
Abstract
Severe diabetic ketoacidosis (DKA) is a critical medical condition that often necessitates emergency treatment and hospitalization. Although DKA primarily impacts individuals with type 1 diabetes (T1D), its annual incidence among adults with T1D ranges from 4% to 8% following diagnosis. Continuous glucose monitoring (CGM) has become a standard tool for managing T1D and type 2 diabetes (T2D) in patients using insulin or aiming to improve self-management. However, advances in continuous dual glucose-ketone monitoring (DGK) technology offer new possibilities for clinical research and patient care. This article explores the potential applications of DGK in clinical research, with a focus on T1D, while also considering its broader relevance for T2D and other patient populations.
Keywords
Introduction
Severe diabetic ketoacidosis (DKA) is a life-threatening medical condition that often requires emergency department treatment and inpatient care. While DKA mostly affects individuals with T1D, with incidence rates of DKA after T1D diagnosis ranging from 4% to 8% of T1D adults each year, 1 approximately one-third of adults hospitalized for DKA have poorly controlled or newly diagnosed type 2 diabetes (T2D).2,3 It is often associated with insulin deficiency, illness, acute infection, or misdiagnosis in diabetes subtypes.4,5 While individuals with severe DKA typically present with significant hyperglycemia (>250 mg/dL), glucose concentration may be substantially lower owing to additional insulin doses taken as part of sick day management by patients before arrival in the emergency room, or possibly in the setting of extreme exercise or pregnancy. 2 However, the increasing use of sodium–glucose transporter inhibitor (SGLT-2i) in individuals with T1D (off-label) and those with T2D has been associated with “euglycemic DKA” (euDKA), generally defined by blood glucose levels that are only moderately elevated (<200 mg/dL).6–9 These factors, including SGLT-2i therapy, render traditional blood glucose and continuous glucose monitoring (CGM) less effective in detecting the development of DKA.
Recently, the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) updated the 2009 DKA guidelines. 2 In the new guideline, the blood glucose cut point will decrease from 250 to 200 mg/dL, considering that 10% of DKA occurs with euglycemia or near-normoglycemia, especially in SGLT2i users with T1D who may have reduced their insulin dosages too aggressively. 10 This is also an issue in people with T1D who are treated with glucagon-like peptide-1 receptor agonist (GLP-1 RA) therapy. 11 Table 1 summarizes the changes in the 2024 DKA guideline. Notably, all the criteria have been modified, except for pH <7.3. The significant changes in the definition of DKA and the inclusion of quantitative β-hydroxybutyrate (BHB) levels for diagnosis provide strong motivation for the clinical application of continuous measurement of ketones.
American Diabetes Association Diabetic Ketoacidosis Guideline: 2024 Versus 2009
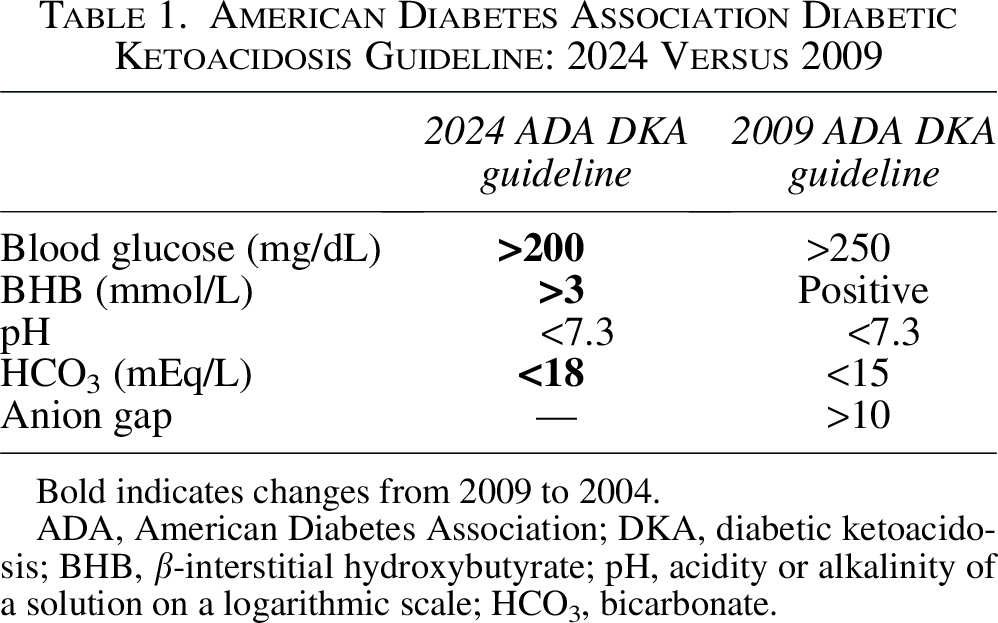
Bold indicates changes from 2009 to 2004.
ADA, American Diabetes Association; DKA, diabetic ketoacidosis; BHB, β-interstitial hydroxybutyrate; pH, acidity or alkalinity of a solution on a logarithmic scale; HCO3, bicarbonate.
CGM has transformed diabetes management, providing important insights into the dynamics of fluctuating glucose levels and their implications for patient care. While CGM has become a standard tool in managing T1D and T2D using insulin or those trying to address self-management behaviors, the emerging technology of continuous dual glucose-ketone monitoring (DGK) presents new opportunities for clinical research and patient care. This article discusses the potential applications of integrating DGK into clinical research, focusing mainly on T1D, while also exploring its broader utility in T2D and other patient groups.
Assessing the safety of new medication classes
Recent epidemiological studies highlight the ongoing challenge of achieving the evidence-based targets for glycemic exposure levels.12–14 However, advancements in diabetes medications and technologies are expanding the range of treatment options that may improve management outcomes.15,16 In recent years, innovative treatments for T2D have emerged, including SGLT-2i medications,6–8 GLP-1 RAs,17,18 and first-in-class medications, such as tirzepatide, a dual GLP1, and glucose-dependent insulinotropic polypeptide receptor agonist,19–22 and finerenone, a nonsteroidal mineralocorticoid receptor antagonist that offers substantial renal and cardiovascular benefits for individuals with T2D and chronic kidney disease (CKD). 23 While these new medications hold promise for improving T1D metabolic management and cardiorenal protection, clinicians face the challenge of weighing their benefits against potential risks, such as DKA, associated with some of these emerging treatments. As reported by Anson et al., increased off-label use of SGLT-2i therapy in T1D increases the risk of DKA, with a lower risk associated with GLP-1 RA formulations. 24
One of the challenges of investigating new medications and their impact on the risk and prevalence of DKA is its low incidence rate, which makes it difficult to study DKA in short-duration trials with small and diverse populations. An early systematic literature review revealed that the incidence of DKA in individuals with T1D varied significantly by country, ranging from 0–56 per 1000 patient-years in eight studies to 0–128 per 1000 people. 25 Clinical trial populations of SGLT-2i in T1D had placebo group incidence rates that were substantially lower,6–9 even lower than the event rates of major adverse cardiovascular events in high-risk T2D. Cardiovascular disease safety trials have traditionally needed trial cohorts ranging in sample size from approximately 7,000 to 17,000 participants.26–28
Given the demonstrated risk of DKA associated with SGLT-2i therapy and the need for statistical efficiency of ketone-related outcomes, investigators are beginning to include ketone monitoring in their SGLT-2i study protocols.29–31 However, even assuming full participant adherence to their prescribed ketone monitoring, measurements from current methods (e.g., urine ketone, capillary blood ketone testing) will not provide sufficient granularity to answer important research questions about the impact of these medications on DKA risk. This is of particular importance because research into ketone dynamics during normal and prolonged fasting in T1D has revealed that even fasted plasma ketone levels at the higher end of the target glucose range (3.9–10 mmol/L) are associated with greater insulin production and urinary excretion. 32 This implies that those individuals with T1D waking up with such levels are “living on the edge,” such that an intercurrent illness, or, as demonstrated in a recent analysis, the use of SGLT-2i medications can interfere with the urinary excretion of ketones and raise circulating plasma levels. 32
DGK represents a promising advancement in diabetes research, particularly for T1D. It offers the ability to measure interstitial BHB, the main metabolic product of fat breakdown and blood ketone elevation. By providing a continuous stream of real-time data on ketone fluctuations, on par with CGM frequency at 5-min intervals (or at least every 15 min to characterize BHB excursions), the use of DGK would enable investigators to better understand the safety profile of these medications in diverse populations. One example of a trial population in which DGK would provide both mechanistic data on the use of SGLT-2i medications in T1D and also a protocol to mitigate DKA events is the Sodium Glucose Co-Transport-2 Inhibition Diabetes and Kidney Function Loss in Type 1 Diabetes (SUGARNSALT) study, which is investigating the effects of SGLT-2i therapy in T1D patients with CKD. 33 However, this study was launched before the broad availability of DGK, and instead uses capillary blood ketone measurements as part of the mitigation strategy.
Developing and assessing mitigation strategies
Two major consensus guidelines define different risk categories for BHB levels in SGLT2i users with T1D. Normal BHB is defined as <0.6 and <1 mmol/L, and the cut point BHB to initiate a risk mitigation strategy is defined as >0.6 and >1.5 mmol/L by the International Consensus Protocol 10 and the STOP DKA Protocol, 34 respectively. Table 2 compares the differences between two commonly used risk mitigation protocols for SGLT-2i users with T1D. It should be noted that the ADA and the EASD guidelines recommend a capillary ketone level of 3.0 mmol/L or greater for diagnosis of even mild DKA. 2
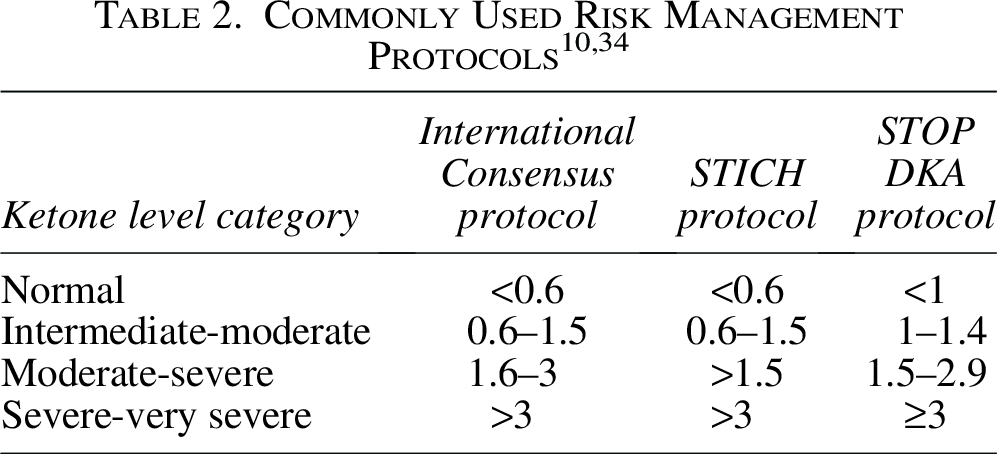
None of these cut points are evidence-based and are without any prospective study, therefore it is not possible to define risk categories. Several expert opinions and consensus recommendations (STICH, 35 International Consensus, 10 STOP DKA 34 ) were published to mitigate the DKA risk in SGLT-2i users with T1D. In addition to regular ketone monitoring, the STICH protocol suggested injecting an insulin bolus, consuming 30 g of carbohydrates, and drinking water, without providing details on the BHB level at which patients should initiate the protocol. The International Consensus suggested administering bolus insulin, consuming 15–30 g of carbohydrates, and drinking 300–500 mL of water hourly if BHB >0.6 mmol/L. 33 The STOP DKA protocol suggested a more complex approach that used both BHB levels and blood glucose levels in the intervention. If the BHB is >1 mmol/L, it is suggested that the protocol is started based on blood glucose levels. 34 Little is known about the effectiveness and safety of these protocols as well as their acceptability by the patients using SGLT2i in T1D.
Early initiation of risk mitigation protocols can cause anxiety and discomfort. On the contrary, late initiation can result in DKA. Therefore, to test any risk mitigation strategy to prevent DKA in SGLT2i users with T1D, the first step should be to properly define the risk categories. DGK could be used to develop and assess mitigation strategies aimed at reducing the risk of DKA in high-risk populations. These strategies could include:
Early intervention protocols
Clinical trials could evaluate protocols that use DGK data to trigger early interventions, such as insulin adjustments, hydration recommendations, or carbohydrate intake, when ketone levels begin to rise. For example, DGK could alert patients and health care providers when ketone levels reach 1.5 mmol/L, prompting immediate action to prevent further escalation. A current trial underway provides guidance for ketone management at ketone levels of 1.0, 1.5, and 2.5 mmol/L, with target levels for ketones <0.6 mmol/L. 29 Trials could also assess whether DGK-based interventions reduce the incidence of DKA compared with standard care. For example, researchers could compare outcomes in patients using DGK with those relying on traditional capillary ketone testing.
Risk stratification
It would be important to know if there are any correlations between specific patient phenotypes (e.g., age, gender, race/ethnicity), and the severity of DKA or the length of time spent in ketosis before clinical DKA develops. DGK data could be used to identify individuals at higher risk of DKA based on their ketone profiles. For example, studies using DGK could investigate whether patients who frequently experience ketone levels above 0.9 mmol/L are more likely to develop DKA in the future. This information could guide personalized prevention strategies, such as intensified education, closer monitoring, or adjustments to therapy.
Long-term risk prediction
In recent studies by Song et al. and Bapat et al., investigators reported that data from systematic use of point-of-care capillary ketone measurements could predict future DKA events.36,37 Involving secondary analysis of clinical trial data in participants with T1D randomized to the SGLT-2i empagliflozin or placebo in which the protocol called for at least twice-weekly well-day capillary blood ketone monitoring, 7 the analysis provided proof of concept that routine capillary measurements of ketone levels on well-days, outside of acute illness, can identify individuals either taking or not taking SGLT-2i who are at higher risk of DKA in the following month to a year. Maximum ketone levels ≥0.8 mmol/L derived from 1 month of monitoring were associated with over a threefold likelihood of DKA regardless of SGLT-2i use. In addition, this prediction was found to be independent of common risk factors for DKA such as female sex or insulin pump use. Rather than having clinicians assess risk factors that are prevalent enough in the T1D population to make them clinically less useful, the finding of well-day peak ketone levels ≥0.8 mmol/L over the course of a month represented the highest prediction regardless of risk factors. These results suggest that the routine use of capillary ketone testing provides an additional strategy to mitigate future DKA events. DGK could further refine these findings by providing continuous data, enabling more accurate risk stratification and intervention. Specifically, rather than DGK having a single threshold to identify when an individual may be entering DKA acutely, such as at a level of 3.0 mmol/L or greater, the DGK could evaluate the distribution for more subtle, well-day ketone elevations of ≥0.8 mmol/L. If an individual’s routine DGK ketone level exceeds the threshold, it could nonurgently prompt DKA prevention interventions, such as optimizing basal insulin and implementing sick day management education to reduce the risk of DKA. Further research examining DGK and DKA risk could determine if other parameters, such as measures of ketone variability, exposure at different ranges, and rates of ketone excursions, could have a greater diagnostic prediction of future DKA risk.
Integration of DGK into automated insulin delivery algorithms
Advanced automated insulin delivery (AID) systems, equipped with sophisticated algorithms, utilize CGM data to adjust basal insulin delivery and, in many systems, correction boluses, based on CGM readings. This is important because of the increased risk of DKA primarily due to occlusions. 38 However, it should be noted that evidence exists to suggest that this DKA risk has been decreasing over time.39,40 Randomized controlled trials (RCTs) have demonstrated that AID systems improve glycemic control and reduce the risk of hypoglycemia in individuals with T1D41,42 and T2D.43,44
Integrating DGK capabilities into AID systems could provide a new layer of safety and effectiveness. Clinical studies could investigate how DGK data can be used to enhance AID algorithms, enabling them to respond to glucose levels and ketone levels. For example, an AID system could amplify the algorithm’s typical insulin delivery when ketone levels rise, even if glucose levels remain stable or only slightly elevated (e.g., developing euDKA), thereby contributing to the prevention of the onset of DKA. Other studies could explore how DGK data can be used to individualize insulin delivery algorithms to match each patient’s unique physiology. For example, patients who are prone to rapid ketone accumulation could benefit from more aggressive insulin adjustments, while others may require less intensive intervention.
Clinical trials could be designed to assess the effectiveness of DGK-enhanced AID systems in mitigating DKA risk during high-risk scenarios, such as pump malfunctions, infusion-site failures, or the use of adjunct therapies, such as SGLT-2i. For example, DGK data could help detect early signs of ketone accumulation, alerting users to take preventive actions in addition to the automated amplification of insulin delivery. Trials could also be designed to compare outcomes in patients using standard AID systems versus those using DGK-integrated systems to determine the added benefit of this technology. Additional studies could evaluate whether these DGK-enhanced systems improve patient-reported outcomes, such as reduced anxiety about DKA and improved quality of life.
Applications beyond T1D
Type 2 diabetes
Although much of the focus on DKA has been in T1D, DGK could also be valuable in T2D trials to assess the safety of new medications and lifestyle interventions (e.g., fasting, ketogenic diets in which carbohydrates are restricted) in T2D. As with the previously mentioned SUGARNSALT study, DGK could also be applied in other conditions, such as CKD and heart failure, where greater ketosis risk may exist—alternatively, under the hypothesis that circulating ketones may have a salutary effect on renal parenchyma by offering an alternative fuel and counteract oxidative stress, inflammation, and fibrosis. DGK in T2D could provide personalized medicine approaches to determine the subset with insulin deficiency who may more likely benefit from insulin or insulin-providing agents in their T2D pharmacotherapy regimen. For those on insulin, DGK would aid in monitoring safe insulin treatment, indicating any insulinopenic states that require attention before escalating to DKA.
Pregnancy
Identifying harmful levels of ketonemia is an ongoing challenge for clinicians in determining the significance of elevated ketone levels during pregnancy for both maternal and fetal health, regardless of diabetes type. Pregnancy causes numerous physiological adaptations that increase the risk of DKA compared with nonpregnant women. While elevated ketone levels are generally associated with hyperglycemia, there may be ketonemia with normal glucose due to a lack of maternal glucose, due to fetal growth, and/or long periods of fasting, such as overnight. 45 This becomes even more challenging with gestational diabetes mellitus, especially in those who are diet-controlled.
Metrics and correlations
A key challenge is establishing standardized reporting of DGK data in trials, which was historically an issue for CGM before the international consensus on the utilization of CGM data in research. 46 Determination of the equivalent of the ambulatory glucose profile for ketones would facilitate greater homogeneity in study designs, strengthening findings from relevant meta-analyses and systematic reviews. A valid starting point would be to report time above 0.6, 1.0, 1.5, and 3.0 mmol/L, as these are consistent with expert consensus cut points, while knowledge of ketone level variability and stability is determined in observational studies and trials.
Nondiabetic populations
In observational studies, DGK could be used to quantify the normal distribution of ketones in different populations. In addition to the various diabetic populations, these studies could include athletes, whose ketone levels may fluctuate due to exercise, individuals with/without diabetes on ketogenic or “starvation” diets, and individuals with acute and/or chronic disorders (e.g., pancreatitis, Cushing’s syndrome, myocardial infarction), or treated with nondiabetes medications (e.g., glucocorticoids, thiazide diuretics, antipsychotics). It is interesting to note in this context that even though 0.6 mmol/L marks the threshold for abnormal ketone levels determined by the distributions in nondiabetic individuals, a recent study has demonstrated that the average ketone concentration achieved in nondiabetic individuals after a 6-day prolonged fast was approximately 4 mmol/L. 47
Summary
DGK offers a new dimension of care by continuously measuring interstitial BHB, the primary ketone produced during fat metabolism. DGK technology can enhance clinical research and patient care, particularly in T1D, by providing granular data on ketone levels and trends. DGK is especially relevant in studies designed to assess the safety of new medications that may pose an increased risk for DKA. DGK could also play a pivotal role in developing and assessing strategies to reduce DKA risk in high-risk populations.
Clinical trials could also assess the effectiveness of DGK-enhanced AID systems in mitigating DKA risk during high-risk scenarios, such as pump malfunctions or adjunct therapies such as SGLT-2i. In addition, DGK data could be used to individualize insulin delivery algorithms.
DGK has broader applications beyond T1D. Data from DGK could be valuable in T2D trials to assess the safety of new medications and lifestyle interventions, such as fasting or ketogenic diets. It could also be applied in conditions that are risk factors for ketosis. It also has potential applications in pregnancy management. Other populations of interest might include athletes, individuals on ketogenic diets, and those with acute or chronic disorders, such as pancreatitis or myocardial infarction. Observational studies could be conducted to identify correlations between ketone development and other factors such as glucose variability, insulin sensitivity, and dietary patterns.
DGK could also be used to investigate the relationship between ketones and other factors, such as time in target glucose range, glucose variability, insulin sensitivity, and dietary patterns. Findings from these types of studies would generate important insights that could inform health care providers and improve patient education on ketone relevance. Table 3 presents examples of potential research questions and study designs that could elucidate our understanding of the potential value and utility of incorporating DGK into clinical trials and other research programs.
Potential Research Applications of Dual Glucose-Ketone Monitoring
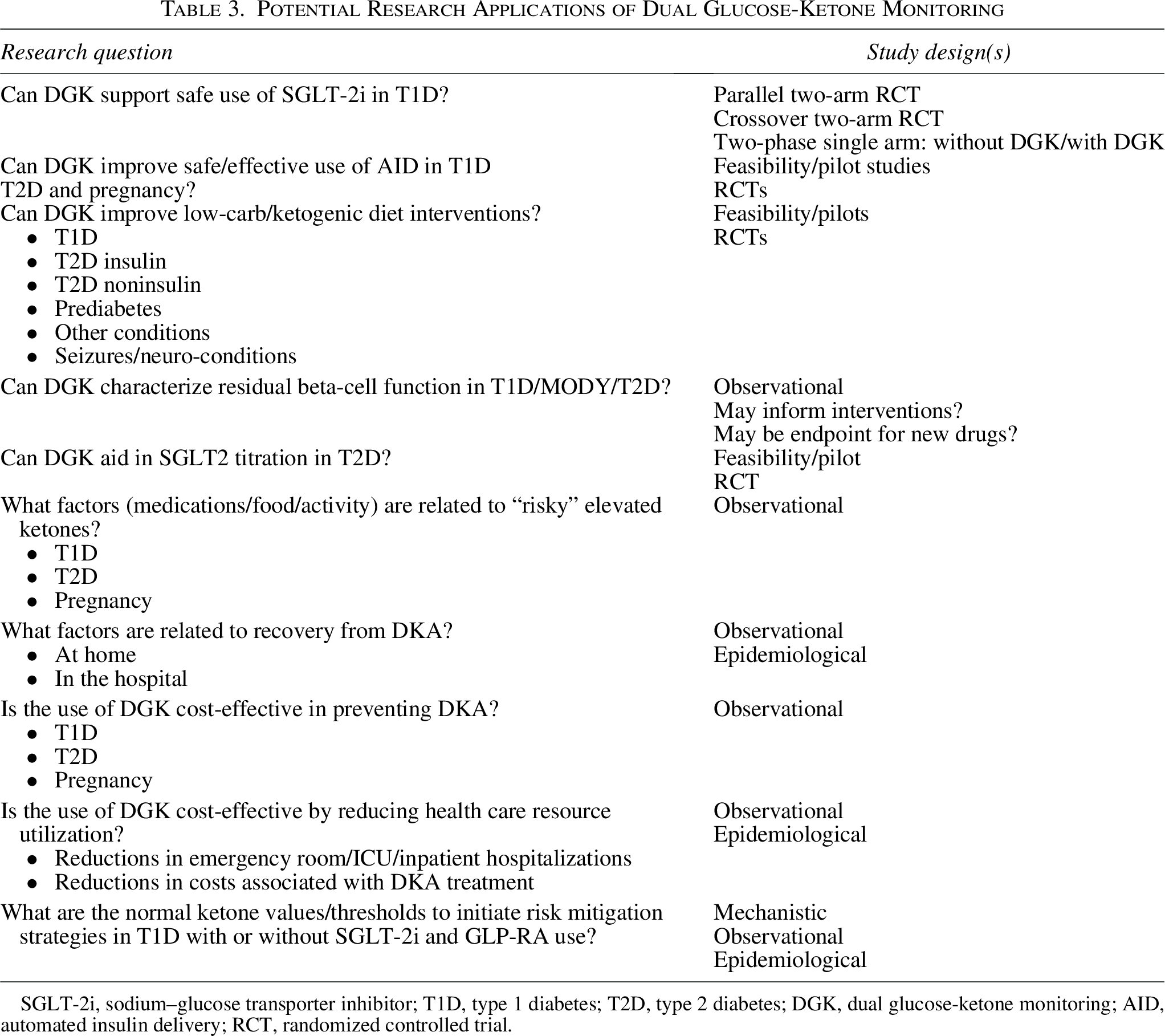
SGLT-2i, sodium–glucose transporter inhibitor; T1D, type 1 diabetes; T2D, type 2 diabetes; DGK, dual glucose-ketone monitoring; AID, automated insulin delivery; RCT, randomized controlled trial.
DGK represents a significant advancement in diabetes research and care, particularly for T1D. By providing real-time data on ketone levels, DGK could improve the safety and effectiveness of emerging diabetes therapies, enhance AID systems, and guide personalized prevention strategies. However, in addition to establishing metrics for assessing DKA risk, standardized protocols for DGK use in clinical trials are needed to ensure consistency and strengthen findings from meta-analyses. This would include establishing ketone thresholds for specific populations and conditions, which is critical for defining clinical interventions. As the technology evolves, DGK has the potential to transform diabetes management and reduce the burden of DKA, improving outcomes and quality of life for patients with diabetes.
Authors’ Contributions
H.K.A., B.A.P., and T.C.D.: Conceptualization, original draft, and review and editing.
Footnotes
Acknowledgment
The authors wish to thank Christopher G. Parkin, MS, CGParkin Communications, Inc., for his editorial assistance.
Author Disclosure Statement
H.K.A. reports receiving research funding from Abbott Diabetes Care, Dexcom, Tandem Diabetes, Medtronic, and Roche. H.K.A. received honorarium for consulting from Dexcom, Tandem Diabetes, Medtronic, and Roche. B.A.P. has received honoraria for educational events from Abbott, Dexcom, Insulet, Medtronic, Novo Nordisk, and Sanofi. His research institute has received funding from the Bank of Montreal and Novo Nordisk for research support. He has served as an advisor to Abbott, Boehringer Ingelheim, Dexcom, Insulet, Nephris, Sanofi, and Vertex. T.C.D. is an employee of Abbott Diabetes Care.
Funding Information
Abbot Diabetes Care funded the development of this article.