
Abstract
Objective:
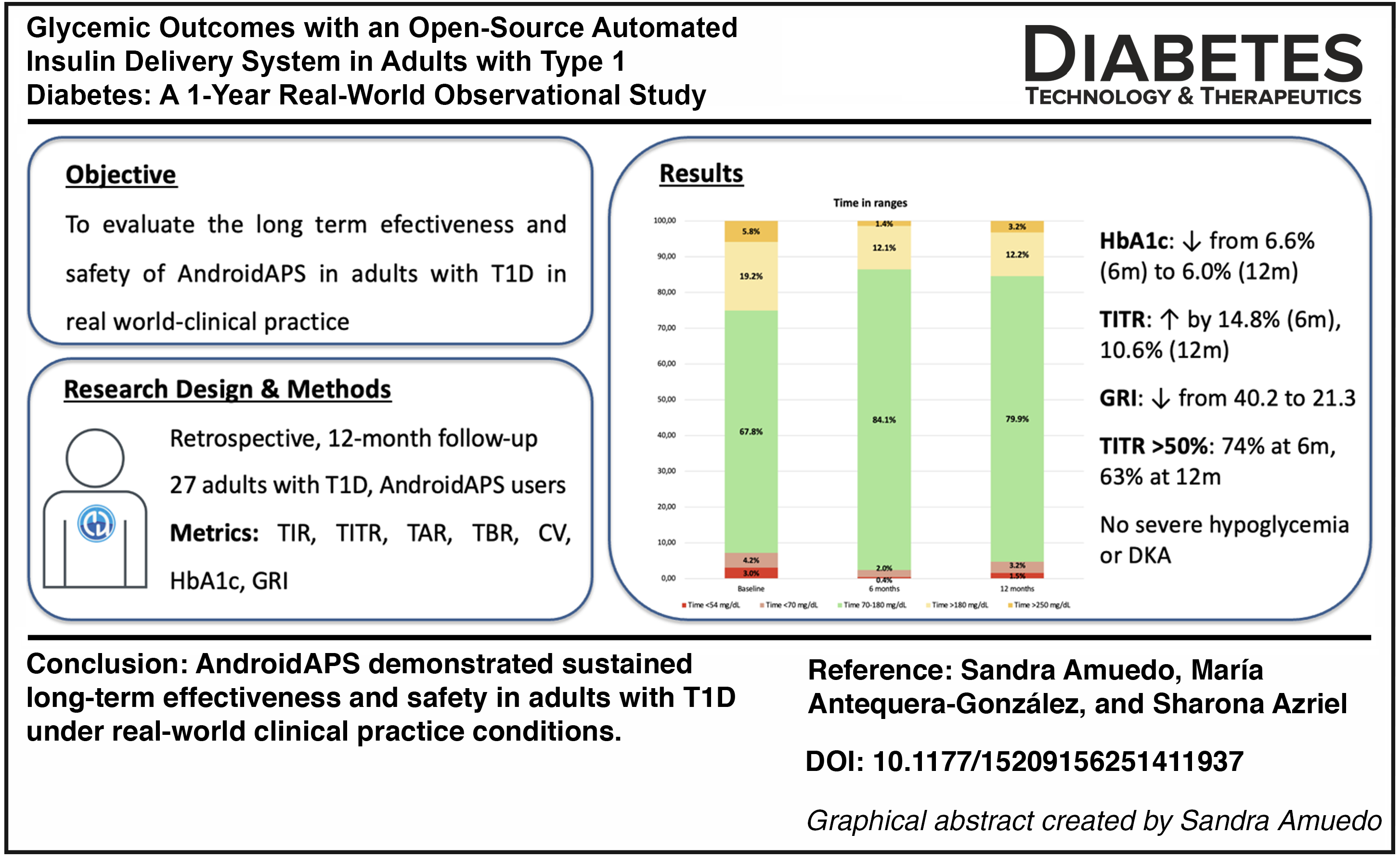
To evaluate the long-term effectiveness and safety of the AndroidAPS (AAPS) system in adults with type 1 diabetes (T1D) under real-world clinical conditions.
Methods:
This retrospective, single-center study included 27 adults with T1D (mean age 39 ± 9.6 years; 55.6% women; diabetes duration 21.5 ± 11.3 years) who initiated AAPS and were followed for 12 months. Glycemic metrics were obtained from real-time continuous glucose monitoring (rtCGM) data. Primary outcomes were changes in time in range (TIR; 70–180 mg/dL) and HbA1c. Secondary outcomes included time in tight range (TITR; 70–140 mg/dL), time below range (TBR), coefficient of variation (CV), and the glycemic risk index (GRI). Safety outcomes included severe hypoglycemia and diabetic ketoacidosis (DKA).
Results:
TIR increased from 67.8% at baseline to 84.1% at 6 months and 79.9% at 12 months (P < 0.001). HbA1c decreased from 6.6% to 6.1% and 6.0%, respectively. TITR improved by 14.8% at 6 months and 10.6% at 12 months, while GRI decreased from 40.2 to 21.3. Over 88% of participants achieved TIR > 70% and CV < 36% at both follow-ups, and up to 74% achieved TITR > 50% at 6 months, remaining at 63% at 12 months. No episodes of severe hypoglycemia or DKA were reported.
Conclusions:
AAPS demonstrated sustained long-term effectiveness and safety in adults with T1D under real-world clinical practice conditions. Glycemic outcomes were comparable to those reported with commercially available closed-loop automated insulin delivery systems, supporting AAPS as a viable and effective advanced management option for T1D.
Keywords
Introduction
Automated insulin delivery (AID) systems represent a major advancement in the management of type 1 diabetes (T1D), improving glycemic outcomes and reducing treatment burden. However, cost, accessibility, and regulatory limitations have restricted their adoption. 1
Open-source AID (OS-AID) systems—also referred to as “do-it-yourself” (DIY) artificial pancreas systems—have emerged as community-driven, customizable alternatives integrating real-time continuous glucose monitoring (rtCGM) and insulin pump therapy, and are developed and maintained by online communities of people with T1D and their families under the #WeAreNotWaiting movement. 2 The most widely used platforms are AndroidAPS, Loop, and OpenAPS. AndroidAPS (also now called AAPS), designed for Android devices, uses the OpenAPS algorithm and allows different configurations including temporary basal rate automation only (oref0) or also small microboluses called “supermicroboluses” (SMB) (oref1), based on predicted glucose trends. 3
Although OS-AID systems are not formally approved by regulatory agencies, the recent FDA authorization of Tidepool Loop, a commercial version of the Loop algorithm, illustrates growing recognition of these approaches. 4 Clinical supervision remains essential to ensure appropriate follow-up and documentation of off-label use.
Evidence from clinical trials5–11 and real-world studies2,12–18 shows that OS-AID systems can lower HbA1c, increase time in range (TIR), and reduce time below range (TBR) and above range (TAR), improving quality of life. In recent years, the evidence base supporting OS-AID has expanded considerably, with emerging trials incorporating longer follow-up and more rigorous methodological designs. Within this evolving context, real-world data such as ours offer valuable insight into the sustained effectiveness and safety of these systems in routine clinical practice.
Recently, complementary metrics such as the glycemic risk index (GRI) and time in tight range (TITR; 70–140 mg/dL) have been proposed to refine glycemic assessment.19,20 The GRI quantifies hypo and hyperglycemia, emphasizing extreme values, whereas TITR reflects time in euglycemia and may better discriminate control in well-managed patients.
In this context, this study aimed to evaluate, under real-world clinical conditions, the long-term effectiveness and safety of AAPS in adults with T1D, incorporating expanded metrics such as GRI and TITR alongside conventional glycemic parameters.
Material and Methods
Study design and population
This was an observational, single-center, retrospective study with a 12-month follow-up period conducted under routine real-world clinical practice conditions including adults with T1D previously treated with multiple daily insulin injections (MDI) or continuous subcutaneous insulin infusion (CSII), all using rtCGM. Participants initiated AAPS between November 2018 and December 2020 as part of routine follow-up at the Endocrinology and Nutrition Department of Infanta Sofía University Hospital (Madrid, Spain). The study followed the Declaration of Helsinki, and all participants provided written informed consent.
All participants used the oref1 (SMB) version of AAPS on compatible smartphones connected to an Accu-Chek Insight insulin pump. System settings, including glycemic targets and algorithm parameters, were individualized by users without a standardized protocol. However, as part of routine care in our department, the clinical team provided ongoing support to individuals using OS-AID systems. This included education during follow-up visits, review of CGM and insulin delivery data, and collaborative adjustment of configuration parameters when appropriate. Such involvement forms part of our standard clinical practice to ensure safe and effective OS-AID use.
Outcomes
Primary outcomes were changes in TIR (70–180 mg/dL) and HbA1c at 6 and 12 months after system initiation. Secondary outcomes included changes in TAR (>180 and > 250 mg/dL), TBR (<70 and < 54 mg/dL), TITR (70–140 mg/dL), mean glucose, coefficient of variation (CV), glucose management indicator (GMI), and GRI with components hypoglycemia (CHypo) and hyperglycemia (CHyper). Safety endpoints included severe hypoglycemia, diabetic ketoacidosis (DKA), and diabetes-related hospitalizations.
Data collection and analysis
Glycemic data were retrospectively extracted from electronic medical records and the Nightscout platform. For each time point (baseline, 6 and 12 months), data from the last 14 days with >75% sensor use were analyzed. HbA1c was measured using the National Glycohemoglobin Standardization Program.
The GRI was calculated using the standard formula: GRI = (3.0 × %TBR < 54 mg/dL) + (2.4 × %TBR < 70 mg/dL) + (1.6 × %TAR > 250 mg/dL) + (0.8 × %TAR > 180 mg/dL). The theoretical maximum value was 100. Based on the GRI percentile, participants were classified into five zones representing progressively worse glycemic profiles: zone A (0–20 percentile), zone B (21–40), zone C (41–60), zone D (61–80), and zone E (81–100).
Statistical analyses were performed using SPSS version 25 (IBM Corp., Armonk, NY, USA). Continuous variables were compared using paired t or Wilcoxon tests, and categorical variables with chi-square. A P value of <0.05 was considered significant.
Results
A total of 27 adults with T1D (mean age 39 ± 9.6 years; 55.6% women) were included. Mean body mass index (BMI) was 25.4 ± 3.8 kg/m2, diabetes duration 21.5 ± 11.3 years, and baseline HbA1c 6.6% ± 0.5%. Nineteen participants (70.4%) used CSII with sensor-augmented pump therapy and 8 (29.6%) MDI therapy, all with rtCGM.
Comorbidities included retinopathy (18.5%), neuropathy (7.4%), and prior severe hypoglycemia (3.7%). None had recent DKA nor diabetic nephropathy. Four participants used adjuvant agents (two SGLT2i and two GLP-1 receptor agonists).
All participants used AAPS in conjunction with an Accu-Chek Insight insulin pump. Regarding the CGM system, 18 participants (66.7%) used the Dexcom G6, and 9 (33.3%) used the FreeStyle Libre modified with NFC–Bluetooth transmission. Most participants (66.7%) had a university-level education, including four healthcare professionals and three engineers.
Glycemic outcomes
TIR (70–180 mg/dL) increased from 67.8% ± 12.8% at baseline to 84.1% ± 6.4% at 6 months and 79.9% ± 10.0% at 12 months (P < 0.001), accompanied by significant reductions in TAR > 180 mg/dL (19.2% ± 13.6% to 12.1% ± 6.0% and 12.2% ± 6.1%) and TAR > 250 mg/dL (6.5% [3–11] to 1.2% [0–3] and 2.2% [0–5]) at 6 and 12 months, respectively (P < 0.001 for all).
Mean glucose decreased from 141 ± 21.2 mg/dL to 126.2 ± 14.6 mg/dL at 6 months and 129.3 ± 11.5 mg/dL at 12 months (P < 0.001), with a parallel reduction in GMI from 6.5% ± 0.7% to 6.2% ± 0.8% and 6.1% ± 0.8%. TBR < 70 mg/dL decreased from 4.2% ± 2.6% to 2.0% ± 1.4% and 3.2% ± 1.8%, and TBR < 54 mg/dL from 2.6% [0.5–5] to 0.4% [0–4] and 0.9% [0–4] at 6 and 12 months, respectively (P < 0.001 for all) (Table 1, Fig. 1).
Glycemic Outcomes and System Use at 6 and 12 Months Following AAPS Initiation
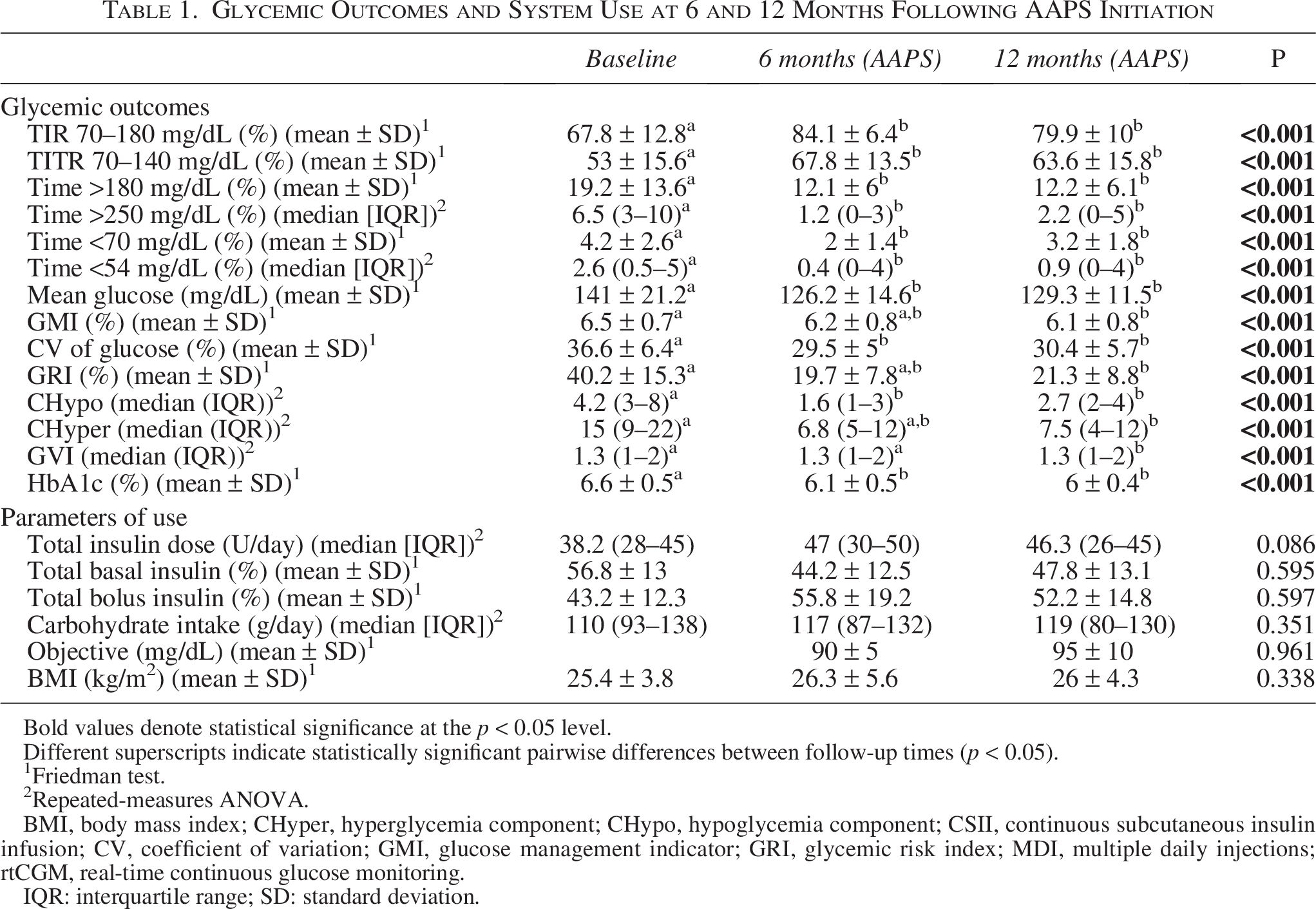
Bold values denote statistical significance at the p < 0.05 level.
Different superscripts indicate statistically significant pairwise differences between follow-up times (p < 0.05).
1Friedman test.
2Repeated-measures ANOVA.
BMI, body mass index; CHyper, hyperglycemia component; CHypo, hypoglycemia component; CSII, continuous subcutaneous insulin infusion; CV, coefficient of variation; GMI, glucose management indicator; GRI, glycemic risk index; MDI, multiple daily injections; rtCGM, real-time continuous glucose monitoring.
IQR: interquartile range; SD: standard deviation.
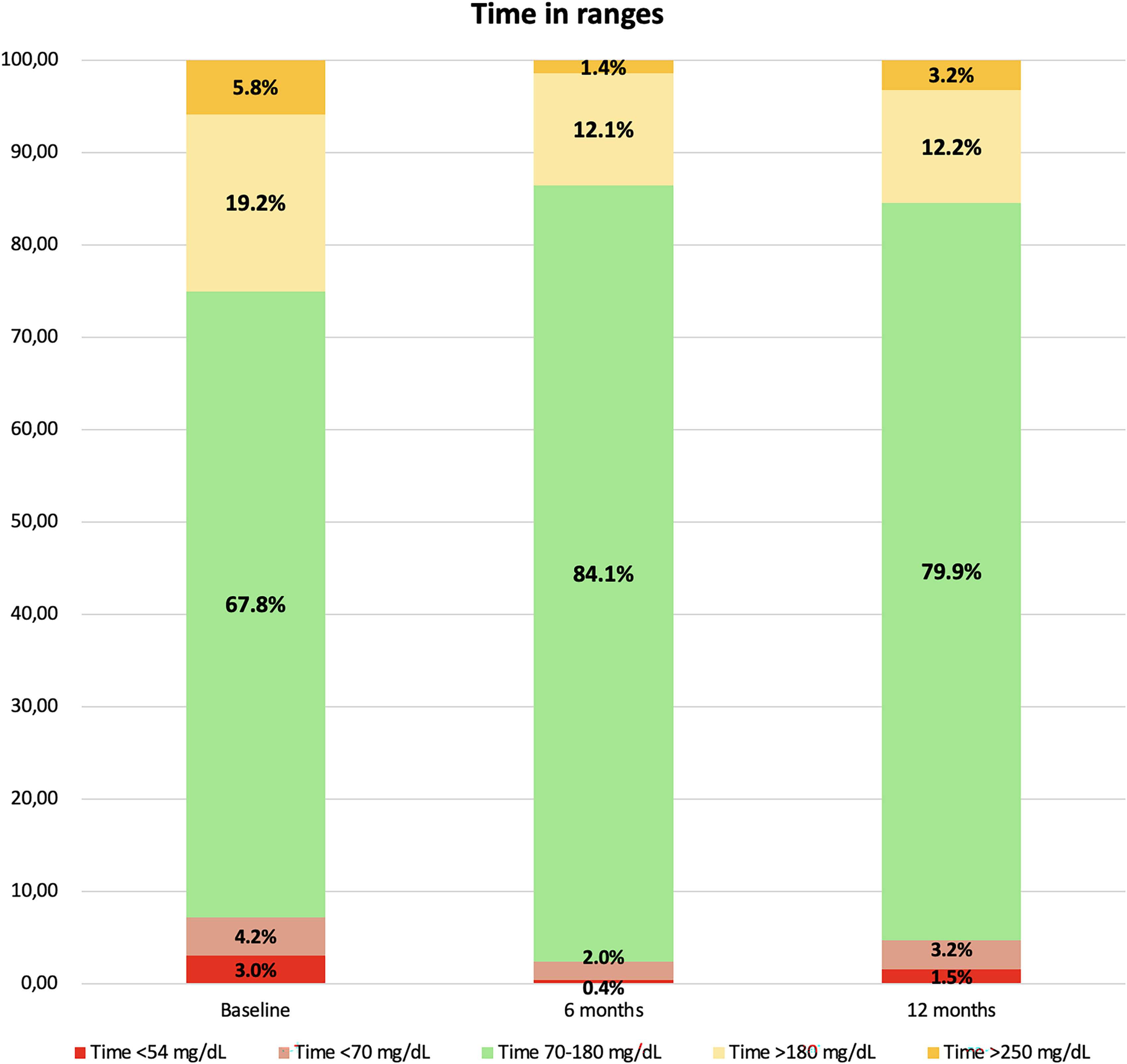
Column charts showing percentage time below range (TBR < 54 and < 70 mg/dL), time in range (TIR 70–180 mg/dL), and time above range (TAR > 180 and > 250 mg/dL) at baseline, 6 months, and 12 months of AndroidAPS (AAPS) use.
CV improved from 36.6% ± 6.4% to ≈30% (P < 0.001). HbA1c decreased by 0.5% at 6 months and 0.6% at 12 months (P < 0.001). GRI decreased from 40.2 ± 15.3 at baseline to 19.7 ± 7.8 and 21.3 ± 8.8 at 6 and 12 months, respectively (P < 0.001), with parallel reductions in CHypo (4.2 [3–8] to 1.6 [1–3] and 2.7 [2–4]) and CHyper (15 [9–22] to 6.8 [5–12] and 7.5 [4–12]) (Fig. 2).
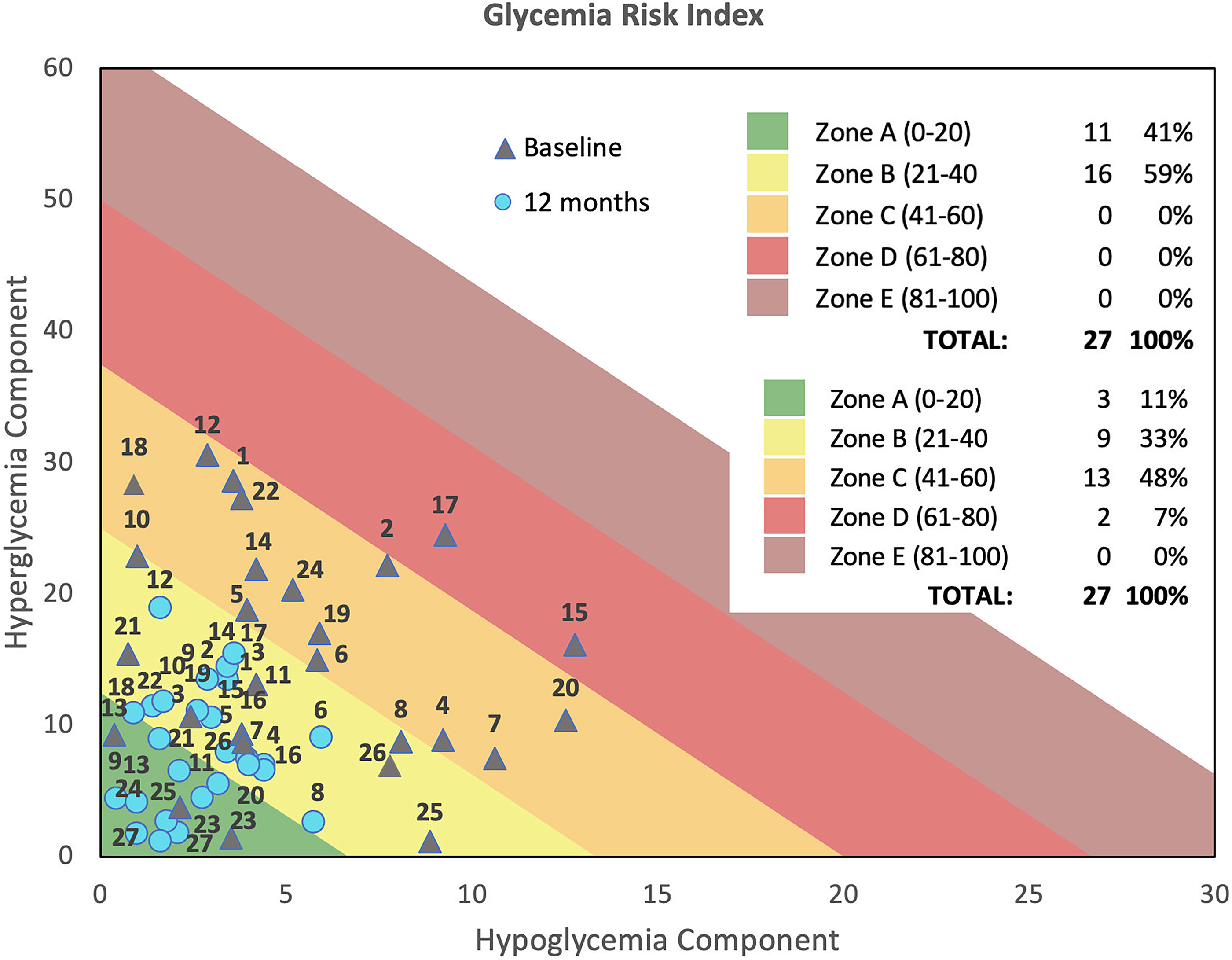
Glycemic risk index (GRI) grid displaying the hyperglycemia component (CHyper) versus the hypoglycemia component (CHypo) at baseline and after 12 months of AAPS use.
The proportion of participants achieving TIR > 70% increased from 44.4% to 100% at 6 months and 88.9% at 12 months, while those with TBR < 4% rose from 51.8% to 88.9% and 92.6%, respectively. Participants meeting both targets increased from 25.9% to 88.9% and 81.5%. TITR > 50% rose from 22.2%–74.1% and 63.0%, and CV < 36% from 48.1% to 88.9%. At baseline, 74.1% of participants had HbA1c <7.0%, increasing to 92.6% at 6 months and 96.3% at 12 months. The proportion achieving HbA1c ≤6.5% rose from 44.4% to 85.2% at 6 months and 81.5% at 12 months.
GRI showed strong negative correlations with TIR (r = −0.92) and TITR (r = −0.82) and positive correlations with HbA1c (r = 0.82), GMI (r = 0.77), TAR > 180 mg/dL (r = 0.89), TAR > 250 mg/dL (r = 0.85), and mean glucose (r = 0.69). Moderate positive correlations were also found with TBR < 70 mg/dL (r = 0.39) and TBR < 54 mg/dL (r = 0.47) (P < 0.001 for all). No significant changes were observed in BMI, total daily insulin dose, basal/bolus ratio, or carbohydrate intake during follow-up.
Safety
No severe hypoglycemia, DKA, or diabetes-related hospitalizations occurred during follow-up, and all participants continued using AAPS. Reported satisfaction was high, although not formally assessed.
Discussion
Despite major advances with AID systems, up to 28% of users still fail to meet recommended glycemic targets, highlighting persistent unmet clinical needs. 21 In this context, open-source AID (OS-AID) systems, developed and maintained by individuals with T1D and their families, have emerged as accessible and customizable alternatives outside conventional regulatory frameworks.
Real-world evidence has shown that OS-AID systems improve glycemic outcomes, safety, and quality of life in both pediatric13,22,23 and adult2,8,12,14–17 populations, although data on their long-term sustainability remain limited.
This study demonstrates sustained real-world use of AAPS over 12 months in adults with T1D, with clinically relevant improvements in TIR (+16.2% at 6 months and +12.0% at 12 months), HbA1c (−0.6%), TITR, and GRI, without increases in TBR or serious adverse events.
These findings are consistent with previous short-term studies using AAPS8,15 and other OS-AID systems such as Loop, 12 as well as longer-term evaluations by Patel 16 and Liarakos. 17 Wu et al. 15 reported a 9.3% increase in TIR (final 84.3%) and a 0.8% reduction in HbA1c after 3 months, while Gawrecki et al. 8 observed an 11.3% increase in TIR (final 79.3%) and a 0.5% decrease in HbA1c. In a multicenter study of 558 Loop users, Lum et al. 12 found a 6.6% rise in TIR (final 73%) and a 0.3% HbA1c reduction, without increased TBR.
To date, only two studies have evaluated OS-AID systems beyond 1 year of use: Patel et al. 16 (1.4 years; TIR 73%, TBR < 70 mg/dL 2.4%, HbA1c −0.9%) and Liarakos et al. 17 (1.7 years; HbA1c −0.8%, TIR 78.6%, TBR 3.2%).
Our findings are also comparable to those of the CREATE clinical trial, in which AAPS was used for 24 weeks in 22 adults with T1D, achieving a TIR of 74.5%, TBR of 1.6%, and an HbA1c reduction of −0.5%, with sustained improvements during the extension phase.9,10
Furthermore, comparative studies suggest that OS-AID systems can achieve glycemic outcomes equivalent to, or even superior to, those of commercial systems. 24 The CODIAC study showed similar TIR values between AAPS (84.2%) and Control-IQ (85.7%) after 3 months of use. 11 Likewise, Wu et al. reported higher TIR with OS-AID (78.3%) compared with commercial systems (71.2%) in real-world settings over 12 weeks. 25
In our study, 88.9% of participants achieved TIR > 70% and TBR < 70 mg/dL < 4% at 6 months, and 81.5% maintained this at 12 months, exceeding the results from CREATE 9 (64%) and Liarakos et al. 17 (45.3%). These differences are more likely explained by the characteristics of real-world use in our cohort, where users were able to adjust settings freely and without protocol-imposed limitations, together with behavioral factors such as lower carbohydrate intake. Collectively, these elements may have contributed to achieving higher TIR values under routine clinical conditions. Higher proportions also reached HbA1c <7% (92.6% and 96.3% at 6 and 12 months) and ≤6.5% (85.2% and 81.5%), compared with Lum et al. 12 (75%) and Liarakos et al. (75.7% and 51.4%).
Unlike previous studies by Patel and Liarakos,16,17 our analysis included additional metrics such as CV, TITR, and GRI. Glycemic stability improved notably, with 88.9% maintaining CV < 36% at 12 months. To our knowledge, this is the first study to assess the long-term effects of AAPS on TITR (70–140 mg/dL) and GRI.
Although no consensus exists on optimal TITR thresholds, values >50% are considered clinically relevant. In our cohort, 67% (n = 18) and 78% (n = 21) achieved TITR > 50% at 6 and 12 months, supporting its value as a complementary metric in AID users. TITR has emerged as a sensitive metric of euglycemia, complementing traditional indicators such as TIR, HbA1c, and CV. In our cohort, TITR increased by 14.8% at 6 months and 10.6% at 12 months (mean 67.8% and 63.6%), while GRI decreased from 40.2 to 21.3. These results exceed those of commercial systems, with TITR increases of only 5% and GRI above 28% in Control-IQ, and a +11.6% TITR (final 48.8%) with MiniMed™ 780G. 26
Despite good baseline control (HbA1c 6.6%), AAPS use further improved TIR, TITR, HbA1c, and CV, without increases in TBR or adverse events. Given the baseline CV (36.6%) above the recommended <36%, its reduction is clinically relevant and may lower long-term complication risk. 27 Although the margin for improvement was narrower in this well-controlled cohort, individuals with higher baseline HbA1c showed greater reductions, while those already within target still achieved relevant gains in complementary metrics such as glycemic stability. These findings suggest that AAPS may benefit both users with suboptimal control and those already meeting recommended goals.
Most users had higher education but no advanced technical expertise, indicating that AAPS can be adopted by individuals with diverse backgrounds. While education may ease initial adoption, sustained use appeared more related to user motivation and engagement than to technical proficiency. These aspects should be considered when interpreting the generalizability of our findings.
Strengths include the 12-month follow-up, exclusive evaluation of AAPS in adults, availability of rtCGM data before initiation, and use of emerging metrics such as TITR and GRI. Importantly, unlike most observational studies, all data were extracted from objective medical records during routine care, enhancing the robustness of the findings. Limitations include the retrospective design, lack of a control group, and possible self-selection bias. No structured patient-reported outcomes were collected. Although users frequently expressed high satisfaction during routine visits, validated measures of quality of life, treatment burden, or user experience were not obtained, preventing a formal assessment of the broader impact of AAPS. Although improvements were sustained at 12 months, small declines in TIR and TITR and a rise in TBR underscore the need for longer-term evaluation. Finally, the individualized configuration of AAPS parameters, despite routine clinical support, was not standardized and reflects real-world use, but may limit reproducibility and generalizability to other settings.
Conclusions
This study provides evidence supporting the long-term effectiveness and safety of the AAPS system in adults with T1D under real-world conditions. Sustained improvements in TIR, TITR, GRI, and HbA1c were observed without increased hypoglycemia, demonstrating AAPS as a viable and effective option for advanced management of T1D.
Authors’ Contributions
S.Amuedo, M.A.-G., and S.Azriel wrote the initial research proposal, reviewed the proposal and the study results, and wrote the article. S.Amuedo., M.A.-G, and S.Azriel reviewed and edited the research proposal and article, and contributed to the discussion. All authors read and approved the final version of this article.
Footnotes
Funding Information
No funding was received for this article.
Disclosure Statement
The authors declare that they have no known competing financial interests that could have appeared to influence the work reported in this article.