
Abstract
Objective:
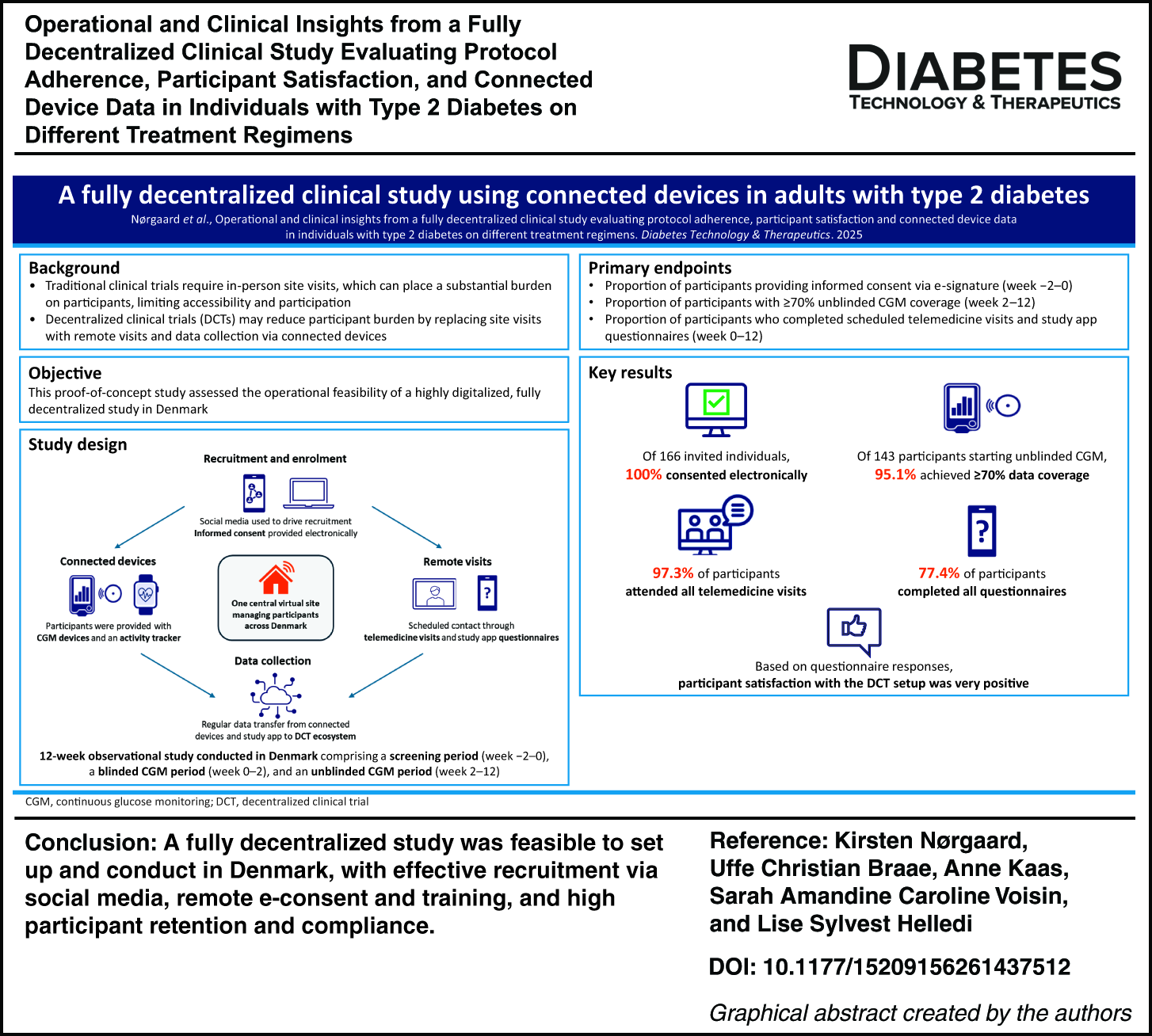
Traditional clinical trials place a substantial burden on participants owing to the need for frequent, tightly controlled site visits, which can limit access and participation. Advances in digital health allow for decentralized clinical trials (DCTs), with site visits replaced by virtual contact and data collection, potentially reducing burden and broadening access. This proof-of-concept study assessed the operational feasibility of a fully remote, digitalized DCT.
Methods:
This was a 12-week observational study conducted in Denmark; adults with type 2 diabetes were recruited via social media. Following e-consent, participants were provided with continuous glucose monitoring (CGM) devices and an activity tracker, with data collected via smartphone apps. All visits and support were conducted remotely. Primary endpoints were: proportion consenting via e-signature (weeks −2 to 0), proportion with ≥ 70% unblinded CGM coverage (weeks 2–12), and percentage of scheduled telemedicine visits and questionnaires completed (weeks 0–12). Safety was monitored remotely through adverse event (AE) reporting during telemedicine visits.
Results:
Most study places were filled within 2 days of advertisement. Of 166 invited individuals, 100% consented electronically; 156 were enrolled, and 87% completed the study. Among participants starting unblinded CGM, 95% achieved ≥70% data coverage, meeting international completeness standards. Adherence to remote interactions was high: 97% attended all telemedicine visits, and 77% completed all questionnaires; 72% completed all scheduled remote interactions. Satisfaction with the study and CGM devices was very high, although adherence to the activity tracker was low (12% with ≥70% coverage) owing to technical issues. Safety monitoring via remote AE reporting revealed no unexpected findings.
Conclusions:
A fully remote study was feasible to set up and conduct in Denmark, with rapid recruitment, high retention, and high compliance with CGM and telemedicine visits. DCTs have the potential to reduce participant burden, improve recruitment, and increase the representativeness of clinical trial populations.
Keywords
Introduction
The traditional format of clinical trials imposes a significant inconvenience on study participants to travel and attend multiple in-person visits. Consequently, attracting participants and maintaining engagement throughout a trial can be challenging. In addition, potential eligible participants could be excluded because they live in remote areas or a far distance from study sites or because they have commitments that would make attending multiple study visits in-person difficult (e.g., childcare or work commitments). From an operational perspective, this format often necessitates multiple study sites, which need to be managed and staffed, adding to the cost and complexity of running a clinical study.
Decentralized clinical trials (DCTs) are defined as clinical studies where some or all trial-related activities (i.e., hybrid trials which incorporate some DCT elements or fully decentralized trials) are conducted at locations other than traditional clinical trial sites, enabling participation from participants’ homes or local healthcare facilities. 1 The primary operational objective of DCTs is to reduce the burden on participants by removing or minimizing the need for them to travel to study sites. 2 This increases convenience and allows the recruitment of individuals who would otherwise be unable to take part in a clinical trial. 3
Advances in digital health technologies, such as connected devices and app-based patient support solutions, now allow the collection of data remotely. This can increase the ease of participating in a clinical trial and could potentially improve recruitment and participant retention. 4,5 Moreover, these technological advances allow for the collection of more granular data, which can provide improved insight into disease understanding and treatment. It is expected that clinical endpoints will become increasingly digital in the future. 6
While still in their early stages, studies that incorporate DCT elements are expected to become more widely used in the future owing to several factors. 7 These include the increased feasibility of running fully decentralized or hybrid studies resulting from the advancement of technology and digitalization, the need for flexibility and increased accessibility for participants when taking part in clinical trials, increased flexibility in regulations for conducting clinical trials, and the need for increased operational efficiency.
This proof-of-concept study builds upon learnings from a small pilot study and assessed the operational feasibility of a full-scale DCT setup to conduct a fully remote, observational study including individuals with type 2 diabetes (T2D) who were residents in Denmark. 8 The study used telemedicine visits and connected devices, namely a continuous glucose monitoring (CGM) device and an activity tracker (heart rate-enabled smartwatch) for the remote collection of data via associated apps. In addition, this study aimed to explore characteristics of the CGM-based glucose profiles obtained from participants, evaluate participant satisfaction with the overall study design, remote interactions, and connected devices, and gauge participant adherence to wearing a CGM device and an activity tracker for remote collection of data.
Materials and Methods
Study design and participant recruitment
This was an observational study with a fully DCT setup conducted remotely between April 30, 2024, and January 7, 2025, in Denmark (ClinicalTrials.gov: NCT04809311). The study duration for each participant was 14 weeks, which comprised a 2-week screening period and a 12-week data collection period. The study design is presented in Supplementary Figure S1.
Eligible participants were adults (aged ≥ 18 years) with a diagnosis of T2D for more than 3 months prior to signing the informed consent. Participants who did not have a blood glucose meter at home were excluded from participating in the study. This was to ensure that participants understood their blood glucose levels and the implications of those levels, as well as having the ability to monitor their blood glucose in case of low sensor glucose values. The full inclusion and exclusion criteria are presented in Supplementary Table S1. Study participants with T2D were recruited via social media advertisements (Facebook and Instagram) that linked to the study landing page.
Site model and research visits
One virtual central site was established for the study; all study staff were hired for the study, and all worked remotely from their homes except for the study principal investigator who was based at the Steno Diabetes Center Copenhagen, Denmark. All study staff had regular online interactions with each other to ensure quality and consistency of information and of the support given to participants.
Regular remote interactions were scheduled throughout the study, including remote visits (RVs; online telemedicine/telehealth video calls between participants and study staff) and interactions with the study app (SAis), which consisted of the completion of online questionnaires for self-reporting in the study app. In total, four RVs at weeks −2, 0, 2, and 6 and four SAis at weeks 1, 4, 7, and 12 were scheduled during the study. An overview of the participant journey during the DCT is presented in Figure 1. Study staff were contactable between RVs to provide first-line technical support to participants, if required.
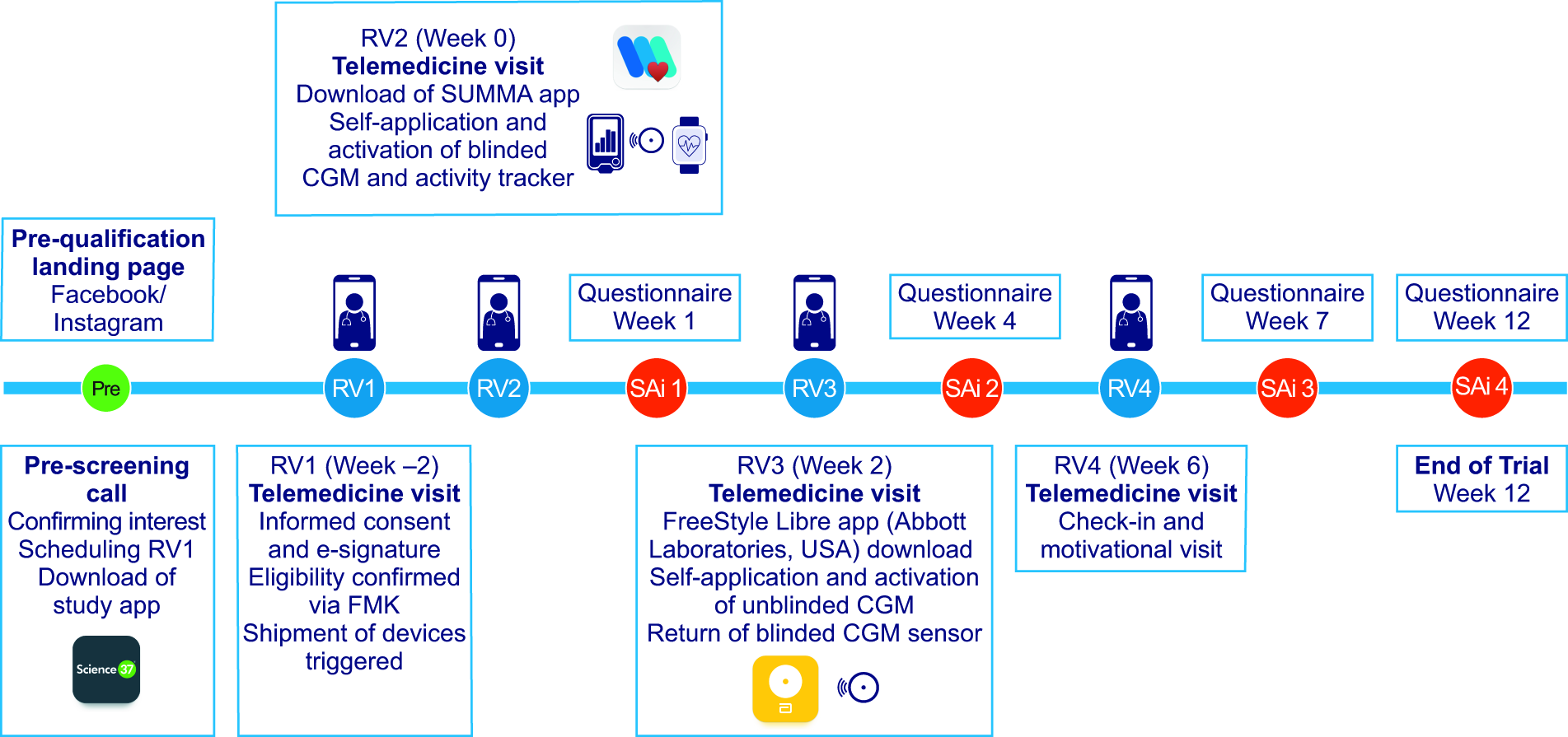
Participant journey timeline. CGM, continuous glucose monitoring; FMK, Fælles Medicinkort (Prescription database); RV, remote visit; SAi, study app interaction.
Study completers were defined as those participants who completed the final SAi at week 12, although the exact time span could vary slightly depending on the start date of the blinded CGM device and/or activity tracker (RV2), time of change to unblinded CGM device (RV3), and the date of the end of study interaction (SAi4).
Devices, apps, and measurements
During the remote visit at week −2 (RV1), participants received and were able to sign the informed consent form (either during or directly after the remote visit) via Adobe Sign using their MitID, which is a unique personal identifier and secure digital key for Danish residents to access various public and commercial self-service solutions. Signing the informed consent form included consenting that qualified medical personnel could access and independently verify the participants’ prescribed medication to confirm their eligibility through the Danish shared medication record Fælles Medicinkort (FMK). FMK is a national database containing up-to-date information on prescribed and dispensed medications for all Danish citizens.
Once individuals had provided e-consent for study participation and were confirmed to be eligible for the study by an investigator, participants were provided with a suite of study devices. Devices included one blinded CGM device (FreeStyle Libre Pro-IQ sensor and reader; Abbott Laboratories, USA), six unblinded CGM devices (five CGM sensors for the 10-week unblinded CGM period plus an additional sensor in case of issues) (FreeStyle Libre 2 CGM device; Abbott Laboratories, USA), and an activity tracker (Pulse HR smartwatch; Withings, France). Participants were asked to self-apply the devices and to wear them for approximately 12 weeks in total. CGM sensors for both the blinded and unblinded CGM devices had a 14-day wear period before requiring replacement with a new sensor by participants. As participants were naive to CGM use, they were provided with modified (blinded CGM) and commercial (unblinded CGM) training materials, both in paper form and electronically, detailing how to apply and use the CGM sensors and the accompanying FreeStyle Libre phone app. They were also provided with an additional concise document created by the PI, which explained time in range (TIR) in the context of CGM measurements and provided instructions on taking control measurements with a standard blood glucose meter. Last, participants were informed that any concerns regarding their CGM values should be discussed with their usual healthcare provider. Study staff acted as first-line technical support for participants and provided remote guidance during telemedicine visits on how to apply and activate the connected devices on first use.
Participants used their own smartphone and were required to download three apps to be used throughout the study: the Science 37 study app (Science 37, USA), which participants used to access the DCT platform (this enabled participants to enter their personal information and to access their informed consent information, training materials, the telemedicine visit video module, and study questionnaires); the FreeStyle LibreLink app (Abbott Laboratories, USA) for the unblinded CGM device; and the Precision Digital Health (PDH, USA) SUMMA mobile app, which displayed the data collected by the activity tracker.
CGM data were collected in two phases during the study: a 2-week blinded CGM period (measured using the FreeStyle Libre Pro-IQ) from weeks 0 to 2 and a 10-week unblinded CGM period (measured using the FreeStyle Libre 2) from weeks 2 to 12. The blinded CGM was activated by participants via a CGM reader device, which was subsequently shipped back, along with the blinded CGM sensor, by prepaid post to the central site after use for data extraction. The blinded CGM period was calculated from the time of the first blinded CGM measurement at RV2 (week 0) until the sensor stopped collecting data after 14 days or removal of the blinded CGM device. The unblinded CGM period was calculated from the time of the first unblinded CGM measurement at RV3 (week 2) until 10 weeks after this measurement. Time gaps of ≥15 min were classified as missing data, as 15 min is the normal reading interval for this device. The percentage of time spent in a given sensor glucose range was calculated as the number of glucose measurements within that range divided by the total number of measurements recorded during that period.
Throughout the study, data were collected through connected devices, by participants self-reporting via the study app, or by study staff entering data into the DCT platform. An overview of the data flow ecosystem is presented in Supplementary Figure S2.
Treatments
As the study was observational, no medications were provided to participants; participants continued their glucose-lowering treatment independently of this study and at their treating physician’s discretion, as per standard clinical practice. Participants were encouraged to contact their treating physician if they had any questions/concerns regarding their treatment.
Participants were allocated to one of three study groups according to their self-reported current glucose-lowering treatment, which was subsequently verified by an investigator via FMK: metformin ± other oral glucose-lowering medications (OGLMs), basal insulin ± OGLMs, or glucagon-like peptide-1 (GLP-1) ± basal insulin (loose and fixed combination) ± OGLMs. Participants were able to change their medication under the advisement of their treating physician during the study; this was recorded during RVs and was also verified via FMK at the end of the study. Participants who failed the screening criteria because they were receiving the wrong glucose-lowering medication were still invited to provide informed consent to enable verification of their glucose-lowering medications via FMK.
Endpoints
The primary endpoints included evaluation of the number of participants who were invited to consent and consented via e-signature (yes/no) during screening (weeks −2 to 0), the number of participants with at least 70% unblinded CGM data (yes/no) from the time of first unblinded CGM measurement until 10 weeks after, and the percentage of questionnaires and per-protocol planned RVs completed by participants from week 0 until the end of study (week 12). The screening visit (RV1) was not included in the total RV count.
Secondary endpoints included the percentage of time in range (TIR; 70–180 mg/dL [3.9–10.0 mmol/L]), time above range (TAR; >180 mg/dL [>10.0 mmol/L]), and time below range (TBR; <70 mg/dL [<3.9 mmol/L]) from the time of the first recorded unblinded CGM measurement until the last unblinded CGM measurement, mean blood glucose (mmol/L), mean glycemic variability (coefficient of variation [CV%] of glucose measurements) from the time of the first recorded unblinded CGM measurement until the last unblinded CGM measurement, and the number of participants with at least 70% heart rate (pulse) data (yes/no) from the time of the first heart rate measurement until 12 weeks after.
Additional assessments
Participant satisfaction with the study overall and specifically with the remote interactions (telemedicine visits), the use of CGM, and the use of the activity tracker was assessed with the distribution of scores from questionnaire responses for each question from SAi1, SAi2, SAi3, and SAi4 (scheduled at weeks 1, 4, 7, and 12, respectively) that were asked on a 5-point Likert scale and by assessing the median score. This was also assessed with the percentage of responses received for each multiple-answer question from SAi1, SAi2, SAi3, and SAi4.
Safety/adverse events
Safety was in accordance with pharmacovigilance for the marketed products being taken by participants and was monitored remotely through adverse event (AE) reporting during telemedicine visits or during unscheduled phone calls/help desk calls.
Study oversight
This study was conducted in accordance with the principles of the Declaration of Helsinki, 9 the guidelines for Good Pharmacoepidemiology Practices, 10 national regulations, and in accordance with relevant data privacy laws and internal requirements. The study protocol, any amendments, participant information/informed consent form, and any other written information to be provided to the participant and participant enrollment procedures were submitted, reviewed, and approved by an independent ethics committee (De Videnskabsetiske Komitéer for Region Hovedstaden, study number H-20036248) before the study was initiated. Written study information was available to the participant in electronic format, and participant informed consent was obtained before any study-related activity.
Statistical analysis
Descriptive statistics were used to describe all endpoints. No hypothesis testing or hypothesis generation was planned, and no formal comparison between treatment groups was performed.
Results
Participant recruitment and disposition
Participant recruitment via social media resulted in over 125,000 views of the study advert, which in turn resulted in over 22,000 landing page views (Fig. 2). Of the 2522 individuals who completed and submitted the pre-qualifying questionnaire, 770 passed the prequalifying questionnaire. However, not all 770 were invited to attend a prescreening call owing to the extreme interest in participating in the study. Within 2 days following the launch of study recruitment, 415 individuals had been signed up for study participation after passing prescreening questions. Consequently, advertisement of the study was stopped.
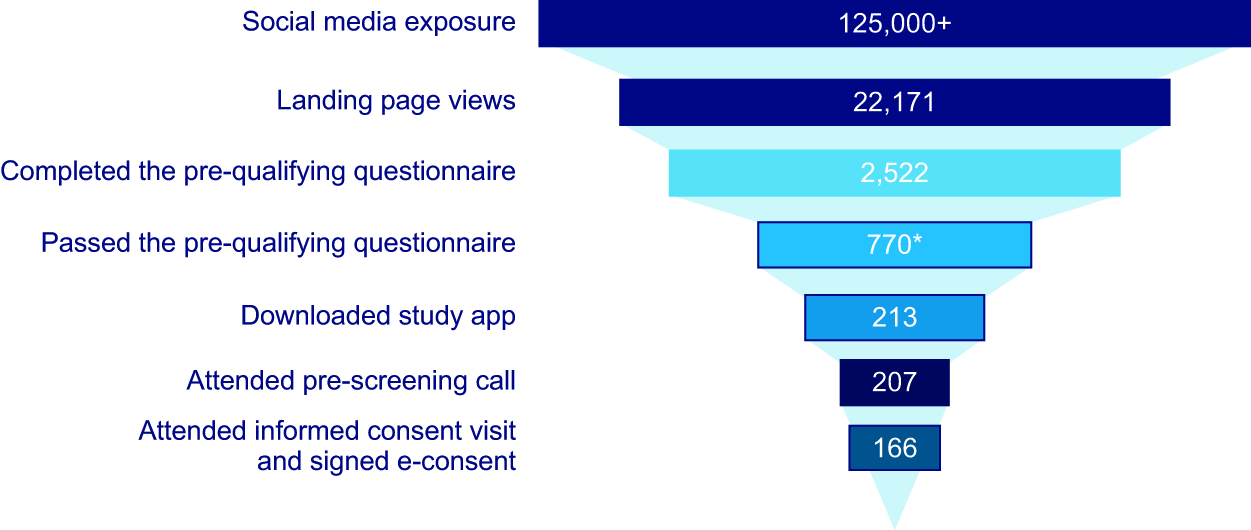
DCT study recruitment. *Owing to extreme interest in participating in the study, not all 770 participants were invited to a prescreening call. DCT, decentralized clinical trial.
With such high demand, mitigation actions were implemented to manage the expectations of potential participants in the form of information letters and the establishment of a waiting list. When it became apparent that most individuals who had been prescreened in the basal insulin group were also receiving treatment with GLP-1, recruitment was reopened specifically targeting users of basal insulin ± OGLMs only. This was done to demonstrate the feasibility of recruiting within a specific treatment regimen. All participants who were invited to attend the informed consent visit (RV1) were invited to sign the informed consent form via email; all provided informed consent via e-signatures.
Participant baseline characteristics and demographics
Baseline characteristics and demographics of the enrolled participants are shown in Table 1. A wide geographical distribution of participants who were residents across Denmark was recruited. The mean age of participants was 59.6 years, with a balanced sex distribution (male 50.6%, female 49.4%). The education level of included participants covered the whole range from primary school to long-term higher education, with medium-term higher education being the most common education level (29.5% of participants).
Participant Demographics and Baseline Characteristics
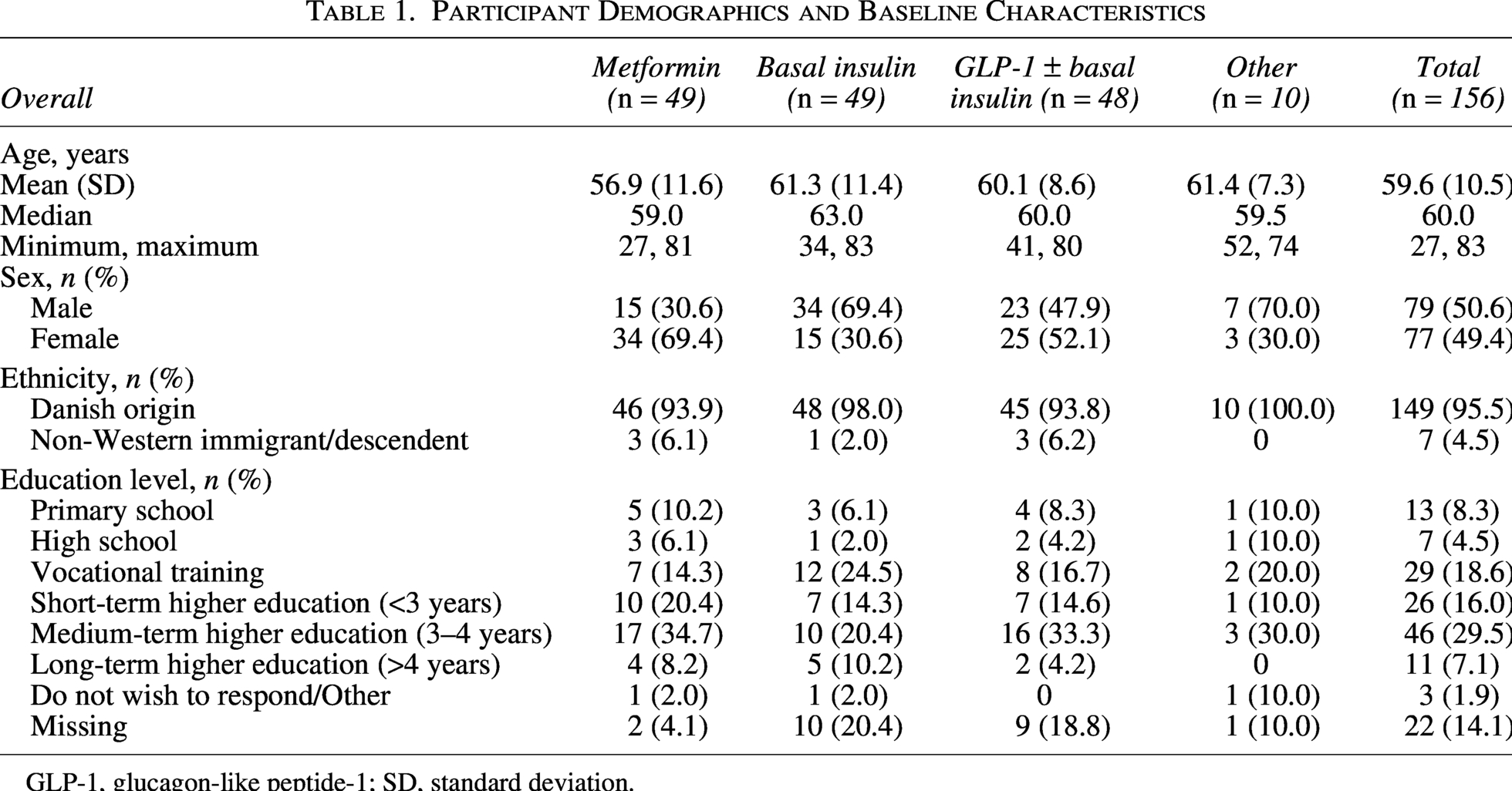
GLP-1, glucagon-like peptide-1; SD, standard deviation.
A small number of participants (n = 10) were receiving different medications than the three predefined treatment regimens and were allocated to another treatment group labeled as “Other.” Five participants were mistakenly enrolled because they did not fit into one of the predefined treatment groups; these participants were included in the “Other” group because they would contribute to the operational endpoints of the study and because the primary and secondary endpoints did not involve any comparison between treatment groups. Owing to a long period of time between the RV1 and RV2 telemedicine visits, an additional five participants changed their glucose-lowering medication that they were receiving at screening (RV1) from one that was in one of the three predefined treatment regimens to a glucose-lowering medication that was not. These participants were also included in the “Other” group; this enrollment was not considered to be a protocol deviation, as medication changes during the study were allowed.
Most participants continued with the same glucose-lowering medication that they were receiving at the time of screening until the end of the study. However, eight participants across all three predefined treatment groups did change their glucose-lowering medication over the course of the study (Supplementary Table S2).
Primary endpoints
Consent via e-signature
Of 166 individuals who were invited to provide informed consent electronically, 100% consented via e-signature. Of those 166 individuals, 156 were enrolled in the study; 10 individuals violated the eligibility criteria (eight did not meet the inclusion criteria as confirmed by study investigators, and two had hidden addresses, which prevented their names from appearing on the e-signature form). Out of the 156 enrolled participants, 146 (93.6%) attended the remote visit at week 0 (RV2), while 10 participants discontinued either before or at this visit and were subsequently excluded from the analysis. In total, 136 participants (87.2%) completed the study by completing SAi4 at week 12.
Engagement with remote interactions
Of the participants who continued with the study following the remote visit at week 0 (RV2), 97.3% attended all three of the per-protocol planned RVs (telemedicine visits), and 77.4% completed all four required SAi questionnaires (Fig. 3). In total, 72.4% of the study population (113 of 156 enrolled participants) completed all remote interactions (three RVs and four SAis).
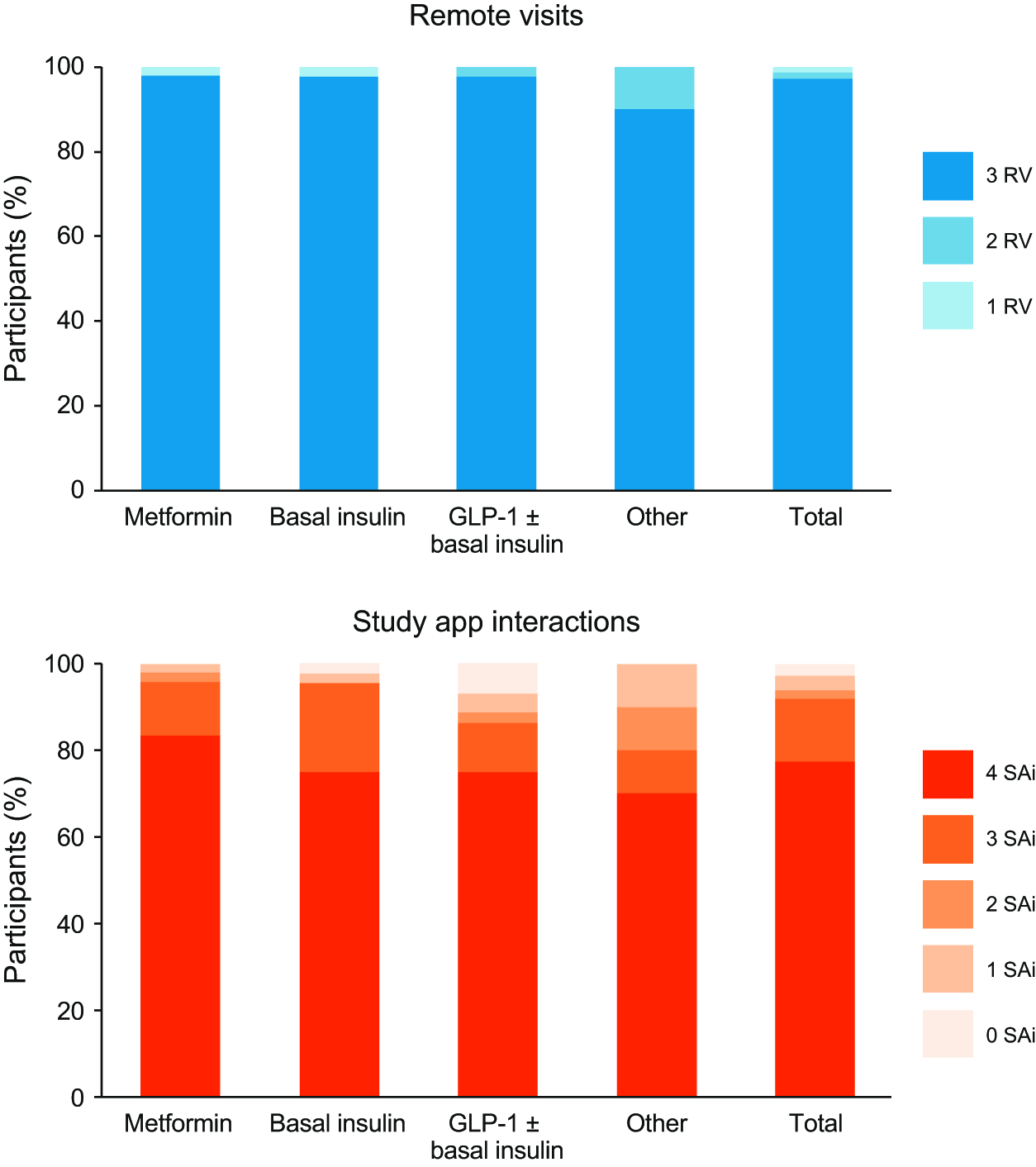
Participant engagement with remote interactions (remote visits [telemedicine visits] and study app interactions). GLP-1, glucagon-like peptide-1.
CGM coverage
All of the 146 participants who attended the remote visit at week 0 (RV2) were able to self-apply and activate the blinded CGM device. In total, 143 participants (97.9%) transitioned from a blinded to an unblinded CGM device during RV3 and were successfully able to download the associated study apps, create a user account, and self-apply and activate the unblinded CGM device. Of these participants, 131 (91%) adhered to the 13–16 days (2 weeks optimal) interval between device changes, indicating strong compliance with study procedures and the schedule between RV2 and RV3 (weeks 0–2).
Among the 143 participants who attended the remote visit at week 2 (RV3), there was high adherence to the unblinded CGM with 95.1% of participants providing at least 70% unblinded CGM coverage for the planned study duration, including seven participants (4.9%) who did not complete SAi4 (Fig. 4). This indicates that high CGM use adherence was maintained even among some participants who did not complete the final questionnaire (SAi4). Another seven participants (4.9%) completed the study but provided less than 70% unblinded CGM coverage. There were 13 participants who discontinued before or at RV3 (week 2) and were not included in these data. Overall, there were few data gaps, with 90.6% of unblinded CGM data collected. In the remaining 9.4% of missing, unblinded CGM data, 8.7% corresponded to data gaps of 0–24 h and 0.6% were data gaps of more than 24 h (Fig. 5).
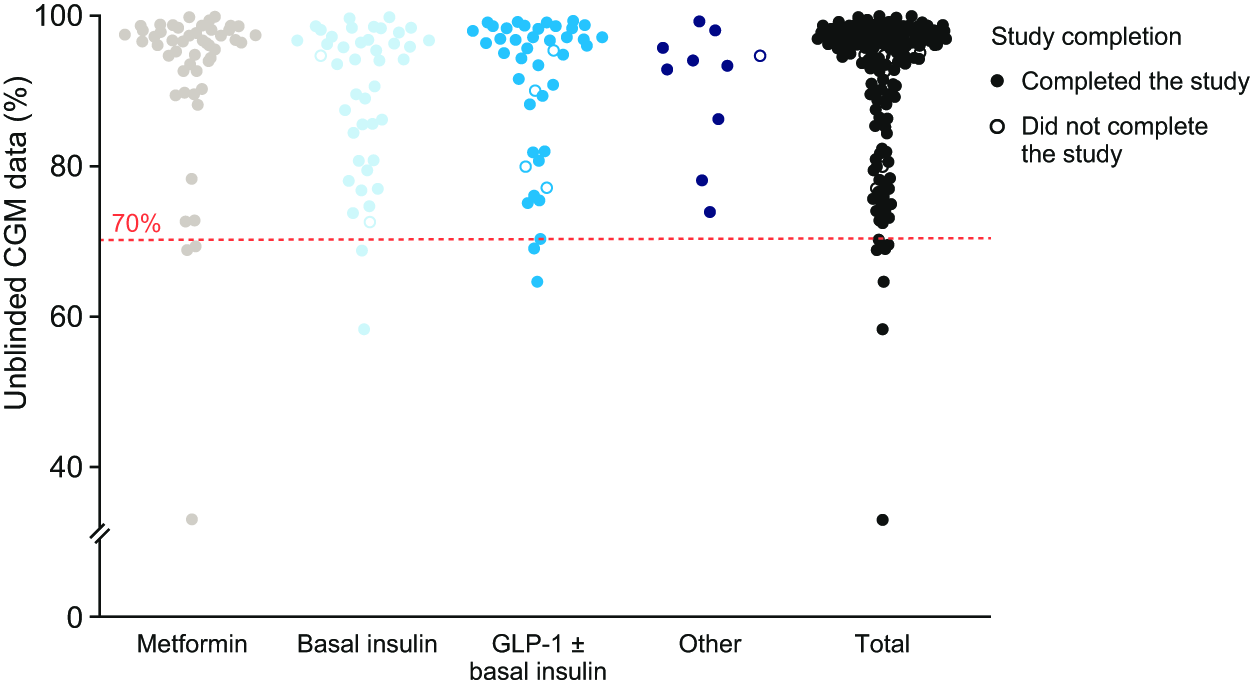
Participant CGM data availability during the unblinded CGM data collection period. CGM, continuous glucose monitoring.
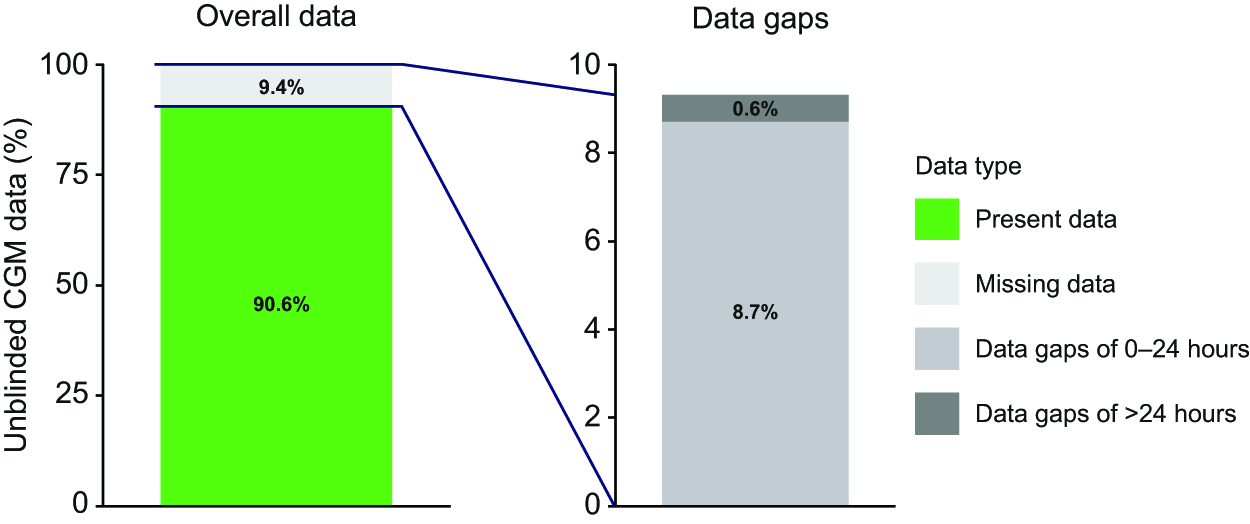
Total missing data and data gaps during the unblinded CGM data collection period. Proportion of present and missing data during the unblinded CGM data collection period. Values have been rounded to 1 decimal place.
Secondary endpoints
CGM data (TIR, TAR, and TBR), mean blood glucose, and glycemic variability
During the blinded CGM data collection period (weeks 0–2), the mean percentage of TIR was 78.4%, TAR was 19.9%, and TBR was 1.7%, while during the unblinded CGM collection period (week 2–12), for the total study population, the mean percentage of TIR was 83.2%, TAR was 15.7%, and TBR was 1.1% (Fig. 6). During the unblinded period, the mean (SD) glucose measurement was 139 (40) mg/dL (7.7 [2.2] mmol/L), with a CV of 24.0% (6.5%). Mean sensor glucose during the unblinded CGM collection period was 123 mg/dL (6.8 mmol/L) for participants in the metformin group, 162 mg/dL (9.0 mmol/L) for participants in the basal insulin group, and 125 mg/dL (6.9 mmol/L) for participants in the GLP-1 ± basal insulin group. Glycemic variability (CV) during the unblinded CGM collection period was 20.8% for participants in the metformin group, 28.0% for participants in the basal insulin group, and 22.8% for participants in the GLP-1 ± basal insulin group.
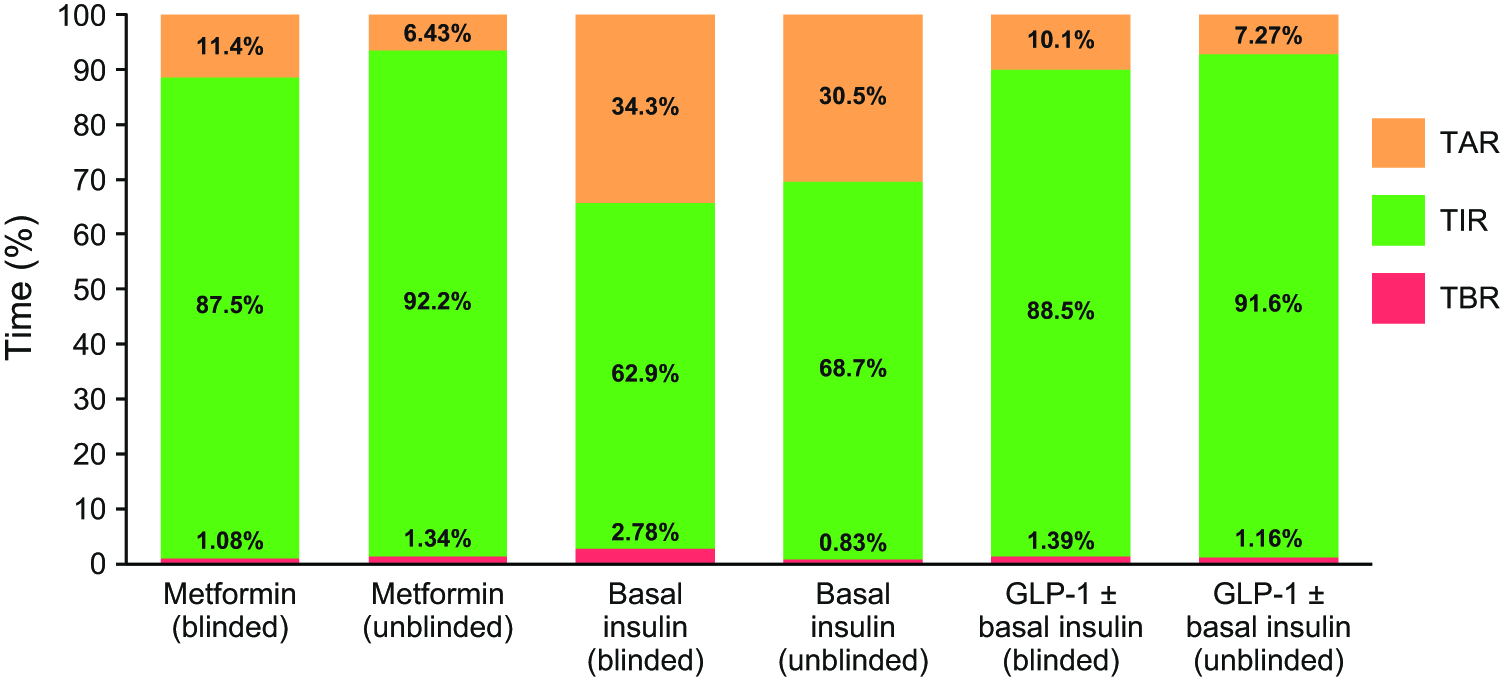
Participant CGM-based metrics during the blinded and unblinded data collection periods. CV, coefficient of variation; TAR, time above range (>180 mg/dL [>10.0 mmol/L]); TBR, time below range (<70 mg/dL [<3.9 mmol/L]), TIR, time in range (70–180 mg/dL [3.9–10.0 mmol/L]).
Participants with at least 70% heart rate (pulse) data
Of the 146 participants who attended RV2 (week 0), only 17 (11.6%) provided heart rate data for at least 70% of the planned duration of the study due to technical issues with the activity tracker, skin irritation caused by the activity tracker wristband, and data setup (Supplementary Table S3).
Safety/adverse events
A total of 13 AEs were reported in 12 participants; 11 AEs resolved with minor sequelae (Supplementary Table S4). Most AEs (n = 11) were related to skin irritation caused by the activity tracker wristband. No serious AEs or deaths were reported during the study.
Additional outcomes
Overall, based on responses to the SAi questionnaires, participant satisfaction with the DCT study was very positive (Fig. 7), with >90% of participants indicating that they were pleased to be able to access all of the study information on their smartphones and agreed that their interactions with study staff were positive, despite not having physical in-person visits. In general, participants reported a high level of satisfaction with the remote interactions that they had with study staff, with most indicating that they did not require more RVs with the study staff (Supplementary Fig. S3). Participant satisfaction with the CGM devices was predominantly positive (Supplementary Fig. S4), with most participants indicating that they were able to attach the glucose monitor to their upper arm with ease and understand their blood glucose readings displayed in the FreeStyle LibreLink app. In comparison, participant satisfaction with the activity tracker was less positive (Supplementary Fig. S5), with participant feedback indicating that this was likely owing to issues with the setup of the activity tracker and issues with data synchronization.
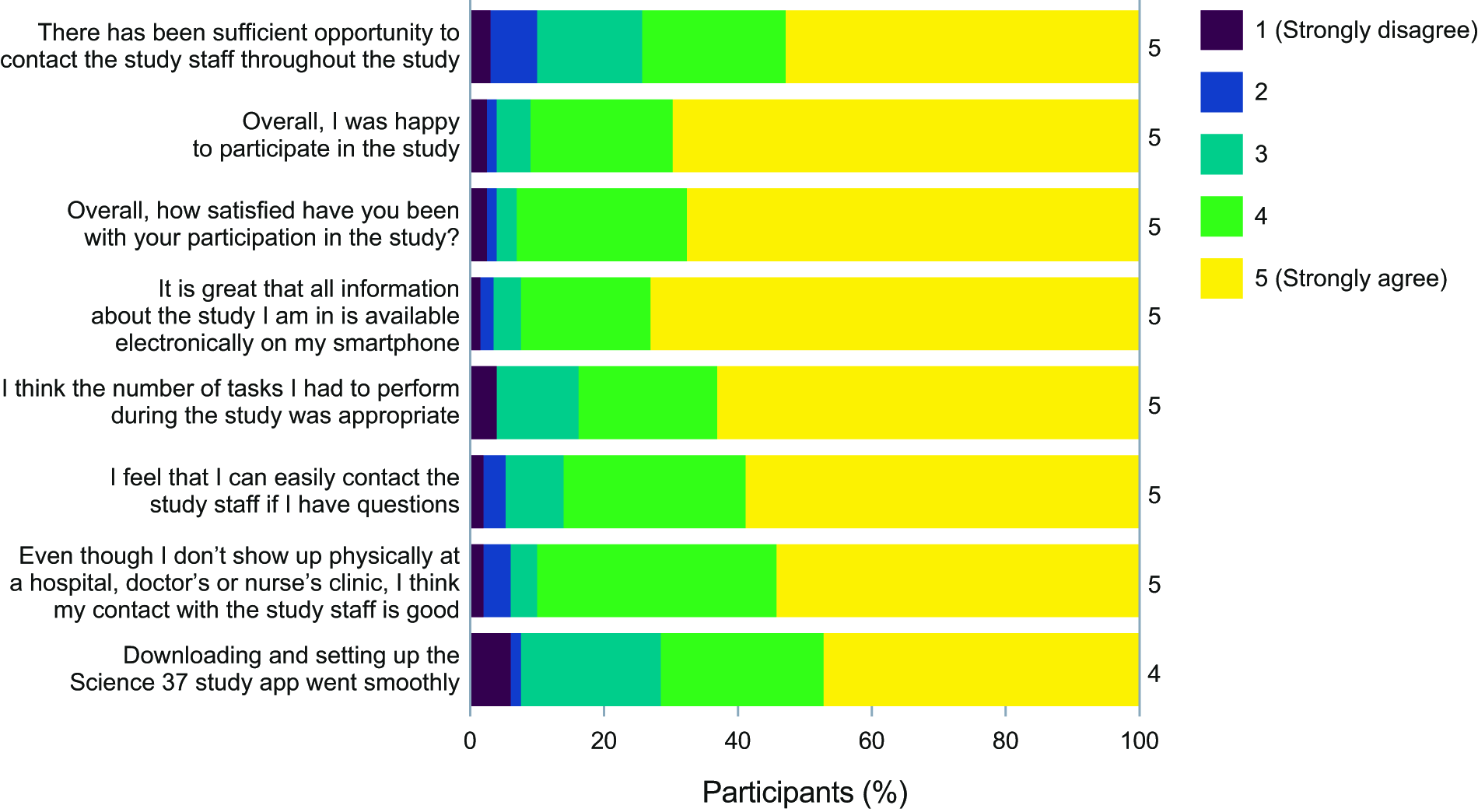
Participant responses to questions related to overall satisfaction with the study. Responses to questions from all four SAis were pooled together and grouped by topic (overall study, remote interactions, CGM, and activity tracker). The figure displays answers to questions asked on a Likert scale, and the numbers on the right-hand side of the bars show the median score. SAi, study app interaction.
Discussion
This observational study investigated the feasibility of setting up and conducting a fully decentralized study in adults with T2D in Denmark. Participant recruitment via social media was rapid and effective, leading to an overabundance of people signing up to participate in the study. Furthermore, obtaining informed consent electronically worked well, with 100% of invited participants providing consent via e-signature during screening. It was also possible to enroll participants from all parts of Denmark, including those who lived far from clinical sites or those who had work or childcare commitments. Providing multiple devices and apps to participants was feasible, although it required guidance from study staff and user-friendly introductory materials and guides. However, while participation in remote interactions and participants’ compliance with scheduled visits, completion of questionnaires, and adherence to CGM use were high, this was not the case with the activity tracker, most likely owing to technical issues experienced by participants.
Participant retention throughout the study was high, and participants were overall happy and satisfied with participating in the study. Having only RVs (telemedicine visits) was not an issue; participant satisfaction was not negatively affected by this, and participants developed a trusting relationship with study staff despite interactions only taking place remotely.
The main driver for participants to enroll in this study was not only the remote aspect but also the possibility to obtain a CGM device, which is not routinely provided to people living with T2D in Denmark. Most participants indicated via the SAi questionnaires that they were very satisfied with having continuous insight into their own glycemic data via the unblinded CGM and associated app. Considering this, offering a CGM device could be a compelling enrollment incentive for participants, with the potential to drive active participation and retention in future studies.
These results demonstrate that it is possible for study participants to download apps, create digital user accounts, and self-apply and activate CGM devices in a remote setting. More specifically, it was possible to obtain CGM data remotely with high data integrity; good adherence and compliance and few data gaps were observed during both the blinded and unblinded data collection periods, and particularly during the transition between these two periods of the study (RV2 to RV3). Newer CGM devices have real-time streaming capabilities and extended “backfill” capabilities (during a temporary disconnection between a CGM device and a phone/receiver, measurements continue to be recorded and stored, which are then transmitted and updated once the connection has been restored; in this way, no CGM data are lost during periods of disconnection) that would be expected to further reduce data gaps during unblinded CGM use.
Adherence to CGM use was high, with most participants meeting international data-completeness standards (≥70% coverage over ≥ 14 days). 11 These thresholds are widely accepted for the confident interpretation of CGM metrics and for predicting longer-term glycemic outcomes. 11 Meeting these standards in a fully remote setting supports the robustness of the glycemic findings and demonstrates the feasibility of achieving high CGM engagement without in-person contact.
Participant satisfaction with the activity tracker was in direct contrast to the CGM devices; only 11.6% of participants provided heart rate data for at least 70% of the planned study duration owing to technical issues. User satisfaction with the activity tracker was low, caused by setup and synchronization issues, partly because an older version of the activity tracker was used (compared with the latest models with more up-to-date features and capabilities) and partly because the PDH SUMMA app setup did not work seamlessly. Additionally, some participants reported skin irritation caused by the activity tracker wristband. These findings suggest that all devices used should be user-friendly and up-to-date, with user comfort and experience as a key consideration when planning a DCT or hybrid study. Furthermore, the technical setup and integration should be robust and thoroughly tested as much as possible prior to study launch. In this study, unforeseen technical difficulties were encountered despite rigorous testing.
No serious AEs occurred, and no safety concerns related to the DCT setup were identified during the conduct of the study. Most AEs reported were minor (e.g., skin irritation from the activity tracker wristband) and resolved with minimal intervention.
Despite demonstrating the operational feasibility and quality of data collected throughout the study, significant challenges were encountered, which warrant discussion. Most protocol deviations that occurred during the study (24 of 41 total protocol deviations) were owing to expired blinded CGM sensors. This was caused by a longer than protocol-defined time between the remote visit at week −2 (RV1, the completion of which triggered the shipment of devices to participants) and the remote visit at week 0 (RV2), which also meant that several RV2 visits needed to be rescheduled. Factors contributing towards these delays included participants’ summer vacations, staff shortages, or overload, resulting in an extended enrollment time. Expired CGM sensors were not used during the study, and new sensors were shipped to participants.
There was a steep learning curve for site staff who had not participated in a full DCT study setup before. It became clear that the number of site staff that had been recruited was insufficient to keep pace with the enrollment plan, especially in the beginning phases of the study, where demands on site staff were high, owing to unfamiliarity with the DCT setup, an underestimated workload, and technical issues experienced by participants with their own smartphones. Owing to a high number of people signing up for the study and an underestimation of time spent on informing and guiding participants during the initial telemedicine visits, particularly in the early stages of the study such as the informed consent visit (RV1), frequent rescheduling of visits RV1 and RV2 was required until study staff had become familiar with the study platform and procedures. Moreover, the DCT setup placed high demands on the availability and capability of the study staff in addressing technical IT issues, especially as study staff acted as first-line technical support to participants. Because participants used their own smartphones, there was extensive guidance required to check and adjust the settings of their phones (e.g., phone operating systems needed to be updated, text size settings needed to be changed) and to aid with the installation and setting up of the study apps. Issues with the setup and synchronization of the activity tracker, in particular, placed an extra burden on study staff. Ensuring a robust setup and offering clear guidance on how to obtain support is crucial. In future studies, these technical issues could be avoided by providing smartphones with pre-installed study apps to participants, although this would increase study costs and require participants to manage an additional phone.
Other technical challenges were related to the data flow ecosystem, which was required to ensure that participant data were collected correctly while maintaining data privacy and security. The automated data flow did not function as intended, and some data had to be transferred manually. Throughout the study, notifications and reminders were sent to participants. However, SMS (text message) notifications did not work as intended due to international carrier restrictions.
Previous remote care studies evaluating CGM primarily focused on providing clinical support within routine care and therefore differ from our DCT design, which applied remote procedures across all aspects of a clinical trial. 12 Our study builds on a prior 3-week pilot study in 26 adults with T2D in Denmark assessing selected DCT elements; however, its short duration and small number of participants limited the ability to capture outcomes such as participant adherence to study procedures, participant retention, and potential device or app fatigue. 8 By extending the duration to 14 weeks, including a larger and more geographically diverse cohort, fully online recruitment and e-consent process, scheduled telemedicine visits, and remote data collection, the present study more closely reflects a full-scale DCT and may serve as a reference point for future DCT trials requiring closer clinical monitoring.
A strength of this study is that the DCT setup permitted the inclusion of a broader range of people, who possibly would not be able to participate otherwise due to practicalities. Moreover, the DCT setup reduced the burden on participants by removing the need to travel to a study site for in-person visits, which may have resulted in increased engagement and maintained participation/retention due to increased flexibility and convenience. Consequently, the data collected are likely more representative of real-world data. The DCT design enabled study staff to work remotely from their own homes, providing flexibility and potentially improving staff work–life balance. Additionally, allowing participants to view their own CGM data via the associated app enhanced engagement, and in future studies where permitted, such granular, real-time data collection could provide valuable insights into disease management and treatment patterns for sponsors and investigators.
However, this study also had some limitations that warrant consideration. There was selection bias owing to the non-randomization of treatment groups and the technical capabilities of participants, who may have faced technical barriers and device compatibility issues when downloading and using the study app, especially when using their own smartphone. Recruitment of participants through social media may have excluded individuals who are not active on these platforms, impacting the inclusiveness of the study. Recruitment appeared to have been positively impacted by specific components of the DCT setup (i.e., the inclusion of CGM), and therefore studies conducted under the same conditions but with other components might experience differences in recruitment speed and compliance. Moreover, the feasibility of “remote” randomization could not be evaluated because the study was observational.
Because this study was only conducted in one country, it may limit the generalizability of conducting a similar, fully remote study in different settings. For example, the national acceptability of e-signatures for the informed consent process in Denmark may not apply elsewhere. Moreover, it may not be possible to confirm participants’ medications in other healthcare settings that do not have a centralized database. Additionally, this study was conducted in Denmark, a relatively small country in terms of geographical size and population. Conducting similar studies in larger and more populous countries may present additional technical and logistical challenges.
Conclusions
This proof-of-concept study demonstrated the feasibility of setting up and running a highly digitalized, fully decentralized study in Denmark. The DCT setup has the potential to reduce participant enrollment time and lessen the burden experienced in traditional clinical studies. As a result, the DCT setup could enhance participant diversity, thereby improving generalizability by better reflecting the broader population. This may ultimately help to close the efficacy–effectiveness gap in clinical research.
Authors’ Contributions
A combination of academic authors and authors who are employees of Novo Nordisk A/S (the study sponsor) participated in developing the study concept and design and in collecting the data. All authors were involved in the analysis and interpretation of data, participated in preparing the article, and approved the final article that was submitted.
Footnotes
Acknowledgments
The authors thank all study participants and study site staff. The authors thank Tim Dunn, PhD, of Abbott Diabetes Care Inc. The authors also wish to thank Science 37 Inc., which provided the study app and the DCT platform, and conducted the study via their direct-to-patient site on behalf of Novo Nordisk A/S. Medical writing support was provided by Adam Hargreaves, PhD, of Oxford PharmaGenesis, Oxford, UK, with funding from Novo Nordisk A/S.
Author Disclosure Statement
K.N. serves as an adviser to Abbott Diabetes Care, Convatec, Medtronic, Novo Nordisk, and Tandem; owns stocks in Novo Nordisk; has received research grants to her institution from Dexcom, Medtronic, Novo Nordisk, and Zealand Pharma; and has received fees for speaking from Medtronic and Novo Nordisk. U.C.B., A.K., S.A.C.V., and L.S.H. are employees of Novo Nordisk A/S and own stock or stock options in Novo Nordisk A/S.
Funding Information
This study was funded by Novo Nordisk A/S. The CGM devices and supplies used during this study were provided by Abbott Laboratories, USA.
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.