
Abstract
Introduction
Effective airway clearance is crucial in COPD management, and oscillatory positive expiratory pressure (OPEP) devices are a potential adjunct therapy for this. However, their clinical efficacy remains uncertain due to limited trial data.
Aim
To update our previous (2020) systematic review investigating the use of OPEP devices to augment sputum clearance in COPD.
Methods
Randomised Clinical Trails s evaluating OPEP devices in COPD were identified from PubMed, CINAHL, Medline, Cochrane, and Embase (2020–2024). Outcomes included lung function, exercise capacity, exacerbations, and health-related quality of life (HRQoL), with pooled estimates calculated using random-effects models.
Results
Twelve trials (741 participants) were included. OPEP devices significantly reduced exacerbations (Odds Ratio: 0.39) and improved exercise capacity (+49 m at 6MWD). Small improvements were observed in FVC%, while HRQoL changes were not statistically significant. Accumulating evidence suggests benefits for sputum clearance and reduced antibiotic use. Devices were generally well accepted and safe.
Conclusion
OPEP devices appear to be safe and may reduce exacerbations, improve functional exercise capacity, and support sputum clearance in COPD.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is characterised by persistent airflow limitation and airway inflammation, 1 with mucus hypersecretion commonly contributing to cough, dyspnoea, and impaired health-related quality of life 2 Airway clearance may be supported by pharmacological therapies and non-pharmacological techniques, including oscillatory positive expiratory pressure (OPEP) devices, which generate expiratory oscillations and positive pressure to mobilise secretions and reduce airway collapse. 3 The positive expiratory pressure produced also helps prevent airway collapse, enhance collateral ventilation, and support secretion clearance. Adjustable valves in OPEP devices allow modification of expiratory resistance. A previous systematic review reported potential short-term benefits of OPEP therapy on sputum clearance and exercise capacity; however, conclusions were limited by small sample sizes, short intervention durations, methodological heterogeneity, and limited evidence for clinically important outcomes such as exacerbations. 4 Since that review, several additional randomised controlled trials have been published, including studies with larger sample sizes, longer intervention durations, and broader assessment of clinically relevant outcomes, substantially expanding the available evidence base. These newer studies provide an opportunity to address limitations identified in the earlier review and determine whether emerging evidence alters previous conclusions regarding the effectiveness of OPEP devices in COPD. An updated systematic review is therefore warranted to synthesise this expanded evidence base and reassess the role of OPEP therapy in COPD management. 5
Methods
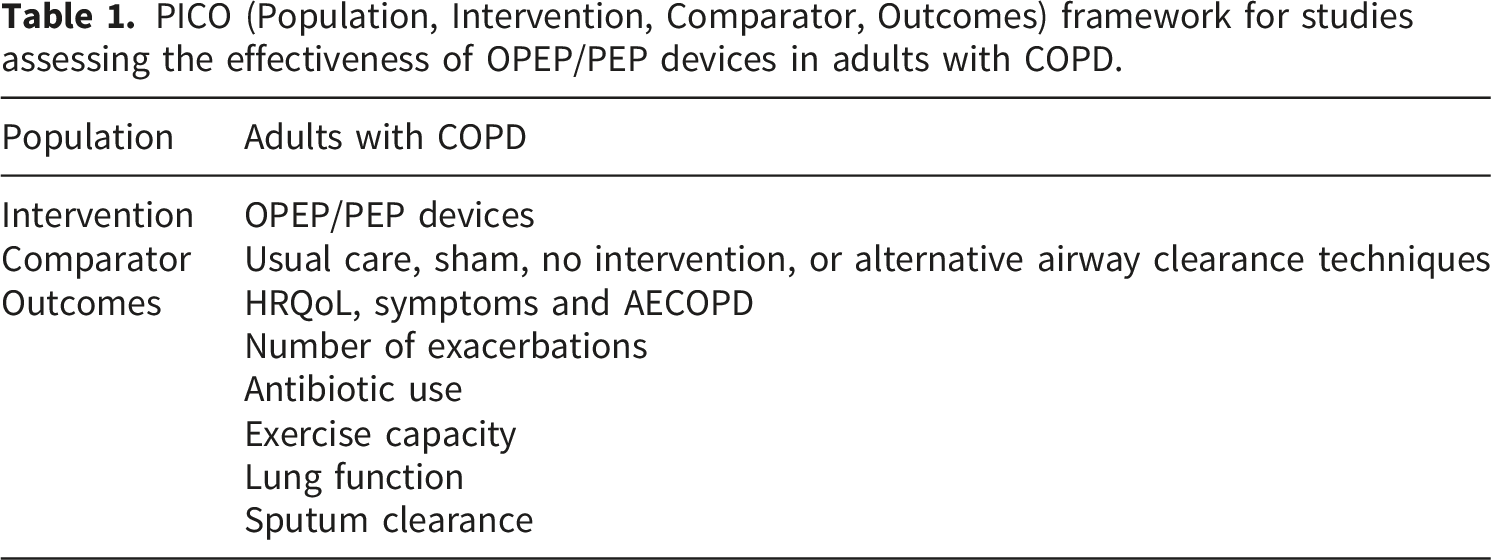
PICO (Population, Intervention, Comparator, Outcomes) framework for studies assessing the effectiveness of OPEP/PEP devices in adults with COPD.
Inclusion criteria
Eligible studies were randomised controlled or crossover trials involving adults with COPD as the primary respiratory diagnosis, defined according to established diagnostic criteria (post-bronchodilator FEV1/FVC <0.70 consistent with Global Initiative for Chronic Obstructive Lung Disease recommendations, evaluating OPEP devices. Mixed respiratory populations were excluded unless COPD-specific data were reported separately.4,5
Exclusion criteria
Studies were excluded if they were not in English. Studies involving mixed respiratory populations were excluded unless outcome data for participants with COPD could be extracted separately. Studies that included participants with COPD but did not report outcomes specific to COPD were excluded. Additionally, studies that assessed only a single treatment session were excluded, as this review focused on interventions involving repeated use and clinically meaningful outcomes that require sustained treatment exposure, rather than short-term physiological effects observed after a single session.
Search strategy
Searches were conducted across PubMed, CINAHL, Medline (Ovid), Cochrane, and Embase databases. In consultation with a librarian, additional manual searches were performed on the reference lists of relevant primary studies and reviews to identify any additional studies that may not have been captured in the original search (Appendix 1).
Search procedures
The main author conducted the search, after which all articles were imported into EndNote, and duplicates were removed using Rayyan QCRI. Titles and abstracts of all articles were screened. A manual search of reference lists from relevant studies was performed to identify potentially suitable articles that might have been missed from the database search. Subsequently, a full-text review of all included articles was conducted. Any study that did not meet the inclusion criteria was excluded, and reasons for exclusion were recorded according to the PRISMA flowchart (Appendix 2).
Data extraction
Data related to studies, populations, and outcomes were extracted independently by two reviewers using a standardised data-extraction form developed for this review. Study characteristics included authors’ names, year of publication, country, study duration, and research design. Population characteristics included the number of subjects, age, gender, BMI, GOLD grade if reported, Forced Expiratory Volume in one second as a percentage of predicted (FEV1%), number of COPD patients who consented to participate; number of index-year exacerbations (mean ± SD), sputum clearance, health-related quality of life (HRQoL), physical activity, and fatigue. After extraction, the two reviewers cross-checked all entries for accuracy and completeness. Any discrepancies were resolved through discussion and, when necessary, consultation with a third reviewer. This process ensured consistency and minimised errors in the final dataset.
Data analysis
The synthesis of results centred on evaluating primary outcomes, including health-related quality of life (HRQoL), COPD symptoms, frequency of acute exacerbations, lung function parameters, and exercise capacity. Additionally, patient adherence indicators such as acceptance, completion, and dropout rates were assessed. A meta-analysis was conducted to calculate pooled differences and 95% confidence intervals (CIs) for key outcomes, comparing the OPEP group with the control group. A random-effects model was applied to ensure conservative estimates. Continuous outcomes were presented as mean differences (D), and standardised mean differences (SMD) were used when outcomes were measured on varying scales. For categorical data, odds ratios (OR) were employed. Study heterogeneity was examined using the I2 statistic, while publication bias was evaluated through funnel plots of included studies, and certainty of evidence for key outcomes was additionally assessed using the GRADE (Grading of Recommendations Assessment, Development and Evaluation) approach (Appendices 3, 4). Analyses were conducted with the Cochrane Collaboration’s Review Manager Software RevMan (5.4.1). The acceptance rate was calculated as the proportion of participants who consented to participate out of all those approached for the trial. The completion rate was defined as the number of participants who completed the study relative to those enrolled, and the dropout rate was calculated based on the number who withdrew from each treatment arm as a fraction of those who initially consented. 8 An additional meta-analysis was undertaken to estimate pooled differences and 95% CIs for acceptance, completion, and dropout rates between the OPEP and control groups. Rates were weighted by study sample size and combined using random-effects models. All rates are reported as proportions with 95% CIs.
Results
Between 2020 and 2024, a systematic search of PubMed and Embase identified 91 records, of which 11 duplicates were removed. After screening 80 titles and abstracts, 69 records were excluded, leaving 11 articles for full-text review. Four additional randomised controlled trials met the eligibility criteria and were included alongside the eight studies from the previous review
6
(Figure 1) (Table 2). Forest plot comparing HRQoL measures (CAT and SGRQ) scores in OPEP interventions vs non-OPEP interventions. New and old studies include.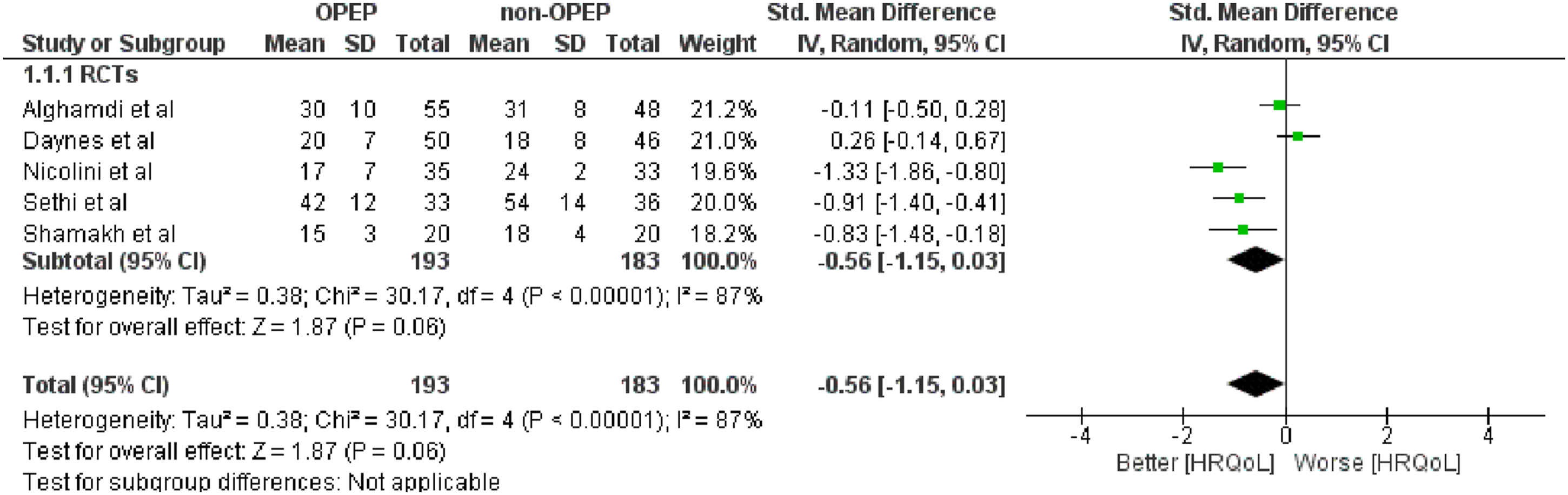
Characteristics of included studies
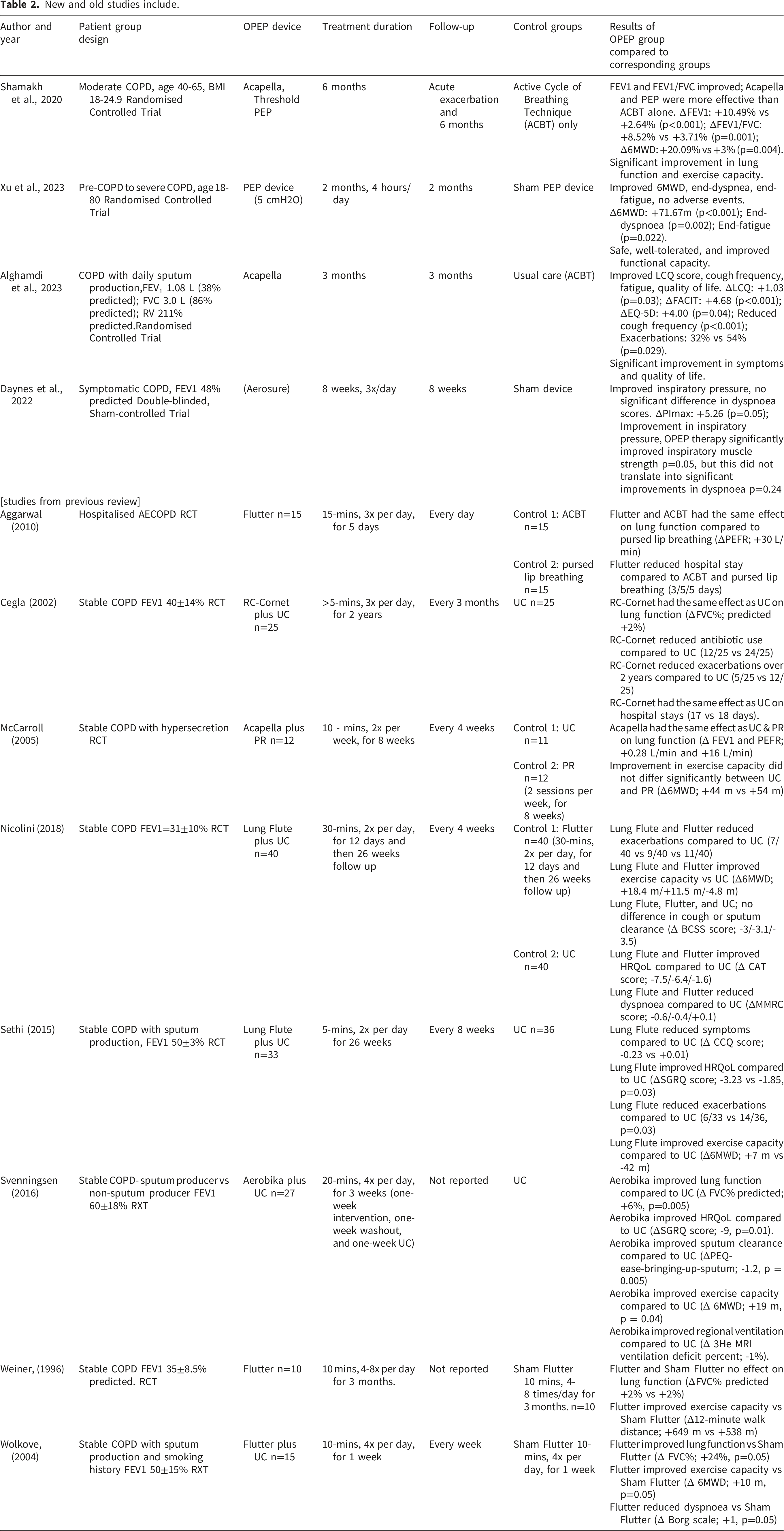
Twelve randomised controlled trials involving 741 participants were included in this updated review, comprising eight studies from the previous review and four newly identified trials. Sample sizes ranged from 25 to 122 participants, with most studies enrolling patients with stable COPD, although a small number included participants during acute exacerbations. Participants represented a range of disease severity and symptom burden, with some studies specifically recruiting individuals with chronic sputum production. A variety of OPEP and PEP devices were evaluated, including Acapella, Flutter, Aerobika, Lung Flute and RC-Cornet, with intervention durations ranging from several weeks to two years. Comparator groups included usual care, sham devices, and alternative airway clearance or physiotherapy interventions. Overall, studies were heterogeneous in participant characteristics, intervention protocols and follow-up duration. Detailed study and participant characteristics are summarised in (Table 2).
Risk of bias assessment
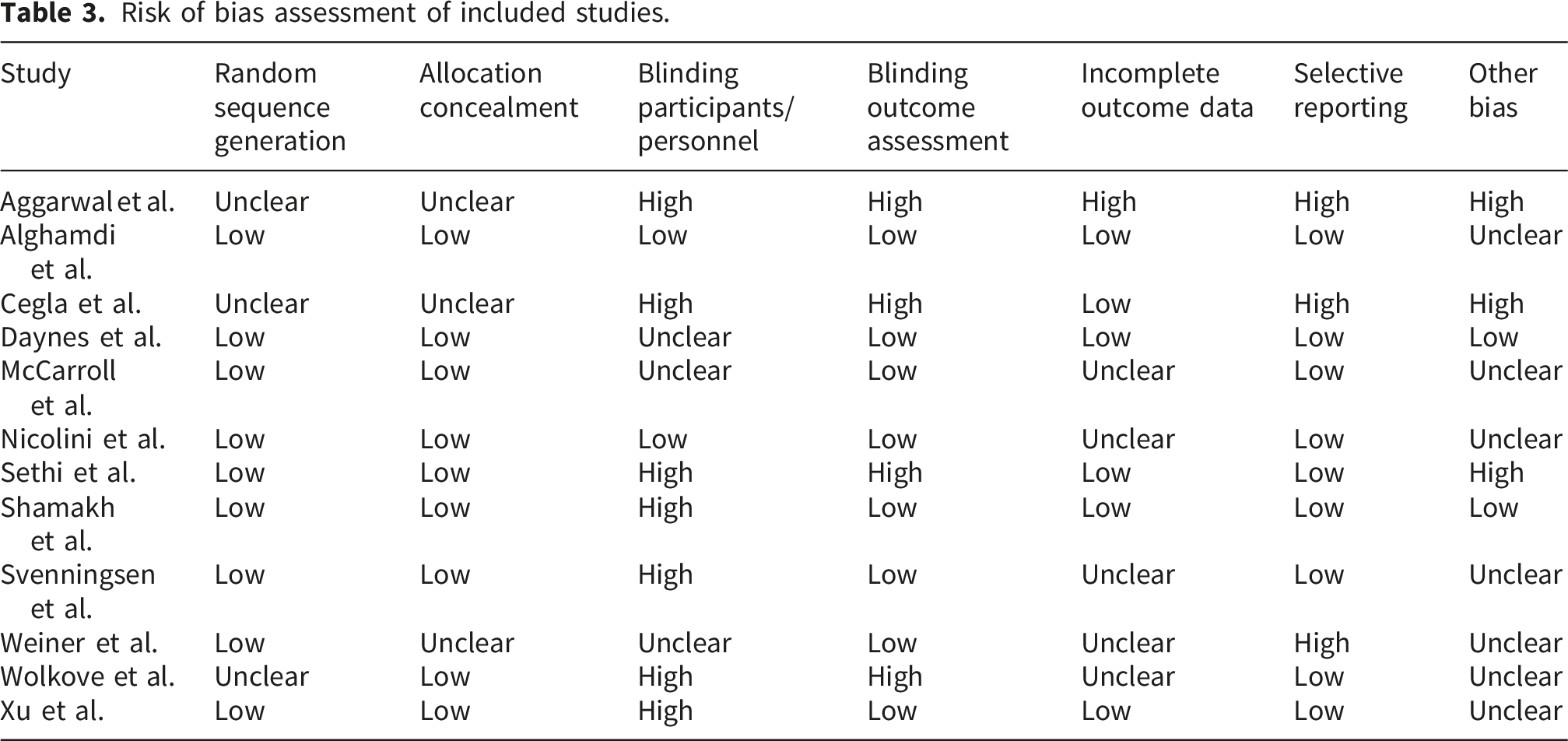
Risk of bias assessment of included studies.
Acceptance, completion, and dropout rates
Across the twelve included randomised controlled trials evaluating PEP and OPEP devices in COPD, acceptance, completion, and dropout rates were generally favourable. Overall, 350 participants completed their assigned intervention, while 31 (approximately 9%) withdrew before study completion. The primary reasons for dropout included loss to follow-up (66%), COPD exacerbations (16%), death (6%), back pain (6%), MRI-related discomfort (3%), and unknown reasons (3%). From these studies, the unweighted acceptance, completion, and dropout rates were 82%, 91%, and 6%, respectively.
Stable COPD
HRQoL, symptoms and AECOPD
Health-related quality of life (HRQoL) was reported in five randomised controlled trials.10–14 When pooled, the meta-analysis for improved HRQoL was not statistically significant in patients using OPEP devices compared with non-OPEP controls (SMD = –0.56; 95% CI: –1.15 to 0.03; p = 0.06) although the direction of effect favoured the OPEP intervention. Substantial heterogeneity was observed (I2 = 87%), suggesting considerable variability in effect estimates, likely arising from differences in study populations, intervention duration, device characteristics, and the HRQoL measurement tools used (Figure 1).
Number of exacerbations
Exacerbations were reported in four randomised controlled trials.10,12,13,15 The pooled analysis showed that OPEP device use was associated with a significant reduction in exacerbation events compared with non-OPEP controls (OR = 0.39; 95% CI: 0.23 to 0.64; p = 0.0003) the pooled analysis showed that OPEP device use was associated with a significant reduction in exacerbation events compared with non-OPEP controls (OR = 0.39; 95% CI: 0.23 to 0.64; p = 0.0003). This corresponds to an estimated 61% reduction in exacerbation risk among patients using OPEP devices. There was no observed heterogeneity (I2 = 0%), indicating a consistent effect across studies despite differences in sample size, device type, and patient characteristics. As such, there is moderate confidence, according to the GRADE assessment, that OPEP devices reduce exacerbation frequency, and the true effect is likely to be close to the observed estimate (Figure 2). Forest plot comparing exacerbation events of OPEP use vs usual care in stable COPD.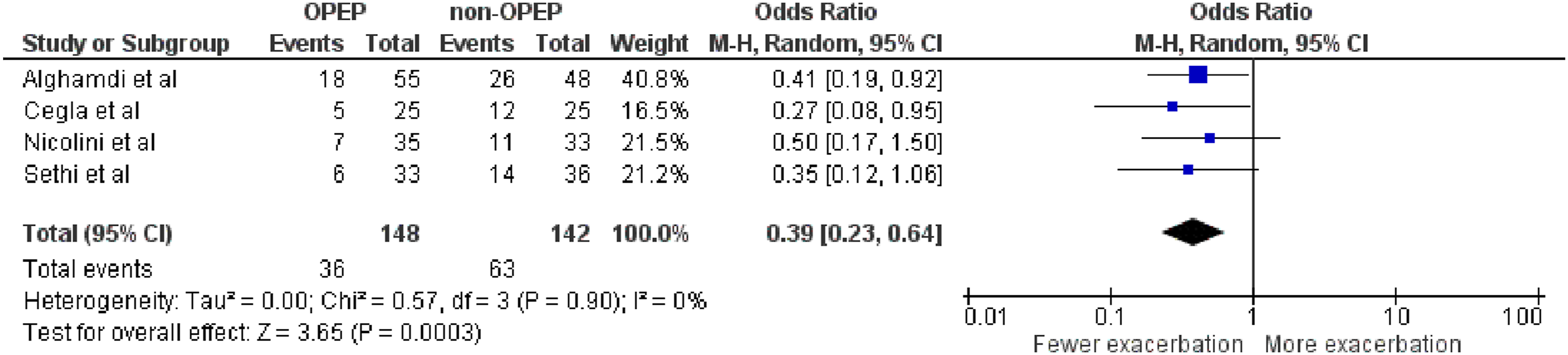
Antibiotic use
Antibiotic use was inconsistently reported across the included studies. Only one long-term trial 16 evaluated antibiotic consumption as a formal outcome and found that twice-daily use of the RC-Cornet device over a 2-year period significantly reduced the number of patients requiring at least one course of antibiotics compared with the control group (13/25 vs. 24/25; OR = 0.05; 95% CI: 0.01 to 0.38; p = 0.005). None of the remaining eleven studies, including the four newly added trials,10,11,14,17 reported antibiotic use as an outcome measure. Consequently, while the available evidence suggests a potential reduction in antibiotic use with long-term OPEP therapy, the certainty of this finding is limited due to the reliance on a single study and the absence of supporting data from other trials.
Exercise capacity
Six randomised controlled trials12–14,17–19 reported changes in 6-minute walk distance (6MWD). The pooled analysis demonstrated a significant improvement in exercise capacity among patients using OPEP devices compared with non-OPEP controls (MD = 49.39 m; 95% CI: 25.05 to 73.73 m; p < 0.0001). Both newly added studies
14
and
17
contributed to the positive direction of effect, with
17
reporting one of the largest individual improvements (Figure 3). Forest plot comparing exercise capacity measured with 6MWD (in metres) in OPEP interventions vs non-OPEP interventions.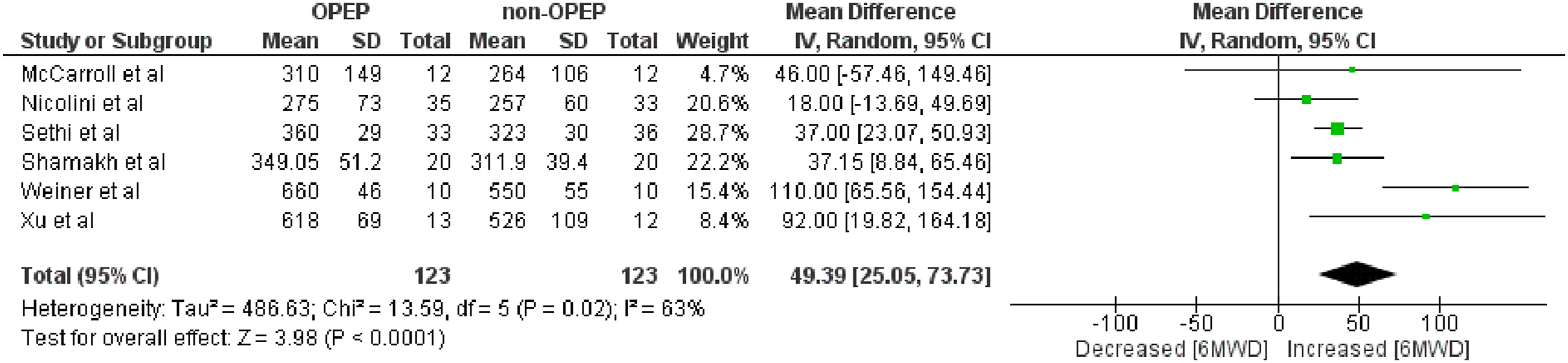
Lung function
Forced vital capacity percentage (FVC%) was reported in six RCTs.10,15–17,19,20 The pooled analysis demonstrated a statistically significant improvement in FVC% among patients using OPEP devices compared with non-OPEP controls (MD = 3.06%; 95% CI: 0.18 to 5.95; p = 0.04). Subgroup analysis showed that long-term studies did not demonstrate significant improvement (MD = 1.43%; 95% CI: –1.36 to 4.22), whereas short-term studies produced a clinically meaningful increase in FVC% (MD = 6.85%; 95% CI: 1.65 to 12.04). The newly added trials
10
in the long-term group and
17
in the short-term group contributed to the overall pooled effect in their respective subgroups. Heterogeneity was low overall (I2 = 10%) but moderate within the short-term subgroup (I2 = 69%), likely reflecting differences in intervention duration, baseline lung function, and device characteristics (Figure 4). Forest plot comparing PFT measured with FVC% long-short term in OPEP interventions vs non-OPEP interventions.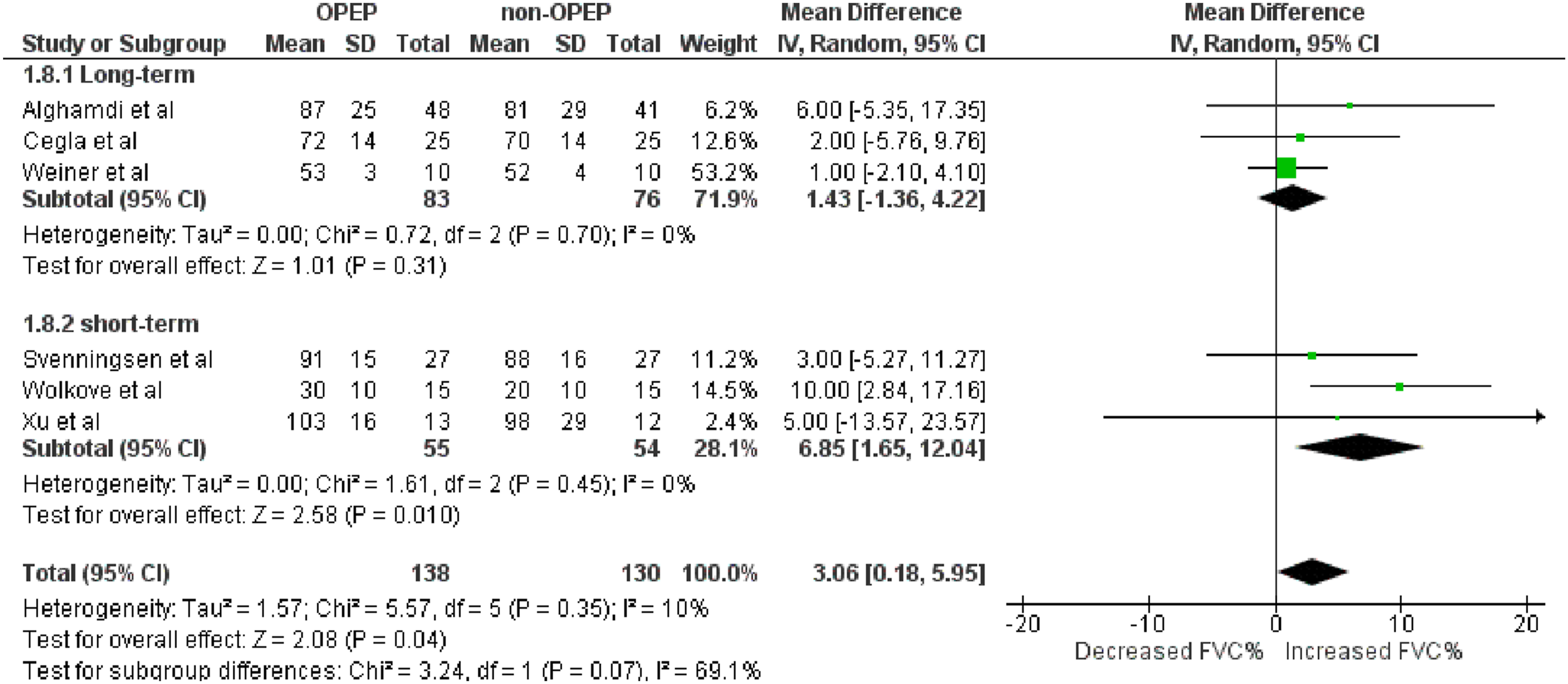
Sputum clearance
Sputum clearance was evaluated in only two of the twelve included studies,10,20,21 each using different oscillatory PEP devices and outcome measures. An earlier RCT 20 assessed sputum clearance over a 3-week period using the Aerobika device and reported a significantly greater improvement compared with usual care, as reflected by lower PEQ ease-of-bringing-up-sputum scores (mean ± SD: 2.70 ± 1.10 vs. 3.60 ± 0.50; p = 0.003), where a lower score indicates better clearance. In contrast, a more recent trial 10 using the Acapella device demonstrated a statistically and clinically significant improvement in sputum clearance, showing a mean increase of 0.50 on the sputum frequency scale (95% CI: 0.27–0.60; p < 0.001), compared with a negligible change in the control group (+0.06). Importantly, none of the included studies reported objective sputum clearance outcomes such as sputum volume or weight, and assessment was limited to patient-reported or symptom-based measures.
Discussion
In COPD, improving sputum clearance remains a key therapeutic objective, given its association with daily symptom burden, health-related quality of life, and risk of acute exacerbations. 22 Findings from this updated review suggest that OPEP devices may improve several clinically relevant outcomes, including symptoms, exacerbation frequency, exercise capacity and sputum clearance. A reduction in antibiotic use was also observed in the only long-term trial reporting this outcome. 20
This update included four additional randomised controlled trials, increasing the evidence base from eight to twelve studies and expanding the pooled sample from 339 to 741 participants. While a previous 2020 review 6 suggested potential benefits of OPEP devices for reducing exacerbations and improving exercise capacity, those findings were based on a limited number of predominantly short-term studies with low-certainty evidence. The present update strengthens and extends those earlier observations through a broader evidence base, more precise pooled effect estimates, and more consistent signals of benefit.
Exacerbation outcomes were generally modest but directionally consistent, with pooled results demonstrating a reduction in exacerbation risk among patients using OPEP devices. However, the number of contributing studies remains small, most interventions were relatively short in duration, and methodological limitations, particularly related to blinding and outcome reporting, temper confidence in these findings. Health-related quality of life showed a non-significant trend favouring OPEP therapy, though with substantial heterogeneity likely reflecting variation in patient populations, intervention duration, device type and outcome measures used. 23 This variability highlights the need for greater standardisation of outcome assessment in future trials.
Exercise capacity improved across studies reporting 6-minute walk distance,12,17,18,24–26 with pooled gains of approximately 49 m, exceeding commonly reported minimal clinically important difference thresholds for COPD (approximately 25–35 m), supporting the clinical relevance of this finding. 23 Longer-duration interventions appeared to show particularly consistent benefits, suggesting that sustained treatment exposure may be important.
Although sputum production is a prominent and distressing symptom for many individuals with COPD, it remains relatively neglected in current COPD guidelines.4,22,27,28 Neither the Global Initiative for Chronic Obstructive Lung Disease (GOLD) nor the American Thoracic Society/European Respiratory Society (ATS/ERS) guidelines make explicit recommendations on sputum clearance techniques,21,22,29 whereas the National Institute for Health and Care Excellence (NICE) guidelines briefly suggest the use of PEP devices or active cycle of breathing techniques for “excessive” sputum, 30 without defining the threshold at which these should be implemented. The findings of this review suggest that patients with chronic sputum production may derive the greatest benefit from OPEP therapy. Only one included study differentiated sputum producers from non-producers, and those with regular sputum demonstrated more pronounced improvements. 20 Future research should therefore adopt clearer phenotyping to identify the subgroups most likely to respond.
A range of OPEP and PEP devices were evaluated, with generally high acceptance and completion rates, suggesting good patient acceptability. The largest improvements in symptoms, HRQoL, and exacerbations were seen with Acapella, Lung Flute, and Aerobika, whereas fewer benefits were observed with Flutter 10 13. This may reflect differences in device mechanisms, including adjustable resistance, oscillation frequency, and ease of use. 31
Dropouts in OPEP trials were commonly related to COPD exacerbations, highlighting the need for flexible study designs that can accommodate temporary interruptions or modification of device use. In addition, factors such as cognitive ability, physical technique, and the level of training provided to patients may influence adherence and overall treatment success. Real-world application of OPEP devices exhibits considerable variability, and healthcare professionals themselves express uncertainty concerning optimal thresholds for device prescription and patient selection. This uncertainty reflects challenges similar to those identified in the trials included in this review. 32
Overall, this review highlights gaps in the existing evidence base and identifies priorities for future research. These include stratifying patients by sputum production, standardising outcome measures, evaluating longer-term effectiveness, and conducting direct comparisons between device types.
Limitations
This review has several limitations. Many trials were at high risk of performance and detection bias due to limited blinding in device-based interventions and incomplete reporting of missing data and adherence, which reduced confidence in the findings. Outcome measures varied widely, contributing to heterogeneity and limiting comparability. Most studies were small and short-term, restricting assessment of long-term effectiveness. Few trials stratified patients by sputum burden, and no direct comparisons between OPEP devices were available.
Conclusion
This updated review suggests that OPEP devices may reduce exacerbations, improve exercise capacity, enhance sputum clearance, and produce short-term benefits for lung function in COPD, particularly in patients with chronic sputum production.
Supplemental material
Supplemental material - Use of oscillatory positive expiratory pressure (OPEP) devices to augment sputum clearance in COPD: An updated systematic review and meta-analysis
Supplemental material for Use of oscillatory positive expiratory pressure (OPEP) devices to augment sputum clearance in COPD: An updated systematic review and meta-analysis by Ahmed A. Alzahrani, Saeed M Alghamdi, Mansour S. Majrshi, Ali M Alasmari, Surinder S Birring, Lizzie Grillo, Nicholas S Hopkinson in Chronic Respiratory Disease.
Supplemental material
Supplemental material - Use of oscillatory positive expiratory pressure (OPEP) devices to augment sputum clearance in COPD: An updated systematic review and meta-analysis
Supplemental material for Use of oscillatory positive expiratory pressure (OPEP) devices to augment sputum clearance in COPD: An updated systematic review and meta-analysis by Ahmed A. Alzahrani, Saeed M Alghamdi, Mansour S. Majrshi, Ali M Alasmari, Surinder S Birring, Lizzie Grillo, Nicholas S Hopkinson in Chronic Respiratory Disease.
Supplemental material
Supplemental material - Use of oscillatory positive expiratory pressure (OPEP) devices to augment sputum clearance in COPD: An updated systematic review and meta-analysis
Supplemental material for Use of oscillatory positive expiratory pressure (OPEP) devices to augment sputum clearance in COPD: An updated systematic review and meta-analysis by Ahmed A. Alzahrani, Saeed M Alghamdi, Mansour S. Majrshi, Ali M Alasmari, Surinder S Birring, Lizzie Grillo, Nicholas S Hopkinson in Chronic Respiratory Disease.
Supplemental material
Supplemental material - Use of oscillatory positive expiratory pressure (OPEP) devices to augment sputum clearance in COPD: An updated systematic review and meta-analysis
Supplemental material for Use of oscillatory positive expiratory pressure (OPEP) devices to augment sputum clearance in COPD: An updated systematic review and meta-analysis by Ahmed A. Alzahrani, Saeed M Alghamdi, Mansour S. Majrshi, Ali M Alasmari, Surinder S Birring, Lizzie Grillo, Nicholas S Hopkinson in Chronic Respiratory Disease.
Supplemental material
Supplemental material - Use of oscillatory positive expiratory pressure (OPEP) devices to augment sputum clearance in COPD: An updated systematic review and meta-analysis
Supplemental material for Use of oscillatory positive expiratory pressure (OPEP) devices to augment sputum clearance in COPD: An updated systematic review and meta-analysis by Ahmed A. Alzahrani, Saeed M Alghamdi, Mansour S. Majrshi, Ali M Alasmari, Surinder S Birring, Lizzie Grillo, Nicholas S Hopkinson in Chronic Respiratory Disease.
Supplemental material
Supplemental material - Use of oscillatory positive expiratory pressure (OPEP) devices to augment sputum clearance in COPD: An updated systematic review and meta-analysis
Supplemental material for Use of oscillatory positive expiratory pressure (OPEP) devices to augment sputum clearance in COPD: An updated systematic review and meta-analysis by Ahmed A. Alzahrani, Saeed M Alghamdi, Mansour S. Majrshi, Ali M Alasmari, Surinder S Birring, Lizzie Grillo, Nicholas S Hopkinson in Chronic Respiratory Disease.
Footnotes
Author contributions
AA led the review update, data extraction, and manuscript drafting. SMA contributed to the original review and protocol. MSM and AMA assisted with data extraction and analysis. NSH, SSB, and MIP supervised the study and provided critical input. LG provided coordination and editorial review. All authors approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Trial registration
Registration ID number: International Prospective Register of Systematic Reviews (PROSPERO): CRD42024554789.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.