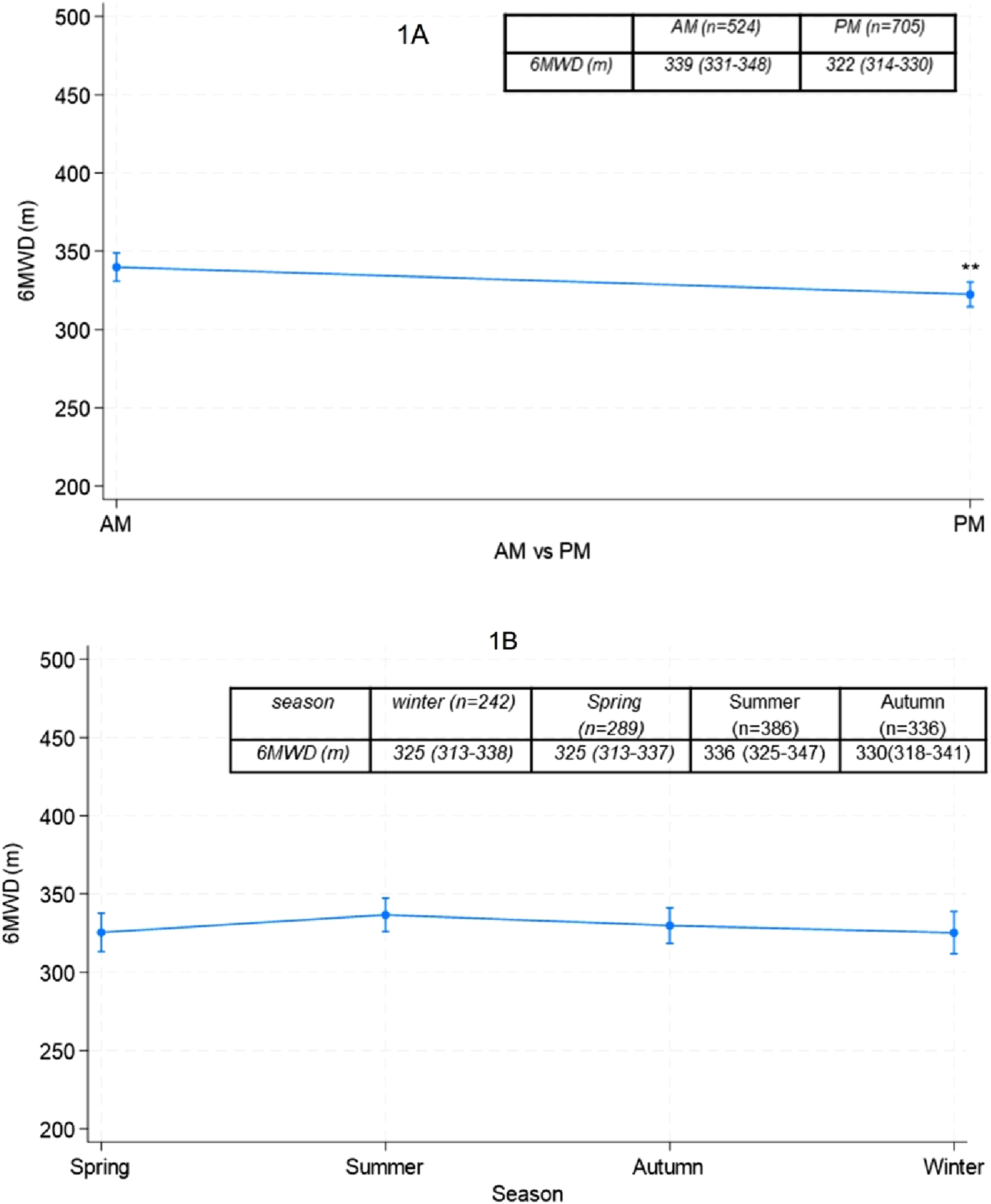
6MWD AM vs PM by PH disease classification
A two-way ANOVA was performed to investigate the effect of time of day on 6MWD across PH disease classification and the interaction was not significant F= 0.24 (p = 0.14). See supplementary Figure 1 for estimated marginal means for 6MWD across PVD disease subtypes AM vs PM (supplementary Figure 1).
6MWD AM vs PM by WHO functional class
There was no significant interaction between time of day and WHO functional class on 6MWD (p =0.138). Although a small numerical decrease in afternoon 6MWD was observed in patients with moderate-to-severe functional class (WHO II–IV), this difference did not reach statistical significance, suggesting that the effect of time of day on walking performance was consistent across functional classes. See Supplementary Figure 2.
6MWD difference across seasons cross sectional cohort
Demographics of the cross-sectional cohort across the seasons.
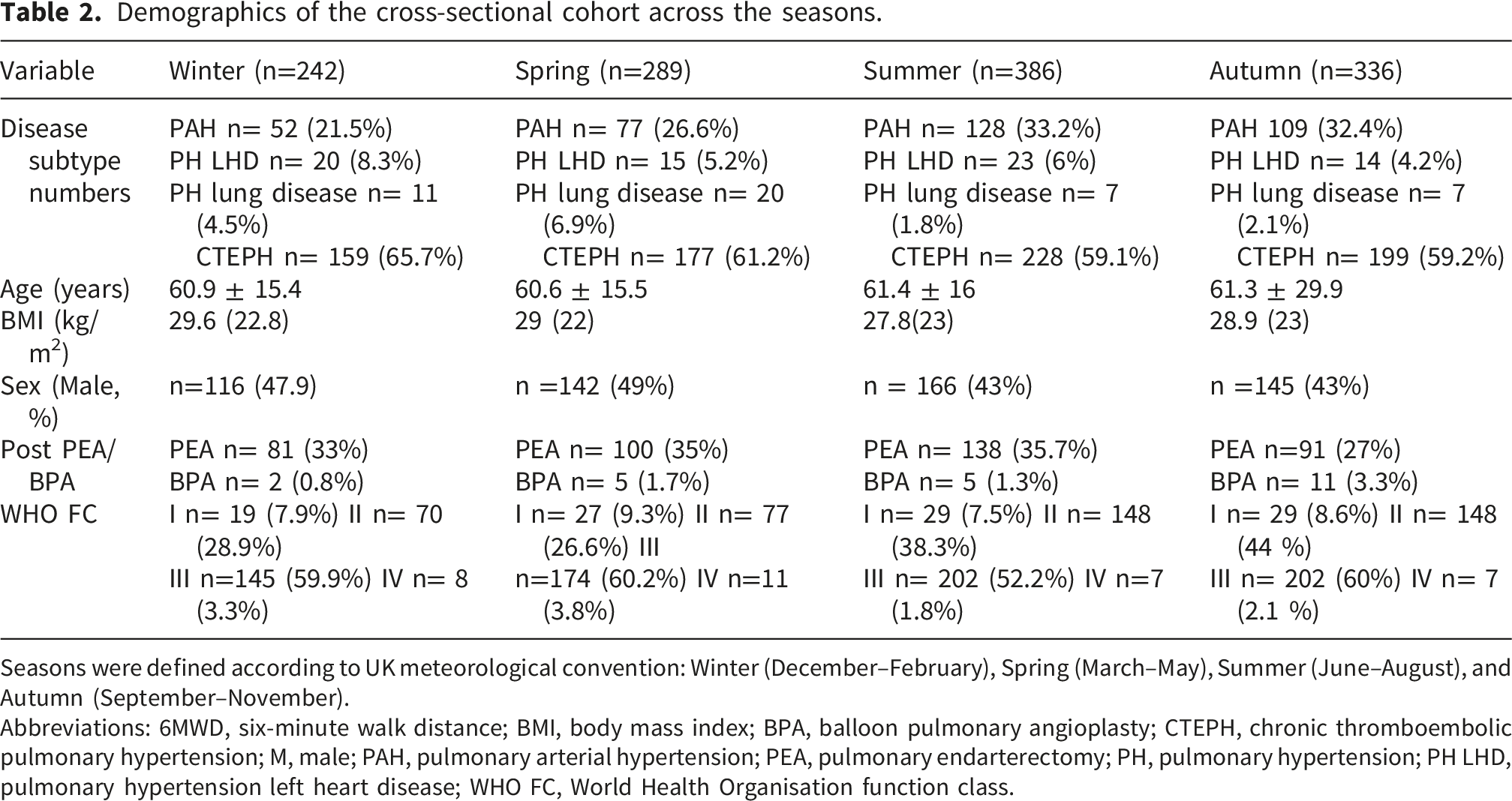
Seasons were defined according to UK meteorological convention: Winter (December–February), Spring (March–May), Summer (June–August), and Autumn (September–November).
Abbreviations: 6MWD, six-minute walk distance; BMI, body mass index; BPA, balloon pulmonary angioplasty; CTEPH, chronic thromboembolic pulmonary hypertension; M, male; PAH, pulmonary arterial hypertension; PEA, pulmonary endarterectomy; PH, pulmonary hypertension; PH LHD, pulmonary hypertension left heart disease; WHO FC, World Health Organisation function class.
6MWD difference between seasons whole cross-sectional cohort
There was no effect of season on 6MWD (p =0.47) (Figure 1(B)). Estimated marginal means for 6MWD were as follows: Winter, 325 m (95% CI: 313-338); Spring, 325 m (95% CI: 313-337); Summer, 336 m (95% CI: 325-347); Autumn, 330 m (95% CI: 318-341).
Longitudinal analysis
In total 516 patients were included into the longitudinal analysis cohort. In total 912 6MWT measurements were in the AM and 1792 measurements were PM. Each patient had at least 1 AM and PM measurement in the analysis. A total of 419 patients had at least one 6MWT in Winter, 410 in Spring, 434 in Summer, and 472 in Autumn. The total number of 6MWT measurements per season was as follows: Winter (n=578), Spring (n=616), Summer (n=690), and Autumn (n=818). Median number of walk visits included for each patient in the analysis was 5 (IQR 4). The median time from the first (baseline) 6MWT each included 6MWT visit was 580 days (IQR 1,037), representing the median follow-up duration.
Cohort characteristics
At baseline, cohort (n=516) characteristics were as follows. Mean Age was 57.7 ± 16.3 years, 242 were male (42%) and BMI was 29.0 ± 8.77. Among the 554 patients, 210 (40.7%) were classified as WHO Group 1 PAH, 6 (1.1%) as WHO Group 2 PH due to left heart disease, 15 (2.9%) as WHO Group 3 PH due to lung disease, and 285 (55.4%) as WHO Group 4 chronic CTEPH. At baseline, among the 515 patients, 36 (6.9%) were in WHO Functional Class I, 166 (32.2.%) in Class II, 306 (59.4%) in Class III, and 8 (1.5%) in Class IV. During the follow-up period, a total of 166 patients underwent or were already post PEA and 59 patients underwent BPA at least once.
AM vs PM longitudinal cohort
In the fully adjusted linear mixed-effects model, time of day (AM vs. PM) was not significantly associated with 6MWD (PM vs. AM: β = 5.18 m, 95% CI −1.22 to 8.41; p = 0.125). The adjusted marginal mean 6MWD was 394 m (95% CI 369-420) in the morning compared to 398 m (95% CI 372–423) in the afternoon (Figure 2(A)). AM vs PM x PEA/BPA status interaction was not significant indicating that BPA/PEA status did not modify the time-of-day effect. Therefore, final model estimates and reported adjusted marginal means are based on the model, without including this interaction term. (a) Estimated marginal means (95% CI) AM vs PM longitudinally for whole PH cohort. (b) Estimated marginal means (95% CI) for 6MWD AM VS PM by WHO functional class longitudinally.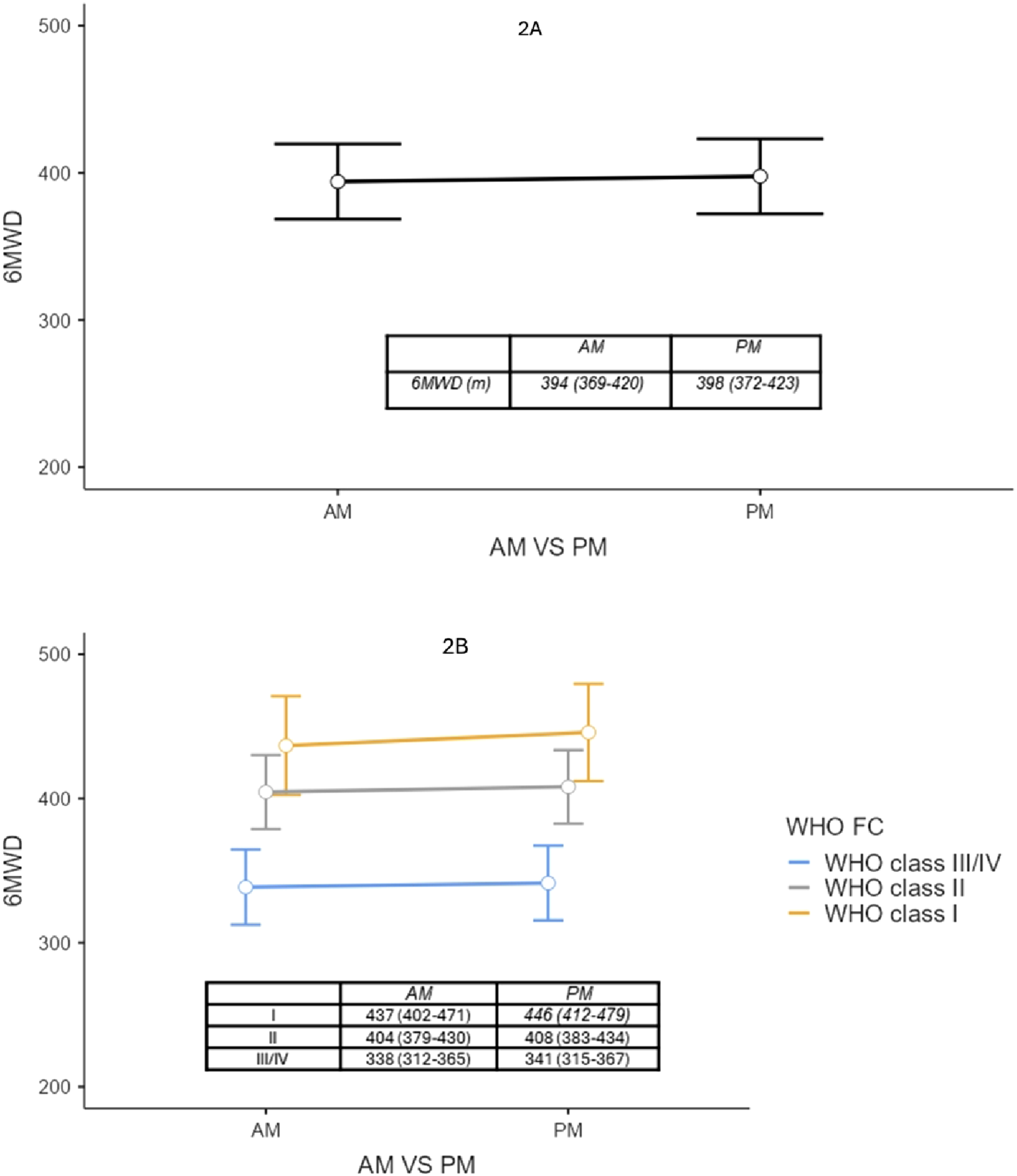
There was no significant effect of time of day on 6MWD across WHO functional classes (p > 0.05) (Figure 2(B)).
Other significant predictors of higher 6MWD included post-BPA/PEA status (β = 34.6 m, p < 0.001), male sex (β = 38.6 m higher than females, p < 0.001), younger age (β = −2.4 m per year, p < 0.001), and longer time since baseline (β = 0.006 m per day, p = 0.009). PH diagnosis (PAH vs. CTEPH: β = 25.5 m, p = 0.009) also influenced 6MWD. Lower WHO Functional Class was associated with 6MWD, with patients in class I and II walking significantly farther than those in class III/IV (class I: β = 101.31 m, 95% CI 76.80–125.82; class II: β = 66.35 m, 95% CI 53.85–78.86; both p < 0.001).”
Overall, these results indicate that time of day had no effect on 6MWD, while disease severity, demographic factors, and clinical status were the primary determinants.
AM vs PM 6MWT parameters
For secondary 6MWT parameters, only maximal heart rate was significantly higher in the afternoon compared to the morning (β = 1.49 bpm, 95% CI 0.26–2.73; p = 0.01 estimated marginal mean AM 113 (109-118) bpm vs 115 (111-119) bpm. No significant differences were observed for resting heart rate, resting or minimal SpO2, or Δ Borg scale (see supplementary table 1 for estimated marginal means for secondary 6MWT parameters.
6MWT seasonal effects
In the fully adjusted linear mixed model 6MWD did not differ significantly between seasons, with estimated differences compared to Winter of β −5.63 m in Spring (95% CI −12.3 to 1.02; p = 0.09), β −2.84 m in Summer (95% CI −8.8 to 3.11; p = 0.34), β and −4.77 m in Autumn (95% CI –10.8 to 1.27; p = 0.122). Season x PEA/BPA status interaction was not significant. indicating that BPA/PEA status did not modify the seasonal effect Therefore, final model estimates and reported adjusted marginal means are based on the model, without including the interaction term.
The estimated marginal mean 6MWD was similar across seasons: Winter 401 m (95% CI 376–427), Spring 395 m (95% CI 370–420), Summer 399 m (95% CI 374–424), and Autumn 398 m (95% CI 373–423). (Figure 3). Estimated marginal means (95% CI) longitudinally by season for the whole cohort. Seasons were defined according to UK meteorological convention: Winter (December–February), Spring (March–May), Summer (June–August), and Autumn (September–November).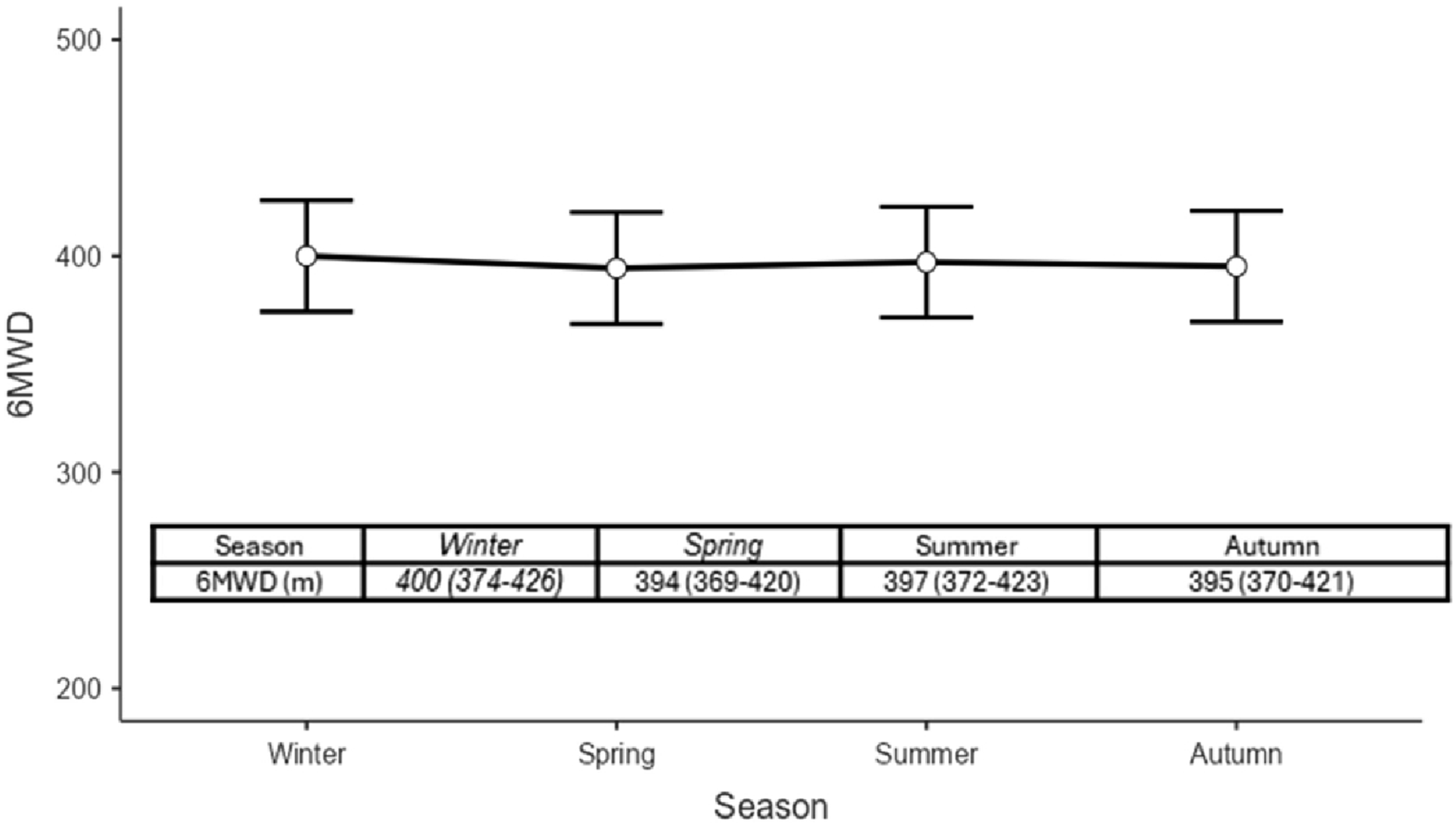
Seasonal secondary 6MWT parameters
Estimated marginal means indicated that resting HR was significantly lower in summer (74.3 bpm, 95% CI 71.4–77.2) and Autumn (75.5 bpm, 95% CI 72.6-78.4) compared with winter (77.3 bpm, 95% CI 74.4–80.3; p<0.01). Similarly, maximal HR was lower in summer (113 bpm, 95% CI 109–117) and autumn (114 bpm, 95% CI 110–118) compared with winter (116 bpm, 95% CI 112–120; p<0.01 for both). Resting and minimal SpO2, as well as Δ Borg (post–pre) scores, remained stable across all seasons (Results are presented in supplementary Table 2).
Discussion
In this study, we examined diurnal and seasonal variation in 6MWD among patients with PH using both cross-sectional and longitudinal approaches. Our longitudinal analyses suggest that 6MWD is not significantly influenced by time of day or season. These findings suggest that, despite guideline recommendations to perform repeat 6MWTs at the same time of day, diurnal and seasonal variation may not represent a major source of variability in this population.
The present study directly evaluated diurnal and seasonal effects on 6MWT performance in PH, addressing a gap in evidence highlighted by ATS guidance, which advises same-time repeat testing but without PH specific evidence. 8 This is important to clarify, as diurnal variation could represent a confounding factor in longitudinal follow-up and clinical trials, and may be harder to control in contemporary remote digital walk tests which can be more patient initiated. 24 In healthy individuals, exercise capacity and ventilatory function often follow a circadian rhythm, with higher function in the afternoon compared with the morning, reflecting underlying diurnal changes in physiology.9–11 In PH, fatigue is highly prevalent15–17 and may worsen throughout the day, potentially counteracting these physiological advantages and leading to poorer 6MWD performance later in the day.
A cross-sectional analysis was conducted to provide an initial assessment of potential time of day effects on 6MWD. In adjusted models, 6MWD was on average 17 meters higher in the morning compared with the afternoon across the PH cohort. This effect was not modified by PH disease classification or WHO functional class.
Following these findings, longitudinal analyses were performed to evaluate within-patient changes in 6MWD over time, providing insight into how individual performance varied throughout the day. In contrast to the cross-sectional results, the longitudinal analysis showed no significant time of day effect on 6MWD. Other factors including demographics (age, sex, BMI), PH diagnosis, WHO functional class, and intervention status (PEA/BPA) were significant determinants of 6MWD, as expected. Similarly, previous studies in elderly and other patient populations have reported no significant time-of-day effect on 6MWD.12–14 However, a major limitation of most of these studies was their small sample sizes (12–24 patients), while one study in multiple sclerosis patients was cross-sectional and included only 80 participants. 14
The discrepancy between cross-sectional and longitudinal findings likely reflects the distinction between patient and within-patient effects. Although morning and afternoon cohorts were broadly similar cross-sectionally, small residual differences in age, PH disease classification, and a higher proportion of post-PEA/BPA patients assessed in the morning may have contributed to the observed 17-m difference, even after adjustment. In contrast, the longitudinal analysis leveraged repeated measures within the same individuals, reducing inter-individual variability and providing a more robust estimate of diurnal effects. Fatigue, a common symptom in PH, may also influence single test occasions but be attenuated with repeated testing over time as patients adapt to the procedure. Longitudinal models additionally accounted for clinical trajectory and interventions, which may outweigh any small diurnal variation. A limitation of the longitudinal analysis was the imbalance in test timing (912 AM vs 1792 PM observations), which may reduce precision of AM estimates. Overall, these findings suggest that the modest cross-sectional difference likely reflects cohort composition and short-term variability rather than a sustained clinically meaningful diurnal effect, supporting that flexibility can occur in scheduling repeat 6MWT in routine clinical practice.
The current ATS 6MWT guidelines 8 do not provide recommendations regarding control for seasonal variation during testing. However, studies in clinical populations such as PH, heart failure and COPD have consistently reported lower levels of physical activity during winter months,18–21,25 which may translate into reduced exercise capacity and highlight the need for direct investigations of seasonal effects on 6MWT performance. In our study, both cross-sectional and longitudinal analyses demonstrated no significant seasonal variation in 6MWD when looking at the North hemisphere-centric re seasons. To date, investigations into this question have been limited. Rothman et al. (2025), using retrospective data from the ASPIRE registry, similarly reported no significant seasonal variation in field exercise tests, including the 6MWT and incremental shuttle walk test. 18 A longitudinal extension of our digital walk test study has also found that whilst passive daily step counts vary by season (lower in the Winter months), there is no effect seen on outdoor remote digital walk test distances. 26 Taken together, our findings, along with the current evidence base, strongly suggest that seasonal variation does not significantly influence 6MWD in PH cohorts in the northern hemisphere. However, as this was a single centre study conducted in a controlled indoor environment with stable ambient temperature (21–22°C), the findings may not be generalisable to regions with more extreme environmental conditions. Higher ambient temperatures and humidity may influence exercise capacity and symptom burden, 27 and future studies across different geographical settings would be warranted.
We additionally examined the longitudinal effects of time of day and season on secondary 6MWT parameters. Among these, the only parameter demonstrating a significant effect was HR. Specifically, maximal HR during the 6MWT was significantly higher in the afternoon compared with the morning. The finding of higher maximal HR in the afternoon is consistent with known circadian variation in autonomic tone and cardiovascular responsiveness, with sympathetic activity and body temperature both typically peaking later in the day. It was similarly demonstrated in two other studies in elderly subjects and patients with heart failure for HR to be significantly higher in the afternoon compared with the morning.9,10 It is also supported by a meta-analysis investigating healthy and clinical cohorts that showed greater HR response in the afternoon. 9
Longitudinal analyses demonstrated that maximal HR during the 6MWT was significantly lower in summer and autumn compared with winter. Several mechanisms could explain this finding: colder months are associated with increased sympathetic activity and peripheral vasoconstriction, which raise HR during exercise, while seasonal hormonal fluctuations, including catecholamines and cortisol, may augment cardiovascular responsiveness. The variations in maximal HR across time of day and season were statistically significant but small. These changes are unlikely to have a meaningful impact on overall functional performance, including 6MWD, in PH. However, minor fluctuations may still be relevant when interpreting HR-based measures such as heart rate reserve or chronotropic response. In practice, although these effects are unlikely to meaningfully alter outcomes.
This study has several strengths and limitations. A key strength is that, to our knowledge, it is the first study to explore time of day and seasonal effects on 6MWD in PH. Although focused on PH, the findings may be relevant to other chronic respiratory disease settings where serial 6MWTs are used for monitoring, supporting greater flexibility in test scheduling. Both the cross-sectional and longitudinal cohorts were relatively large, although the longitudinal cohort was smaller due to discharge and incomplete follow-up. This was a retrospective study; residual confounding is possible. However, the primary question concerned diurnal and seasonal variation in 6MWD, and the longitudinal mixed-effects models used repeated within-patient measures to reduce confounding from stable patient characteristics. This approach provides a robust estimate of diurnal and seasonal effects, making residual confounding an unlikely explanation for the absence of a sustained effect on 6MWD. There was an imbalance in test timing (912 AM vs 1,792 PM observations), which may reduce precision of AM estimates, although mixed models can accommodate unbalanced data. Finally, the cohort was predominantly WHO Group 1 (PAH) and Group 4 (CTEPH), with limited representation of PH due to left heart or lung disease, and findings may not be generalisable to these subgroups. A further limitation relates to the use of a single 6MWT at each visit. While repeat testing is recommended to account for a learning effect, in routine PH clinical practice single tests are commonly performed in experienced patients undergoing serial 6MWT assessments. Therefore, any learning effect is likely minimised and unlikely to differentially influence time of day or seasonal comparisons.
Future studies using prospective designs and randomised protocols are needed to confirm these findings, allowing improved control of potential confounding and more robust assessment of time-of-day effects. Additionally future studies should evaluate whether similar time of day effects are present in other chronic respiratory diseases, particularly COPD, where symptoms and functional limitation are often worst in the morning. 28
To conclude in this large PH cohort, we found that 6MWD was largely stable across different times of day and seasons. While maximal HR showed small but statistically significant variations higher in the afternoon and slightly lower in summer and autumn these changes did not translate into meaningful differences in 6MWD. These findings support the robustness of 6MWD as a functional measure in PH and suggest that, although consistency in test timing may be ideal for secondary physiological parameters like HR, small diurnal or seasonal effects are unlikely to influence clinical interpretation or longitudinal follow-up of 6MWD. Prospective studies are warranted to confirm these findings and further refine recommendations for timing of 6MWT in clinical and research settings.
Supplemental material
Supplemental material - Diurnal and seasonal variation in six-minute walk distance in pulmonary hypertension: Implications for clinical monitoring
Supplemental material for Diurnal and seasonal variation in six-minute walk distance in pulmonary hypertension: Implications for clinical monitoring by Lucy Robertson, Katherine Bunclark, Mark Toshner, Joanna Pepke-Zaba, Karen Sheares, John Cannon, Dolores Taboada Buasso, Karl P. Sylvester, Joseph Newman, and Ben Knox-Brown in Chronic Respiratory Disease.
Supplemental material
Supplemental material - Diurnal and seasonal variation in six-minute walk distance in pulmonary hypertension: Implications for clinical monitoring
Supplemental material for Diurnal and seasonal variation in six-minute walk distance in pulmonary hypertension: Implications for clinical monitoring by Lucy Robertson, Katherine Bunclark, Mark Toshner, Joanna Pepke-Zaba, Karen Sheares, John Cannon, Dolores Taboada Buasso, Karl P. Sylvester, Joseph Newman, and Ben Knox-Brown in Chronic Respiratory Disease.
Supplemental material
Supplemental material - Diurnal and seasonal variation in six-minute walk distance in pulmonary hypertension: Implications for clinical monitoring
Supplemental material for Diurnal and seasonal variation in six-minute walk distance in pulmonary hypertension: Implications for clinical monitoring by Lucy Robertson, Katherine Bunclark, Mark Toshner, Joanna Pepke-Zaba, Karen Sheares, John Cannon, Dolores Taboada Buasso, Karl P. Sylvester, Joseph Newman, and Ben Knox-Brown in Chronic Respiratory Disease.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.