
Abstract
Sensory processing shapes how people respond to environmental stimuli, influencing their ability to regulate themselves, make choices and participate in activities. Evidence indicates that people with mental health problems often experience sensory-processing difficulties that reduce rehabilitation participation. Secure forensic mental health settings are designed to manage behaviours that challenge; however, research indicates the physical environment not only limits opportunities for meaningful participation in rehabilitation activities but may also influence sensory experiences. Despite the interplay between the secure environment, sensory processing and participation, these concepts are seldom discussed in the literature. This qualitative study aimed to explore service users’ experience of sensory processing and occupational participation. Five male service users shared their lived experience through semi-structured interviews. Reflexive thematic analysis was used to construct meaning. Five main themes were developed: (a) Rules and procedures limit sensory self-management; (b) Perceptions of participation opportunity vary; (c) Restricted environments shape sensory experience; (d) Opportunities exist for improvement and increased engagement; (e) Kindness restores comfort and sensory security. These findings indicate secure environments should be adapted to address sensory processing needs to promote participation. Further research is needed to build on these findings and develop sensory-informed services.
Introduction
Sensory processing refers to the nervous system's function of processing intrinsic and extrinsic sensory input to generate behavioural responses (Dunn, 2001). This neurological function is a universal human experience shaped by context and environment (Williams, 2017), as it links individuals to their natural and built surroundings (The British Standards Institution, 2022). Responses include not only the capacity for emotional regulation but also the ability to perform activities, therefore influencing mental and physical health (Bailliard et al., 2022). For example, if the environment is too bright or too noisy, a person may struggle to focus on tasks or relax. When environmentally rooted sensory experiences align with sensory preferences, individuals are better able to participate meaningfully in daily activities, also referred to as occupations (Bailliard, 2015). This occupational participation is best defined as engagement in meaningful activities that individuals want or need to do (The World Federation of Occupational Therapists, 2025) and has been inextricably linked to enhanced quality of life (O’ Flynn et al., 2018).
It follows that when an individual's sensory preferences are met through personalised adaptations of occupations or environments, their ability to participate is likely to improve (Dunn, 2001) and potentially their quality of life as well. However, growing evidence suggests that individuals with mental health issues experience sensory processing differences, such as feeling over- or under-stimulated by sensory information. Environmental sensory mismatches, including excessive noise or restricted space, can lead to withdrawal and reduced participation (Andersson et al., 2021).
Forensic mental health services are designed to support recovery while also ensuring safety and public protection (Connell, 2016). This dual function may produce tension between the need to facilitate therapeutic activity and to provide containment. This can result in highly structured environments which not only restrict autonomy (Seppänen et al., 2018) but also reduce the therapeutic potential of the service. For example, a service user who is sensitive to noise may avoid group therapy in a ward environment that echoes due to a lack of soft furnishings. This lack of participation may be a barrier to their progression in rehabilitation. Indeed, the literature indicates that service users have described secure environments as boring (Bowser et al., 2018), over-regulated or monotonous (Tomlin et al., 2020) and as places where time can feel wasted (Farnworth et al., 2004).
Understanding sensory processing and occupational participation in secure settings is essential for creating sensory-informed therapeutic spaces that foster occupational participation. In restricted environments, adapting surroundings to meet sensory preferences presents a greater challenge due to potential risk. It therefore requires careful and collective consideration. While current trends are rightly towards a greater use of community-based care, there is growing recognition of the need to enhance the quality of life for individuals requiring longer term secure admissions (Holley et al., 2020).
Recent literature has highlighted the need to better understand sensory processing issues in mental health populations (van den Boogert et al., 2022). This recognition has prompted the development of initiatives to increase service users’ sensory awareness and improve self-regulation skills, including the introduction of sensory modulation programmes (Machingura & Lloyd, 2017). Within this broader sensory modulation approach, an emerging body of research suggests that inpatient environmental adaptations, such as sensory rooms and equipment, can improve self-regulation (Dawson et al., 2025; Haig & Hallett, 2023). Wiglesworth and Farnworth (2016) focused on the introduction of a sensory room in a secure setting, with quantitative data indicating reduced service user stress alongside positive staff perceptions reported in the qualitative findings. Although these interventions indicated reductions in distress, they did not explore their impact on participation from a service user perspective.
A qualitative study explored autistic individuals’ sensory experiences in prison settings (Vinter et al., 2023). This enabled the authors to generate tailored recommendations to improve conditions, including greater access to vocational rehabilitation. These findings highlight the importance of understanding how sensory needs influence individuals’ experiences within restrictive environments. However, research exploring forensic mental health service users’ lived experiences of sensory processing and occupational participation is limited.
Research Aim
This qualitative research explored forensic mental health service users’ inpatient experiences of sensory processing in relation to occupational participation.
Methods
Open Science and Transparency
The data are not publicly available due to confidentiality and ethical restrictions related to participant privacy. Sharing the data would compromise the consent participants gave to take part. No preregistration was conducted.
Qualitative Approach and Research Paradigm
A qualitative descriptive approach was adopted to investigate service users’ lived experiences. The study was informed by phenomenological concepts of meaning and interpretation (Dibley et al., 2000), enabling exploration of contextually situated experiences of sensory processing and occupational participation. Reflexive thematic analysis (Braun & Clarke, 2021) was used to analyse the data and construct themes. This study formed part of a broader PhD thesis that also included a scoping review and a second qualitative study with occupational therapists.
Researcher Characteristics and Reflexivity
All researchers are occupational therapists with experience in academia and clinical mental health practice. Being insider researchers (Braun & Clarke, 2021) indicated the suitability of a qualitative approach, underpinned by phenomenology, to harness reflexive researcher positionality and offer a more nuanced understanding of the phenomenon under exploration (Dibley et al., 2000). However, this insider position also posed a risk of bias. To chart perceptions, reflections and decision-making, a reflexive log was used throughout the research journey (Palaganas et al., 2017) and discussed within team meetings.
Context
Participants (N = 5) were recruited from a single male forensic mental health inpatient setting in the United Kingdom. All participants therefore shared the same ward environments, which enabled the generation of a deeper, rather than broader, phenomenological dataset. As the service was male-only, the absence of female participants represents a limitation of the study.
Sampling Strategy
Following ethical approval, the Chief Investigator (CI), the first author, recruited a site-based Principal Investigator (PI) to act as a gatekeeper for participant recruitment. The PI's familiarity with the service supported careful consideration of participant suitability and liaison with clinical teams. Inclusion criteria were age ≥18 years; a service contact of at least 30 days; current or recent admission under a mental-health section (not a prison section); approval from the PI and Responsible Clinician; capacity to provide informed consent; and willingness/ability to take part in an online interview. Current or recent inpatient status was defined as having been an inpatient within the previous 2 years. Using a purposeful sampling strategy (Vandermause & Fleming, 2011), the PI identified five participants interested in sharing their lived experience of the environments from sensory and participatory perspectives. Smaller purposive samples permit in-depth exploration of lived experience (Dibley et al., 2000).
Ethical Issues Pertaining to Human Subjects
Forensic mental health patients are viewed as potentially vulnerable due to their detention status and the inherent power imbalance (Coffey, 2006), and this was carefully considered during the consent process (Völlm et al., 2017). Participants were assessed as having the capacity to provide informed consent, and their participation was entirely voluntary. Prior to the commencement of the research, a favourable peer-reviewed opinion was provided by both the University Research Ethics Committee and Ref. 2792 and the United Kingdom National Health Service ‘Health and Research Authority’; Ref. 21/NW/0262 . A University risk assessment and data management plan was followed, outlining key ethical considerations related to consent, confidentiality and secure data management. Procedures complied with the United Kingdom Data Protection Act (2018), and pseudonyms were used to preserve participant anonymity.
Techniques to Enhance Trustworthiness
The 21 items in the Standards for Reporting Qualitative Research (O'Brien et al., 2014) guided the presentation of findings, increasing structure and rigour in this process. The United Kingdom Health and Research Authority provided a peer-reviewed process prior to research commencement, to confirm that the research design was ethically sound. Credibility was supported through contemporaneous audit trails using a reflexive journal. Reflective notes were kept during the interview and analysis process, then discussed in supervision to demonstrate transparency (Palaganas et al., 2017). Following the analysis, participants were provided with a one-page visual diagram summarising the findings and invited to provide comment.
Data Collection Methods
The PI verbally invited participants to an interview and provided them with a Participant Information Sheet. Consent was documented using a signed Informed Consent Form and verbally confirmed at the beginning of the interview.
Participants linguistically mediated their lived experiences (Gadamer, 1975) through online, semi-structured interviews with the CI. To orient participants to the topic and gauge baseline understanding, they were asked about their awareness of sensory processing. All reported limited formal awareness, which shaped the discussion's direction and the inductively constructed themes. Open-ended questioning (Dinkins, 2005) and techniques such as incomplete questions (Vandermause & Fleming, 2011) guided participants through a deeper exploration of their experiences. The interview questions were divided into four sections: understanding of sensory processing, environmental experiences, activity provision and a non-directive offer to share their final thoughts on the topic area (Dibley et al., 2000). Example interview questions included: ‘Can you describe the environment of the ward you are on?’ and ‘Is there anything that stops you from taking part in the activities on the ward?’
With participants’ consent and PI support, interviews were recorded and stored securely for the research team's access. The first author familiarised themselves with the data and completed full interview transcriptions, which were securely stored on a password-protected university server in accordance with the United Kingdom data protection requirements. The recordings were destroyed once the anonymised transcripts were analysed.
Participants
Five participants were recruited (see Table 1). To protect participant identity, the demographic data has been presented broadly, and specific details relating to the setting are not disclosed.
Participants’ Anonymised Demographic Information.
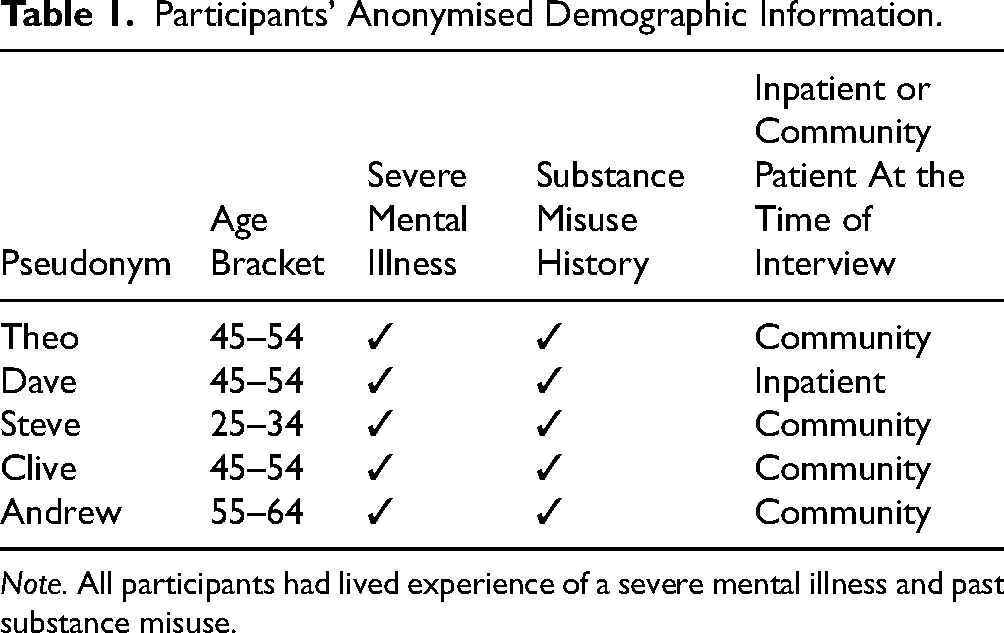
Note. All participants had lived experience of a severe mental illness and past substance misuse.
Data Analysis
The first author analysed the data using Braun and Clarke's (2021) six-phase reflexive thematic analysis framework. This involved familiarisation with the data through transcription and repeated reading of transcripts; generation of initial codes; development and review of themes; refinement and naming of themes; and production of the final report. Analysis was conducted using paper transcripts and flip-chart notes, and later NVivo 12 was used to support theme development. Iterative reading of individual transcripts and the full dataset was considered alongside the first author's concurrent clinical work in a similar environment. Coding, theme development and reflexive journaling were used during structured monthly full-team research supervisions. All supervisors and experienced qualitative researchers contributed to the analysis. Team discussions were used to critically examine assumptions, maintain interpretive openness and manage the potential negative impact of researcher bias. Final themes were refined with reference to relevant forensic mental health and philosophical literature.
Findings
Participants demonstrated limited formal awareness of the term sensory processing; however, they were able to describe rich embodied experiences of the ward environment and its influence on participation. The following themes capture participants’ sensory experiences, which are embedded within their broader discussion of the hospital environment. Rather than a structure being driven purely by the researcher's agenda, points related to occupational participation are presented alongside direct references to sensory processing to acknowledge participant priority in describing their experiences.
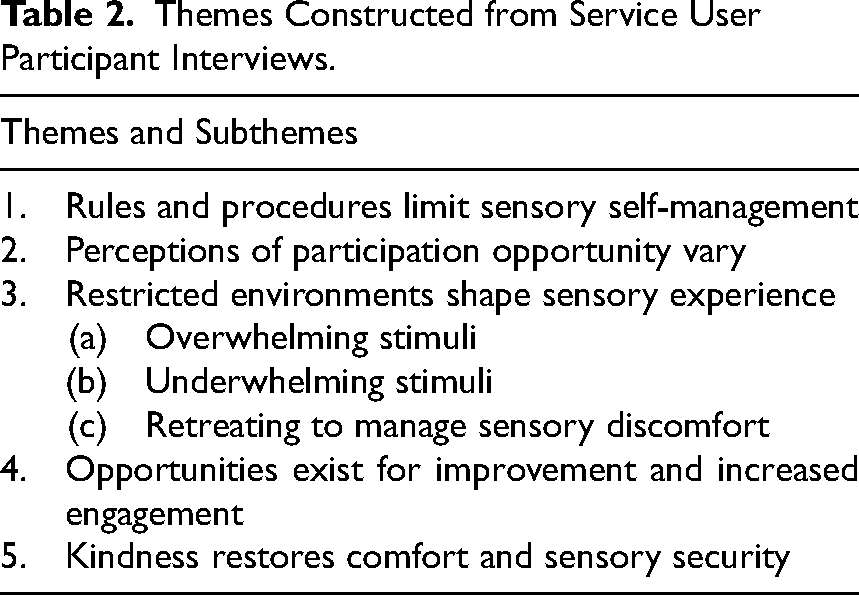
This section outlines the themes derived from the analysis, supported by representative quotations. Themes were developed through iterative engagement with the data. In line with a qualitative descriptive orientation, themes are presented with minimal interpretation in the Findings section, with more extensive interpretive analysis undertaken in the Discussion section. In total, five main themes and three sub-themes were identified, as summarised in Table 2.
Themes Constructed from Service User Participant Interviews.
Rules and Procedures Limit Sensory Self-Management
Participants referred to their lack of control within the environment. The regime was described as a barrier to service users’ ability to self-manage their sensory preferences.
Upon admission, participants were instructed on what was permitted, including restrictions on consumable items that many people rely on for sensory regulation. Sort of taught boundaries very quickly … like not smoking and not having caffeine and things like that. But you get used to that you know. – Theo
Lack of autonomy was also felt regarding sensory comforts and activities meaningful to participants in the communal areas. Theo – So you don’t have loud music … you can put the telly up but they make you turn it off for dinner and stuff like that … again instructing that it's their telly and if they want it off they can you know have it switched off. – Theo
This restriction extended to their personal space within their bedrooms. So you don’t get a t.v. stereo or anything like that (.) so basically just a big room with cupboards and drawers in. – Steve
The rules of the hospital removed personal control over activities which typically provide sensory comfort.
Perceptions of Participation Opportunity Vary
While all participants emphasised the importance of access, there were different perceptions of availability. I did anything from model making … wood work … I did a lot of OT stuff (.) patient forum (.) I was invited to the meetings … I set things up for the hospital…. – Clive
Whereas other participants cited a lack of opportunities. There's not enough to do … more activities … anything to just break up the monotony of being in hospital. – Andrew It's a massive thing of boredom on the induction ward (.) pacing around bored out of my brains. – Dave
While some participants perceived opportunities as adequate and others did not, all were reliant on staff for access to activities. This dependence led to frequent boredom, particularly in high-acuity areas, where service procedures and the sensory and physical environment restrict participation.
There was also recognition of the role of personal agency in relation to participation – the need for a readiness for change, and a desire to move forward. You just need to remember that if you really do want to get out and start living a life you kind of need to engage a bit. – Steve
However, service users are not always ready to participate, particularly when admitted. When you first come here you aren’t in the right frame of mind to participate. – Dave When I first got to the admissions ward I wasn’t busy … all I did was eat and sleep. – Steve
There is also an added pressure created by an awareness of participation being monitored and a fear that lack of participation is pathologised as a clinical concern. Sometimes you don’t feel like participating and then it's reflected on your mental health … it does reflect on your notes which gets fed into your CRMS (Clinical Review Meetings) … so you have to be on best behaviour all the time and that sometimes can get very exhausting. – Theo
Participants sensed the need to participate, even if they did not want to, in order to progress through the system.
Restricted Environments Shape Sensory Experience
Alongside the influence of rules and participation opportunities, participants described some pervasive sensory factors in the environment. These were experienced as impactful.
Overwhelming Stimuli
Participants experienced environments designed to manage behaviours which challenge as difficult, particularly on the admissions ward. These issues impacted everyone's daily experience. The induction ward for instance where people first come is very loud very stressful you know very full on (.) quite uncomfortable at times (.) – Dave
This participant links the noise level with a feeling of stress. Note the use of the word induction, a frequently used word in reference to this ward, instead of admission; this will be discussed later.
Participants recounted the impact of the lights of the hospital on their daily life, and the lights on the wards were referred to by all participants. Lighting was experienced as pervasive and unhelpful. You can nearly read a book with all the lights off because the lights in the hallway are on … no darkness in the rooms. – Dave
There was a sense that the lights were unescapable, even in their bedrooms and even at night, and one participant made a direct link between this negative sensory input and his state of mind. Always fluorescent which gets on your nerves after a while …. – Andrew
This is another example of service users’ lack of control over the sensory environment. These lights offered no adjustable controls, were on all the time and negatively impacted the lived experience.
This lack of autonomy over the sensory environment continued with discussions on the acoustic environment. It could be alarms going off (.) if someone is misbehaving then an alarm would go off and they would respond so you have alarms going off quite often erhm it was kind of loud (.) some people could be louder than others. – Steve
As with the hospital light, noise was also perceived as pervasive day and night. Noise is much louder so that people will be shouting at 6 o’clock in the morning you know waking people up and things like. – Dave
The noises within the environment were described as unpredictable and unsupportive. The auditory environment was experienced as challenging and had an impact on service users’ daily experiences.
Underwhelming Stimuli
Alongside the unsupportive lights and noise, the interior of some of the wards was described as uninviting and the experience of these environments was described as unhomely. Big chunky furniture that you can’t pick up or move … no pictures on the walls or very boring pictures … it was scruffy looking generally but just bland you know sterile. – Andrew
Alongside the stark descriptions of the admissions ward, participants’ experiences of being in the Extra Care Areas (ECAs) were described as punitive. I find it's like being back in a police station. – Theo
The colour of the walls in these areas was discussed, as this increased the sense of discomfort, rather than instilling calm. If someone is misbehaving then you’ve taken them to ECA and you want them to calm down sitting in a wall a room with four walls what are just white isn’t very calming. – Steve All very white very clinical very (.) sort of clean erhm very hospital like. – Dave
These descriptions illustrate that white walls not only fail to instil calm, but also remind participants of custodial or medical environments that carry negative associations for them.
Retreating to Manage Sensory Discomfort
Participants wanted to remove themselves from the communal spaces designed to encourage opportunities to socialise and participate. Leaving these communal areas was seen as the solution to the sensorily challenging environment. The atmosphere isn’t relaxed it isn’t calm (.) because you could have up to five or six people what are quite unwell what are (.) kicking off (.) you just have to take yourself away from it. – Steve
Some had developed skills to manage the noise of the hospital. I’d sit in my room (.) put ear defenders on and (.) meditate that was my way of (.) erhm living in the environment. – Clive
This participant described extreme measures to manage the complex sensory environment of the communal spaces on the ward. Putting ear defenders on prevents this participant from developing the pro-social skills these environments are seeking to support.
Opportunities Exist for Improvement and Increased Engagement
Not all wards were described with such negative descriptions. Once service users transitioned from these environments to rehabilitation wards, their experiences improved. The ward I’m on now is much more relaxed the clientele on there are much more together …. Actually to look at it it's very similar (.) to be honest it's the atmosphere amongst the people that changes the atmosphere. – Dave
Discussions of the social, sensory and physical aspects of the environment highlighted that the environment is shaped by more than just its visible elements. During the interviews, participants were asked their opinion on improvement ideas. Suggestions for improvements included softening the sensory environment. It would be better if they had something on the walls … beanbags in there and a sofa. – Steve
With recognition that design had to meet the needs of service users when they were at their most vulnerable. They get paranoid with people behind them so they try and have their backs against the wall … so they want something that would enclose them (.) like a comfort blanket … with soft furniture. – Clive
There were suggestions for developing activity provision, in particular focusing on getting ready to return to the community with a sense of purpose in their occupational participation. Vocational stuff would be immensely useful. – Andrew They don’t prepare you very well for getting out. – Dave
While there was criticism of the activities on offer, there was also recognition that staff were restricted. You can see they are trying their best. – Theo
Participants appreciated the support staff provided when they were ready to participate.
Participants also mentioned hospital patient forums as a positive space for connecting with others and then contributing to service operations. One participant expressed a desire to share with others a positive experience of an occupation that they found health-promoting. I found model making for me cause I suffer from depression and PTSD … and a lot of people that I talked to found it very (.) therapeutic … we was going to take around the wards … and there was a lot of interest. – Clive
Engaging in this meaningful occupation empowered the participant to contribute to the hospital community.
Participants described how supportive social environments boosted self-worth and participation. Participants valued opportunities for activity, but the admission and ECA areas were seen as restrictive and understimulating, leading to boredom and frustration. Rehabilitation wards were experienced more positively, but with requests for an increase in vocational activities, a greater focus on community reintegration and sensorily improved environments to support participation.
Kindness Restores Comfort and Sensory Security
Alongside participants sharing their experiences of the sensory environment, they also discussed the social and attitudinal environment and how important it was to their progression. The following participant quotation highlights the importance of a therapeutic relationship for an inpatient, noting that a sense of forgiveness from staff can be perceived by the inpatient as acceptance, which can support participation. By creating these occupational opportunities, service users may have increased motivation to participate, improving their self-worth. When you have done something as serious as I had you don’t really have big expectations for yourself …. but they were really nice saying well come and do this and come and do that and you’ll enjoy it and you start to enjoy it and then you start to give again and receive again sort of like so it's a good little learning curve like a stepping stone … that takes you from out of that prison environment and allows you that they are there to help sort of thing and that they play games and things like that and they are prepared to share their time with you in a nice manner sort of thing. – Theo
This highlights the importance of experiencing the kindness of others to recalibrate negative self-perception and move forward with rehabilitation. This is part of the many factors which shape environments in which individuals feel comfortable participating.
Discussion
This research explored forensic mental health service users’ perspectives of sensory processing and the influence this had on participation in meaningful activities, also known as occupations within occupational therapy. Participants shared their experience of sensory processing and emphasised the value of participating in occupations within these settings. They also described barriers that hindered access and negatively influenced participants’ experience of the environment.
The interviews highlighted how sensory, physical and attitudinal aspects of different wards shaped the experience for these service users. The stark sensory environments of admission wards or of areas designed to manage more challenging behaviours, often referred to as ECAs, were experienced as unsupportive at a time when participants were at their most vulnerable. References to the untherapeutic description of the ECA and the negative impact on sensory experience support the suggestion that unmet sensory needs can hinder the neurological function of sensory processing and affect emotional responses (Brown, 2002). Rehabilitation wards were experienced more favourably. The findings highlight that sensory processing is intrinsically linked to environmental context (Clark, 2018). Each space needs to be viewed separately; not all wards are the same.
Although perceptions of opportunities for participation varied, participants predominantly reported a lack of access to and choice in meaningful activities. This was especially so in settings designed to manage behaviours that challenge, where boredom may fuel aggression (Bowser et al., 2018), which is contrary to the services’ intended goals. Positive shifts in terms of rehabilitation were perceived to be linked to service users’ own agency and readiness for change. This supports the notion that experiences of the environment are influenced by multiple components, both intrinsic and extrinsic (Brown, 2002).
Many participants expressed a sense of passivity, feeling controlled by the institution and that rules restrict sensory comfort. However, some also shared positive reflections, particularly on the role of kindness in improving their ability to participate. The literature has previously established that sensory processing influences activity choices (Clince et al., 2016) and that occupational participation is shaped by multiple interacting factors, highlighting its transactional nature (Cutchin & Dickie, 2012). The findings of this research support both points. Participants valued activities in inpatient settings but also described them as monotonous. Similar findings from O’Connell et al. (2010) described a lack of individually tailored occupational opportunities.
These built environments were originally designed to manage risk and prevent escape, but also to be experienced as therapeutic spaces (Department of Health, 2011). Participants noted that, while wards differed, restrictive and low-stimulus areas led to untherapeutic experiences and hindered participation. These stark spaces may create sensory dissonance (Bailliard, 2015), contributing to discomfort and alienation within environments that service users cannot leave or modify.
Reference to some uncomfortable environments, compounded by sterile white walls, supports previous quantitative research indicating that the colour white is not universally experienced as calming (Barrett et al., 2015; Zhang et al., 2022). Indeed, sensorily deprived spaces have been shown to potentially trigger psychosis (Daniel & Mason, 2015). These factors are likely to negatively impact wellbeing and participation, as the forensic mental health environments in which participants were based were experienced as dominating and controlling, indicating that these environments are not designed in a way that naturally facilitates participation.
One method of improving service user experience, which is gaining traction in mental health settings, is the proposed enhancement of inpatient environments, including Ulrich et al.'s (2018) work on environmental re-design to improve wellbeing and reduce aggression. Indeed, the need for improved environmental design has been recognised in forensic mental health estates (NHS England, 2023; Seppänen et al., 2018). As highlighted in this research, service users are well placed to be involved in these design discussions.
While addressing risk potential must remain a priority, this research demonstrates the potential impact of an environment designed for risk management on participation, and this consideration needs to be at the forefront of forensic mental health inpatient redesign initiatives. The subtheme ‘Overwhelming stimuli’ highlights the need to assess the internal environment for individuals at their most vulnerable points during their admission. If the sensory features and other physical factors of an inpatient environment is limiting participation and creating alienation, the right to access occupations becomes an issue of human rights (Whiteford et al., 2020). These findings support concerns that some inpatient environments are not experienced as therapeutically as the designers intended. They may increase rather than decrease aggressive behaviour (Ulrich et al., 2018), leading service users to perceive hostility and withdraw from these environments.
Understanding Contextually Driven Sensory Processing
Participants’ limited formal understanding of sensory processing aligns with Wallis et al.'s (2018) assertion regarding a general lack of awareness of sensory processing needs. These findings support Brown's (2002) view that educating people about environmentally influenced sensory needs can improve self-management and may reduce feelings of disempowerment within forensic mental health services.
Greater awareness of sensory processing will improve services for both short-term and long-term admissions by identifying how to manage personal sensory needs and, ideally, creating more comfortable environments. Enhancing sensory environments may then have a positive influence on both service user and staff wellbeing.
Sensory Rooms and Transitions
Suggested environment improvements included softening and adapting spaces. While sensory rooms have been introduced in some inpatient mental health settings, existing research largely reflects staff perspectives (Wiglesworth & Farnworth, 2016) with limited input from male service users (Novak et al., 2012). This is notable given evidence to suggest females are more likely than males to be aware of or identify sensory differences (Engel-Yeger, 2012). Given that 88% of the United Kingdom's forensic mental health service users are male (Ministry of Justice, 2022), tailored approaches are needed to account for the fact that male service users may have different sensory needs.
However, the value of costly sensory rooms, which services assume support sensory needs, is being questioned. For example, recent research highlighted autistic individuals’ preferences for controllable and individually personalised environments (McCabe et al., 2025). In secure settings, sensory rooms often require supervision (Wiglesworth & Farnworth, 2016) and may reinforce the misconception that sensory needs are confined to specific spaces, drawing attention away from the everyday, every environment nature of sensory processing. These findings demonstrate that service users offer valuable suggestions for adapting ward environments, including specially designated rooms designed for relaxation, to improve sensory comfort. These lived experiences provide an important foundation for future re-design discussions.
Experiencing and Enhancing the Inside Environment
A recurring theme in this research was the stark divide between the hospital's interior and the exterior world, with particular emphasis on the transition between them. Wanting to be outside of the hospital was described as a key client-driven goal. Comfort, positive participation and increased well-being were associated with outside the hospital, not inside, where the interior was described as uninspiring.
Autonomy over inside everyday activities is often restricted, due to the inherently restrictive nature of the service (Ministry of Justice and HM Prison and Probation Service, 2020). This emphasis on security frequently results in sensory experiences more closely aligned with a prison environment, shaped by stringent environmental risk management procedures. Perceptions and experiences of restrictive environments can shape sensory experiences, such as the sound of alarms, echoes from the lack of soft furnishings and constant exposure to harsh lighting. These internal environmental features will therefore affect occupational participation.
There was a reference to sleep being used to pass time, supporting previous research on time use in secure settings (Stewart & Craik, 2007). However, within this research, even the most fundamental occupation, sleep, is disrupted by the sensory aspects of systemic procedures, such as the intrusiveness of constant night-time lighting. These practices, while operationally useful, compromise the sleep environment. Light disturbance is a recognised issue in inpatient psychiatric settings, with Horne et al. (2018) identifying night-time observations as a factor in poor sleep with recommendations for environmental adaptations. As noted by Blume, Garbazza and Spitschan (2019), exposure to light at night can significantly impair sleep quality, a finding echoed by this research.
This aligns with broader discussions in forensic mental health research that consider collaboratively developing strategies to minimise such observation-based intrusions (Collins et al., 2022). This research underscores the importance of changes to the internal lighting environment to increase participation and health and well-being.
A proposed change in lighting is one example of an overall improvement that may address the need to adjust the built environment to enhance service user experience (Ulrich et al., 2018). It supports the importance of considering the sensory environment for the inclusion of those with pronounced sensory needs (National Developmental Team for Inclusion, 2020; The British Standards Institution, 2022) because it can reduce stress (Andrade & Devlin, 2015).
Participants described employing various strategies to manage the auditory environment when it became overwhelming, such as retreating to their rooms and using ear defenders. While these self-regulation techniques may offer temporary relief, they often lead to disengagement from the rehabilitative occupations designed by the multidisciplinary team to support a safe and meaningful discharge. This can also limit social interaction and participation in therapeutic relationships, which are often central to rehabilitation goals. This highlights the need to assess and intentionally modify the auditory sensory environment to support participation rather than avoidance.
Kindness Restores Comfort and Sensory Security
When asked to describe the environment, participants initially emphasised the ward's social dynamics, highlighting the central role of interpersonal relationships in shaping their experiences. Participants’ accounts suggested that sensory experience was also shaped by interpersonal cues, including tone of voice and body language, as well as by experiences of kindness or hostility. Within forensic settings, these social sensory experiences may influence feelings of safety and willingness to participate.
These relational descriptions stood in contrast to the researcher's initial assumptions (Gadamer, 1975), which anticipated that participants would focus primarily on the environment's physical aspects. These findings demonstrate the value of an exploratory interview approach, which allows researchers to access participants’ authentic lived experiences (Dibley et al., 2000). By following participants’ leads, researchers are better positioned to gain insight into the realities of their daily experience and what matters most.
This research also reinforces the complex, transactional relationship between environment and occupation, consistent with Cutchin and Dickie's (2012) theory of transactionalism and the World Health Organisation's categorisation of environmental factors as physical, social and attitudinal (WHO, 2013). Participants reported distinct environmental experiences across ward types, with admissions and ECA wards often perceived as unfriendly and as places where they were ‘inducted’ into being patients. Rehabilitation wards were described more positively, with references to improved atmosphere and experiences of kindness, affirming the importance of positive ‘attitudinal’ environments (WHO, 2013).
Small acts of compassion were identified as pivotal to recovery, aligning with core NHS values (Department of Health and Social Care, 2023) and humanistic approaches. This supports the need to continue moving away from impersonal, institution-focused services towards models of care that recognise and respond to the individual (The King's Fund, 2015), thereby allowing the development of environmentally supportive services grounded in kindness and compassion (Hammarström et al., 2020).
Limitations and Recommendations for Future Research
All researchers were occupational therapists, and their shared professional perspectives inevitably shaped the study. However, this was managed transparently through reflexive journaling and regular supervisory discussions. The sample was drawn from a single male forensic inpatient setting, reflecting both the exploratory nature of the study and the practical challenges of recruitment within secure environments. Future research should seek to include female participants and a broader range of forensic jurisdictions to further develop an understanding of sensory processing and occupational participation in different contexts. Additionally, participants’ length of stay was not collected, which may have influenced experiences of the ward environment and should be considered in future research (Cook et al., 2015).
Practice and Policy Impact
While this research is UK-based and may require adaptation elsewhere, the themes highlight considerations for all inpatient settings. Findings indicate the need to reassess inpatient environments, in which sensory dissonance and restricted access to meaningful occupation may impede participation and progress. Participants described challenges with sound, colour and lighting, especially when they were at their most vulnerable. These issues reflect existing literature, with this research contributing exploratory primary qualitative data. Sensory processing and its influence on occupational participation emerged as a significant, environmentally driven phenomenon, reinforcing the need for further research.
Collaboration between service users and clinicians to develop sensory-informed environments and increased meaningful occupation opportunities may foster empowerment, shorten length of stay and improve quality of life. As Tully et al. (2016) suggest, there is room for innovation in practice.
Recommendations align with the five key research themes:
Conclusion
This exploratory research adds to the growing evidence that secure environments must move beyond safety to become therapeutic landscapes. Meaningful activities need to be adapted across different settings, and environmental barriers addressed, to support self-regulation and increase motivation to participate in rehabilitation occupations. Future research should expand participant diversity and explore how occupational participation and sensory processing awareness can be effectively integrated into international secure mental health settings.
Footnotes
Acknowledgments
The authors would like to thank all service user participants, without whom this research would not have been possible.
Ethical Approval
This study was approved by the Ethics Committee of the Faculty of Health at the University of Plymouth (Ethics Code: 2792) on 5 July 2021. A favourable opinion was obtained by the Health Research Authority (HRA) and Health and Care Research Wales (HCRW) – REC reference: 21/NW/0262 on the 29 October 2021. All participants provided written and verbal informed consents prior to participation in the interview. This included consent for anonymised quotations to be used in publications. This research was conducted in accordance with the Declaration of Helsinki.
Informed Consent
Written and verbal informed consents were obtained from all participants prior to participation in this study. Participants also provided consent for anonymised data and quotations to be used in publications.
Author Contribution(s)
Funding
The authors received the following financial support for the research, authorship, and/or publication of this article: The primary author's PhD was self-funded, except for the final year when an NHS department's Continuing Professional Development fund paid the course fee.
Declaration of Conflicting Interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The first author was employed by the National Health Service (NHS) during the data collection phase of this study. The NHS may potentially benefit from the publication of these findings.
Data Availability Statement
The primary data for this study are not publicly available due to privacy and ethical restrictions. However, data may be available from the corresponding author upon reasonable request and with appropriate ethical approvals.
Authors Note
The lead author is an occupational therapist with experience working in secure mental health settings, which informed the study design and interpretation of findings through a reflexive qualitative approach. This study formed part of the authors PhD research, which also included a scooping review and a study which collected practice-based experiences of sensory processing and occupational therapists from an occupational therapy perspective.
Public Significance Statement
Service users of secure mental health inpatient rehabilitation often have limited control over their environment, which can affect how they manage sensory experiences and participate in rehabilitation activities. This study highlights how secure environments influence sensory processing and participation, showing the importance of creating sensory-informed spaces that support comfort, well-being and promote engagement in rehabilitation.