
Abstract
Background
Accurate assessment of asthma symptom control is central to effective management. Spirometry is the gold standard for evaluating lung function and monitoring physiological impairment, and the Global Lung Function Initiative (GLI) has developed widely used spirometric reference equations applicable across populations. However, population-specific equations may better reflect regional characteristics. This study examined the impact of using different spirometric reference equations on asthma assessment.
Methods
In this cross-sectional study, pre-bronchodilator forced expiratory volume in one second (FEV1), forced vital capacity (FVC), and FEV1/FVC were assessed in 384 adults with asthma, and symptom control status was assessed using the Asthma Control Test (ACT). Reference values, z-scores, and lower limits of normal (LLN) were derived using the GLI Global (GLI-2022 race-neutral) equation (GLIgl), GLI-2012 Caucasian equation (GLI2012_cauc), GLI-2012 Other/mixed equation (GLI2012_other), and Al-Qerem local equation (LOCAL). Agreement between equations was evaluated using Cohen’s kappa, and their sensitivity and specificity for identifying ACT-defined uncontrolled symptoms were assessed.
Results
Spirometric values differed significantly across equations. Associations between spirometric impairment and ACT-defined uncontrolled symptoms were modest, with low-to-moderate discrimination. Higher FEV1 and FVC z-scores were consistently associated with higher ACT scores across all equations, although explained variance was limited and model-fit differences were minimal. Pairwise agreement between equation sets was substantial to near-perfect for FEV1 < LLN (kappa = 0.692-0.907) and FEV1/FVC < LLN (kappa = 0.757-0.945), while LLN-defined impairment rates differed across equations.
Conclusions
The choice of spirometric reference equation substantially influences impairment classification and its concordance with ACT-defined symptom control, but overall predictive performance remains modest. Spirometry should be interpreted as a complementary, rather than standalone, tool in asthma assessment, with careful consideration of population-appropriate reference standards.
Introduction
Asthma is a chronic airway disorder that leads to wheezing, shortness of breath, coughing, and chest tightness, along with variable expiratory airway obstruction.1,2 Asthma is one of the main non-communicable diseases affecting more than 339 million people worldwide across all age groups and causes considerable mortality, morbidity, and healthcare use.3–5 Recent estimates indicate that adult asthma remains common, with prevalence varying substantially across regions and countries. 6 Recent Global Burden of Disease 2021 estimates indicate that asthma accounted for approximately 21.4 million disability-adjusted life years (DALYs) globally in 2021, corresponding to an age-standardized DALY rate of about 265 per 100,000 population. 6
In Jordan, the prevalence of asthma among adults has been reported to reach 10%. 7 A high proportion of uncontrolled asthmatic patients increases disease burden, which can be mitigated by proper management, including regular follow-up and effective education. 8 Accurate evaluation of asthma symptom control and physiological impairment is critical for appropriate management.
Spirometry is widely used in clinical practice as a key tool for evaluating respiratory function as well as for screening and monitoring of asthma. It also enables monitoring of patients’ response to therapy by measuring changes in lung function such as forced expiratory volume in one second (FEV1), forced vital capacity (FVC), and the FEV1/FVC ratio. FEV1 and FEV1/FVC are considered independent risk factors for asthma exacerbations.9,10
To interpret spirometry results accurately, a reference equation is necessary to predict normal values, which are influenced by factors including age, sex, thoracic wall size, height, and ethnicity. 11 Spirometric reference equations developed by the Global Lung Function Initiative (GLI) are among the most widely used. 12 However, using a single spirometric reference equation across different populations has been questioned, as variations in ethnic background, socioeconomic conditions, and environmental exposures may substantially affect lung function measurements, which can subsequently influence classification of physiological impairment and assessment of symptom control. 13 While several studies have examined the impact of spirometric reference equations in children.14,15 There is limited evidence about the effect of these equations on asthma assessment among adults. Therefore, the objective of this study was to investigate the impact of using different spirometric reference equation sets, on the assessment of spirometric impairment and symptom control among Jordanian adults with asthma.
Methods
Study design and participants
This cross-sectional study recruited 385 patients with asthma undergoing treatment at the Respiratory Therapy Unit of the University of Jordan Hospital (JUH), Amman, Jordan. Of these, 384 patients with complete ACT and spirometry data were included in the analytic sample. Patients were recruited during the period of September 2025 to January 2026. The inclusion criteria involved adults 18 years and older with confirmed diagnosis of asthma, and who were able to complete a spirometry test. Eligible patients were selected after reviewing their medical records on the day preceding their scheduled visit at the clinic. Patients were approached during the visit by a trained researcher who informed them about the study’s objectives and assured them that participation is voluntary, in addition to their right to withdraw from the study at any time. Written consent forms were obtained from the participants. Ethical approval was obtained from the Institutional Review Board (IRB) committee of Jordan University Hospital [10-2025/8377]. This study adhered to the ethical principles of the Declaration of Helsinki.
Data collection and study procedure
Sociodemographic and clinical data were collected by the researcher using a demographic sheet that included birthdate, sex, used medications, and available clinical characteristics. Height and weight were measured using standardized instruments on the day of the visit, and body mass index (BMI) was calculated for each patient.
Asthma symptom control, which was the main clinical outcome of the study, was assessed using the Asthma Control Test (ACT). 16 It is a standardized clinical tool routinely used at the study hospital, administered in its validated Arabic version. 17 This test consists of five items assessing asthma control over the past four weeks: (1) the degree to which asthma interfered with daily activities, (2) the frequency of shortness of breath, (3) the frequency of nocturnal symptoms or early morning awakening due to asthma, (4) the frequency of rescue bronchodilator use, and (5) the patient’s overall self-assessment of asthma control. Each item was assessed on a five-point Likert scale yielding a total score ranging from 5 to 25, with higher scores indicating better asthma control. Uncontrolled symptoms were defined as an ACT score of 19 or less.
Lung function was evaluated separately using pre-bronchodilator spirometric parameters: forced expiratory volume in one second (FEV1), forced vital capacity (FVC), and the FEV1/FVC ratio. Pre-bronchodilator values were used in all analyses. Spirometric measurements were performed by a trained respiratory technician in accordance with American Thoracic Society/European Respiratory Society (ATS/ERS) guidelines. 18 All participants were instructed to perform at least three acceptable forced expiratory manoeuvres. To be considered acceptable, the manoeuvres should meet the following: a rapid and forceful start to expiration, low back-extrapolated volume, consistent effort without coughing, and a clear end-of-test plateau on the volume–time graph. Acceptability and repeatability criteria were applied according to ATS/ERS standards, including agreement within 150 mL between the two largest acceptable FEV1 and FVC values.
Statistical analysis
Symptom control was operationalized using the Asthma Control Test (ACT), with uncontrolled symptoms defined a priori as ACT ≤ 19. Spirometric indices (FEV1, FVC, and FEV1/FVC) were evaluated using four equation sets: Al-Qerem local equation (LOCAL), 19 GLI Global (GLI-2022 race-neutral) equation (GLIgl), GLI-2012 Caucasian equation (GLI2012_cauc), and GLI-2012 Other/mixed equation (GLI2012_other).20,21 Predicted values, z-scores, and LLN values were obtained for each equation set using the corresponding reference equations. 22 LLN was defined as the equation-specific 5th percentile of the reference distribution, not the 5th percentile of the present study sample. This corresponds to a z-score of -1.645. Accordingly, below-LLN impairment was classified as FEV1 < LLN or FEV1/FVC < LLN, and the analysis compared the frequency of participants falling below each externally defined LLN rather than deriving a percentile threshold from the present study sample.
LLN-defined impairment frequencies were first summarized overall and by sex to compare how below-LLN classification changed across equation sets. Pairwise agreement in LLN-defined impairment classifications between equation sets was quantified using Cohen’s kappa. Diagnostic performance of each categorical below-LLN definition against ACT-defined uncontrolled symptoms was then evaluated by estimating sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV), overall and stratified by sex. Discrimination for these categorical LLN-based classifications was assessed using the area under the receiver operating characteristic curve (AUC) computed from adjusted model-predicted probabilities; 95% confidence intervals were obtained using the DeLong method, and pairwise AUC differences between equation sets were tested using DeLong’s test with Holm correction within sex and outcome. Associations between categorical below-LLN impairment and uncontrolled symptoms were examined using sex-stratified logistic regression models, with uncontrolled symptoms as the dependent variable and impairment status as the main exposure. These models were adjusted for age, body mass index (BMI), and smoking status; age and BMI were standardized (z-transformed) to improve numerical stability and comparability of coefficients across equations. Multiplicity arising from testing multiple equation sets within each sex and outcome definition was addressed using Holm correction of p-values. All statistical analysis was performed using R version 4.5.2.
After the categorical LLN-based analyses, exploratory ROC analyses were performed to evaluate how well equation-derived FEV1 and FEV1/FVC z-scores discriminated ACT-defined uncontrolled symptoms (ACT ≤ 19). Youden-optimal z-score cutpoints were derived for all four equation sets and are reported in the Supplementary material.
Additionally, ACT total score was analyzed as a continuous outcome to examine symptom burden across the full range of scores. For each equation set, z-scores for FEV1, FVC, and FEV1/FVC were evaluated in separate linear regression models with ACT total score as the dependent variable. Models were adjusted for age and body mass index (BMI), both standardized (z-transformed); combined-sample models additionally included sex, whereas sex-stratified models omitted sex. Heteroscedasticity-consistent type 3 (HC3) standard errors were used to account for potential heteroscedasticity, and Holm correction was applied within each spirometric index and stratum to address multiplicity across equation sets. To compare equation sets on the continuous ACT outcome, model fit was summarized using adjusted R-squared and Akaike information criterion (AIC).
Sample size calculation
The analytic dataset comprised 384 records with complete information. Given the sex-stratified modeling strategy, effective sample sizes were 263 females and 121 males for the diagnostic and regression analyses, with 215/263 female records and 99/121 male records classified as uncontrolled (ACT ≤ 19). For the adjusted logistic regression models, the number of model terms per sex-specific model was limited to the impairment indicator, age, BMI, and smoking status (entered as two indicator terms), yielding event-per-parameter ratios of approximately 215/5 in females and 99/5 in males, exceeding conventional minimum thresholds for stable estimation.
Results
Participant characteristics by sex.
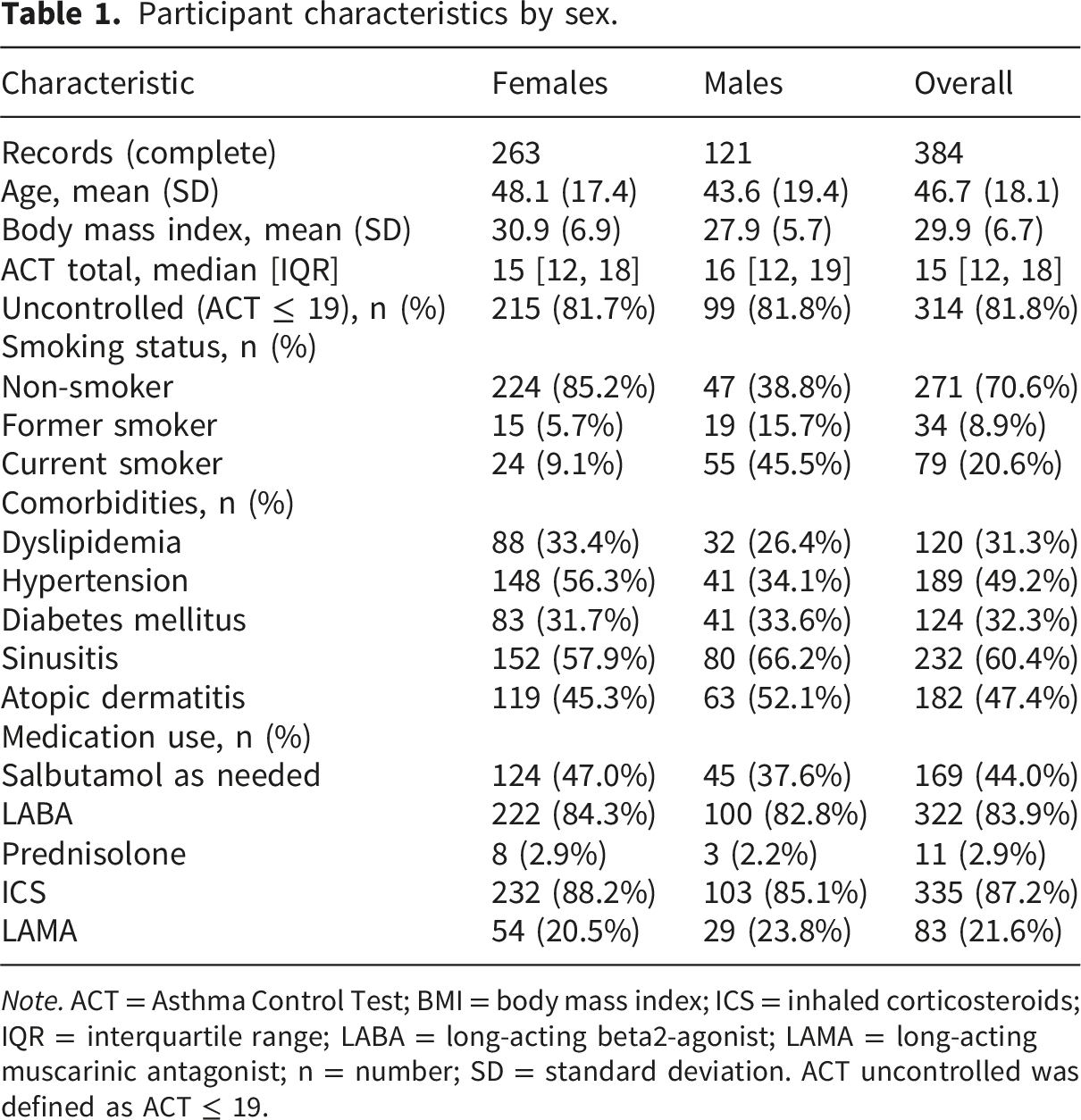
Note. ACT = Asthma Control Test; BMI = body mass index; ICS = inhaled corticosteroids; IQR = interquartile range; LABA = long-acting beta2-agonist; LAMA = long-acting muscarinic antagonist; n = number; SD = standard deviation. ACT uncontrolled was defined as ACT ≤ 19.
LLN-defined impairment frequencies varied across equation sets (Table S1 and Figure S1). Overall, FEV1 < LLN ranged from 23.7% using LOCAL to 37.0% using GLI2012_cauc, corresponding to a 13.3 percentage-point increase for GLI2012_cauc relative to LOCAL. For FEV1/FVC < LLN, LOCAL classified the largest proportion below LLN (29.2%), whereas GLI2012_cauc classified the smallest proportion (20.1%), a 9.1 percentage-point decrease relative to LOCAL. This pattern was broadly consistent within sex strata, with GLI2012_cauc producing the largest FEV1 < LLN frequency and LOCAL producing the largest FEV1/FVC < LLN frequency in both females and males. Nevertheless, pairwise Cohen’s kappa values showed substantial to near-perfect agreement for FEV1 < LLN (0.692-0.907) and FEV1/FVC < LLN (0.757-0.945), with detailed pairwise results provided in Table S2.
Diagnostic performance overall and by sex, according to equation set.
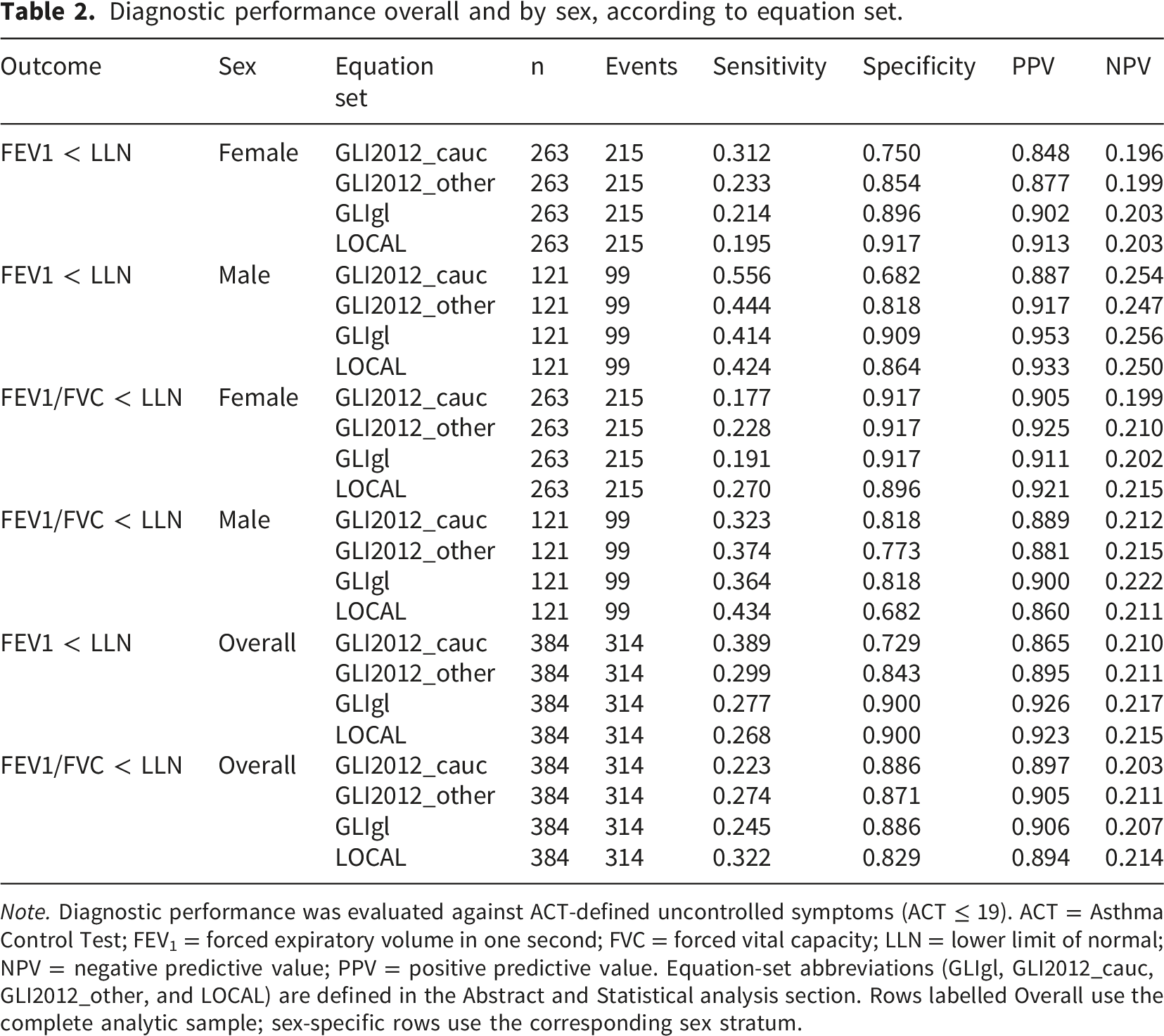
Note. Diagnostic performance was evaluated against ACT-defined uncontrolled symptoms (ACT ≤ 19). ACT = Asthma Control Test; FEV1 = forced expiratory volume in one second; FVC = forced vital capacity; LLN = lower limit of normal; NPV = negative predictive value; PPV = positive predictive value. Equation-set abbreviations (GLIgl, GLI2012_cauc, GLI2012_other, and LOCAL) are defined in the Abstract and Statistical analysis section. Rows labelled Overall use the complete analytic sample; sex-specific rows use the corresponding sex stratum.
Categorical below-LLN discrimination (AUC) by sex and equation set.
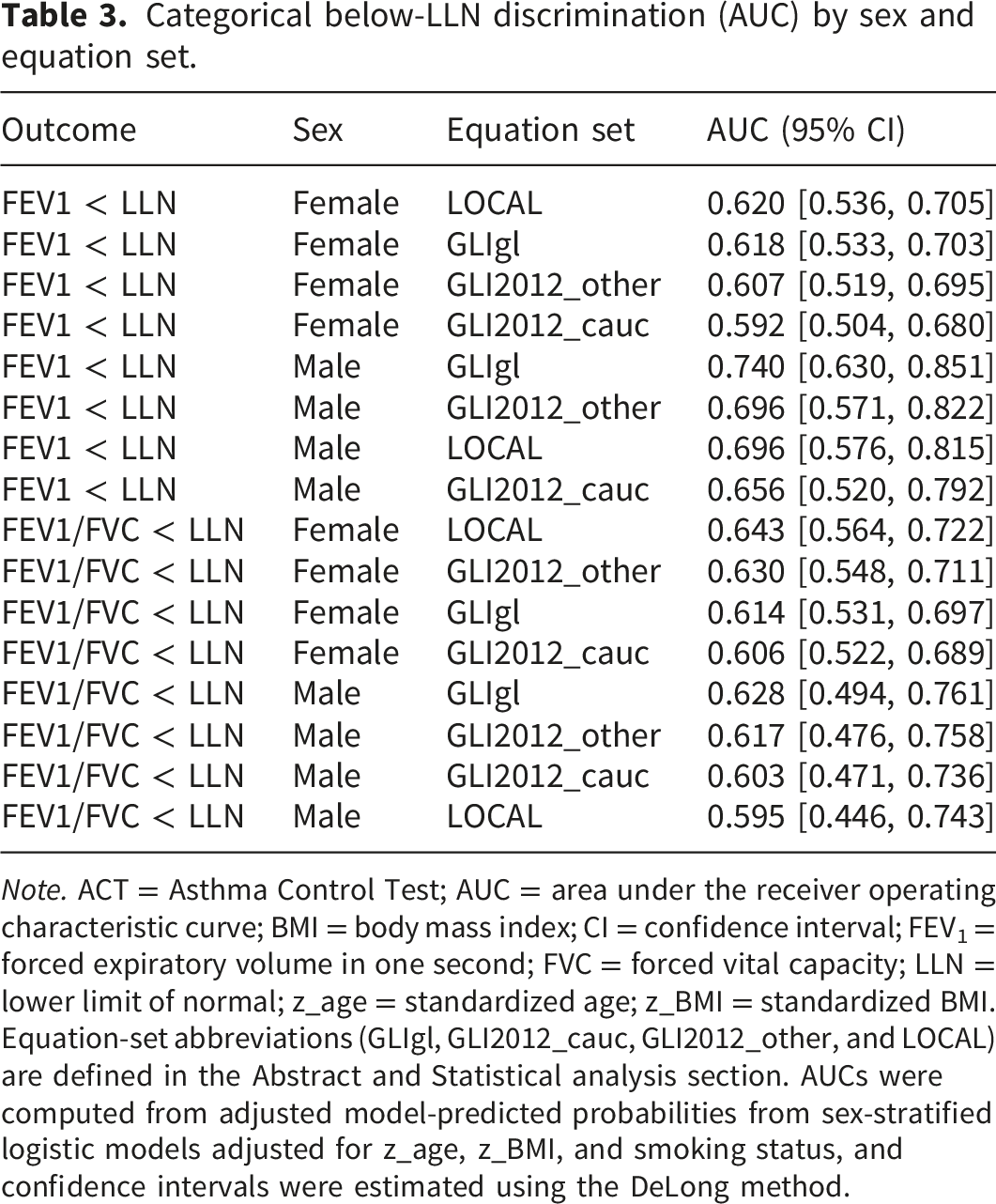
Note. ACT = Asthma Control Test; AUC = area under the receiver operating characteristic curve; BMI = body mass index; CI = confidence interval; FEV1 = forced expiratory volume in one second; FVC = forced vital capacity; LLN = lower limit of normal; z_age = standardized age; z_BMI = standardized BMI. Equation-set abbreviations (GLIgl, GLI2012_cauc, GLI2012_other, and LOCAL) are defined in the Abstract and Statistical analysis section. AUCs were computed from adjusted model-predicted probabilities from sex-stratified logistic models adjusted for z_age, z_BMI, and smoking status, and confidence intervals were estimated using the DeLong method.
Pairwise AUC comparisons using DeLong’s test are provided in Table S3 (see supplementary material). No statistically significant AUC differences were detected for the FEV1 < LLN outcome after Holm correction within either sex. For the FEV1/FVC < LLN outcome among females, only the GLI2012_other versus GLI2012_cauc comparison remained statistically significant after Holm correction (p_holm = 0.048). Among males, no pairwise AUC differences remained significant after Holm correction for the FEV1/FVC < LLN outcome.
Sex-stratified adjusted logistic regression of below-LLN impairment by equation set and ACT classification.
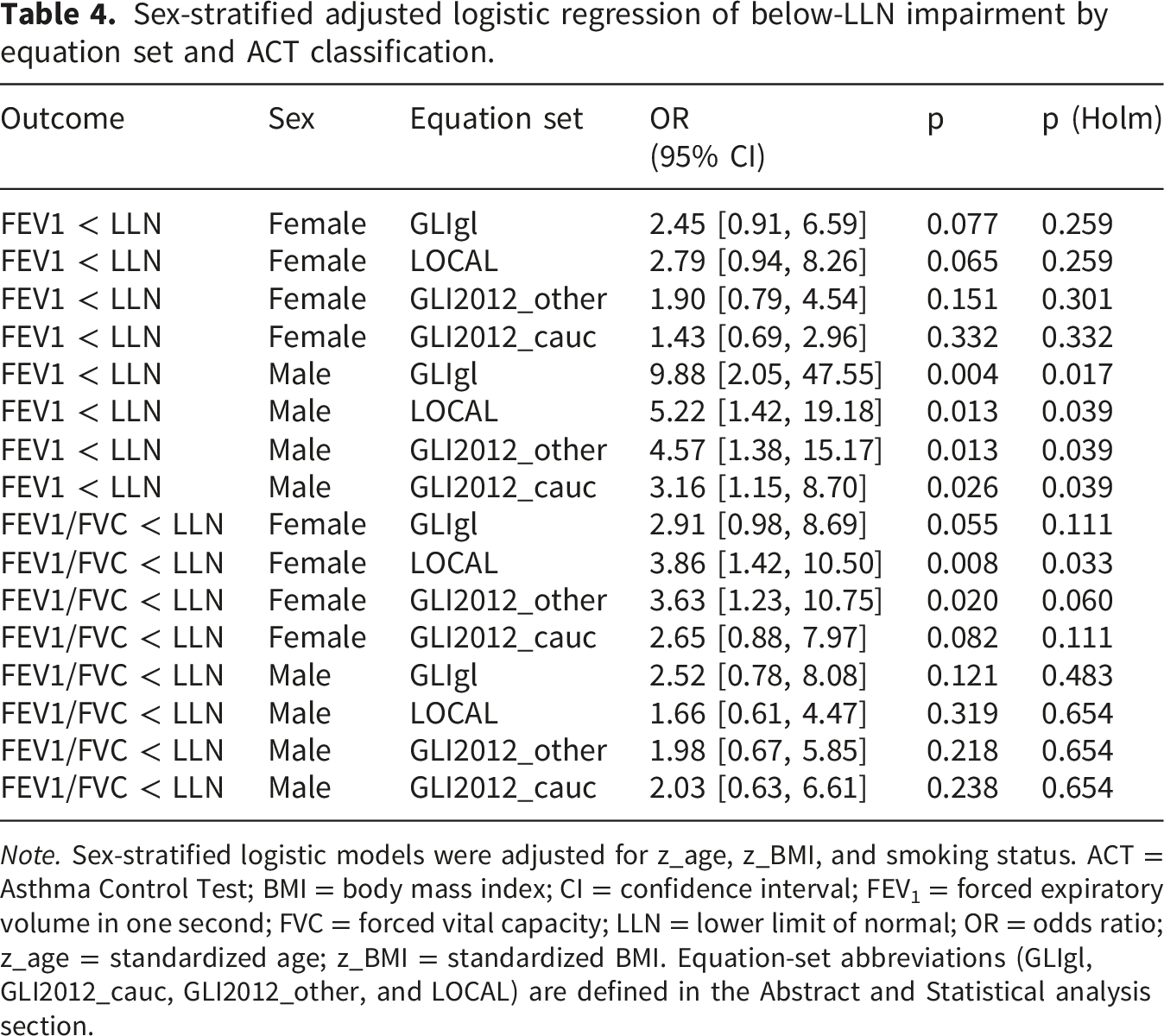
Note. Sex-stratified logistic models were adjusted for z_age, z_BMI, and smoking status. ACT = Asthma Control Test; BMI = body mass index; CI = confidence interval; FEV1 = forced expiratory volume in one second; FVC = forced vital capacity; LLN = lower limit of normal; OR = odds ratio; z_age = standardized age; z_BMI = standardized BMI. Equation-set abbreviations (GLIgl, GLI2012_cauc, GLI2012_other, and LOCAL) are defined in the Abstract and Statistical analysis section.
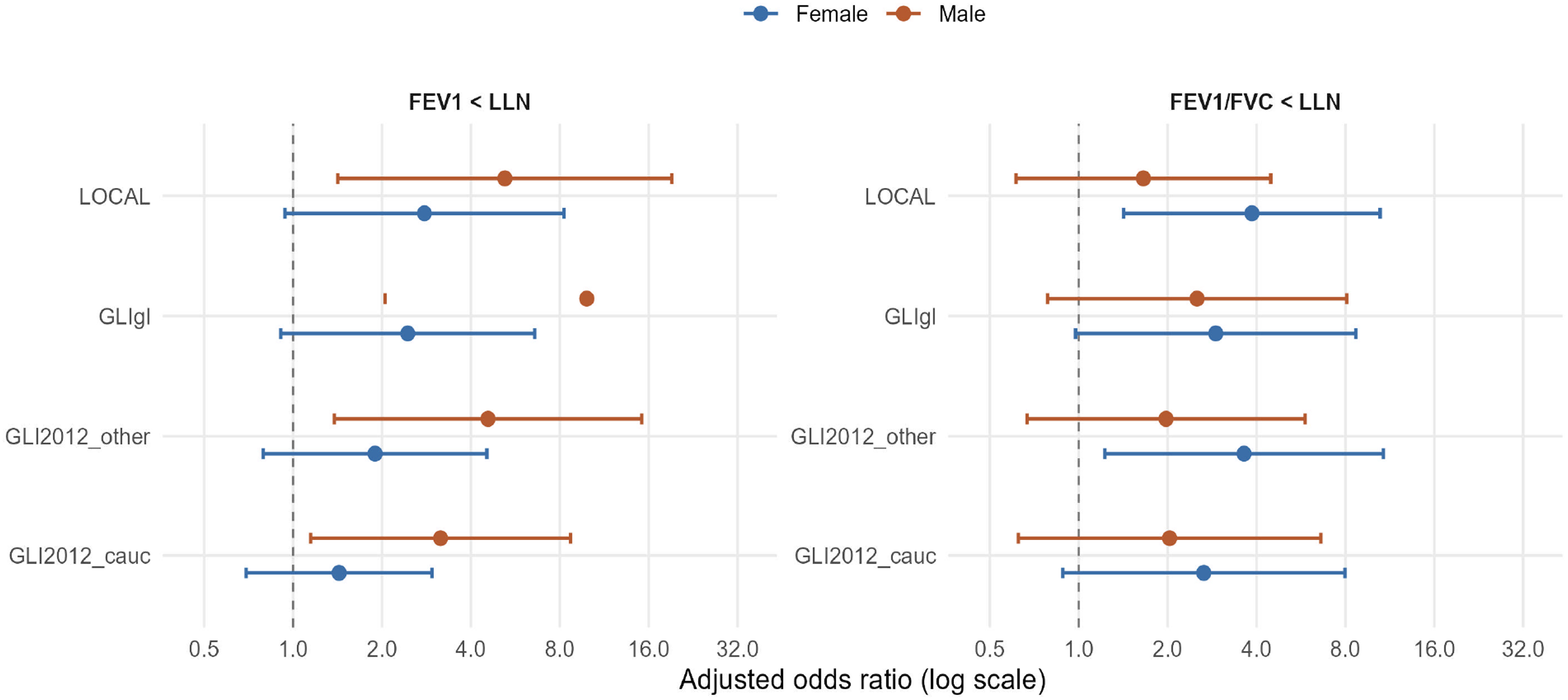
Fixed LLN (z ≤ −1.645): association with ACT uncontrolled after adjustment for age, BMI, and smoking status.
Exploratory ROC analyses showed modest discrimination for ACT-defined uncontrolled symptoms across equation-derived z-scores (Table S4). For FEV1 z-scores, AUCs were similar across equation sets in the overall sample (0.614-0.627), with higher values in males (0.671-0.689) than females (0.588-0.601). LOCAL showed the highest FEV1 z-score AUC overall and within both sex strata, although differences were small. For FEV1/FVC z-scores, AUCs were lower and closely clustered overall (0.572-0.588), in females (0.585-0.608), and in males (0.557-0.560). Youden-optimal cutpoints varied by equation set and sex, indicating that ROC-derived thresholds did not consistently align with the conventional LLN boundary.
Continuous ACT model fit comparison (Δ adjusted R2).
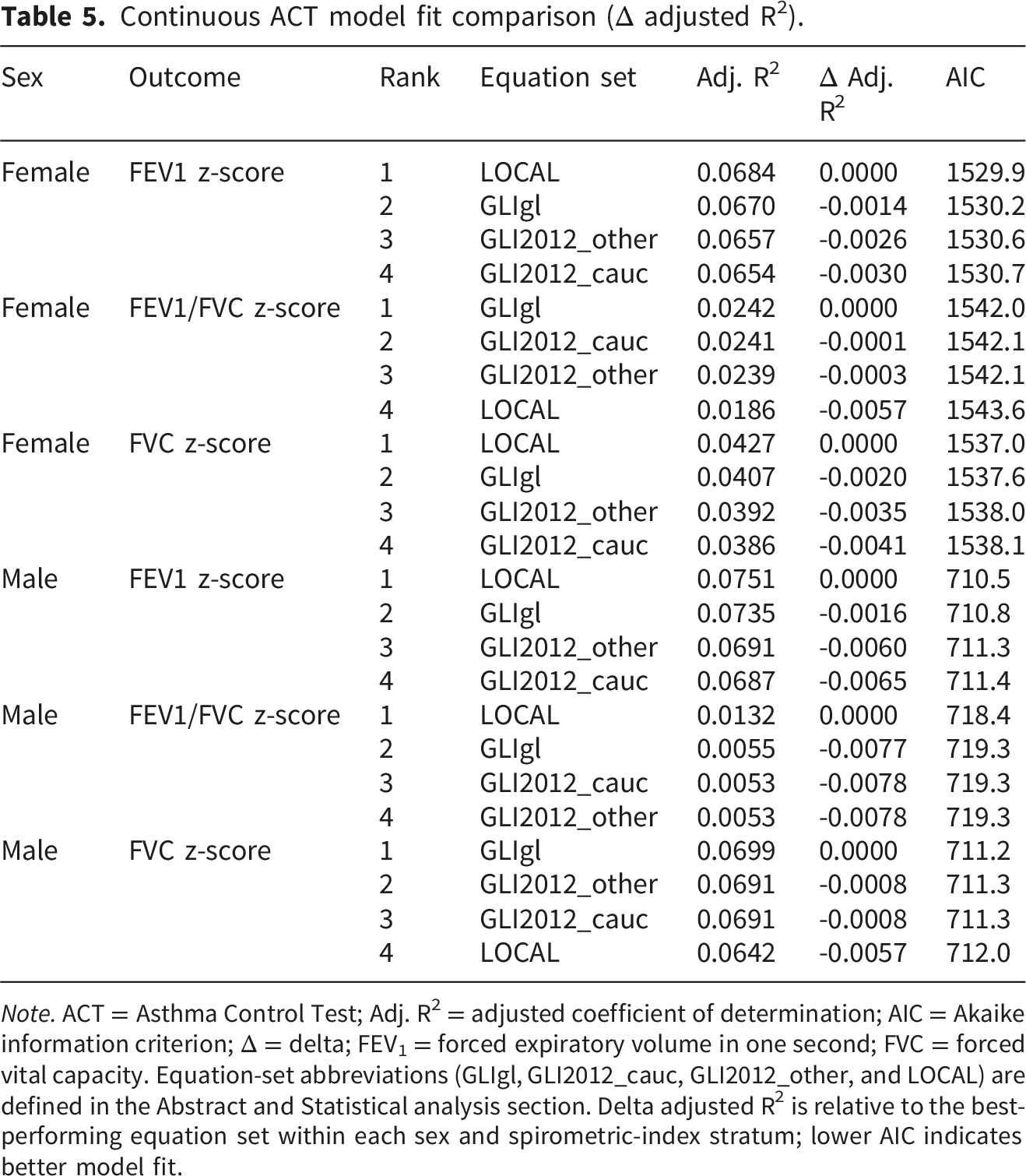
Note. ACT = Asthma Control Test; Adj. R2 = adjusted coefficient of determination; AIC = Akaike information criterion; Δ = delta; FEV1 = forced expiratory volume in one second; FVC = forced vital capacity. Equation-set abbreviations (GLIgl, GLI2012_cauc, GLI2012_other, and LOCAL) are defined in the Abstract and Statistical analysis section. Delta adjusted R2 is relative to the best-performing equation set within each sex and spirometric-index stratum; lower AIC indicates better model fit.
Discussion
This study compared LOCAL with GLI2012_cauc, GLI2012_other, and GLIgl, focusing on how equation choice affects the relationship between spirometric impairment and asthma symptom burden measured using the ACT. The principal finding is that the association between LLN-defined impairment and uncontrolled symptoms was present but modest in discrimination terms, and it varied by equation and by sex. This pattern is clinically plausible because asthma control is multidimensional, and spirometric indices capture only one component of the disease (airflow limitation) that does not consistently track symptom perception and recent symptom frequency. 20
The high prevalence of ACT-defined uncontrolled symptoms is also consistent with the recruitment setting. Patients attending a hospital respiratory therapy unit are more likely to have persistent symptoms, recent treatment concerns, or more complex clinical profiles than patients sampled from the community. 23 Similar regional and Jordanian evidence has shown that poor asthma control is common and is influenced by health-service factors, trigger exposure, and treatment-related factors. 24 In addition, the ACT reflects symptom burden over the previous four weeks, including activity limitation, nocturnal symptoms, rescue medication use, and perceived control,16,25 which may be influenced by adherence, triggers, comorbidities, smoking, obesity, and treatment access. 26 This helps explain why ACT-defined poor symptom control was common while spirometric impairment showed only modest discrimination, and supports interpreting spirometry as complementary to patient-reported symptom assessment rather than as a standalone marker of control.
Across equations, LLN-based impairment definitions were associated with uncontrolled ACT, but overall AUCs remained in the low-to-moderate range. This is consistent with the broader literature showing limited concordance between symptom-based control tools and spirometry in asthma, where patients may report poor control despite preserved lung function, or conversely may have clinically relevant obstruction with comparatively few symptoms. 27 The GINA strategy explicitly notes that lung function does not correlate strongly with asthma symptoms in adults, reinforcing that spirometry should be interpreted as a risk marker and a component of assessment rather than a surrogate for symptom control. 28
The continuous ACT analyses strengthen this interpretation. When ACT was modelled as a continuous outcome, higher z-scores for FEV1 and FVC were consistently associated with higher ACT scores, but the explained variance remained small, and differences in model fit between equations were minimal. This combination, statistically clear associations alongside low R2, suggests that lung function contributes to symptom burden but explains only a limited proportion of between-person variability. This is consistent with several studies that have demonstrated discrepancy between spirometric measurements and symptom-based control measures, with lung functions accounting for a limited proportion of variability in symptoms and quality-of-life outcomes. A retrospective study among adults with asthma found that changes in ACT scores did not correspond to changes in FEV1, and that this discordance was affected by patient characteristics such as age and sex. 29 Another retrospective study of survey responses and spirometry results from 1748 patients with persistent asthma reported a weak and statistically insignificant association between FEV1 and Asthma Control Questionnaire (ACQ) scores. 30 These findings could be attributed to the fact that ACT reflects recent symptoms, activity limitation, nocturnal symptoms, and rescue use, which are influenced by adherence, triggers, comorbidity, and inflammation beyond what is captured by pre-bronchodilator spirometry. 30
Equation choice mattered more for classification behavior and the sensitivity-specificity trade-off than for the continuous z-score-ACT relationship. In the categorical analyses, GLIgl and LOCAL tended to cluster together in overall performance and associations, while GLI2012_cauc often shifted the balance toward higher sensitivity and lower specificity. The GLI2012_cauc and GLI2012_other equation sets were based on multi-ethnic all-age references, but the original consortium acknowledged the need for additional data from several regions, including Arab populations, to refine applicability. 21 The move toward race-neutral interpretation, represented here by GLIgl, was motivated by concerns about embedding race/ethnicity selection in clinical interpretation and by evidence that a single global model can fit comparably to some GLI2012_cauc and GLI2012_other groupings while changing classification for a subset of individuals. 20 In external datasets, adoption of race-neutral equations has been shown to shift z-scores and reclassify impairment status compared with GLI2012_cauc and GLI2012_other, highlighting that “best” performance depends on the outcome anchor and population mix. 31
The LLN-fixed analysis is the most defensible clinically, because LLN on the z-scale corresponds to the 5th percentile (approximately z ≤ -1.645) and is a standard interpretive strategy for defining abnormality. 21 Under this fixed criterion applied to the FEV1/FVC z-score, LOCAL and GLIgl showed broadly similar adjusted associations with uncontrolled ACT, while yielding different sensitivity-specificity balances by sex. This sex-stratified divergence is clinically meaningful: it implies that obstruction thresholds may capture symptom burden differently in women and men, potentially reflecting differences in symptom perception, airway caliber relative to lung size, comorbidity patterns, and phenotype heterogeneity. The key point is not that one equation “wins” universally, but that equation choice changes who is labelled obstructed, and that label aligns imperfectly with symptoms, especially when symptom prevalence is high. 26
The exploratory ROC-derived cutpoints should be interpreted cautiously. Youden-optimal thresholds are mathematically anchored to the sample distribution of symptoms and impairment, and they can drift substantially from LLN when the outcome (ACT≤19) is common and when the predictor has limited resolution or weak monotonicity with symptoms. This is why ROC cutoffs differed by sex and, for some models, produced non-intuitive thresholds. Such results are useful as hypothesis-generating evidence about discordance between symptom control and obstruction, but they are not a substitute for the clinically standard LLN boundary and should be framed as supplementary. 25
Strengths, limitations, and future directions
This study has several strengths. First, to the best of our knowledge, this is the first study to compare LOCAL, GLIgl, GLI2012_cauc, and GLI2012_other in the assessment of spirometric impairment and ACT-defined symptom control in Jordan. Additionally, the adequate sample size enhances the generalizability and statistical power of the study’s findings. Moreover, ACT is a validated measure with a widely used cut-off of ≤19 for poorly controlled asthma, supporting its use as an outcome anchor for binary analyses. Finally, all spirometry tests were conducted by the same trained technician using the same hospital device, ensuring procedural consistency. Nonetheless, some limitations should be acknowledged. First, the cross-sectional design limited our ability to establish causal relationships. Additionally, unmeasured confounding variables, such as environmental exposures or socioeconomic status, may have influenced the results. Finally, the results underline the limitations of treating ACT as a diagnostic reference standard for physiological impairment: uncontrolled symptoms are common and clinically important, but they are not synonymous with persistent airflow limitation. The high prevalence of ACT-defined uncontrolled symptoms in the analyzed sample inflates PPV and depresses NPV, meaning that predictive values should not be over-interpreted, and comparison should focus on associations, discrimination (AUC), and clinically meaningful trade-offs.
Future work should validate these findings in an independent adult cohort and consider outcome anchors beyond symptom control alone, including exacerbation risk, healthcare utilization, and longitudinal change in lung function. It would also be valuable to evaluate whether equation-specific classification differences translate into clinically relevant management differences (e.g., step-up decisions, referrals, or recognition of fixed airflow limitation), especially in settings where selection between GLI2012_cauc and GLI2012_other is uncertain or inconsistently applied. 20
Conclusion
In this adult cohort, equation choice influenced the classification of spirometric impairment and its alignment with asthma symptom control, but overall discrimination of uncontrolled ACT by spirometric impairment remained modest. Continuous ACT analyses showed consistent positive associations with FEV1 and FVC z-scores across equations, yet the explained variance was low, reinforcing that symptom control cannot be inferred from spirometry alone. Using equation-specific below-LLN classification, defined by the 5th percentile of each equation’s reference distribution and equivalent to z-score ≤ -1.645, is the most defensible approach for defining abnormality, while ROC-derived thresholds should be restricted to exploratory or supplementary reporting. The practical implication is that clinicians should interpret spirometry as a complementary tool for risk assessment and phenotyping rather than as a proxy for symptom control, and future validation studies should prioritize outcome-anchored thresholds and external replication across sex and population subgroups.
Supplemental material
Supplemental material - Impact of switching between different spirometric reference equations on the assessment of asthma severity and control among jordanian adults
Supplemental material for Impact of switching between different spirometric reference equations on the assessment of asthma severity and control among jordanian adults by Walid Al-Qerem, Anan Jarab, Khaled Al-Oweidat, Anas Atef Alrawashdeh, Abbas Iter, Walaa Ashran, Dina K. Al-Hashaki, Amir R. Aljayeh, Anas Mohammed, Lama Sawaftah, Yousef Mimi, Maher Khdour in Chronic Respiratory Disease.
Footnotes
Ethical considerations
The study was conducted according to the ethical principles of the Declaration of Helsinki. The authors have obtained ethical approval from the Institutional Review Board (IRB) committee of the Jordan University Hospital (Reference No. 10/2025/8377).
Consent to participate
Written informed consent has been obtained from the participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings are available upon reasonable request from authors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.