
Abstract
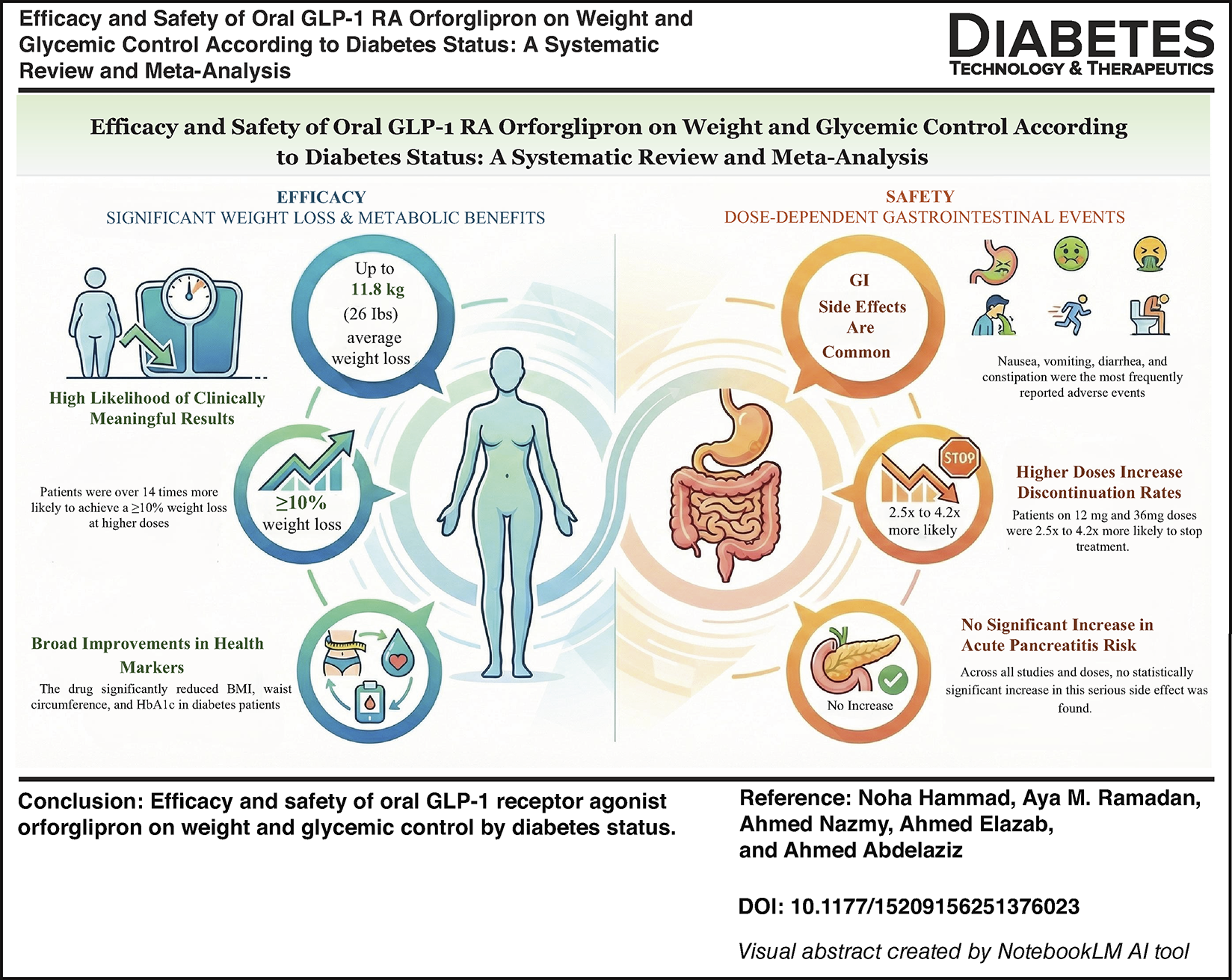
Excess body weight and poor metabolic control remain major contributors to cardiometabolic disease, highlighting the need for effective therapeutic options. This meta-analysis aimed to evaluate the efficacy and safety of once-daily oral orforglipron in obese adults with and without diabetes. Searches were conducted across four databases through November 2025. Five randomized controlled trials (n = 6140) were included. Orforglipron produced consistent, dose-dependent reductions in body weight, ranging from modest losses at 3 mg to more than 6 kg at 36 mg in patients with diabetes. Individuals without diabetes experienced greater weight reductions, approaching 12 kg at the highest dose. Significant improvements in body mass index, waist circumference, and glycated hemoglobin (HbA1c; –1.29%) were also observed. Gastrointestinal adverse events increased with higher dose, and no significant difference in the incidence of acute pancreatitis was identified. Overall, orforglipron demonstrated clinically meaningful metabolic benefits with an acceptable safety profile.
Introduction
Obesity represents a major global health burden and is a leading risk factor for numerous chronic diseases, affecting more than one billion individuals worldwide. 1 Glucagon-like peptide 1 (GLP-1) receptor agonists are incretin-based therapies that provide multiple clinical benefits beyond glycemic control, including substantial weight reduction and improved cardiovascular outcomes. Currently, oral semaglutide, the only available oral GLP-1 receptor agonist, requires strict fasting and timing conditions to ensure adequate absorption and has demonstrated less pronounced weight-loss effect compared with its approved injectable formulation. 2 Preliminary clinical trials suggest that orforglipron demonstrates promising glucose-lowering and weight-reducing effects, with pharmacokinetic properties that support convenient once-daily oral administration. 2 These characteristics may translate into improved treatment adherence and enhanced therapeutic outcomes. 2 However, high-quality evidence is still needed to validate the clinical efficacy of orforglipron and to inform evidence-based practice recommendations. Therefore, this meta-analysis aimed to comprehensively evaluate the available evidence regarding the efficacy of orforglipron in reducing body weight and improving patient-related outcomes in obese adults irrespective of their diabetes status.
Methods
This study was conducted in accordance with the Cochrane Handbook for Systematic Reviews and Meta-analyses of Interventions. We included all phase II and III randomized controlled trials (RCTs) that compared once-daily oral orforglipron with placebo in adults with overweight or obesity, defined as a body mass index (BMI) ≥27 kg/m2 with at least one weight-related comorbidity or a BMI ≥30 kg/m2, with or without type 2 diabetes mellitus.
A comprehensive literature search was performed in PubMed, Web of Science, Scopus, and Cochrane CENTRAL from inception until November 2025 without language restrictions. The search strategy included the following search terms: (orforglipron OR LY3502970 OR “oral GLP-1 receptor agonist” OR “oral GLP-1 RA” OR “glucagon-like peptide-1 receptor agonist”) AND (obesity OR obese OR overweight OR “body weight” OR “weight loss” OR BMI) AND (“type 2 diabetes” OR T2DM OR “diabetes mellitus” OR diabetic OR nondiabetic OR non-diabetic).
Two authors independently screened studies and extracted data using a pilot-tested standardized extraction form. Data were extracted according to the intention-to-treat principle, whereby all randomized participants were analyzed according to their assigned treatment groups. The primary efficacy outcomes included percent and absolute changes in body weight, changes in waist circumference, BMI, and glycated hemoglobin (HbA1c; %). Safety outcomes included treatment discontinuation, gastrointestinal adverse events (diarrhea, nausea, vomiting, and constipation), and acute pancreatitis. A random-effects meta-analysis using restricted maximum likelihood estimation was performed to calculate pooled mean difference (MD) with corresponding 95% confidence intervals. Statistical analyses were conducted using R software (version 4.5.2), and a two-sided P value <0.05 was considered statistically significant.
Results
Five RCTs, GZGI 2023, 3 ATTAIN-1 2025, 4 ATTAIN-2 2025, 5 Frias 2023, 6 and ACHIEVE-1 2025 7 were included in the final analysis, comprising 6140 patients, of whom 2571 (41.8%) were males. The mean (SD) age was 50.3 (12.8) years, and the mean follow-up duration was 49.2 (21.43) weeks. Baseline mean (SD) body weight was 101.6 (22.8) kg, BMI 36.2 (6.7) kg/m2, and waist circumference 113.1 (15.1) cm. All included studies evaluated the effects of orforglipron on weight-related and metabolic outcomes, stratified by diabetes status.
Efficacy outcomes
Orforglipron demonstrated consistent, dose-dependent improvements in weight-related outcomes across both diabetes and non-diabetes populations. In patients with diabetes, percentage body weight reductions were significant at all evaluated doses, with MDs of −2.15% at 3 mg (P = 0.0009), −4.34% at 12 mg (P < 0.0001), and −4.43% at 36 mg (P < 0.0001) (Fig. 1A). In contrast, patients without diabetes experienced larger reductions of –6.40% at 12 mg and −9.69% at 36 mg (both P < 0.0001) (Fig. 1B).
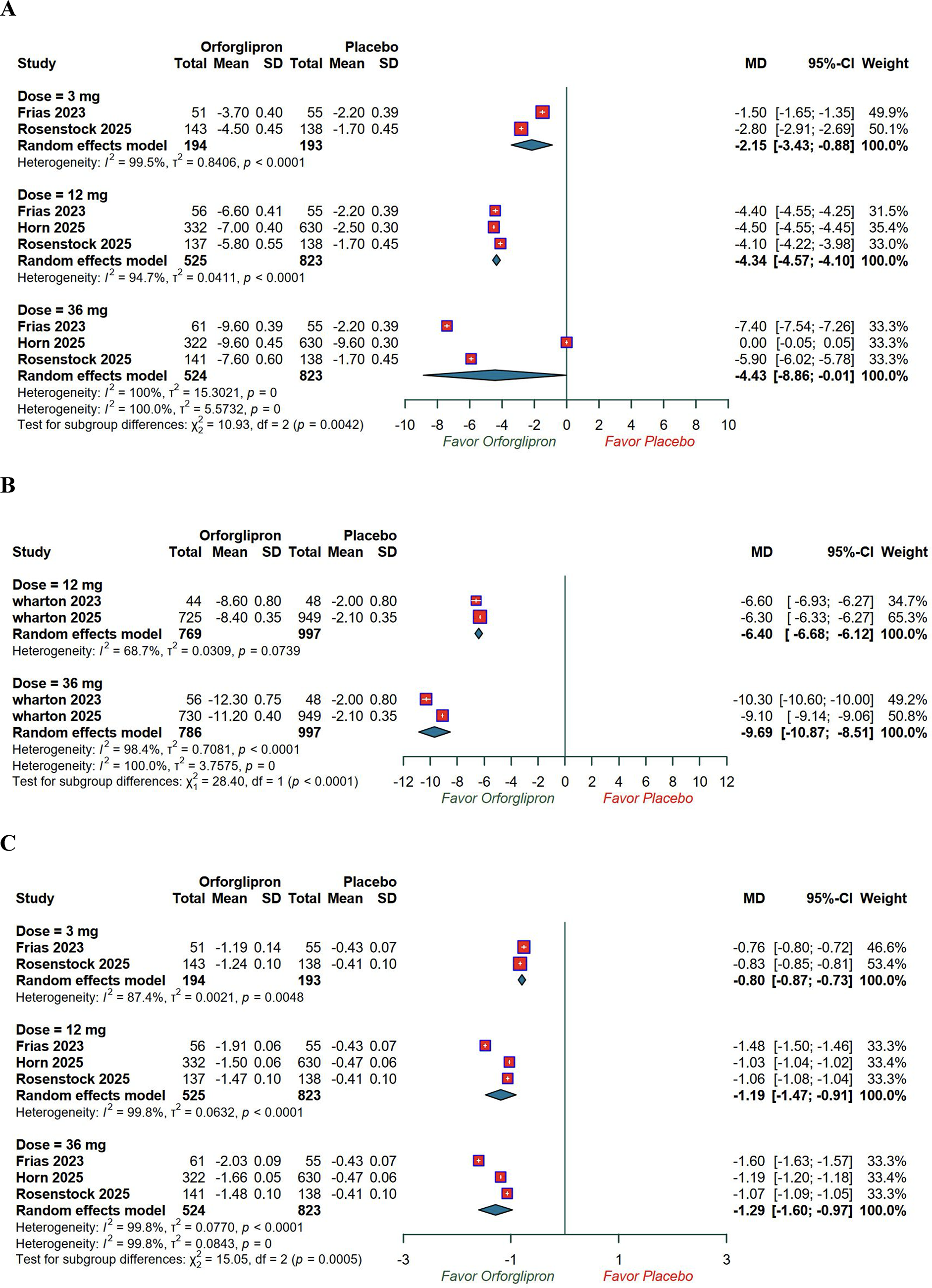
Absolute weight reduction followed a similar pattern. In patients with diabetes, reductions were −2.10 kg at 3 mg (P = 0.0005), −4.17 kg at 12 mg (P < 0.0001), and −6.63 kg at 36 mg (P < 0.0001). In patients without diabetes, greater weight reductions were observed, reaching −8.00 kg at 12 mg and −11.84 kg at 36 mg (both P < 0.0001) (Supplementary Appendix).
Among patients with diabetes, orforglipron significantly reduced HbA1c at all doses, with MDs of −0.80% at 3 mg, −1.19% at 12 mg, and −1.29% at 36 mg (all P < 0.0001) (Fig. 1C).
The probability of achieving clinically meaningful weight loss was significantly higher with orforglipron. For ≥5% weight loss, odds ratios (ORs) in patients with diabetes were 2.76 at 3 mg (P = 0.0065), 4.47 at 12 mg (P < 0.0001), and 7.49 at 36 mg (P < 0.0001). Corresponding ORs in patients without diabetes were 5.02 at 12 mg (P < 0.0001) and 13.95 at 36 mg (P = 0.0009). Similar trends were observed for ≥10% weight loss, with ORs in patients with diabetes of 2.26 at 3 mg (P = 0.0296), 5.76 at 12 mg (P < 0.0001), and 10.11 at 36 mg (P < 0.0001), and in patients without diabetes of 5.03 at 12 mg and 14.31 at 36 mg (both P < 0.0001) (Supplementary Appendix).
For ≥15% weight loss, statistically significant effects were observed only at higher doses. In patients with diabetes, both 12 mg and 36 mg were effective (OR = 7.30 and 15.99, respectively; both P < 0.0001), whereas the 3 mg was not (OR = 2.02, P = 0.5979). In patients without diabetes, significant benefits were observed at 12 mg (OR = 6.39, P = 0.0208) and 36 mg (OR = 15.65, P = 0.003). Consistent reductions were also noted in BMI, with patients with diabetes showing decreases of −0.80 at 3 mg (P = 0.0078), −1.55 at 12 mg (P < 0.0001), and −2.38 at 36 mg (P < 0.0001). Patients without diabetes experienced greater reductions of −2.50 at 12 mg and −4.10 at 36 mg (both P < 0.0001) (Supplementary Appendix).
Waist circumference decreased in a dose-dependent manner, with significant reductions at 12 mg and 36 mg in patients with diabetes (MD = −2.71 and −5.21, respectively; both P < 0.0001). In patients without diabetes, significant reductions were observed at both doses (MD −5.29 and −6.82, respectively; both P < 0.0001). No significant reduction was observed at 3 mg in diabetes (MD = −1.20, P = 0.3905) (Supplementary Appendix).
Safety outcomes
Across all studies, gastrointestinal adverse events were more frequent with orforglipron than placebo, with a clear dose-dependent relationship. Treatment discontinuation rate was significantly higher at 12 mg and 36 mg in patients with diabetes (OR = 2.48, P < 0.0002; OR = 2.59, P < 0.0001) and in patients without diabetes (OR = 3.17, P < 0.0001; OR = 4.22, P < 0.0001). The 3 mg dose did not significantly increase discontinuation rates in patients with diabetes (OR = 3.70, P = 0.18) (Supplementary Appendix).
The risk of diarrhea was increased at all doses in patients with diabetes, while in patients without diabetes a significant increase was observed only at 12 mg. Nausea, vomiting, and constipation were consistently more frequent with orforglipron, particularly at higher doses, in both diabetes and non-diabetes populations. Acute pancreatitis did not differ significantly between orforglipron and placebo at any dose, regardless of diabetes status (all P > 0.05) (Supplementary Appendix).
Discussion
This systematic review and meta-analysis represents the first comprehensive report to date of the efficacy of orforglipron compared with placebo in overweight or obese adults, irrespective of their diabetic status, based on phase II and III RCTs. We included five RCTs comprising 6140 patients in a parallel random-effect model meta-analysis in which MDs for clinical outcomes were assessed at the longest available follow-up duration for each study. Orforglipron demonstrated significant dose-dependent reductions in body weight, waist circumference, BMI, and HbA1c, as well as increased treatment discontinuation rates (Graphical Abstract). Gastrointestinal adverse events also exhibited a clear dose-dependent relationship, whereas no significant difference in acute pancreatitis was observed. These findings support the emerging evidence that orforglipron is an effective oral GLP-1 receptor agonist to induce clinically meaningful weight loss and glycemic improvement comparable with injectable GLP-1 analogs.
FDA-approved once-weekly injectable incretin-based therapies for obesity, such as semaglutide and tirzepatide, have demonstrated average weight reductions of approximately 15% and more than 20%, respectively. 8 Weight loss of at least 10% is generally considered as a clinically relevant threshold associated with substantial metabolic and cardiometabolic benefits. 9 The observed weight reductions in both patients with and without diabetes are consistent with the established physiological mechanisms of GLP-1 receptor activation, including enhanced satiety, delayed gastric emptying, and augmented glucose-dependent insulin secretion. Notably, the greater magnitude of weight loss observed among patients without diabetes may reflect differences in baseline insulin resistance, metabolic rate, or concomitant medication use.
Higher discontinuation rates were observed with increasing doses of orforglipron, reflecting dose-related gastrointestinal adverse effects that are associated with GLP-1 receptor agonist class. Although serious events, including acute pancreatitis, were rare, the limited number of events reduces statistical power to detect meaningful differences. Overall, the safety profile of orforglipron appears consistent with established class effects.
Consistent with the recent meta-analysis by Pandey et al., 10 we observed significant reductions in body weight, BMI, waist circumference, and HbA1c, with a clear dose-dependent pattern of gastrointestinal adverse events. Our study complements and extends these findings by including an additional pivotal phase III trial, 5 increasing the overall sample size to 6140 patients. This larger dataset allows for more precise estimates of treatment effects and provides a comprehensive assessment of dose–response relationships and safety outcomes, including adverse events such as acute pancreatitis.
Compared with traditional oral semaglutide, orforglipron may offer important clinical advantages related to patient convenience and adherence. Oral semaglutide requires fasting administration for at least 30 min prior to food intake, which may limit adherence and reduce real-world effectiveness. 11 In contrast, orforglipron can be administered without regard to meals and demonstrates consistent bioavailability, potentially enhancing treatment compliance and expanding tolerability to GLP-1-based therapies. As such, orforglipron may represent a more practical and effective alternative for individuals reluctant to initiate injectable therapies due to its favorable pharmacokinetic and pharmacodynamic properties. 12
Consistent with the known glycemic effects of GLP-1 receptor agonists, orforglipron significantly reduced HbA1c levels in patient with diabetes. 7 The combined benefits of weight loss and glycemic control may translate into long-term cardiovascular and metabolic protection, as previously demonstrated with agents such as liraglutide and semaglutide.
Nevertheless, several limitations should be acknowledged. First, although our results provide novel insights by including patients with obesity, irrespective of their diabetic status, only five early-phase RCTs with relatively short-term durations (median 38 weeks) were available, which may limit assessment of long-term efficacy and durability. Second, we were unable to conduct a comprehensive evaluation of rare or delayed adverse events, highlighting that further safety measures are needed to quantify the full risk-benefit profile. Finally, heterogeneity in study populations, dosing strategies, and baseline metabolic characteristics may have contributed to variability in treatment response.
Conclusion
This meta-analysis, including 6140 patients across five phase II/III RCTs, demonstrates that orforglipron provides robust, dose-dependent efficacy in reducing body weight and improving glycemic control. Acute pancreatitis and vomiting were rare and did not exhibit a consistent dose–response relationship. The most pronounced weight-loss effects were observed in individuals without diabetes, whereas higher doses of orforglipron achieved superior glycemic control in patients with diabetes, underscoring the importance of patient stratification in its therapeutic decision-making. These findings support orforglipron as a first-in-class oral, non-peptide GLP-1 RA with favorable adherence characteristics and clinical efficacy comparable with injectable GLP-1-based therapies. Further studies should prioritize longer follow-up durations to evaluate cardiovascular outcomes, durability of weight loss, and real-world adherence.
AI and Transparency Statement
No generative AI tools (ChatGPT) were used for data analysis, statistical modeling, or interpretation of results. All analyses and figures were generated by the authors using R software. The graphical abstract was created using NotebookLM solely as a visualization aid to organize and illustrate results already produced by the authors.
Authors’ Contributions
N.H. and A.N. conceived and designed the study. N.H., A.M.R., A.E., and A.A. performed the literature search and screening of studies. A.M.R., A.E., and A.A. contributed to data acquisition and analysis. A.M.R. and A.E. performed statistical analyses. N.H., A.M.R., A.E., and A.N. interpreted the data. N.H., A.M.R., A.N., and A.E. drafted the article, and A.A. and N.H. critically revised it for important intellectual content. A.A. supervised the study. All authors reviewed and approved the final version of the article.
Footnotes
Acknowledgments
Dr. Ahmed Abdelaziz is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Any further requests should be emailed at
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The authors received no financial support for the research, authorship, or publication of this article.
Availability of Data and Materials
All data are available and attached.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.