
Abstract
Automated insulin delivery (AID) systems have improved glycemic metrics in individuals with type 1 diabetes (T1D). Despite this, reaching glycemic targets remains elusive in many youth with T1D. During the honeymoon period after diagnosis, improved beta cell function can promote higher time in range 70–180 mg/dL (TIR). However, a prior study by Boughton et al. found a relatively low mean TIR of 64% ± 14 at 12 months in youth on AID systems started in the first 6 weeks after diagnosis. 1
Recently, in the CLVer study, McVean et al. reported mean TIR of 82% over the course of the trial (Fig. 1) and mean TIR of 78% at 52 weeks in youth aged 7 to <18 years randomized to AID within 31 days of diagnosis, 2 which was substantially higher than TIR in a usual care control group, although there was no benefit observed on C-peptide levels. Moreover, of the 59 participants in the AID group with data at 52 weeks, 49% had TIR > 80% and 78% had TIR > 70% at 52 weeks. 2 This is greater than the percent of youth with TIR 70% 52 weeks after treatment with teplizumab for stage 3 of T1D. 3 This letter discusses aspects of the study that led to achieving high TIR while ensuring support for persistent and effective AID use.
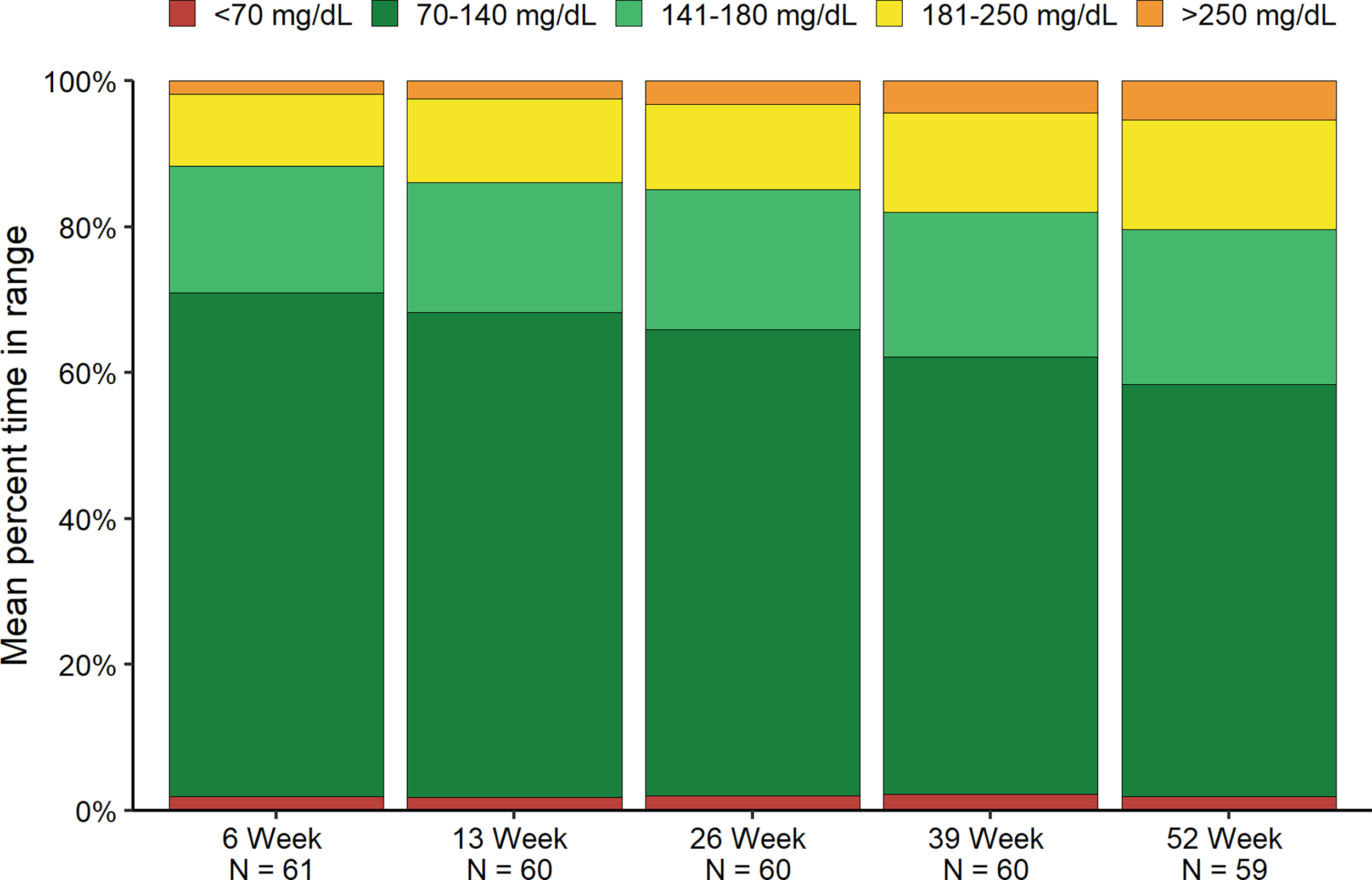
Mean time in glucose ranges in the AID group over time. AID, automated insulin delivery.
Standardized, structured education was provided to participants in the AID group at five in-person visits at baseline, 13, 26, 39, and 52 weeks. A study dietician met with participants at four visits covering carbohydrate counting, meal composition, premeal bolusing, and regular physical activity. Device education focused on remaining in automation and maximizing time in target range of 70–180 mg/dL (goal > 85% time). Checklists ensured consistent education delivery. As families gained experience with diabetes management, participants were permitted to switch AID systems if they were dissatisfied with their randomly assigned system, and 16% used this allowance to personalize treatment.
AID education started early due to randomization in the first month since diagnosis. Therefore, discussions about treatment goals occurred early and repeatedly. The efficacy of clear, consistent expectations of tight targets is highlighted by data from Sweden and mirrored in multinational data and may have promoted high TIR.
A major unique aspect of the education was its intensity at device start, with participants contacted every 1–3 days for the first 2 weeks following device initiation, then twice per week for the second 2 weeks, and then every 1 to 2 weeks for the remainder of the 52-week study. Due to the COVID-19 pandemic, some visits were done via video, and phone contact and text messaging were also utilized. Sites received monthly reports documenting percent time in automation and percent TIR to highlight participants who might need insulin dose optimization or additional education/support. This frequent contact with the study team and focus on optimizing percent time in automation (median 93% time in automation during the study period out to 52 weeks) 2 likely supported the higher mean TIR than had been seen in the study by Boughton et al., which reported median time in automation 76% over 24 months). 1
This ongoing support was provided beyond what is generally possible in standard clinical care. The study teams were available to participants outside of the five per-protocol visits over 52 weeks. Of the unscheduled contacts based on device or glycemic issues, there was an average of 1.0 contacts per participant per month during the first 3 months, 0.6 per month in the second 3 months, 0.6 per month in the third 3 months, and 0.4 per month in the final 3 months. This high frequency of contact may have contributed to persistent and effective device use.
Feasibility and cost-effectiveness of implementing this type of intervention in clinical practice remain to be seen. Despite the rising prevalence of youth with endocrinologic disease, the numbers of pediatric endocrinology training programs and fellows are not commensurate. 4 Recently, Prahalad et al. utilized population health management tools in care of youth with T1D and found that a technology-enabled, team-based approach with weekly data review led to lower HbA1c levels over the first year after diagnosis with average TIR 63% 12 months after diagnosis. 5 These tools might be leveraged in clinical care to provide intensive and individualized support despite the stagnant pediatric diabetes workforce.
In this clinical trial of youth newly diagnosed with T1D randomized to two commercially available AID, mean TIR was high over 52 weeks in the setting of early, frequent contacts and considerable effort from the study teams, who report building strong relationships with the participants and families. The frequent contact provided with device initiation in CLVer may be challenging to implement in clinical practice; however, population health tools may help to support translation of intensive management programs to clinical care.
Data Availability Statement
Data will be made available on a publicly available website (www.jaeb.org) at a later date.
Submitting Agent Statement
This article has been submitted with no editorial input by Jeff Saunders, Jaeb Center for Health Research with submission paid for by the Jaeb Center for Health Research, and all authors authorizing submission of the article via third party.
Authors’ Contributions
M.V.N.: Writing—original draft and reviewing editing. J.S.: Writing—review and editing. C.B.: Writing—review and editing. B.B.: Writing—review and editing. G.F.: Writing—review and editing. A.N.: Writing—review and editing. R.B.: Writing—review and editing. L.K.: Formal analysis and writing—original draft. C.K.: Writing—review and editing. S.B.: Writing—review and editing. E.C.: Writing—review and editing. L.N.: Writing—review and editing. R.M.: Writing—review and editing. L.D.: Writing—review and editing. J.M.: Writing—review and editing. A.M.: Writing—original draft.
Footnotes
Author Disclosure Statement
Dr. Van Name having received consulting/advisory fees from Mankind, Novo Nordisk, and Solano Therapeutics, and her institution has received research funding on her behalf from Lilly, Mankind, Novo Nordic, Prevention Bio, and Sanofi. Dr. Sherr reports having received speaker honoraria from Eli Lilly, Insulet, Medtronic, and Zealand; and serving on advisory boards of Bigfoot Biomedical, Cecelia Health, Insulet Corporation, Medtronic Diabetes, JDRF T1D Fund, StartUp Health T1D Moonshot, and Vertex; receiving consultant fees from Insulet and Medtronic, and that her institution has received research grant support from JDRF, Medtronic, Insulet, and NIDDK. Dr. Bauza has no conflicts of interest or financial disclosures. Dr. Buckingham reports having received consulting/advisory fees from Medtronic, Insulet, Lilly, and NovoNordisk; and his institution has received research funding from Medtronic, Tandem, Beta Bionics, and Insulet. Dr. Forlenza reports that he has served as a consultant, speaker, or advisory board member for Medtronic, Dexcom, Abbott, Tandem, Insulet, Lilly, and Beta Bionics and that his institution has received funding on his behalf for research grants from Medtronic, Dexcom, Abbott, Tandem, Insulet, Lilly, and Beta Bionics. Dr. Neyman reports no conflicts of interest or financial disclosures. Dr. Beck reports no personal financial disclosures but reports that his institution has received funding on his behalf as follows: grant funding and study supplies from Tandem Diabetes Care, Beta Bionics, and Dexcom; grant funding from Bigfoot Biomedical; study supplies from Medtronic, Ascencia, and Roche; consulting fees and study supplies from Eli Lilly and Novo Nordisk; and consulting fees from Insulet, and Zucara. Ms. Kanapka has no conflicts of interest or financial disclosures. Dr. Kollman reports no conflicts of interest or financial disclosures. Ms. Beasley reports no conflicts of interest or financial disclosures. Dr. Cobry reports no conflicts of interest. Dr. Norlander reports no conflicts of interest. Dr. McDonough reports receiving consultancy/speaker fees and advisory board membership for Sanofi and Glooko. Dr. DiMeglio reports receiving consulting or advisory fees from Abata Therapeutics, MannKind, Provention Bio, and Zealand Pharma and study supplies from Dexcom Dr. McVean is now an employee of Medtronic. Dr. Moran reports serving on advisory boards from Dompé Farmaceutici SpA, ProventionBio, and Abata Therapeutics; serving on a data and safety monitoring board for NovoNordisk; and reported that her institution has received grant funding on her behalf from Abbott Diabetes, ProventionBio, Intrexon (now Precigen), and Caladrius Biosciences and study supplies from NovoNordisk, Medtronic, and Abbott Diabetes.
Funding Information
Study funding was provided by Breakthrough T1D (formerly the Juvenile Diabetes Research Foundation). Medtronic, Tandem Diabetes Care, and Dexcom provided the devices used in the trial.