
Abstract
Aims:
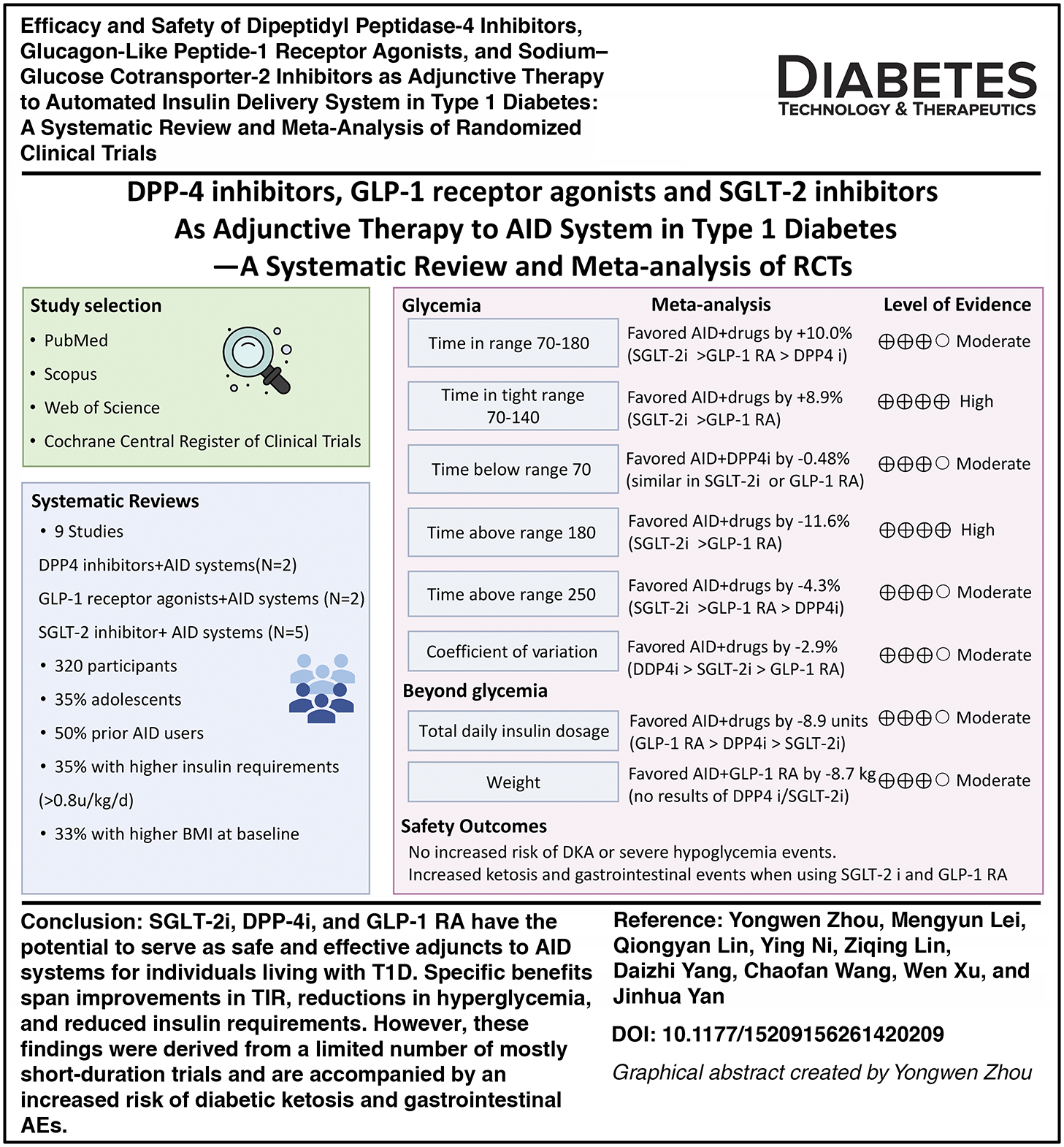
The efficacy of adding various noninsulin hypoglycemic drugs to automated insulin delivery (AID) systems in patients with type 1 diabetes (T1D) was investigated in randomized controlled trials (RCTs), yet no meta-analysis has been conducted. This study aimed to systematically analyze the existing evidence.
Methods:
Four datasets were searched up to August 31, 2025. Inclusion criteria were as follows: T1D populations of any age; comparing any type of noninsulin hypoglycemic drug added to AID systems or not; and reporting primary outcomes (time in range [TIR] = 70–180 mg/dL, 3.9–10.0 mmol/L). Results were pooled using a random-effect meta-analysis. Risk of bias was assessed using the Cochrane RoB2 tool. Quality of evidence was assessed by the Grading of Recommendations Assessment, Development, and Evaluation approach (Registered number: CRD420251107996).
Results:
Nine RCTs met the inclusion criteria, investigating sodium–glucose cotransporter-2 inhibitor (SGLT-2i) (N = 5), glucagon-like peptide-1 receptor agonist (GLP-1 RA) (N = 2), and dipeptidyl peptidase-4 inhibitor (DPP-4i) (N = 2), respectively. Overall, these drugs with AID systems improved TIR by +10.0% (7.4%–12.6%) and time in tight range (TITR; 70–140 mg/dL, 3.9–7.8 mmol/L) by +8.9% (6.8%–11.0%) with I2 of 60.4% and 15.4% (P < 0.001). These improvements were primarily driven by reductions in time above range (TAR) >250 mg/dL (>13.9 mmol/L; −4.3 [−5.8 to −2.8] %), TAR >180 mg/dL (>10.0 mmol/L; −11.6 [−14.7 to −8.5] %), and coefficient of variation (−2.9 [−4.5 to −1.4] %) without increased hypoglycemia. Daily insulin dose decreased by 8.9 units. Among these, SGLT-2i conferred the greatest TIR improvement (+12.5%), followed by GLP-1 RA (+7.1%) and DPP-4i (+6.4%). No significant differences were found in severe hypoglycemia (SH) and diabetic ketoacidosis (DKA).
Conclusions:
SGLT-2i, DPP-4i, and GLP-1 RA may serve as effective and safe adjuncts for T1D individuals using AID systems, offering improvements in TIR, reductions in hyperglycemia, and reduced insulin requirements without evidence of increasing DKA and SH.
Introduction
Over the past decade, automated insulin delivery (AID) systems integrating continuous glucose monitoring, insulin pumps, and algorithm-based insulin dosing strategy have transformed type 1 diabetes (T1D) management. These systems consistently improve time in range (TIR; 3.9–10.0 mmol/L, 70–180 mg/dL) and lower glycated hemoglobin A1c (HbA1c) without increasing hypoglycemia, outperforming traditional insulin therapies. 1 Nevertheless, even with AID systems, many individuals fail to achieve optimal glycemic targets, particularly for postprandial control. Moreover, long-term insulin therapy may contribute to progressive increases in insulin requirement and weight gain. 2 These persistent deficits underscore an urgent need for improved treatment strategies and have prompted increasing interest in adjunctive strategies that target complementary metabolic pathways.
Noninsulin pharmacologic options, including dipeptidyl peptidase-4 inhibitor (DPP-4i), sodium–glucose cotransporter-2 inhibitor (SGLT-2i), and glucagon-like peptide-1 receptor agonist (GLP-1 RA), have been recently reported to offer additional benefits in T1D by improving insulin sensitivity, reducing renal glucose reabsorption, and attenuating postprandial glucose excursions.3,4 More recently, as AID systems are increasingly adopted in clinical practice, several randomized controlled trials (RCTs) have been conducted to investigate the combined use of noninsulin hypoglycemic drugs with AID systems, recognizing the potential for synergistic effects.5–13 These trials, however, differ in study design, intervention types, and reported outcomes, leaving uncertainty regarding the consistency of benefit and the overall safety profile.
Given this emerging but fragmented evidence base, we conducted a systematic review and meta-analysis of RCTs to evaluate the efficacy and safety of the currently reported noninsulin pharmacologic options adjunctively used with AID systems in individuals with T1D, focusing on glycemic outcomes, insulin dose requirements, body weight, and adverse events (AEs).
Methods
Protocol and registration
This systematic review and meta-analysis followed the Cochrane Handbook of Systematic Reviews and was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guideline.14,15 It was registered prospectively at PROSPERO (Registration ID: CRD420251107996).
Data sources and literature searches
The search of databases including PubMed, Web of Science, Scopus, and Cochrane Central Register of Clinical Trials was conducted up to August 31, 2025. The search primarily utilized Medical Subject Headings (MeSH) and free-text terms, including (“type 1 diabetes” OR “diabetes mellitus, type 1” [Mesh]) and (“automated insulin delivery” OR “artificial pancreas” OR “closed loop system” or “closed-loop system”) and the variations. The search used specific noninsulin hypoglycemic drugs as free-text terms, including metformin, alpha-glucosidase inhibitors, thiazolidinediones, DPP-4i, SGLT-2i, GLP-1 RA, and the respective product names. A full list of search terms is found in Supplementary Table S1. Reference lists of included articles were also reviewed to identify any potential articles.
Eligibility and study selection
RCTs were included if they met the following PICO schema: Population (P): Nonpregnant T1D individuals of any age and sex who were using any AID system. Intervention (I) and Comparison (C): Comparison of noninsulin hypoglycemic drugs versus placebo/without drugs as adjunctive therapy to AID systems. Outcome (O): Postintervention glycemic measurement. The exclusion criteria were as follows 1 : Studies involving combination therapy with two or more drugs, 2 retrospective studies, post hoc studies, 3 studies without full-text resources, 4 and studies not published in English.
Literature search results from electronic databases and additional sources were imported into EndNote 20.4 (Clarivate Analytics, Philadelphia, PA), and duplicates were automatically removed. Two authors (Y.Z. and Q.L.) independently screened the titles and abstracts. Full-text articles of potentially relevant studies were then assessed for eligibility. The authors were contacted when eligibility could not be determined due to missing or unclear information. Y.Z. and Q.L. validated the final list of included studies. Disagreements were resolved through discussion or consultation with a third reviewer (J.Y.).
Outcomes of interest
The primary outcome was TIR between T1D individuals using noninsulin hypoglycemic drugs compared with placebo/without drugs as adjunctive therapy to AID systems. Secondary outcomes were time in tight range (TITR; 3.9–7.8 mmol/L, 70–140 mg/dL), time below range (TBR) <3.9 mmol/L (<70 mg/dL; TBR70) and <3.0 mmol/L (<54 mg/dL; TBR54), time above range (TAR) >10.0 mmol/L (>180 mg/dL; TAR180) and >13.9 mmol/L (>250 mg/dL; TAR250), coefficient of variance (CV), mean blood glucose (MBG) and HbA1c, total daily dosage (TDD, units/day), body mass index (BMI), and weight. Safety outcomes included risk of severe hypoglycemia (SH), serious AEs (SAEs), and other AEs, including gastrointestinal side effects, infection, ketoacidosis, and ketosis.
Data extraction
Data were extracted into a predesigned spreadsheet, including information about authors, country, publication year, trial design and duration, number of participants and demographic characteristics, drug types with dosage and titration plan, primary and secondary outcomes, P values, and/or confidence intervals (CIs).
The effect size was the between-group difference in mean changes from baseline. For each RCT, the mean change from baseline between the two groups and its CI were extracted. If the effect size was not available, changes from baseline in each arm were extracted for calculation. If changes from baseline were not available, the postintervention means or medians (if means are not available) were extracted. The 95% CI of effect sizes and the respective P values were collected if available. P value and the SD of differences were used to calculate CI via methods outlined in the Cochrane Handbook.
Risk of bias and Grading of Recommendations Assessment, Development, and Evaluation assessment
Risk of bias for study estimates was assessed using the Cochrane Rob 2 tool. 16 Five domains were used to find potential bias. Risk of bias for each domain and the overall risk of bias were designated as “low,” “some concerns,” or “high” by two independent reviewers (Y.W.Z. and M.Y.L.). Discrepancies between reviewers were resolved by a third reviewer (J.H.Y.).
Certainty of the evidence was determined using the GRADE (Grading of Recommendations Assessment, Development, and Evaluation) framework. 17 The evaluated domains included study design, risk of bias, inconsistency, indirectness, and imprecision. Details on assessment criteria for each domain are provided in Supplementary Table S2.
Data synthesis and meta-analysis
Restricted maximum likelihood random-effects meta-analyses were undertaken for each outcome. These were undertaken using “meta” in R Statistical Software (v4.2.2; R Core Team 2021). Effect sizes, 95% CI, and P values were calculated for each subgroup and for all studies together. For metrics not reported in the same units, standardized mean differences (MDs) were calculated. Forest plots were generated to display results. Heterogeneity statistics were also calculated using tau2 and I2 statistics. The difference in medians was used as an approximation for the MD; however, when the data were very skewed, this might not be an accurate approximation.
Subgroup analyses
Subgroup analyses were restricted to age (adults [≥18 years] or adolescents [<18 years]), study design (open-label or double-blinded; crossover or parallel), intervention duration (≤4 weeks or >4 weeks), with/without AID experience before enrollment, and with/without placebo as the comparator. To further explore sources of heterogeneity, meta-regression models were calculated for these characteristics.
Results
Search results
A total of 135 records were initially identified (Supplementary Fig. S1). After removing duplicates, 60 records were reviewed for abstracts and titles; 9 records were included after excluding conference abstracts, registered records, and protocols.5–13 Two records were excluded as one contained registered information of RCT investigating metformin with AID systems, yet the results were not published 18 ; the other study that evaluated the DPP-4i used with AID did not report TIR. 19 Hence, the included nine studies into meta-analysis ultimately evaluated DPP-4i (N = 2), GLP-1 RA (N = 2), and SGLT-2i (N = 5) adjunctively used with AID systems.
Study characteristics
Details of the included RCTs and participants are summarized in Table 1. Among the included studies, six used a crossover design,7,9–13 and three were double-blinded with placebo as the comparator.5,6,8 Seven studies had an intervention duration of ≥4 weeks (range: 4–32 weeks).5–8,10–12 Half of the studies used TIR as the primary outcome (one focused on daytime TIR)7,9,11–13; the other primary outcomes included a composite endpoint of TIR >70%, TBR70 <4.0%, and >5% weight reduction, 8 change in urinary albumin-to-creatinine ratio, 5 postprandial glucose at 3 h after meals, 6 and MBG. 10
Study Information and Participant Characteristics
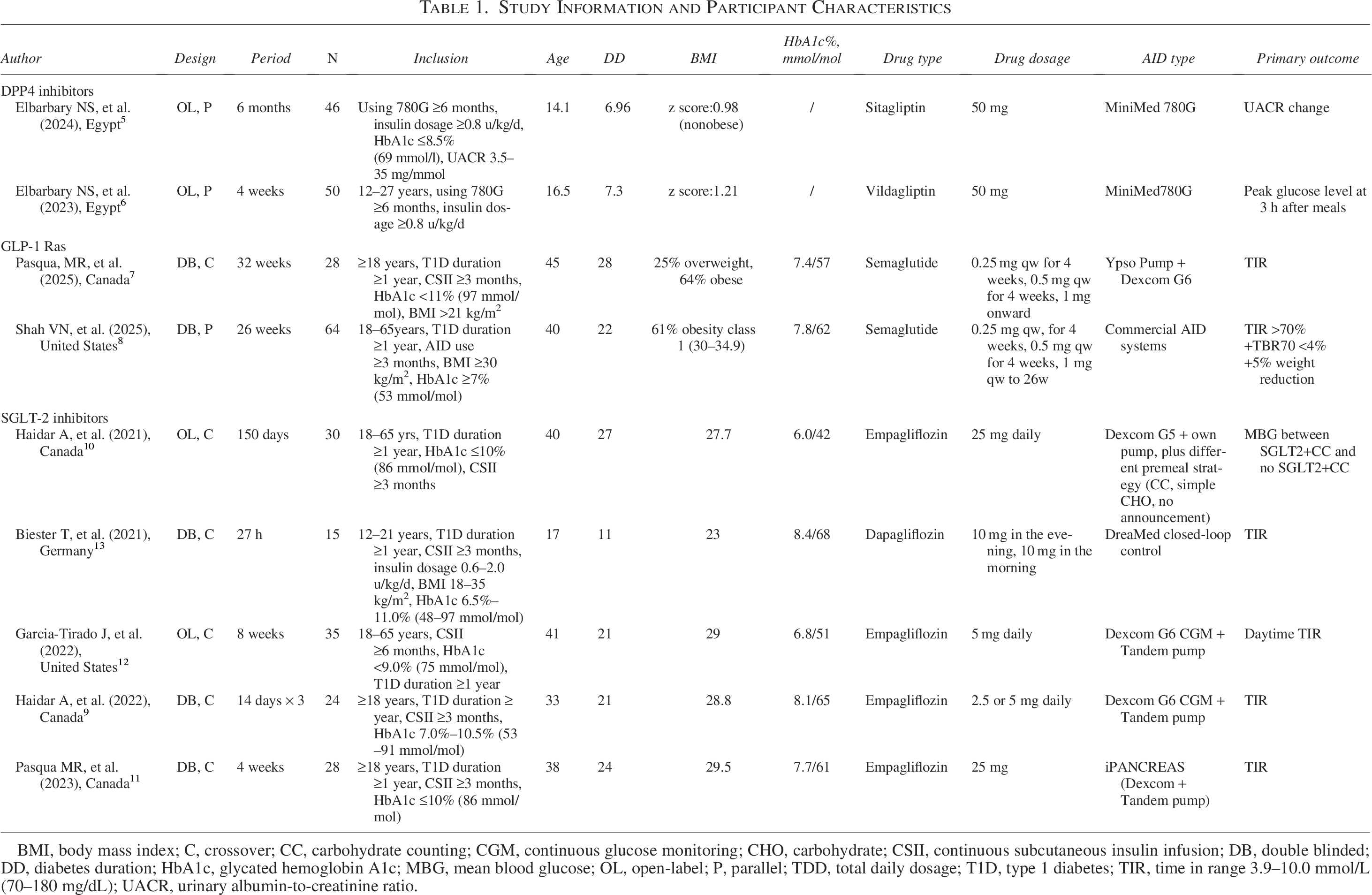
BMI, body mass index; C, crossover; CC, carbohydrate counting; CGM, continuous glucose monitoring; CHO, carbohydrate; CSII, continuous subcutaneous insulin infusion; DB, double blinded; DD, diabetes duration; HbA1c, glycated hemoglobin A1c; MBG, mean blood glucose; OL, open-label; P, parallel; TDD, total daily dosage; T1D, type 1 diabetes; TIR, time in range 3.9–10.0 mmol/L (70–180 mg/dL); UACR, urinary albumin-to-creatinine ratio.
Regarding drug types, DPP-4i were used in two studies (one with sitagliptin® at a maximum dose of 100 mg, and one with vildagliptin® at 100 mg), GLP-1 RA in two studies (semaglutide® at a maximum dose of 1 mg per week), and SGLT-2i in five studies (four with empagliflozin® at 25 mg, and one with dapagliflozin® at 20 mg). Seven studies utilized commercial AID systems, including MiniMed 780G (N = 2)5,6 and Control IQ systems (with Tandem pump or YpsoPump and Dexcom G6) (N = 3),7,9,11 while one used different types of commercial AID systems 8 and another used the DreaMed closed-loop system. 13
For participants, six studies focused on adults (N = 209),7–12 and three on adolescents and young adults (aged 12–21 years, N = 111).5,6,13 Three studies enrolled participants with higher BMI (criteria: >21, 18–35, and ≥30 kg/m2),7,8,13 two studies included those with TDD ≥0.8 units/(kg.d),5,6 and the remaining four studies did not restrict baseline BMI or TDD. Previous use of AID systems or insulin pumps for ≥3 months was reported in three and six studies, respectively. Baseline HbA1c inclusion criteria varied; among the eight included studies reporting baseline HbA1c, only two (16%) studies met the target of <7.0%.10,12
Primary outcomes
All meta-analysis results of TIR (nine studies, N = 320) are presented in Figure 1. Overall, the addition of SGLT-2i, GLP-1 RA, and DPP-4i to AID systems resulted in a significantly greater increase in TIR (MD: 10.0%, 95% CI: 7.3%–12.6%, P < 0.01), with moderate heterogeneity (I2 = 60.4%), corresponding to an improvement of 143 min (2.43 h) per day. Among these, SGLT-2i showed the greatest improvement in TIR, with an additional increase of 12.5% (95% CI: 9.2%–15.8%, P < 0.01, I2 = 52.4%) compared with AID systems alone or with placebo. GLP-1 RA and DPP-4i were associated with TIR improvements of 7.1% (95% CI: 3.2%–11.0%, P < 0.01) and 6.4% (95% CI: 4.0%–8.8%, P < 0.01) with low heterogeneity of 8.3% and 0.0%, respectively (P value for different drug classes was 0.02). The available within-group TIR outcomes are presented in Supplementary Table S7.
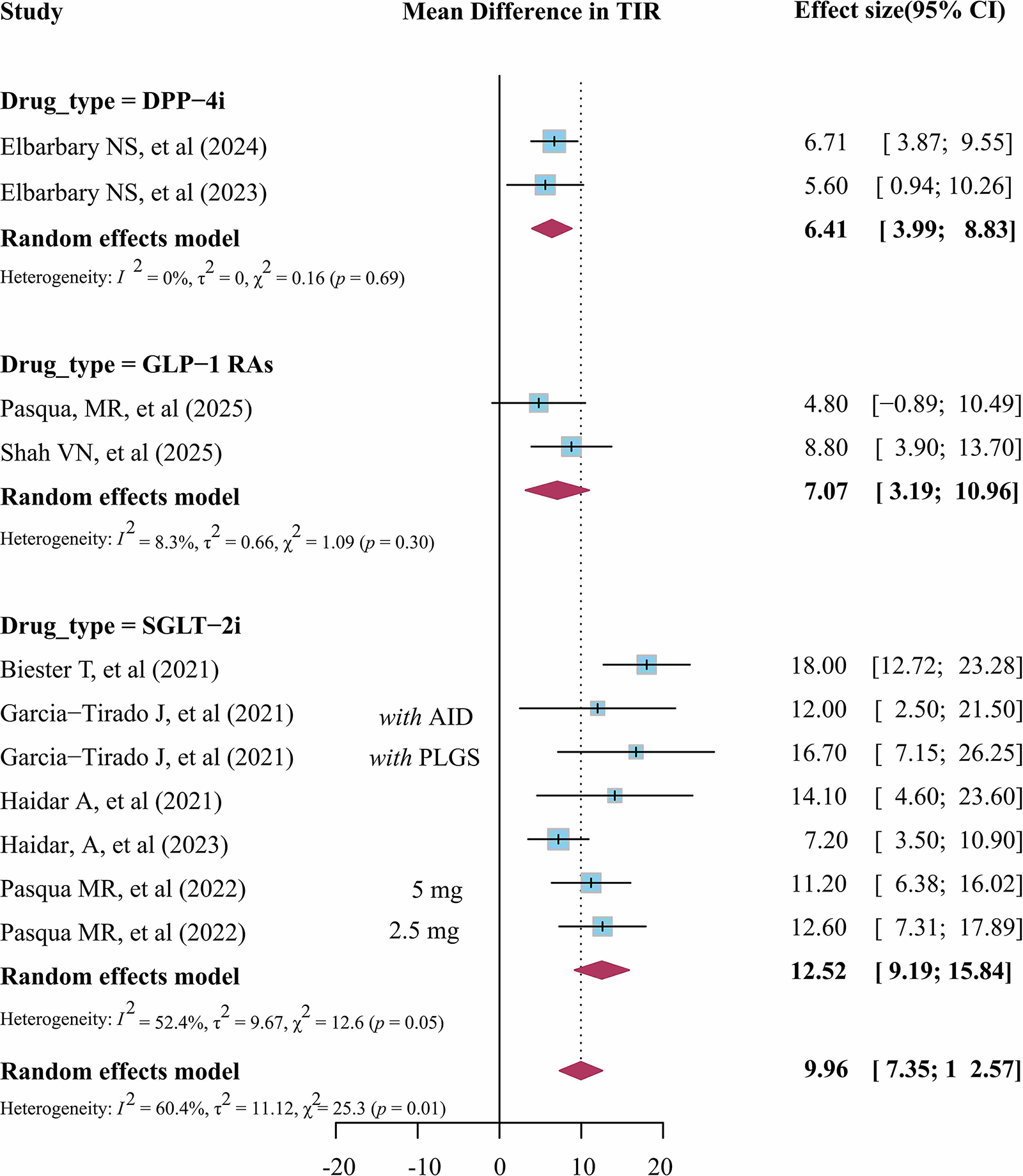
Meta-analysis of TIR. AID, automated insulin delivery; CI, confidence interval; DPP-4i, dipeptidyl peptidase-4 inhibitor; GLP-1 RA, glucagon-like peptide-1 receptor agonist; PLGS, predictive low glucose suspend; SGLT-2i, sodium–glucose cotransporter-2 inhibitor; TIR, time in range.
Secondary outcomes
Postintervention TITR was assessed in seven studies with a total of 224 participants (two studies focused on GLP-1 RA and five studies focused on SGLT-2i). As shown in Figure 2, compared with placebo plus AID systems or AID systems alone, SGLT-2i and GLP-1 RA with AID systems significantly improved TITR by a mean of 8.9% (95% CI: 6.8%–11.0%, P < 0.01, I2 = 15.4%), with SGLT-2i showing a greater improvement (10.4% [95% CI: 7.9%–12.9%], P < 0.01, I2 = 0.0%), accompanied by GLP-1 RA improving TITR by +5.6% (95% CI: 1.8%–9.3%) (P for different drug classes was 0.04).
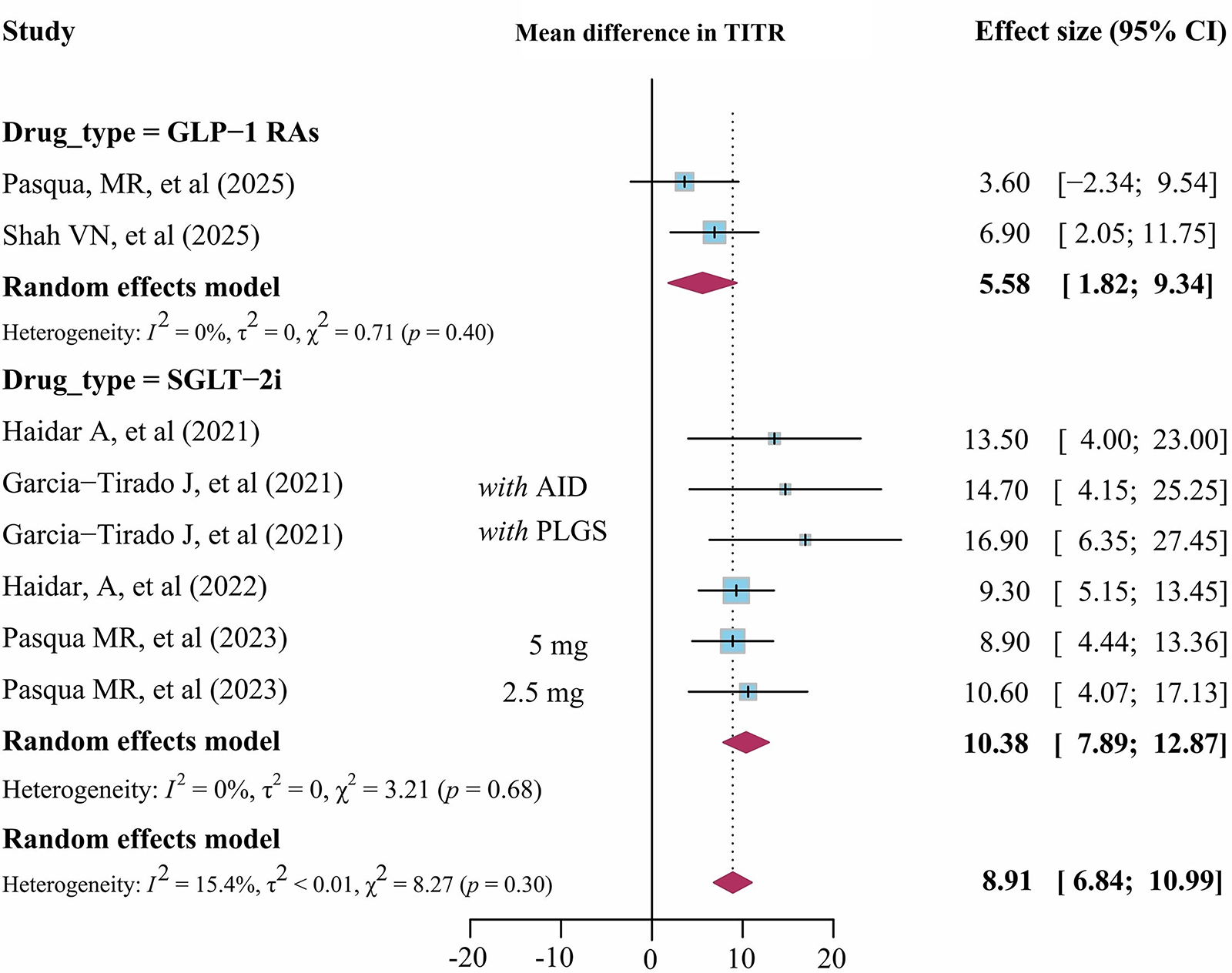
Meta-analysis of TITR. TITR, time in tight range.
All nine studies were pooled for time in hypoglycemia (TBR70; Fig. 3) and time in hyperglycemia (TAR250; Supplementary Fig. S2). The available within-group TBR70 outcomes are presented in Supplementary Table S7. Only eight studies and seven studies, respectively, reported TAR180 (Supplementary Fig. S3) and TBR54 (Supplementary Fig. S4). Overall, TBR70 and TBR54 were not significantly different between groups with the values of 0.2% (95% CI: −0.7% to 0.2%, P = 0.26, I2 = 92.6%) and values of −0.1% (95% CI: −0.2% to 0.01%, P = 0.12, I2 = 62.6%). However, the meta-analysis of two studies (96 participants) investigating DPP-4i demonstrated a significant decrease in TBR70 with MD of −0.5% (95% CI: −0.9% to −0.1%, P = 0.02, I2 = 68.6%). For TAR250, the overall difference in reduction was −4.33% (95% CI: −5.84% to −2.82%, P < 0.01, I2 = 78.0%), with the largest reduction observed in studies using SGLT-2i (MD: −5.7 [−7.6 to −3.7] %, P = 0.01, I2 = 60.7%).
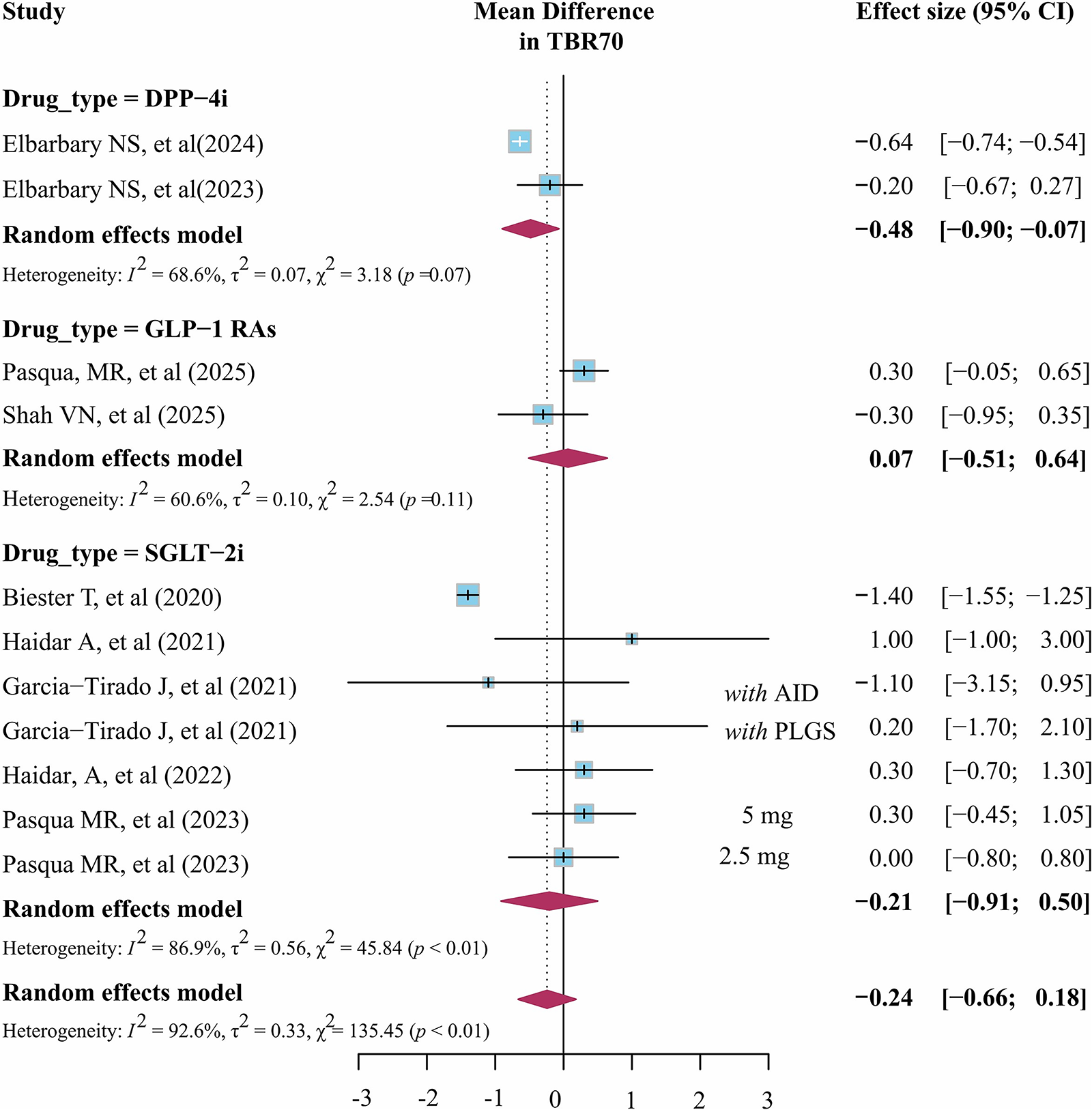
Meta-analysis of TBR70. TBR, time below range.
For glycemic variability (nine studies; Supplementary Fig. S5), SGLT-2i, GLP-1 RA, and DPP-4i used with the AID system demonstrated a significant improvement in CV by reducing −2.9% more (95% CI: −4.5% to −1.4%, P < 0.01, I2 = 73.6%). Among these, DDP-4i showed the largest improvement by −6.5% (95% CI: −11.9% to −1.1%, P = 0.02) with high heterogeneity of 80.3%. For SGLT-2i, MD was still significant by −2.5% (95% CI: −4.4% to −0.6%, P = 0.02, I2 = 73.6%), yet improvement in CV was not significant despite using GLP-1 RA with AID systems, with the effect size of −1.3% (95% CI: −3.0% to 0.5%, P = 0.17) with no heterogeneity (I2 = 0.0%).
Only three studies reported HbA1c outcomes (Supplementary Fig. S6), including two studies evaluating GLP-1 RA and one study evaluating an SGLT2i. The pooled effect size showed a mean reduction of −0.4% (95% CI: −0.9% to −0.2%; −4 mmol/mol [−6 to −2 mmol/mol]), with no observed heterogeneity (I2 = 0.0%, P < 0.01). For MBG (seven studies; Supplementary Fig. S7), the adjunctive therapy combining drugs with AID systems also resulted in a significant reduction of −1.1 mmol/L (95% CI: −1.4 to −0.8; −19.3 mg/dL [−24.8 to −13.5 mg/dL]), with I2 of 57%.
TDD, weight, and BMI
Postintervention TDD (units/day) was reported in nine studies, while one study used units/(kg.d) as the reported units (Supplementary Fig. S8). For the included studies, AID systems with SGLT-2i, GLP-1 RA, and DPP-4i significantly decreased TDD by −8.9 units (95% CI: −12.7% to −5.2%, I2 = 76.8%). Among these, GLP-1 RA showed the largest reduction of −17.3 units (95% CI: −28.6% to −6.6%, I2 = 72%), followed by DPP-4i reducing TDD by −9.5 units (95% CI: −11.9% to −7.0%, I2 = 0.0%) and SGLT-2i reducing TDD by −4.93 units (95% CI: −7.2% to −2.7%, I2 = 0.0%).
Only the studies of GLP-1 RA provided data on weight and BMI, while the other two evaluating DPP-4i reported BMI standard deviation score (BMI-SDS) (Supplementary Figs. S9 and Figs. S10). Meta-analysis showed that AID systems with GLP-1 RA significantly reduced weight by −8.7 kg (95% CI: −10.5 to −6.9 kg; P < 0.001; I2 = 0.0%). For BMI or BMI-SDS, the standardized MD was not significant (−0.94; 95% CI: −1.57 to 3.44; I2 = 76.7%). When using raw data for meta-analyses separately, consistent results were observed, with the nonsignificant MD for BMI in studies using GLP-1 RA (MD −1.49 kg/m2; 95% CI: −3.40 to 0.41; I2 = 0.0%) and a nonsignificant MD for BMI-SDS in studies evaluating DPP-4i (I2 = 73.1%).
Subgroup analyses
Subgroup analyses are presented in Supplementary Table S3. As shown, compared with adults, children and adolescents using SGLT-2i, GLP-1 RA, and DPP-4i combined with AID systems experienced greater reductions in TBR70, TAR180, and TAR250, with significant between-group differences of −0.6% (95% CI: [−1.1, −0.2] %; P = 0.006), −5.1% (95% CI: [−8.2, −2.0] %; P = 0.001), and −1.7% (95% CI: [−3.3, −0.2] %; P = 0.024). Improvements in TIR and TITR were also observed in children and adolescents, with changes of 2.0% (95% CI: [−0.6, 4.6] %) and 0.3% (95% CI: [−1.7, 2.4] %), although these differences did not reach statistical significance (P > 0.05). Among participants without prior experience with AID systems, glycemic outcomes were generally better than those previously using AID systems. Specifically, larger improvements were observed in TIR and TITR (+11.5 [8.2, 14.9] % and +9.4 [7.1, 11.7] %, respectively), with greater reductions in TAR180 and TAR250 (−12.1% [−15.6, −8.7] and −5.1% [−7.1, −3.1] %, respectively) and a smaller reduction in CV (−2.2% [−3.9, −0.6] %).
Safety outcomes
Two SAEs were reported (Supplementary Table S4), both occurring in groups treated with the GLP-1 RA. These included a recurrent tibial fracture following a previous surgery, which was considered unrelated to the study drug, and severe nausea and vomiting leading to hospitalization. In total, 92 AEs were observed among 202 patients, yielding an RR of 1.2 (95% CI: 0.9–1.5) compared with the control group (P = 0.225). Among these, there were no significant differences between the intervention and control groups in the incidences of diabetic ketoacidosis (DKA), SH, or infection, with corresponding RRs of 1.2 (95% CI: 0.3–4.2), 1.1 (95% CI: 0.7–1.5), and 1.9 (95% CI: 0.8–4.4), respectively (P = 0.77, 0.81, and 0.15; Supplementary Table S5). However, with GLP-1 RA or SGLT2i use, gastrointestinal AEs and diabetic ketosis occurred more frequently, resulting in significantly increased RRs of 2.0 (95% CI: 1.4–2.9) and 2.3 (95% CI: 1.4–3.7), respectively (both P < 0.001).
Risk of bias
Measurement of the outcome and selection of the reported result were all presented at low risks of bias in all studies (Supplementary Fig. S11). However, blinding of participants and personnel presented a high risk of bias in four studies as these studies did not use placebo as the comparator. For six crossover trials, two studies did not set up washout periods, and thus, unclear risks of bias from the carryover effects were at some concerns. In addition, missing outcome data also predominantly presented at low risks of bias except for one trial because two patients were lost to follow-up because of poor compliance after randomization and thus the risks of bias were at some concerns.
Certainty of evidence
Overall certainty of evidence for the pooled effect sizes of TIR and TAR180 was rated as high (Supplementary Table S6). Similarly, certainty for the relative risk of AEs and SAEs was also high. For TIR, TBR, and TAR250, the certainty of evidence was rated as moderate, mainly due to moderate-to-high heterogeneity (I2 > 60%). The certainty for MBG was also moderate, primarily because 71.4% of the included studies were assessed as having a high risk of bias. In contrast, the certainty of evidence for HbA1c was rated as low, largely due to one included study with a short duration (<12 weeks), which might not adequately capture the true HbA1c changes and the overlapping CIs with the minimally important difference of 0.5%.
Discussion
This systematic review and meta-analysis presents evidence from RCTs of SGLT-2i, GLP-1 RA, and DPP-4i as adjuncts to AID systems, providing timely insight into a topic of rapidly growing interest in T1D management. Overall, these agents confer a statistically significant and clinically important 10% absolute improvement in TIR and 8.9% in TITR, primarily driven by reducing TAR and glycemic variability. Importantly, these reported benefits occur without increased hypoglycemia and without elevating the risk of AEs and SAE. These overall support the safety but note a higher frequency of gastrointestinal events and diabetic ketosis observed in trials involving GLP-1 RA and SGLT2i, respectively. Beyond glycemic benefits, the adjunctive therapy was also associated with significant reductions in TDD among all drugs studied and in body weight—although the latter was only significant with GLP-1 RA.
Although AID technology has markedly advanced insulin therapy, postprandial hyperglycemia, insulin resistance, and weight gain remain therapeutic challenges for many T1D individuals. 20 In this meta-analysis, the observed TIR improvement is clinically relevant, given the established associations between TIR and reduced risk of long-term complications. Furthermore, the high-certainty evidence supporting TITR improvements further underscores the value of combining pharmacological and technological approaches to address residual treatment gaps. Across the drug classes, the most pronounced improvements in both TIR and TITR were observed with the SGLT-2i, followed by GLP-1 RA and DPP-4i. These incremental benefits align with the insulin-independent glycemic effects of SGLT-2i, including enhanced urinary glucose excretion and reductions in glucose toxicity. The findings are also consistent with prior evidence that adjunctive therapies benefit T1D individuals treated with conventional insulin regimens.3,4 Thus, taken together, the glucose-lowering effects of these agents remain clinically and physiologically relevant even in the era of automation. In contrast, although a statistically significant reduction in HbA1c was observed, the certainty of evidence was rated as low, possibly due to the limited number of included studies or a ceiling effect from already optimized glycemic control in participants using contemporary AID systems. Longer and adequately powered studies are needed to confirm the durability of these effects.
Beyond glycemic control, weight gain and high insulin dosage represent common concerns in T1D management.2,21 In this meta-analysis, adjunctive use of these agents led to an overall 8.9% reduction in TDD, with GLP-1 RA producing the greatest insulin-sparing effects, followed by DPP-4i and then SGLT-2i. These differences are consistent with the pharmacological profiles of GLP-1 RA, which include glucagon suppression and delayed gastric emptying, contributing to both weight loss and reduced insulin requirements. Notably, participants of the included studies were mostly adolescents and adults, either with higher BMI or higher insulin requirements, in whom AID systems alone may not achieve optimal metabolic outcomes. The applicability of these benefits to individuals with normal BMI or low insulin needs remains uncertain and warrants further evaluation. More importantly, unfortunately, evidence regarding weight-related outcomes was limited with only two studies reporting weight change after adding noninsulin hypoglycemic drugs (both GLP-1 RA) onto AID systems therapy.7,8 Given the general weight loss and insulin-sparing benefits, combined with proven benefits to various long-term complications in type 2 diabetes, 22 whether similar benefits could be observed in T1D populations remains under discussion. Thus, additional well-designed trials are required to better assess the potential role of noninsulin hypoglycemic drugs in weight management among AID users.
Safety remains a paramount consideration for both clinicians and individuals with T1D when integrating adjunctive pharmacotherapy with AID systems. In this meta-analysis, the overall incidence of AEs and SAEs did not differ significantly. Importantly, serious complications historically associated with adjunctive therapies—such as DKA and SH—did not increase, supporting the safety of this combination therapy. Nonetheless, similar to previous studies, the elevated incidence of diabetic ketosis with SGLT-2i and gastrointestinal events with GLP-1 RA among T1D populations warrants attention.22,23 These findings highlighted the need for careful patient selection, structured education, and frequent monitoring, particularly in individuals with prior DKA episodes, high insulin sensitivity, or a history of intolerance to incretin-based therapies. Such caution is especially important given the superior glycemic and metabolic benefits from this combination therapy and the rapidly expanding global use of AID systems.
To our knowledge, this is the first meta-analysis evaluating noninsulin hypoglycemic drugs adjunctively used with AID systems. This work extends the current evidence base into the rapidly evolving landscape of automated diabetes technology and addresses a critical knowledge gap at the intersection of pharmacotherapy and advanced insulin delivery. Another key strength lies in the stratified analysis by drug class, which provides clinically actionable insights and supports personalized therapeutic decision-making. Furthermore, the detailed and nuanced evaluation of safety outcomes offers important reassurance for real-world clinical implementation. However, several limitations should be acknowledged. Although the search strategy encompassed most noninsulin hypoglycemic agents, to date, only SGLT-2i, DPP-4i, and GLP-1 RA have been reported, while a study on metformin is currently underway. 18 The number of available studies and participants was limited, and most trials were short-term (<6 months), precluding assessment of long-term durability and safety. Although the subgroup analysis of different drugs added to AID systems is informative, direct comparisons across studies with varying designs and sample sizes may introduce bias into the results. Moderate-to-high heterogeneity was observed in some outcomes, potentially reflecting variations in AID systems, drug classes, dosing regimens, and participant characteristics (e.g., BMI, prior use of AID systems). In addition, blinding was not feasible in some studies, which may introduce performance bias, and crossover designs without washout periods could raise concerns for carryover effects. Certainty of evidence for some secondary and safety outcomes was downgraded for imprecision due to wide CIs and infrequent AEs.
Conclusion
In conclusion, this systematic review and meta-analysis indicates that SGLT-2i, DPP-4i, and GLP-1 RA has the potential to serve as safe and effective adjuncts to AID systems for individuals living with T1D. Specific benefits span improvements in TIR, reductions in hyperglycemia, and reduced insulin requirements. However, these findings were derived from a limited number of mostly short-duration trials and are accompanied by an increased risk of diabetic ketosis and gastrointestinal AEs. Therefore, while the adjunctive pharmacotherapy may complement AID systems in selected individuals, its broader clinical role requires confirmation in adequately powered and long-term randomized trials with robust safety assessment.
Authors’ Contributions
Y.Z., M.L., and Q.L.: Conduct/data collection, analysis, and writing—article. Y.N. and Z.L.: Analysis. D.Y.: Writing—article. J.Y., W.X., and C.W.: Design and writing—article. All authors have read and approved the final article.
Footnotes
Acknowledgments
Dr. J.Y. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. The authors thank Professor Benjamin John Wheeler for his revision for language improvement.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Noncommunicable Chronic Diseases-National Science and Technology Major Project (2023ZD0508200, 2023ZD0508203).
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.