
Abstract
Introduction:
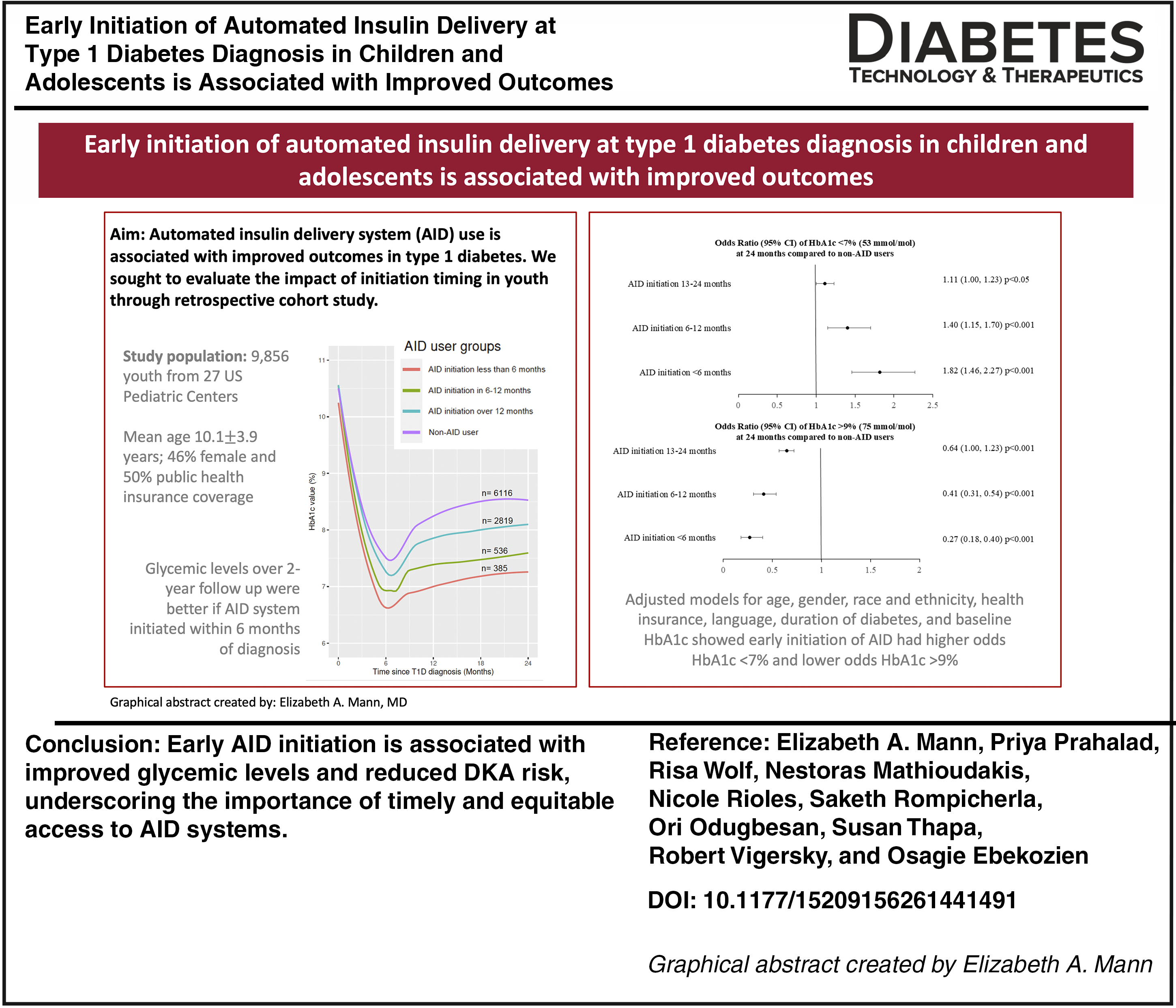
This retrospective cohort study evaluates the impact of timing of automated insulin delivery (AID) initiation on glycemic outcomes in youth with type 1 diabetes.
Methods:
Data from 9856 children and adolescents diagnosed with type 1 diabetes between 2020 and 2022 across 27 U.S. centers were analyzed. Participants were grouped by AID initiation timing in months: <6, 6–12, 13–24, or no AID use. Hemoglobin A1c (HbA1c) trajectories, diabetes-associated ketoacidosis (DKA), and severe hypoglycemia rates were assessed over 24 months after T1D diagnosis.
Results:
Earlier AID initiation was associated with lower HbA1c at 24 months (median 7.1% in the <6-month group vs. 9.8% in non-users, P < 0.001). DKA rates were threefold higher in non-AID users. Adjusted models confirmed the timing of AID initiation independently predicted HbA1c outcomes.
Conclusions:
Early AID initiation is associated with improved glycemic control and reduced DKA risk, underscoring the importance of timely and equitable access to AID systems.
Introduction
Background and rationale
Lower hemoglobin A1c (HbA1c) in childhood, adolescence, and young adulthood for people with type 1 diabetes is associated with a lower risk of microvascular and macrovascular complications,1–3 yet young people struggle to meet glycemic targets. The mean HbA1c among children (1–15 years) and adolescents and young adults (16–25 years) is 8.6% (SD 2.1) and 8.6% (SD 2.2), respectively. Despite improvements over recent years, in part attributed to the availability of diabetes technology, these remain above the American Diabetes Association target of 7.0%. 4
Advanced diabetes technologies, particularly automated insulin delivery (AID) systems, are now recognized as the gold standard therapy for individuals with T1D. 5 Their use is associated with reduction in HbA1c, severe hypoglycemia (SH) events, and diabetes-associated ketoacidosis (DKA) for people with type 1 diabetes.6,7 Neurocognitive function in the short term also associates with glycemic levels, and glycemic improvement with AID use has been linked to improved neurodevelopment and cognition.8,9 Despite the demonstrated benefits,5,10–16 significant racial and ethnic disparities exist in the use of pediatric and adult populations with type 1 diabetes. 4
In small, controlled environments, early initiation of AID systems after diagnosis in children and adolescents with type 1 diabetes improves short-term glycemic outcomes. In a randomized trial of 97 youth ages 10–17 years, initiation of AID systems within 21 days of diagnosis was associated with improved time in range (TIR) (70–180 mg/dL [3.9–10.0 mmol/L]) and lower HbA1c at 12 months. 17 Another randomized trial of 113 youth ages 7–17 years with type 1 diabetes also showed improved TIR at 6 months of diagnosis following initiation of AID systems within 31 days of diagnosis. 18
The T1D Exchange Quality Improvement Collaborative (T1DX-QI) is a multicenter learning health network made up of pediatric and adult diabetes centers across the United States. Originally established in 2016, it now includes over 60 centers.19–21 Organization and development of the data sharing within the network have been previously described. 22 Data collection, governance, and central analysis within the T1DX-QI allow for population studies analyzing real-world outcomes with the purpose of implementing real-time changes in clinical practices to improve patient care. 23
This retrospective cohort study across the pediatric centers in the T1DX-QI assessed the association between use and timing of AID initiation and HbA1c outcomes at 24 months post-diagnosis in children and adolescents with type 1 diabetes.
Methods
Study design
Data were obtained from 27 pediatric diabetes centers in the T1DX-QI network. The Western-Copernicus Group Institutional Review Board centrally approved this as an exempt population-based study with HIPAA consent waived, as no identifiable information was used. Data-sharing centers also obtained necessary ethical approvals to share deidentified data with T1DX-QI.24,25 Data collection methods, including data specifications, are well documented.26,27
This study included children and adolescents 18 years of age or younger diagnosed with type 1 diabetes between 2020 and 2022 with at least 2 years of follow-up data after diagnosis in the database and including at least one HbA1c value beyond 18 months from diagnosis. The cohort was grouped into four categories based on the timing of AID initiation following diagnosis: within 6 months, between 6 and 12 months, between 13 and 24 months, and those who did not initiate AID within the follow-up period.
The primary outcome was HbA1c, and all those obtained clinically between diagnosis and the 2-year follow-up period were included in the analysis. HbA1c outcomes were analyzed relative to timing from type 1 diabetes diagnosis. Secondary outcomes included DKA events and SH events defined as blood glucose <54 mg/dL (3.0 mmol/L) or low blood glucose requiring assistance over the course of data collection. Demographics and diabetes management variables included age at diagnosis, gender (female/male/nonbinary or other), race and ethnicity, health insurance type (public/private/other), and preferred language.
Temporal trends in HbA1c for each initiation group were visualized using locally estimated scatter plot smoothing (LOESS) to flexibly model nonlinear relationships between time and outcome without imposing a parametric functional form. Categorical variables were analyzed across subgroups using logistic regression models, while continuous variables were compared using Student’s t-tests. Models were adjusted for age, gender, race and ethnicity, health insurance type, preferred language, duration of diabetes, and baseline HbA1c.
Results
Study population characteristics
There were 9,856 children and adolescents with type 1 diabetes included in this analysis, and baseline characteristics were analyzed by age sub-cohorts in Table 1. The mean age was 10.1 years, 46% were female (n = 4,532), and 50% were from marginalized racial and ethnic groups (n = 4,944). Public insurance coverage was 50% overall but decreased with age (50% in 2–5 years, 32% in 6–12 years, and 29% in 13–18 years). Reported AID systems used included Tandem’s t:slim X2 and Mobi, Insulet’s Omnipod 5, Beta Bionic’s Islet, and Medtronic’s 670G, 770G, & 780G.
Summary of Study Population with Sub-Cohorts by Age. Values Are Reported as n (%) Unless Otherwise Specified
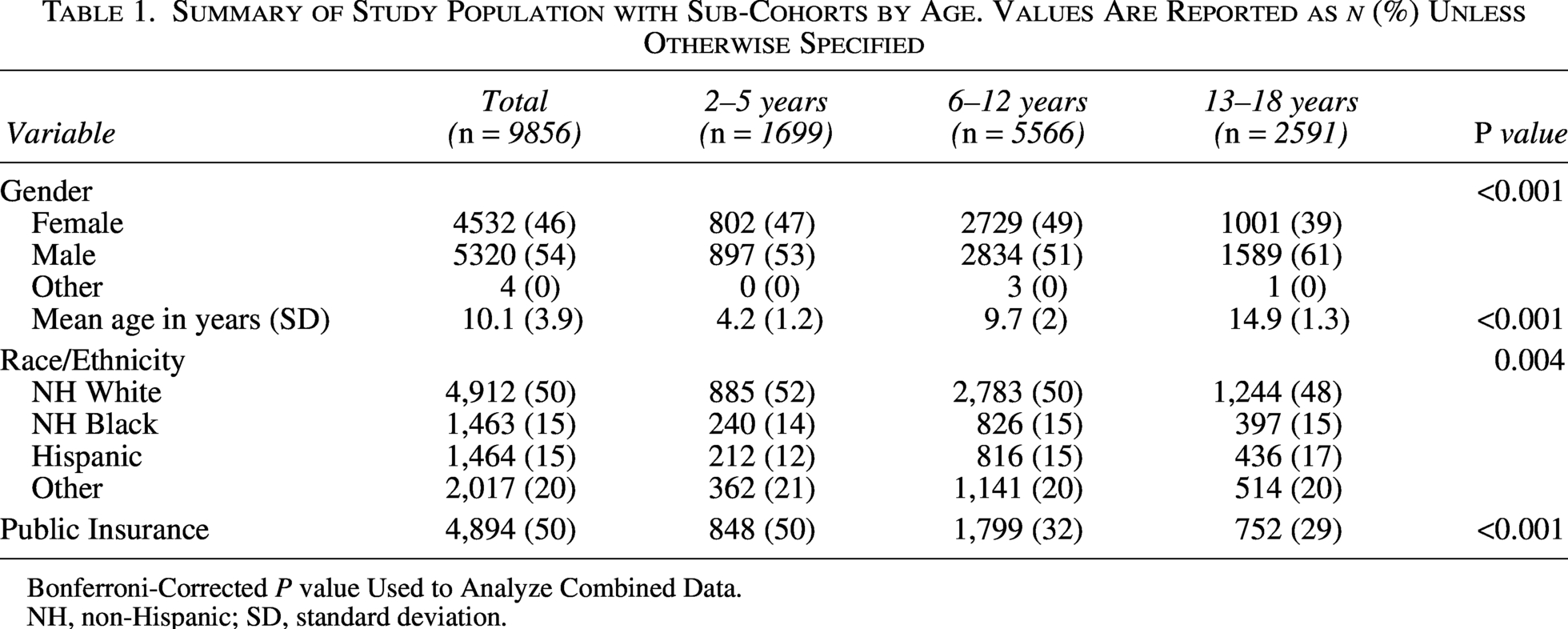
Bonferroni-Corrected P value Used to Analyze Combined Data.
NH, non-Hispanic; SD, standard deviation.
Comparison of AID initiation and non-AID initiation groups
Table 2 summarizes the distribution of the study population by AID initiation timing. During the 2-year follow-up period, 38% of children and adolescents started AID systems: 4% <6 months (n = 385), 5% between 6 and 12 months (n = 536), and 29% between 13 and 24 months following diagnosis (n = 2,819). While the groups were consistent in mean age and gender, they showed key differences by race/ethnicity and insurance type. Non-Hispanic White individuals made up 71% of the <6-month group but only 46% of the non-AID users. Public insurance coverage was lowest among early AID initiators (19% in <6-month group, 22% in 6–12-month group) and highest among non-AID users (34%).
Distribution of Cohort by AID Initiation Post-Diagnosis
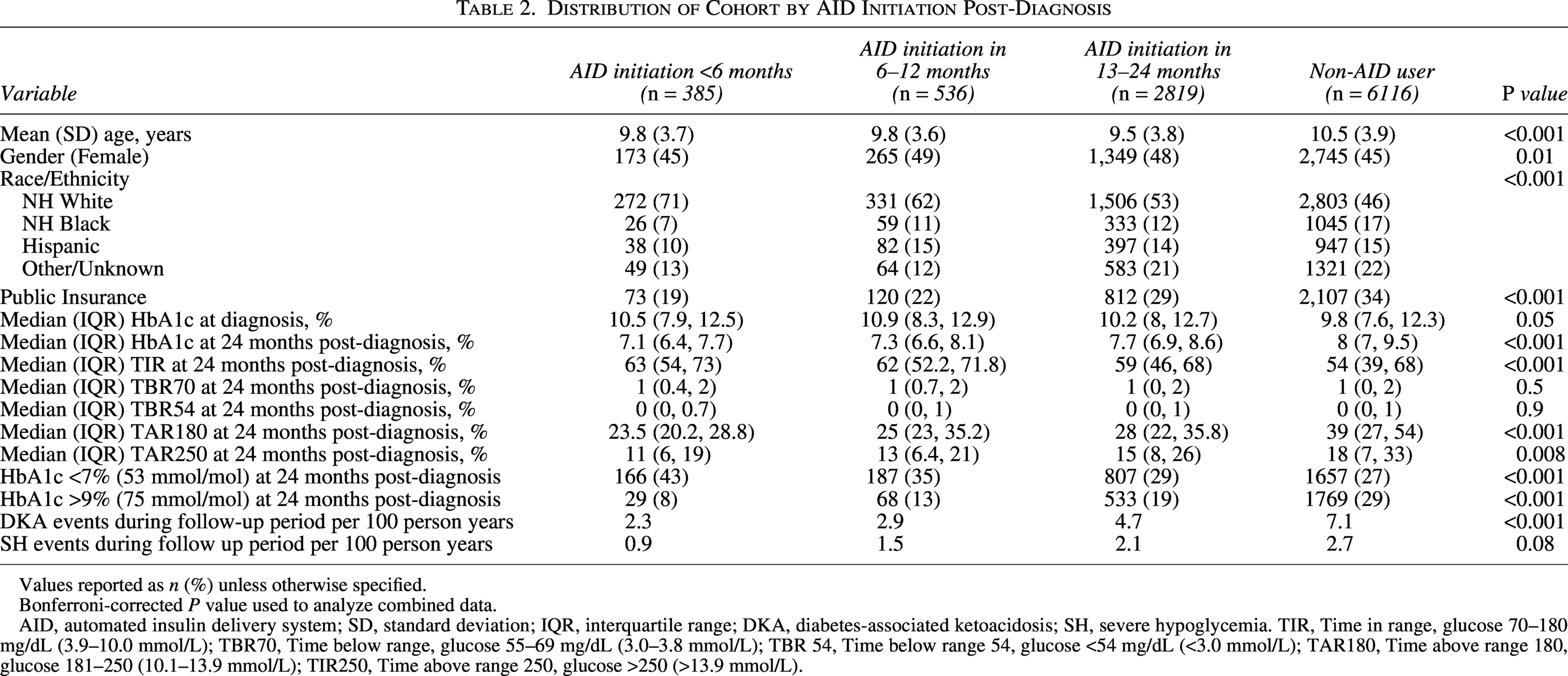
Values reported as n (%) unless otherwise specified.
Bonferroni-corrected P value used to analyze combined data.
AID, automated insulin delivery system; SD, standard deviation; IQR, interquartile range; DKA, diabetes-associated ketoacidosis; SH, severe hypoglycemia. TIR, Time in range, glucose 70–180 mg/dL (3.9–10.0 mmol/L); TBR70, Time below range, glucose 55–69 mg/dL (3.0–3.8 mmol/L); TBR 54, Time below range 54, glucose <54 mg/dL (<3.0 mmol/L); TAR180, Time above range 180, glucose 181–250 (10.1–13.9 mmol/L); TIR250, Time above range 250, glucose >250 (>13.9 mmol/L).
Outcomes and AID initiation timing
Overall, HbA1c measurement availability was similar across all user groups. At 24 months post-diagnosis, median HbA1c was lowest in the <6 months AID group (7.1%, 54 mmol/L) and highest in non-AID users (9.8%, 84 mmol/mol), as shown in Table 2. The rates of DKA during the follow-up period were three times higher in the non-AID users compared to the early initiation group (7.1 vs. 2.3 per 100-person years, P < 0.001). The rates of SH events decreased with earlier AID initiation, but the trend was not statistically significant.
Temporal trends in HbA1c by user group are visualized in Figure 1 with a LOESS plot. Following the expected early decrease in HbA1c post-diagnosis, the <6-month AID group had the lowest HbA1c nadir at 6 months. This cohort had the lowest mean HbA1c throughout the follow-up period out of 24 months. There was a gradient association with mean HbA1c in the other user groups, as the 6–12-month AID group had the next highest HbA1c trajectory, and the 13–24-month AID group was slightly higher than that. The non-AID user group had the highest HbA1c nadir and subsequent mean levels at all time points.
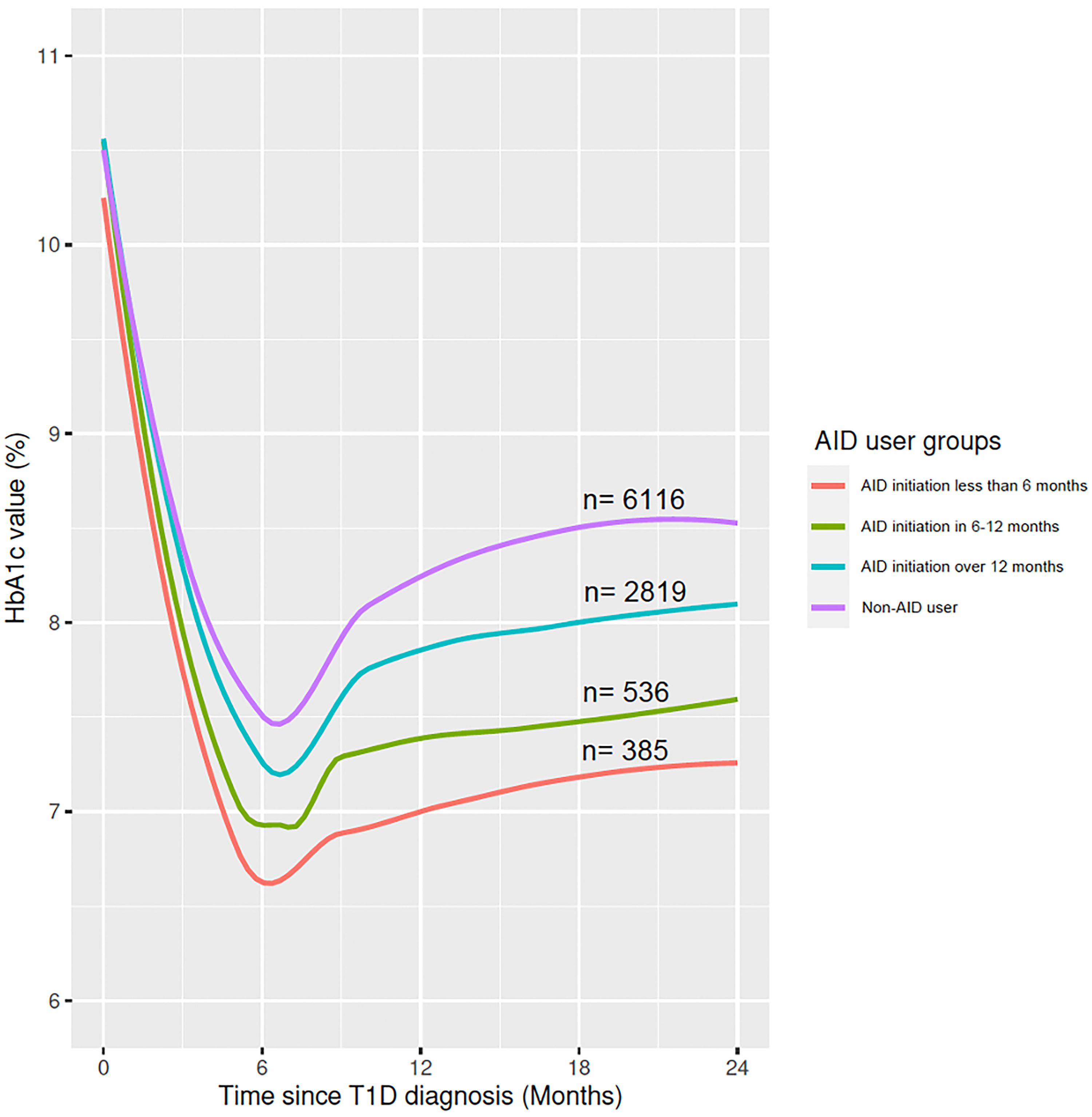
LOESS plot demonstrating mean HbA1c trend by AID initiation group post-diagnosis.
Adjusted models for age, gender, race and ethnicity, insurance, language, duration of diabetes, and baseline HbA1c demonstrated differences between HbA1c outcomes at 24 months by user group (Fig. 2). Compared to non-AID users, AID users who initiated in <6 months had a 1.82 odds ratio (95% CI 1.46–2.27) (P < 0.001) of having HbA1c <7% (53 mmol/mol) and 0.27 odds ratio (95% CI 0.18–0.40) (P < 0.001) of having HbA1c >9% (75 mmol/mol) at 24 months. The 6–12 month and 13–24 month groups also had increased odds ratio of HbA1c < 7% (53 mmol/mol) and lower odds ratio of HbA1c >9% (75 mmol/mol) at 24 months compared to non-AID users (P ≤ 0.05).
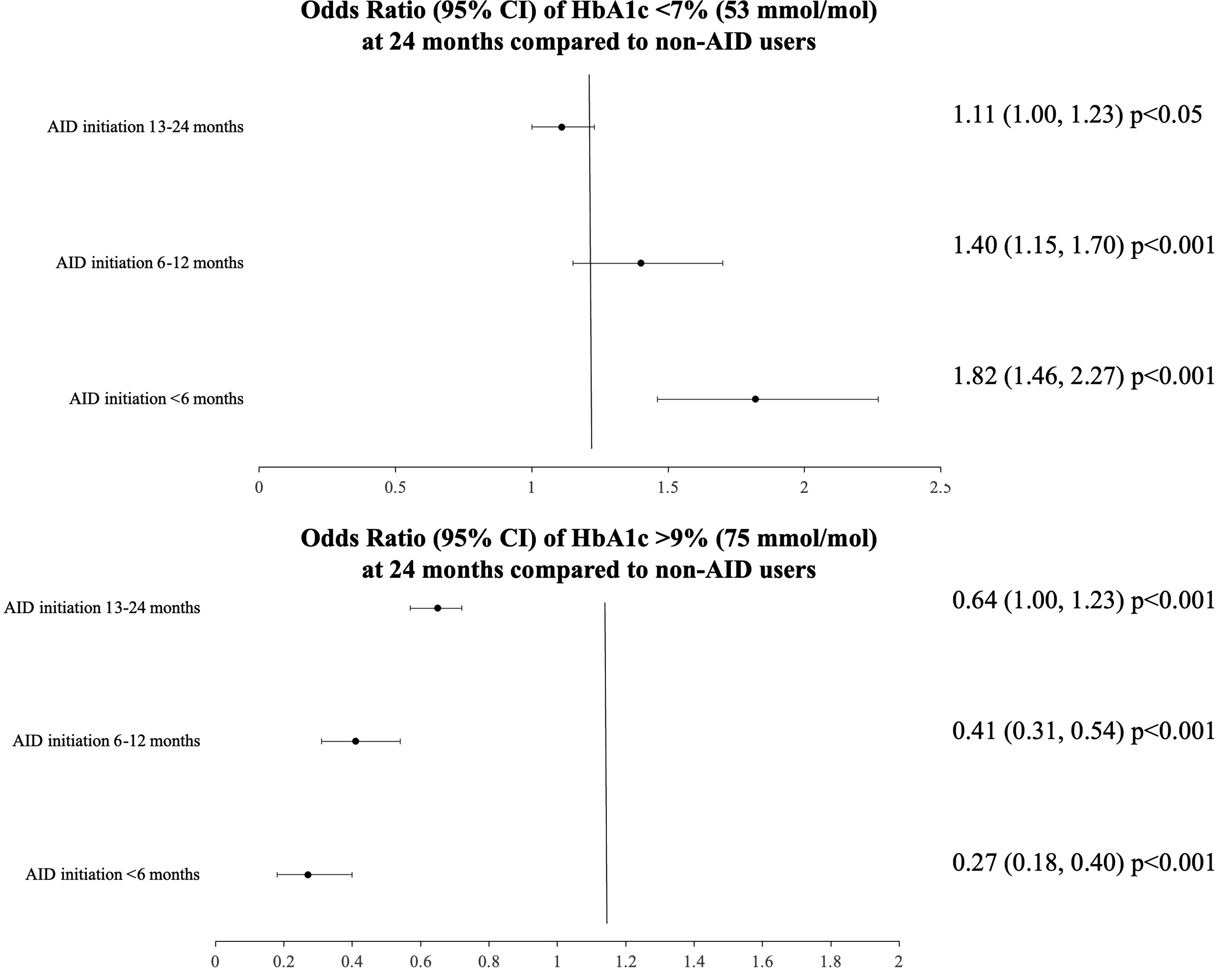
Forest plot of adjusted odds ratio (95% CI) using logistic regression models for HbA1c outcomes at 24 months post-type 1 diabetes diagnosis by AID initiation group using the reference group of non-AID users. Models adjusted for age, gender, race and ethnicity, health insurance, language, duration of diabetes, and baseline HbA1c.
Discussion
This retrospective cohort study involving nearly 10,000 U.S. children and adolescents with type 1 diabetes demonstrated that earlier initiation of AID following diagnosis is associated with improved glycemic levels 2 years later. Specifically, the median HbA1c at this interval was significantly lower in AID users compared to non-AID users. This association remained statistically significant after adjusting for age, gender, race and ethnicity, health insurance type, preferred language, and baseline HbA1c. Initiating AID within 6 months of diagnosis was associated with a highest likelihood of achieving target HbA1c levels (<7%; 53 mmol/mol) and the lowest likelihood of elevated HbA1c (>9%; 85 mmol/mol) compared to non-AID users. This large-scale real-world analysis supports similar findings from smaller research trials over a longer follow-up period.
Early initiation of AID systems likely impacts HbA1c beyond the effect from CGM through several mechanisms. By automating insulin delivery, AID reduces the burden of constant monitoring and manual dosing, leading to more precise and timely insulin administration. This approach may also help establish effective self-management strategies while alleviating diabetes-related distress and burnout through fluctuations in endogenous insulin production following diagnosis. These findings suggest that both the utilization of AID and the timing of its initiation are critical factors influencing HbA1c outcomes.
While early initiation of AID systems showed improved glycemic outcomes, those who initiated within the earliest timeframe were disproportionately non-Hispanic White and privately insured. In addition to disparities based on socioeconomic status, racial, ethnic, and insurance-related disparities in diabetes technology are well documented.28–30 Barriers to use in marginalized racial and ethnic groups include increased experiences of diabetes-related stigma and provider bias. 31 And that these disparities extend to timing of initiation, as demonstrated in this analysis, suggests potential implications for long-term glycemic levels, underscoring the importance of early and equitable access to AID systems.
Several limitations of the study warrant consideration. The ability to detect glycemic differences in the later AID initiation group (13–24 months) was limited by post-initiation HbA1c data, though the earlier initiation groups had more robust collection periods. The use of clinical registry data introduces potential unidentified confounders that may be affecting the association between AID initiation timing and HbA1c outcomes. The T1DX-QI registry does not include DKA status at diagnosis, family history of type 1 diabetes, AID use in family members, nor caregiver education level, which may individually influence AID use and outcomes. Additionally, this may have contributed to selection bias, as individuals and families more engaged or experienced in diabetes self-management or more highly resourced may have been more likely to start AID use sooner. To mitigate this, user groups were compared across socio-demographic variables, and multivariate models were adjusted for identifiable confounders. The presence of differential patient loss at follow-up between AID initiation groups could also lead to attrition bias; however, sensitivity analyses revealed similar attrition rates across groups. Exploration of DKA events because of AID systems or their use is not available given the limitations of this discrete dataset, but future work should explore real-world data to understand the impact of AID use on DKA rates.
In summary, this analysis encompasses a large, diverse population of children and adolescents with type 1 diabetes and demonstrates the glycemic benefits of early AID initiation. Addressing barriers to timely adoption through targeted advocacy is imperative to reduce disparities in AID timing and use. Comprehensive strategies focusing on policy reform, insurance coverage expansion, and standardized care pathways along with targeted equity initiatives are needed to improve early AID access, aiming to reduce disparities and improve glycemic outcomes.
Authors’ Contributions
E.A.M. and P.P. contributed to the conceptualization of the study and writing of the first draft. S.R. completed data curation and formal analysis and review and editing. R.W., N.M., N.R., O.O., S.T., R.V., and O.E. contributed to the review and editing of the article. All authors approved the final version of the article. E.A.M. is the guarantor of this work and, as such, has full access to all the data in the study and takes responsibility for the integrity of the data and accuracy of the data analysis.
Footnotes
Author Disclosure Statement
P.P. has served on advisory boards for Sanofi and Insulet. R.V. is an employee of Medtronic Diabetes. E.A.M., R.W., N.M., N.R., S.R., S.T., and O.E. report no conflicts of interest relevant to this article.
Funding Information
This study was supported by the Helmsley Charitable Trust which funds the T1D Exchange QI Collaborative. The authors also acknowledge the contributions of the people living with diabetes, their families, diabetes care teams, and collaborators within T1DX-QI, who continually seek to improve care and outcomes.