
Abstract
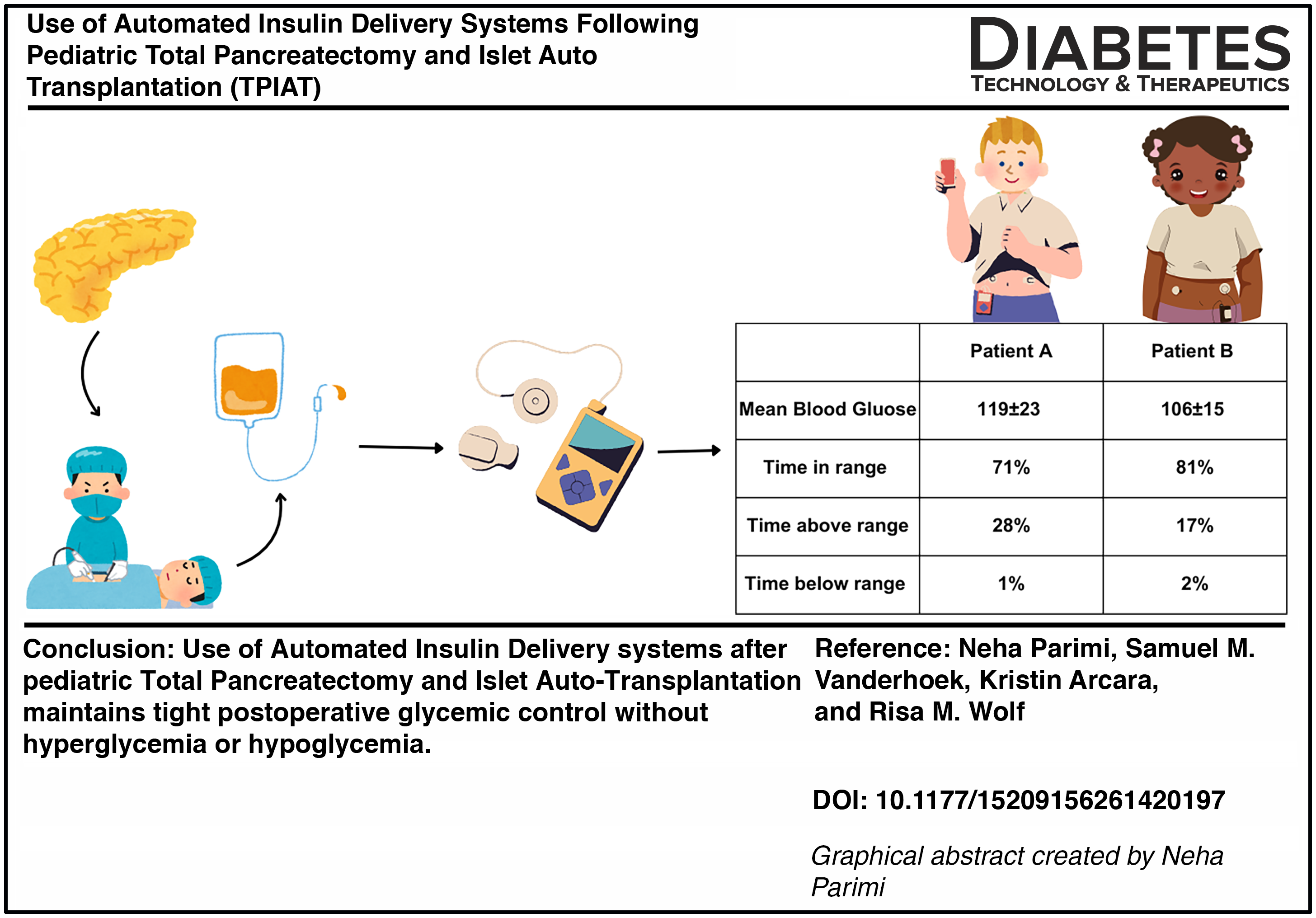
Total pancreatectomy with islet auto-transplantation (TPIAT) treats intractable pain in patients with pancreatitis. Automated insulin delivery (AID) systems improve glycemic control in patients with diabetes, but their role in post-TPIAT glycemic management needs exploration. This case series included two patients who initiated AID after TPIAT at the Johns Hopkins Children’s Center from August 2024 to June 2025. Following TPIAT, a 10-year-old male using AID met the glycemic target of 80–130 mg/dL with a mean blood glucose of 119 ± 23 mg/dL, time in range of 71%, time above range of 28%, and time below range of 1%. Similarly, in a 16-year-old female using AID after TPIAT mean blood glucose was 106 ± 15 mg/dL, time in range was 81%, time above range was 17%, and time below range was 2%. AID use after TPIAT can maintain tight glycemic control without hypoglycemia or hyperglycemia and may be considered for use in post-TPIAT glycemic management.
Keywords
Introduction
Total pancreatectomy and islet auto transplantation (TPIAT) is a surgical procedure to treat intractable pain in patients with chronic or acute recurrent pancreatitis. 1 While total pancreatectomy eliminates the source of pain and improves quality of life, it also removes insulin-producing islet cells of the pancreas. 2 To preserve endogenous insulin secretion, total pancreatectomy is immediately followed by islet auto-transplantation, which is the isolation and intraportal reinfusion of islet cells. The reinfused islet cells subsequently become functional and produce endogenous insulin. Studies report that approximately 29% of youth remain insulin independent one-year post-TPIAT. 3
Factors associated with insulin independence post-TPIAT include young age, high reinfused islet cell mass, and tight postoperative glycemic control.3,4 A tight glycemic target of 80–130 mg/dL is recommended to ensure maximal survival of reinfused islet cells and improved outcomes post-TPIAT.5,6 To maintain recommended glycemic target and provide adequate rest for reinfused islet cells, exogenous insulin is administered after TPIAT. 4 Exogenous insulin is administered as an infusion immediately post-TPIAT and subsequently as subcutaneous insulin, delivered as multiple daily injections (MDI) or via insulin pumps. 7
Diabetes technology use, including insulin pumps and continuous glucose monitors (CGMs), has increased over the past decade. 8 These technologies are known to improve glycemic control by increasing time-in-range (TIR), lowering HbA1c, and reducing episodes of diabetic ketoacidosis and hypoglycemia.9,10 Owing to these benefits, CGM and insulin pump use has expanded beyond routine diabetes care to post-TPIAT glycemic management.11,12
Insulin pump use post-TPIAT is well-described, yet few have reported on use of automated insulin delivery (AID) systems post-TPIAT, particularly in the pediatric population. AID systems integrate continuous glucose monitoring (CGM) data and automate insulin delivery from insulin pumps, mimicking physiological insulin release. These systems allow for precise dose delivery and are more effective in maintaining glycemic control when compared with insulin pumps and MDI.13,14 Given the benefits of AID systems and paucity of literature on their use post-TPIAT in the pediatric population, we sought to describe our experience of using AID systems in pediatric patients after TPIAT.
Materials and Methods
Study design and participants
This case-series included two patients under 21 years old, who underwent TPIAT at the Johns Hopkins Children’s Center between August 2024 and June 2025 and were transitioned from insulin infusion to AID system. This study was approved by the Johns Hopkins Institutional Review Board in accordance with the Declaration of Helsinki with a waiver of consent.
Post-TPIAT procedures
A standard protocol was followed for perioperative glycemic management. 4 Intraoperatively, upon removal of pancreas, patients were initiated on insulin infusion of 0.025–0.05 units/kg/h and dextrose-containing fluids with a target glucose range of 100–120 mg/dL. As of August 2024, at our pediatric center, patients were postoperatively transitioned from insulin infusion to AID system for subcutaneous insulin administration. In preparation for AID initiation, patients were provided Dexcom G7 CGMs and insulin pump training before TPIAT. All patients were initiated on either Tandem Mobi or Tandem T:Slim X2 in sleep activity mode, as it allows for tight glycemic target of 112.5–120 mg/dL. Patients were initiated on a standardized dose of 0.5 units/kg/day of subcutaneous insulin in the pump, and insulin doses were titrated to glycemic target of 80–130 mg/dL. Once patients resumed oral intake of carbohydrates, they were advised to administer bolus insulin doses for carbohydrate coverage and also give correction doses for any postprandial blood sugars above 130 mg/dL. These correction doses were advised to be given every 90 min to avoid insulin stacking and subsequent hypoglycemia.
Data collection
Demographics and medical history were collected from electronic medical records (EMR). Details of mean blood glucose (MBG), insulin doses and boluses were collected from Tandem Source. TIR, time-above-range (TAR), time-below-range (TBR), and glucose variability (CV) were collected from Dexcom Clarity. Patients were considered in glycemic target range when blood sugars were between 80 and 130 mg/dL. 4 Blood sugars above 130 mg/dL or below 80 mg/dL were considered hyperglycemia and hypoglycemia, respectively. Data collected was from the first day of AID use through hospital discharge and up to 2 weeks after AID initiation.
Results
Patient A is a 10-year-old male, (46.3 kg with a BMI of 24.85 kg/m2), with a 2-year history of recurrent pain and frequent hospitalizations due to acute recurrent pancreatitis with chymotrypsin C (CTRC) and cationic trypsinogen gene mutations. He underwent TPIAT with spleen preservation (islet cell count was not recorded in EMR). He was initiated on an intravenous insulin infusion intraoperatively. The insulin infusion continued through postoperative day-2 (POD-2), and MBG was 100.5 mg/dL (range 88–122 mg/dL). On POD-3, he transitioned from insulin infusion to Tandem Mobi system in sleep activity mode. On the first day of Tandem Mobi use, patient A was on sugar-free liquids, and the day after, he transitioned to liquid diet containing sugars (Fig. 1). On these 2 days (POD-3 and POD-4), AID delivered an average daily dose of 5.23 units of basal insulin and maintained MBG of 98 ± 11 mg/dL. Patient A’s TIR was 97% with 3% lows. On POD-5, patient A’s diet advanced to solid foods with carbohydrates, and patient administered correction boluses. For the following 3 days until discharge (POD-5 to POD-8), the patient’s MBG was 124 ± 26 mg/dL, with seven average daily boluses, 12.27 units of average daily insulin, and 97 g of average daily carbohydrates. During this time, patients’ TIR was 63% with 37% highs and CV of 20.7%. Notably, on POD-6, patient’s glucose was elevated (maximum 199 mg/dL) due to delayed pump change (Fig. 1). Following site change, glucose levels returned to normal. Overall, in the 2 weeks after AID initiation post-TPIAT, patient’s MBG was 119 ± 23 mg/dL with an average daily insulin dose of 16.68 units and seven daily boluses. In addition, Patient A’s TIR was 71%, TAR was 28%, TBR was 1%, and CV was 19.7%.

Glycemic control with AID use after TPIAT. Elevated blood sugar due to delayed pump change.
Patient B is a 16-year-old female, (76.4 kg with a BMI of 31.33 kg/m2) with chronic fibrosing pancreatitis predisposed by mutations in CTRC gene, requiring seven hospital admissions since diagnosis at 34 months of age. She underwent TPIAT with splenectomy and received 2350 IEQ/kg of islet cells intraoperatively. Postoperatively, she was initiated on intravenous insulin infusion, which continued until POD-3. Her MBG while on insulin infusion was 107.3 mg/dL (range 93–119 mg/dL). On POD-4, she initiated a Tandem T:Slim X2 in sleep activity mode. She was on a liquid diet (containing sugar). Her MBG on the first day of AID system use (POD-4) was 116 ± 12 mg/dL, average daily insulin was 6.8 units, and she administered two boluses correcting for carbohydrates. Her TIR was 91% with 9% TAR and 11.1% CV. On POD-5 she transitioned to a solid diet with carbohydrates. From AID initiation through discharge (POD-4 to POD-11), her MBG was 106 ± 15 mg/dL, average daily insulin was 11.11 units, and she administered an average of 3 boluses/day with average daily carbohydrate intake of 99 g. In addition, her TIR was 91%, TAR was 5%, TBR was 4%, and CV was 14.4%. Overall, in the 2 weeks from pump initiation, patient B’s MBG was 106 ± 15 mg/dL, and the average daily insulin dose was 6.95 units with two average daily boluses. Her TIR was 81%, TAR was 17%, TBR was 2%, and CV was 15.4%.
Prior to transplant, there was no evidence of dysglycemia in either patient. Postoperatively, both patients recovered without any complications, and neither received hydroxyurea as part of postoperative care.
Discussion
This case series describes the experience of using AID systems, specifically Tandem Mobi and Tandem T:Slim X2, in two pediatric patients who underwent TPIAT. Both patients remained within recommended post-TPIAT glycemic target range with AID use. To our knowledge, this is one of the first studies highlighting the use of AID systems in pediatric patients after TPIAT and the maintenance of postoperative tight glycemic control.
Studies report the importance of maintaining postoperative euglycemia for improved patient recovery. 15 Stress of surgery and anesthesia increases counter-regulatory hormones, leading to insulin resistance and hyperglycemia. 16 Tight glycemic control is especially important in the context of TPIAT, given that survival of transplanted islet cells depends on postoperative euglycemia. 4 A study of adults using Medtronic pumps after TPIAT demonstrated improved glycemic control with use of this AID system. 17 Similarly, our study found that MBG for both patients who used AID after TPIAT remained within the recommended post-TPIAT tight glycemic range of 80–130 mg/dL, without hyperglycemia or hypoglycemia. 4 They also achieved the goals of TIR (>70%), TAR (<25%), and TBR (<4%). 18 Patient A’s TIR was slightly lower at 71%, likely related to high blood sugars on POD-6 from delayed pump change. However, his TIR still remained above target. Overall, these findings indicate effectiveness and safety of AID use after TPIAT in pediatric patients.
Patients at our institution were initiated on Tandem Mobi or Tandem T:Slim X2 pump. 17 Tandem pumps are unique, as they offer a specialized sleep activity mode in which AID algorithm adjusts basal insulin delivery based on a treatment range of 112.5 − 120 mg/dL, therefore offering tighter glycemic control. 19 Both patients in our study used pumps in sleep activity mode and effectively remained within glycemic target range. Advances in technology have led to the development of newer AID systems that have lower glycemic thresholds (as low as 87 mg/dL). 20 Therefore, future evaluation will be important to assess effectiveness of these promising systems.
Insulin initiated with AID was based on the standard dosing protocol. However, insulin needs changed with diet advancement post-TPIAT. As patients progressed to consuming solid foods, insulin needs gradually increased, and patients bolused to correct for carbohydrate intake. Patient B’s insulin requirements were lower compared with Patient A’s, and she was able to maintain euglycemic status with a smaller number of boluses. Therefore, insulin dose titration should be individualized with AID use after TPIAT.
Our series is among the first to report on the experience of using AID systems after TPIAT in the pediatric population. However, there are limitations. This study reports the experience of two patients who underwent TPIAT at a single center, and our findings may not be generalizable to all populations. Future studies with larger sample sizes, longer follow-ups, involving multiple sites, and more robust study designs are required to provide additional insight into safety, effectiveness, and long-term outcomes of AIDs after TPIAT.
Conclusions
In conclusion, our study demonstrated that AID use after TPIAT can be effective for postoperative glycemic management in pediatric patients. With more centers now performing TPIAT, our study findings could inform hospital policies to adopt AIDs for post-TPIAT glycemic management.
Authors’ Contributions
R.M.W. and K.A. conceived of the study. N.P. collected data and created figures. N.P. and R.M.W. wrote the article. All authors made critical contributions to the article. All authors edited, reviewed and approved the article.
Footnotes
Author Disclosure Statement
R.M.W. reports receiving research support from Lilly Diabetes, Novo Nordisk, and Sanofi outside the submitted work. R.M.W. is a consultant for Sanofi. N.P., S.V., and K.A. have no conflicts of interest.
Funding Information
No funding was received for this study.
Data Availability
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.