
Abstract
Background:
Lifestyle interventions focusing on diet and physical activity often fail to achieve sustained weight loss, primarily due to low adherence. Intermittently scanned continuous glucose monitoring (isCGM) may serve as a behavioral feedback tool, enhancing motivation and compliance in individuals with obesity.
Objectives:
To evaluate whether incorporating isCGM into a structured lifestyle intervention improves weight loss, body composition, and metabolic outcomes in women living with obesity.
Methods:
In this 12-week randomized controlled trial, 35 women with overweight or obesity (body mass index [BMI] > 25 kg/m2) were assigned to either an intervention group (n = 17) using isCGM at baseline, mid-intervention, and study end, or a control group (n = 18) using isCGM only at baseline and end. Both groups participated in supervised exercise (3 sessions/week) and received identical dietary counseling. Primary outcomes included changes in body weight and BMI; secondary outcomes comprised body composition, adherence to dietary recommendations, and CGM metrics (time in range [TIR], time below range [TBR], coefficient of variation, HbA1c).
Results:
Compared with controls, the intervention group achieved significantly greater reductions in body weight (−5.5 ± 2.3 kg vs. −0.2 ± 1.8 kg, P < 0.001), BMI (−1.9 ± 0.6 vs. −0.1 ± 0.4 kg/m2, P < 0.001), waist-to-height ratio, body fat, and visceral fat, alongside increased muscle mass and improved dietary adherence (P < 0.05). Clinically meaningful weight loss (≥3% BMI and body fat reduction) occurred in 35% of the intervention group versus 0% of controls. TIR improved modestly in the intervention group (P = 0.03).
Conclusions:
Integrating isCGM into lifestyle interventions enhances adherence and supports clinically significant improvements in body composition and glycemic control among women with obesity. Larger, longer-term studies are warranted to confirm these findings.
Keywords
Introduction
Excess body weight (either in the preclinical or clinical stage) represents a health care burden and is closely linked to a variety of health complications. At the population level, these conditions are typically diagnosed using the body mass index (BMI), according to which individuals with a BMI between 25 and 30 kg/m2 are classified as overweight/preobese, while those with a BMI of 30 kg/m2 or higher are considered obese. 1 As a more relevant measure of visceral adiposity, waist circumference, waist-to-hip ratio (WHR), and waist-to-height ratio are used,2,3 and in routine clinical practice, assessment of body composition is most commonly performed by bioimpedance scales that suggest the proportion of fat mass and fat-free mass (including muscle, bone, and water) and help monitor success of different weight-loss interventions. 4 Excess body weight and obesity increase the risk of chronic diseases that can affect all organ systems. In addition to their impact on health, these conditions also pose significant financial burdens on health care systems. 3
In women, excess weight and obesity are associated with a range of health issues, such as prediabetes or diabetes, MASLD, polycystic ovary syndrome (the most common cause of infertility), depression, anxiety, and musculoskeletal disorders. These conditions greatly affect quality of life, prompting many women to seek support through forums or groups focused on body image, weight loss, and weight reduction. Unfortunately, only a small percentage of overweight or obese individuals consult a health care professional or seek dietary advice unless they already have chronic diseases.5,6
Despite a general understanding of the importance of proper nutrition and regular physical activity for preventing and treating obesity, very few overweight individuals adopt these habits. Even among those who participate in structured exercise programs, long-term adherence tends to be low. Moreover, there is a notable lack of scientifically based recommendations for personalized diets, as well as for the effects of specific macronutrients on energy metabolism and glucose levels during weight loss programs in individuals without dysglycemia. Moreover, there is insufficient guidance regarding the most effective types, durations, and intensities of exercise needed to achieve clinically significant weight loss (5%–7% of initial BMI). 7
Today, continuous glucose monitoring (CGM) devices are increasingly used to evaluate overall well-being and nutrition, extending beyond their primary role in monitoring glucose levels in individuals with diabetes. CGM systems consist of a sensor implanted under the skin, typically on the back of the upper arm, which continuously measures glucose levels in the interstitial fluid. These readings can be accessed via a special scanner or a smartphone. In addition to displaying current glucose levels, CGM systems illustrate trends in glucose changes through directional arrows: horizontal (stable), upward (rising), or downward (falling), alerting users to fluctuations in glucose levels.
The use of CGM, especially intermittently scanned CGM (isCGM), offers insights into how different macronutrients impact glucose levels and, indirectly, how they influence the secretion of various hormones important for metabolism (such as insulin and incretins) as well as energy storage. 8 Although the literature on this subject is still limited, current findings suggest that using isCGM can enhance quality of life, better regulate blood glucose levels, and reduce vascular complications associated with hyperglycemia.9,10 However, evidence on its role in weight management among individuals with obesity but without diabetes remains limited, 11 although recently, the availability of CGM has increased its use in other populations to avoid diabetes, improve both physical and mental performance, and motivate healthy behavioral choices. 12 This randomized controlled trial aimed to investigate whether integrating isCGM into a structured 12-week lifestyle intervention could enhance weight loss, improve body composition, and support adherence to diet and exercise in women living with obesity. We hypothesized that participants using isCGM would achieve greater reductions in body weight, BMI, and visceral fat, alongside improved dietary adherence and metabolic markers, compared with those receiving the same intervention without isCGM feedback.
Evidence supporting the use of intermittently scanned CGM in populations without diabetes is emerging. Kitazawa et al. demonstrated that integrating isCGM with smartphone-based lifestyle counseling improved weight and behavioral outcomes in individuals at high risk for diabetes. 11 Similarly, Chekima et al. reported improvements in body composition and metabolic parameters when real-time CGM was combined with a low glycemic index diet in overweight adults. However, data in women with obesity but without dysglycemia remain limited, providing the rationale for the present study. 13
Materials and Methods
Study design and participants
This study was designed as a 12-week, prospective, randomized, controlled, open-label trial investigating the impact of isCGM on weight loss, body composition, and lifestyle adherence among women living with obesity. Eligible participants were euthyroid adult females aged 18–60 years, with a BMI >25 kg/m2, and normal fasting glucose levels. Exclusion criteria included prediabetes or diabetes, diagnosed hypo- or hyperthyroidism, significant anemia, pregnancy, or musculoskeletal conditions precluding participation in exercise. Participants were recruited through public advertisements and screened for eligibility during baseline assessments. All provided written informed consent before enrollment. Only women were included to reduce biological heterogeneity related to sex-specific differences in fat distribution, hormonal regulation, glucose metabolism, and behavioral responses to lifestyle interventions. Given the relatively small sample size, restricting the cohort to women improved internal validity. The study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines and approved by the Ethical Committee of the University of Zagreb, Faculty of Kinesiology (Approval No. 84/2024). The trial was prospectively registered at ClinicalTrials.gov (NCT07026903). A schematic overview of the study design and timeline is provided in Figure 1. The figure illustrates baseline assessments, timing of isCGM use, duration of the intervention, and final outcome assessments for both the intervention and control groups.
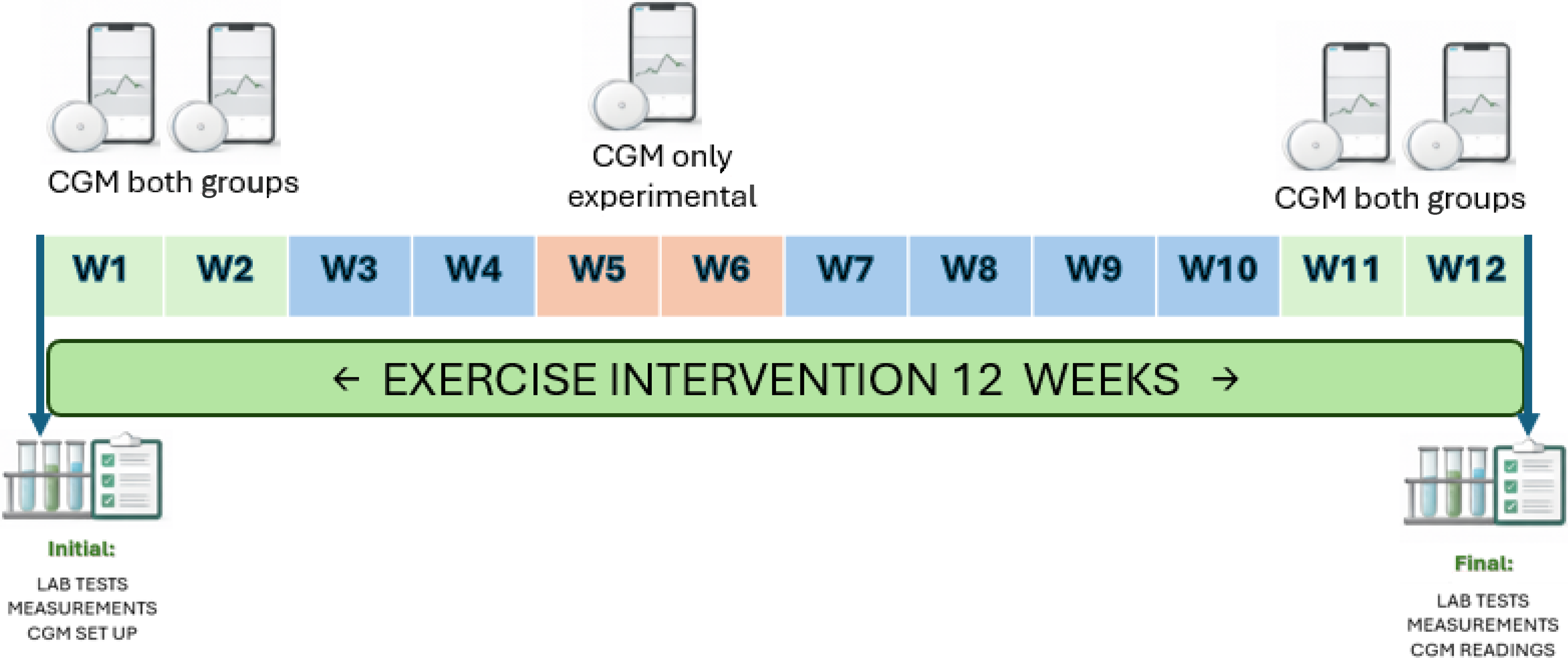
The intervention group used intermittently scanned continuous glucose monitoring (isCGM) for 14 days at baseline, during weeks 5–6, and at study end (weeks 11–12). The control group used isCGM for 14 days at baseline and at study end only. Both groups participated in identical supervised exercise and dietary counseling throughout the 12-week intervention.
Sample size and randomization
Sample size was estimated using G*Power software (version 3.1.9.7) to detect a medium effect size (Cohen’s d = 0.5) with 80% power and α = 0.05, resulting in a required minimum of 16 participants per group. A total of 35 subjects were included in the study. Participants were randomly assigned (1:1) to either the intervention group (isCGM-enhanced lifestyle program) or the control group (standard lifestyle program) using a computer-generated randomization list prepared by an investigator not involved in data collection. Due to the nature of the intervention, blinding was not feasible for participants or investigators.
Intervention protocol
All participants received a structured lifestyle intervention, consisting of individualized nutritional counseling and a supervised exercise program. Each participant received a personalized hypocaloric meal plan, developed by a licensed nutritionist, based on individual energy requirements and macronutrient distribution of 45%–50% carbohydrates, 25%–30% fat, and 20%–25% protein. Participants attended educational sessions covering portion control, balanced meals, and meal timing. Dietary adherence was assessed at study end via structured interviews and categorized as adherent or nonadherent. Participants attended three 60-minute supervised exercise sessions per week, led by a certified kinesiologist. Sessions included aerobic, resistance, and flexibility training, targeting moderate-to-vigorous intensity (60%–75% HRmax). Attendance was recorded, and only participants completing ≥90% of sessions were included in the final per-protocol analysis. The FreeStyle Libre 2 (Abbott, USA) isCGM system was used. The intervention group wore isCGM sensors for 14 days at baseline, weeks 5 and 6, and weeks 11 and 12, providing mid-program feedback. The control group wore isCGM sensors for 14 days at baseline and week 11/12 only. Participants were instructed to scan the sensor at least 8 times per day and review glucose trends via the mobile app. Those in the intervention group were encouraged to use glucose feedback to adjust meal composition and timing.
Anthropometric and bioelectrical impedance analysis (BIA) measurements were collected at baseline and 12 weeks under standardized conditions (morning, fasting state, light clothing, no exercise 24 h prior).
Exercise attendance was tracked via session logs. Dietary adherence was determined by a structured dietitian interview and food diary review at week 12.
Outcome measures
Primary outcomes were defined as change in body weight (kg) and change in BMI, whereas secondary outcomes included changes in body composition: percentage of body fat, visceral fat index, and skeletal muscle mass, assessed using BIA; anthropometric measures: waist, hip, chest, thigh, and biceps circumferences; waist-to-hip ratio (WHR); waist-to-height ratio (WHtR); laboratory markers: fasting glucose, HbA1c (eGMI), and lipid profile; CGM metrics: time in range (TIR; 3.9–10 mmol/L), time below range (TBR; <3.9 mol/L), time above range (TAR; >10 mol/L), coefficient of variation (CV); and adherence: dietary adherence (self-reported, binary: adherent/nonadherent) and exercise attendance. A composite CGM outcome score was constructed by standardizing (z-scores) and summing changes in TIR, CV, and mean glucose. Higher composite scores reflected improved glycemic stability. This composite was used to explore integrated CGM-related changes rather than isolated metrics. A composite morphological outcome was predefined to capture clinically meaningful body composition changes. This composite was defined as achieving both a ≥3% reduction in BMI and a ≥3% reduction in body fat percentage at 12 weeks. These thresholds were selected based on evidence that 3%–5% reductions in adiposity are associated with metabolic and cardiovascular benefits in lifestyle interventions. This composite outcome was exploratory and developed specifically for this trial. In addition, a success score combining the composite morphological outcome and a TIR ≥ 1% increase was predefined.
A ≥1% increase in TIR was considered an exploratory indicator of CGM improvement. Given the normoglycemic status of participants and high baseline TIR values (>96%), larger absolute improvements were not anticipated. This threshold reflects relative improvement in glycemic stability rather than clinical normalization.
Statistical analysis
Data were analyzed using Statistica 14.1 (TIBCO Software, USA). Analyses followed a per-protocol approach, including only participants completing ≥90% of sessions. Baseline differences between groups were tested using independent-samples t-tests. Analysis of Covariance was applied to assess post-intervention differences between groups, adjusting for baseline values. Nonparametric data (e.g., CGM metrics) were analyzed using the Mann–Whitney U test. Categorical data (e.g., dietary adherence, composite outcome achievement) were compared using the chi-square or Fisher’s exact test. Results are presented as mean ± standard deviation (SD) or median (IQR). Statistical significance was set at P < 0.05. Effect size (Cohen’s d) and observed power were calculated for primary outcomes.
Results
Participant baseline characteristics
A total of 48 women were screened, and 35 met the inclusion criteria and were randomized to either the intervention group (n = 17) or the control group (n = 18). All participants completed the 12-week intervention and were included in the per-protocol analysis (≥90% attendance). No adverse events or dropouts were reported. Baseline characteristics were comparable between groups (Table 1). There were no significant differences in age, BMI, body composition, anthropometric measures, or metabolic parameters, except for slightly lower HbA1c levels in the intervention group (P = 0.03). Both groups were similar in duration of excess weight, sedentary work status, and baseline physical activity levels.
Baseline Characteristics of Participants in the Intervention and Control Groups
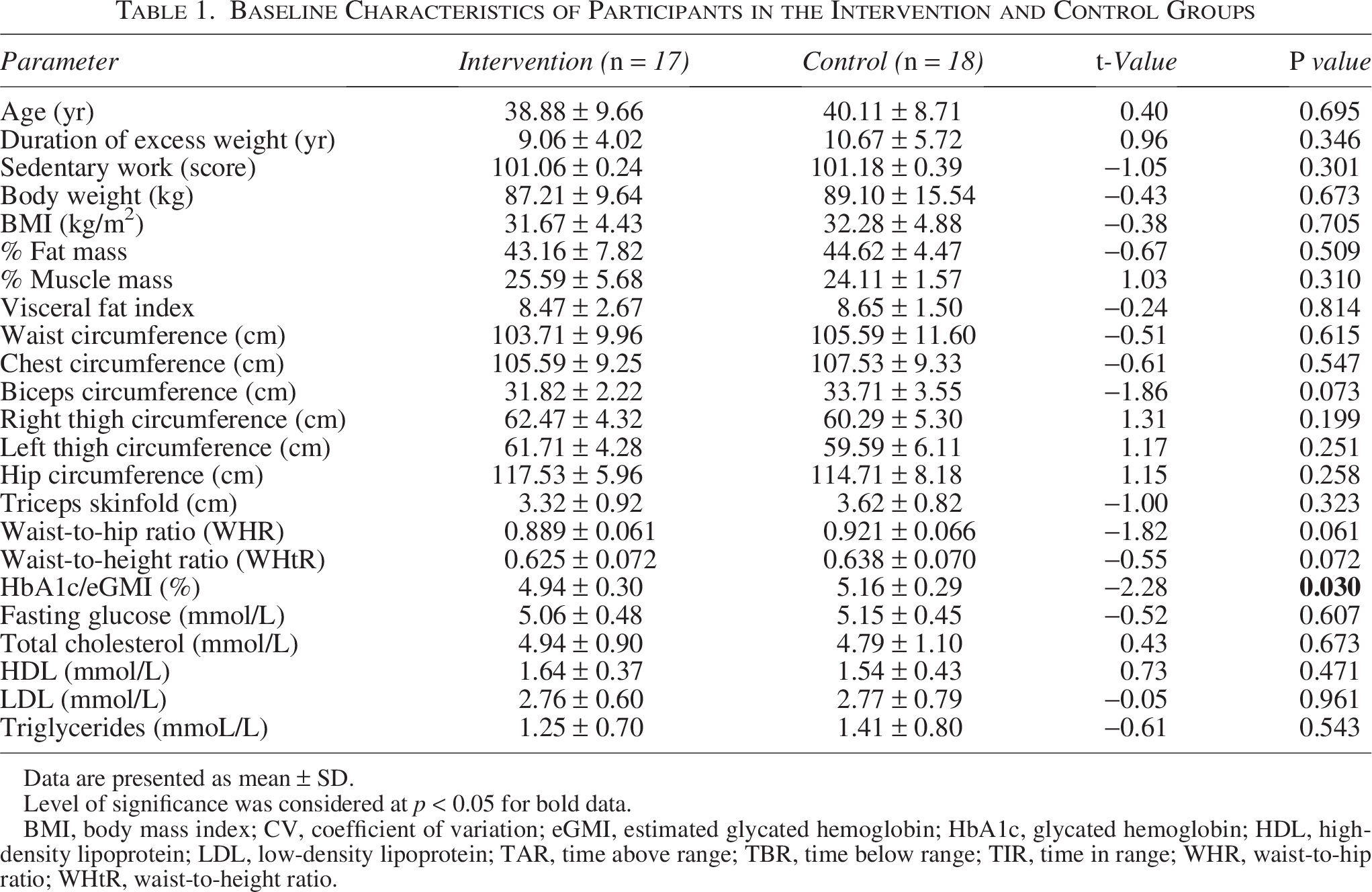
Data are presented as mean ± SD.
Level of significance was considered at p < 0.05 for bold data.
BMI, body mass index; CV, coefficient of variation; eGMI, estimated glycated hemoglobin; HbA1c, glycated hemoglobin; HDL, high-density lipoprotein; LDL, low-density lipoprotein; TAR, time above range; TBR, time below range; TIR, time in range; WHR, waist-to-hip ratio; WHtR, waist-to-height ratio.
Adherence to the intervention
At the end of the study, dietary adherence was significantly higher in the intervention group compared with controls (76.5% vs. 38.9%, P < 0.05, Fisher’s exact test; Table 2). Exercise adherence was ≥90% across all participants by design.
Dietary Adherence by Study Group and Between-Group Comparison of Changes in Anthropometric, Body Composition, Biochemical, and CGM-Derived Outcomes at 12 Weeks
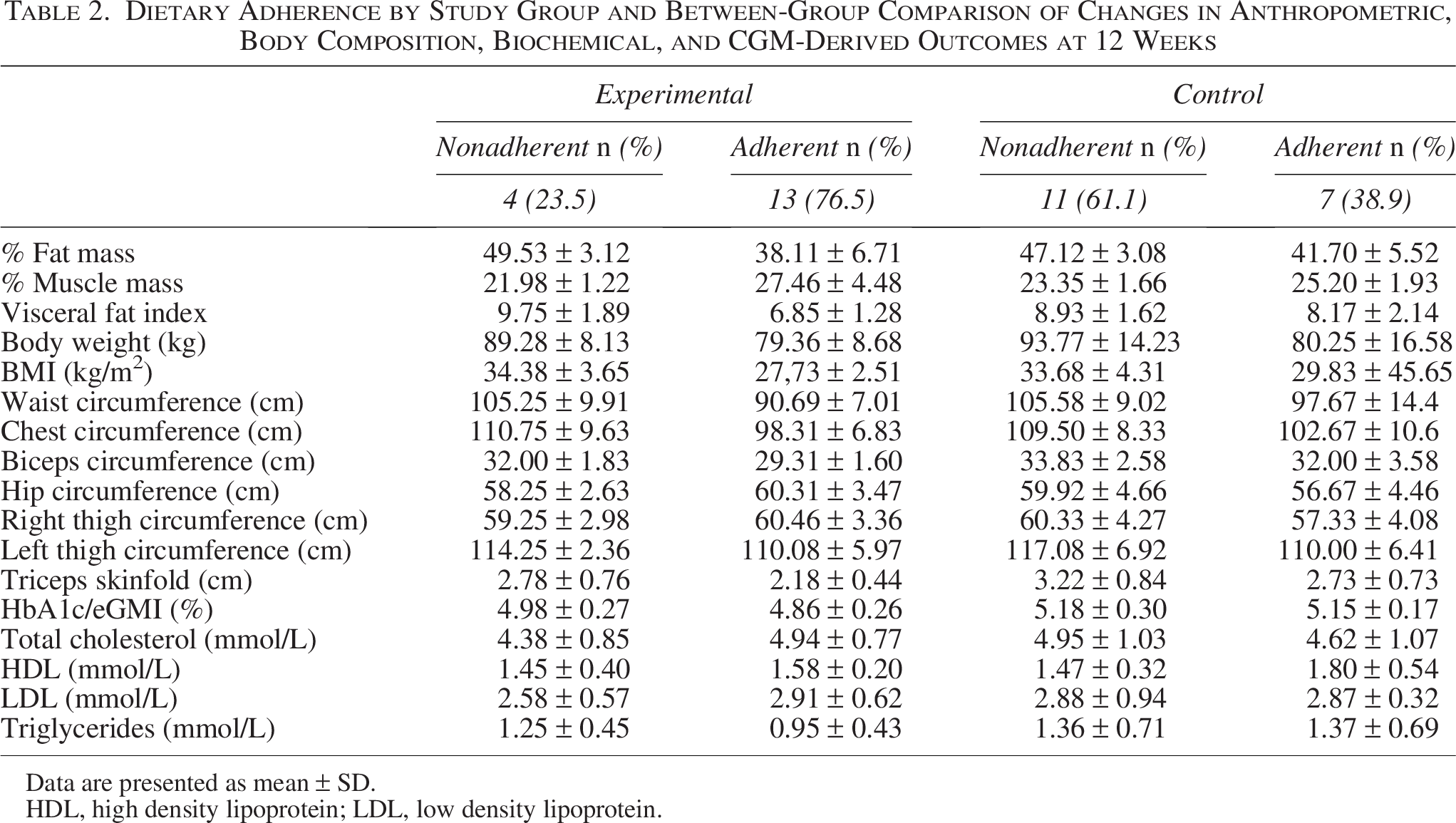
Data are presented as mean ± SD.
HDL, high density lipoprotein; LDL, low density lipoprotein.
Table 2 presents the comparative analysis of anthropometric, body composition, and biochemical parameters between participants who adhered to the prescribed dietary plan and those who did not, regardless of their original group assignment. A descriptive subgroup analysis was performed to explore differences in outcomes between participants who adhered to the prescribed diet and those who did not, within each study group. No inferential statistical comparisons between adherence categories across the entire trial were performed.
Anthropometric and body composition outcomes
After 12 weeks, participants in the isCGM group demonstrated significantly greater reductions in key anthropometric parameters compared with controls as follows (Fig. 2): body weight: −5.5 ± 2.3 kg versus −0.2 ± 1.8 kg (P < 0.001; Cohen’s d = 0.88); BMI: −1.9 ± 0.6 kg/m2 versus −0.1 ± 0.4 kg/m2 (P < 0.001); waist-to-height ratio: significant reduction (P < 0.001); waist circumference: −10.8 ± 5.1 cm versus −1.9 ± 4.3 cm (P < 0.001); body fat (%): −3.2 ± 1.8% versus −0.4 ± 1.3% (P < 0.01); visceral fat index: −1.8 ± 0.9 versus −0.3 ± 0.8 (P < 0.01); muscle mass (%): +2.4 ± 1.1% versus +0.1 ± 0.8% (P < 0.05). No significant differences were found in WHR between groups (P = 0.39). Reductions in limb circumferences were all greater for the experimental group (P < 0.001).
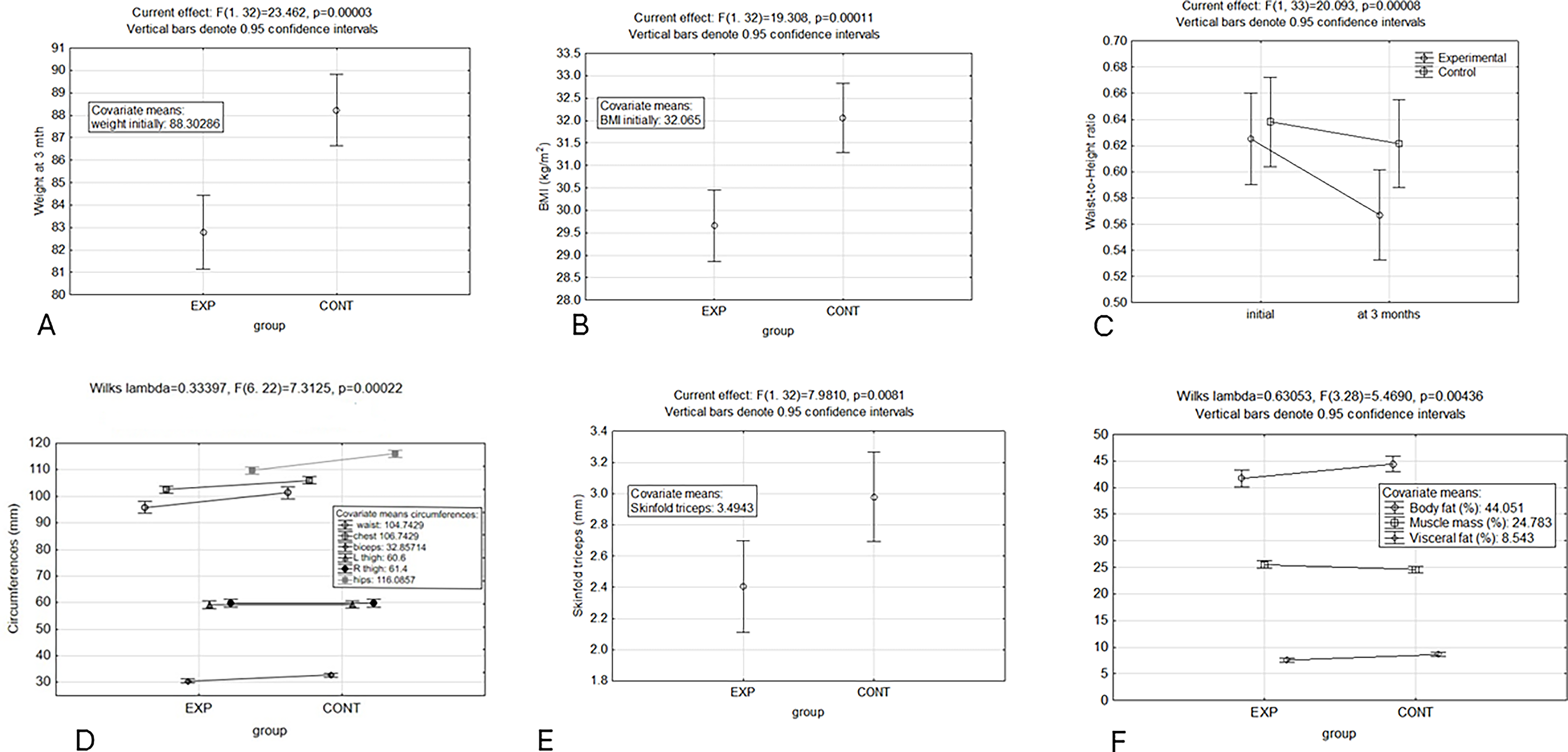
Mean changes
Laboratory findings
Both groups maintained normal fasting glucose and lipid profiles throughout the intervention. However, a trend toward HbA1c reduction was observed in the intervention group (−0.10 ± 0.05% vs. −0.01 ± 0.04%; P = 0.061; Fig. 3), suggesting early metabolic improvement even in normoglycemic individuals. No significant between-group differences were detected for total cholesterol, LDL, HDL, triglycerides, or fasting glucose levels (P > 0.1 for all).
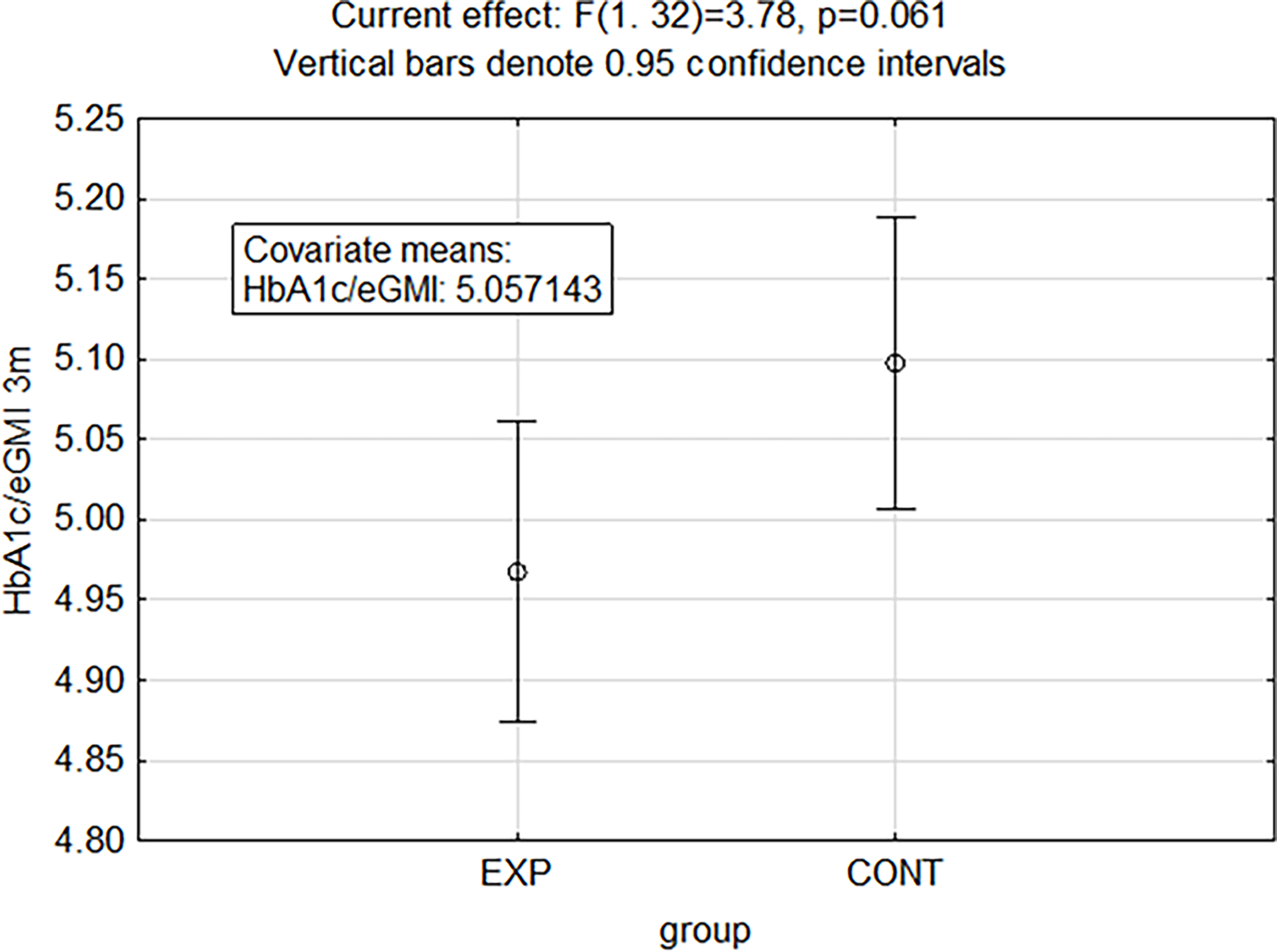
Change in glycated hemoglobin (HbA1c) after 12 weeks. A trend toward greater HbA1c reduction was observed in the intervention group compared with controls (P = 0.061; independent-samples t-test). Data are mean ± SD.
CGM metrics
Detailed changes in CGM-derived metrics are presented in Table 3. Compared to controls, the intervention group demonstrated a modest but significant improvement in TIR, specifically: ΔTIR: +1.8 ± 1.1% vs. +0.2 ± 0.9% (P = 0.03), Mann–Whitney U test; ΔTBR: −0.3 ± 0.2% vs. +0.1 ± 0.3% (P = 0.12); Δcoefficient of variation: nonsignificant between groups (P = 0.78).
Between-Group Differences in CGM-Derived Metrics

Data are presented as mean ± SD.
P values were calculated using the Mann–Whitney U test.
Composite outcomes
The morphology composite score, integrating percentage changes in body weight, BMI, body fat, visceral fat, and muscle mass, was significantly higher in the intervention group (P = 0.006; Fig. 4A), while the CGM metrics composite score (composed of changes in TIR, CV, and mean glucose) showed a positive but nonsignificant difference (P = 0.14; Fig. 4B).
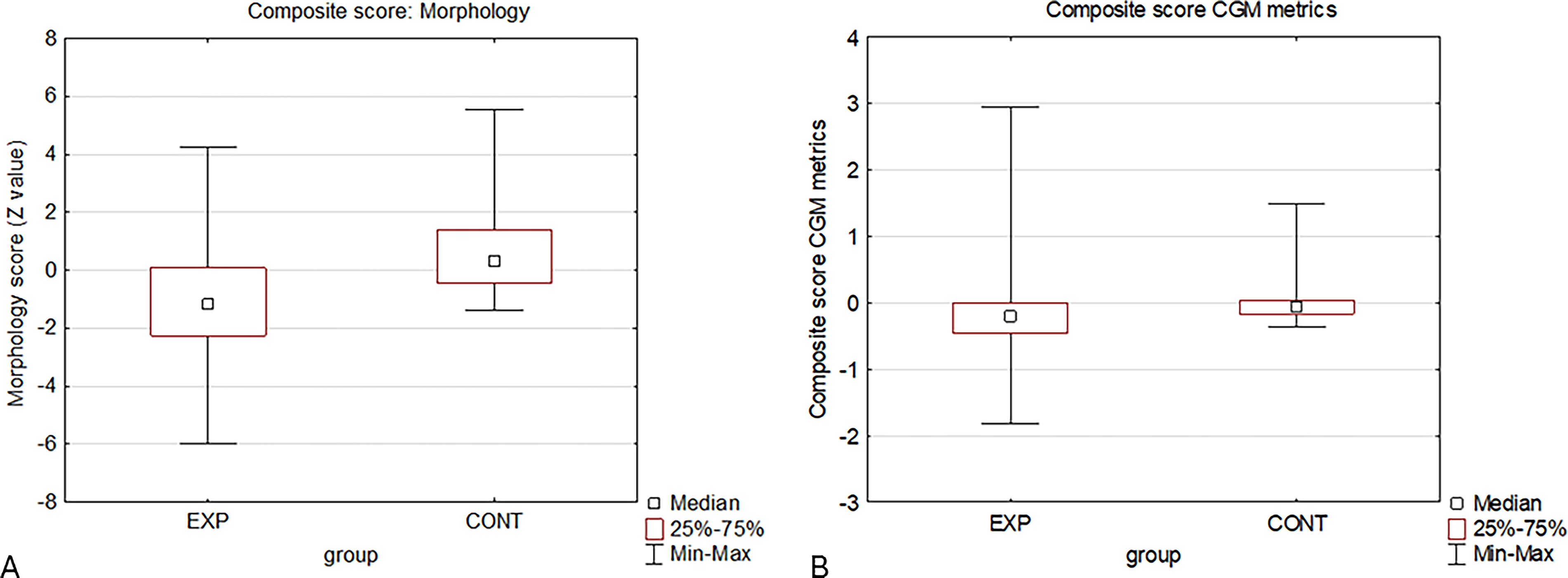
Comparison of composite morphology outcome scores between intervention and control groups. The composite score was derived from standardized changes in body weight, BMI, fat mass, visceral fat, and muscle mass. The intervention group achieved significantly higher composite scores (P = 0.006; independent-samples t-test)
Clinically meaningful improvements (≥3% reduction in both BMI and body fat) were achieved by 35% of participants in the intervention group versus 0% in the control group. Moreover, 53% of intervention participants met at least one success criterion (morphological composite outcome or increase in TIR ≥ 1%) compared with 11% in the control group (P < 0.001, chi-square; Fig. 5). Mentioned exploratory success outcome was developed specifically for this trial. The ≥3% reduction thresholds were selected based on evidence that 3%–5% reductions in adiposity are associated with metabolic and cardiovascular benefits in lifestyle interventions, while an increase in TIR ≥ 1% represented a CGM metric reflecting improvement in glycemic stability.
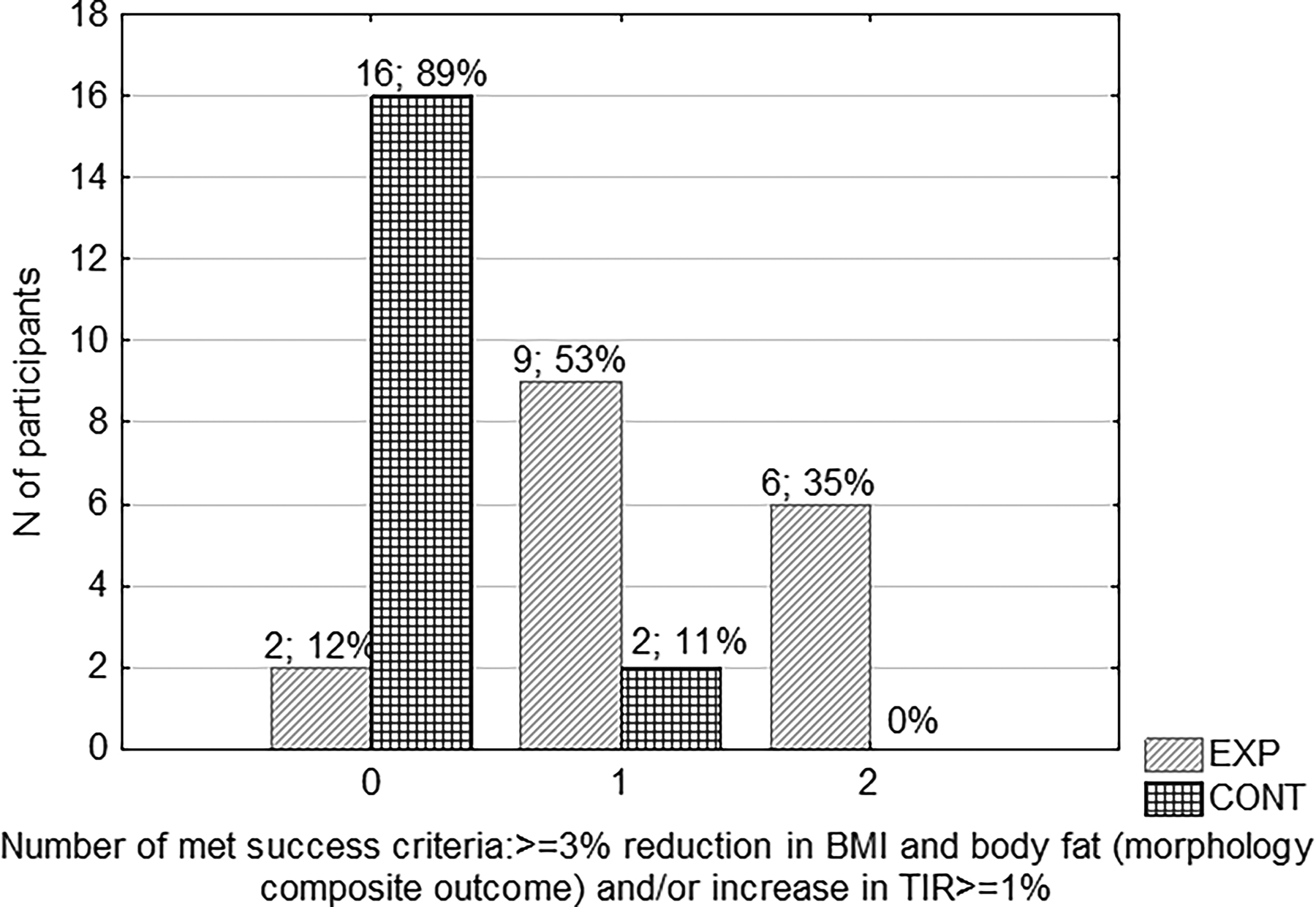
Proportion of participants achieving predefined success criteria: ≥3% reduction in both BMI and body fat (morphological success) or ≥1% increase in TIR (CGM success). A significantly higher proportion of participants in the intervention group met at least one success criteria (P < 0.001; chi-square test).
Discussion
This randomized controlled trial demonstrates that integrating intermittently scanned CGM (isCGM) into a structured 12-week lifestyle intervention significantly enhances weight loss, body composition, and dietary adherence in women living with obesity. Participants using isCGM achieved a mean body weight reduction of 5.5 kg compared with minimal change in controls, alongside greater decreases in BMI, waist circumference, body fat, and visceral adiposity. Muscle mass increased significantly, and dietary adherence was nearly doubled among participants receiving mid-program isCGM feedback. Furthermore, modest but meaningful improvements in TIR were observed, suggesting enhanced metabolic stability even in normoglycemic individuals. At the same time, the use of a ≥1% TIR improvement threshold should be interpreted cautiously and was intended as an exploratory marker in a normoglycemic population with minimal baseline variability. Nonetheless, these findings support the utility of isCGM as a behavioral and motivational adjunct to lifestyle therapy in obesity management.
Our findings align with growing evidence that CGM-based feedback can improve adherence and weight outcomes. Kitazawa et al. demonstrated that combining smartphone-based lifestyle counseling with isCGM in adults at high risk for diabetes led to significant reductions in body weight and improvements in self-regulation behaviors. 11 Similarly, Chekima et al. 13 reported that integrating real-time CGM with a low glycemic index diet improved body composition and metabolic parameters in overweight adults. In line with these studies, our results extend this evidence to a distinct population—women with obesity but without dysglycemia—showing that periodic isCGM use can reinforce behavioral change and produce clinically meaningful reductions in adiposity. 13
In contrast to previous work primarily focused on glycemic outcomes, this study emphasizes the behavioral feedback mechanism of isCGM. Earlier reviews (Amoh et al., 2025; Klonoff et al., 2023) proposed that CGMs’ real-time visualization of glucose fluctuations can empower individuals to recognize physiological responses to dietary intake and physical activity.9,12 Our data support this concept: participants exposed to continuous glucose trends more frequently demonstrated higher adherence to dietary recommendations and achieved superior weight and fat loss, suggesting that self-monitoring fosters accountability and intrinsic motivation, key determinants of long-term lifestyle success.
Importantly, our findings highlight that adherence to the nutritional component of the intervention was a strong determinant of overall success, irrespective of group allocation. Participants who demonstrated higher adherence achieved substantially greater reductions in body weight, BMI, and both total and visceral fat, while concurrently preserving or even increasing muscle mass. These results emphasize that consistent compliance with dietary recommendations exerts a more powerful influence on body composition improvements than group assignment alone. This observation aligns with prior evidence identifying dietary adherence as the principal predictor of successful weight loss across a range of intervention models. 14 The preservation of lean mass among adherent participants further suggests that sustainable adherence may promote better metabolic efficiency and protect against sarcopenic adaptations during caloric restriction.15,16 The observed improvements in TIR and reductions in TBR among the isCGM group may indicate greater metabolic flexibility and stabilized glycemic responses to meals. Even subtle glucose variability within normoglycemic ranges has been associated with appetite dysregulation and compensatory eating behaviors (Kishimoto & Ohashi, 2022). 17 By providing immediate visual feedback, isCGM likely mitigates these fluctuations, helping participants recognize and adjust dietary triggers that produce postprandial spikes or dips. Additionally, minimizing subclinical hypoglycemic episodes may reduce cravings and energy dips that undermine adherence to calorie-restricted diets. Collectively, these physiological and behavioral adaptations may underpin the improved body composition outcomes observed.
The increase in muscle mass, despite significant fat loss, is clinically relevant. Preservation or gain of lean tissue during weight reduction improves resting metabolic rate and supports sustained energy balance. 18 This finding underscores the value of combining supervised resistance training with dietary modification and technology-based self-monitoring—an integrated model consistent with contemporary recommendations for obesity treatment. 7
These findings carry important implications for early obesity management, particularly within the framework of the updated European definition distinguishing preclinical and clinical obesity. 3 In preclinical obesity—characterized by excess adiposity without overt metabolic dysfunction—behavioral interventions have the greatest potential to reverse disease progression. Incorporating isCGM into such programs offers a nonpharmacologic, data-driven strategy to enhance adherence and promote metabolic awareness before comorbidities emerge.
From a public health perspective, isCGM-assisted interventions could be scaled through digital platforms, enabling remote feedback and self-guided learning. Prior studies suggest that combining CGM with telemonitoring or app-based support further strengthens adherence and engagement. 10 Implementing such hybrid models in primary care or community weight management settings may improve outcomes while minimizing costs associated with pharmacotherapy or late-stage obesity complications.19–21
The study’s strengths include its randomized controlled design, high adherence to the intervention (>90%), and integration of objective outcome measures—body composition via bioimpedance, glycemic variability via isCGM, and adherence assessment. The inclusion of women without dysglycemia highlights isCGM’s potential role in preventive care, expanding its application beyond diabetes management.
However, several limitations should be acknowledged. The sample size was modest (n = 35), limiting statistical power for secondary outcomes and generalizability. The 12-week duration precludes conclusions on long-term weight maintenance or metabolic adaptation. Dietary adherence was self-reported, introducing potential recall bias; future studies should incorporate objective dietary tracking tools or biomarkers. Additionally, the open-label design may have introduced performance bias, as awareness of isCGM use could itself increase motivation. The exclusion of men limits the generalizability of our findings. Sex-related differences in metabolic responses and behavioral adaptations to CGM feedback warrant future studies that include both sexes. Despite these limitations, effect sizes for primary outcomes were large (Cohen’s d = 0.88), supporting the robustness of the findings.
The magnitude of weight and body composition changes observed with intermittent isCGM use was greater than anticipated. Although detailed meal-by-meal CGM-linked behavioral data were not collected, several mechanisms may explain this effect. Visual feedback on glucose excursions likely enhanced dietary self-regulation, reinforced meal timing awareness, and reduced consumption of foods associated with postprandial spikes. Improved glycemic stability may also have reduced appetite variability and cravings, indirectly supporting sustained caloric adherence. These behavioral mechanisms warrant further investigation using real-time dietary logging and qualitative assessments.
Indeed, further research should investigate the sustainability of isCGM-facilitated weight loss and whether continued or intermittent use yields long-term behavioral change. Larger multicenter trials across diverse populations, including men and individuals with comorbidities, are warranted. Future studies may also explore integration with digital health platforms, leveraging real-time feedback, gamification, and personalized coaching to maximize adherence and scalability. Cost-effectiveness analyses will be essential to determine the feasibility of incorporating isCGM into routine obesity care.
Conclusion
In summary, the addition of intermittently scanned CGM to a structured lifestyle intervention significantly improved adherence, body composition, and metabolic stability in women living with obesity. By combining behavioral reinforcement with objective feedback, isCGM may represent a valuable adjunct for early-stage obesity management. These results highlight the promise of personalized, technology-enabled strategies to enhance lifestyle modification and prevent progression to metabolic disease.
Authors’ Contributions
M.G. and M.C.B. conceptualized the study; I.O. and G.T. collected the data and participated in the execution of protocol; M.C.B., I.B.-C., V.C., L.R., and S.C.V. analyzed the data; I.B.-C. and M.C.B. drafted the article and wrote the final version; all authors read and agreed upon the final version.
Footnotes
Acknowledgments
The authors would like to thank the nutritionist, Tea Premoša Bašek, for creating personalized meal plans and for providing valuable dietary advice to the participants during the course of the study. Moreover, the authors are thankful to participants for their adherence to the study protocol.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
The authors received no funding for their work.