
Abstract
Background:
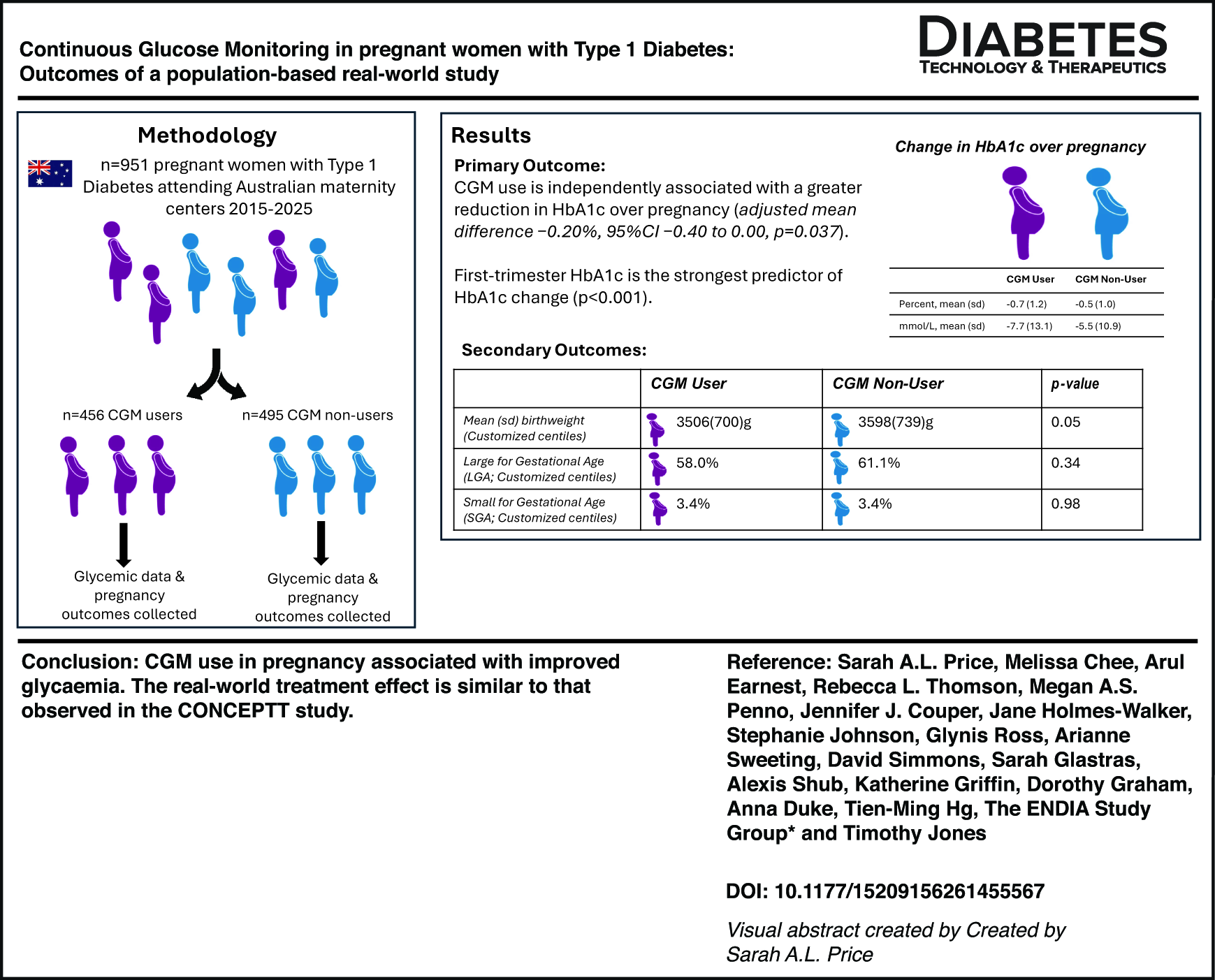
Continuous glucose monitoring (CGM) is increasingly used by women with type 1 diabetes (T1D) during pregnancy, but there are limited data on glycemic and pregnancy outcomes in large real-world cohorts.
Methods:
We collected glycemic and pregnancy outcome data from women with T1D across Australian centers between 2015 and 2025. The primary outcome was change in HbA1c from the first to the third trimester of pregnancy. Prespecified secondary outcomes included trimester-specific mean HbA1c, the proportion of women achieving HbA1c ≤6.5% (≤48 mmol/L) and ≤7.0% (≤53 mmol/L) in the third trimester, and a range of maternal and neonatal health outcomes.
Results:
Among 951 women, 456 (48%) were CGM users. Demographics and baseline characteristics were similar between CGM users and nonusers. For the primary outcome, adjusted linear regression models accounting for first-trimester HbA1c and insulin regimen demonstrated that CGM use was independently associated with a greater reduction in HbA1c over pregnancy (adjusted mean difference −0.20%, 95% confidence interval [CI] −0.40 to 0.00, P = 0.037). First-trimester HbA1c was the strongest predictor of HbA1c change (P < 0.001).
After adjustment for first-trimester HbA1c, first-trimester body mass index, insulin regimen, parity and year of delivery, CGM use was not associated with large- or small-for-gestational-age offspring and there was no significant difference between the groups in mean birthweight. Among primiparous women, CGM use was associated with lower odds of cesarean section after adjustment for confounders (adjusted odds ratio 0.22, 95% CI 0.08–0.58, P = 0.002).
Conclusions:
CGM use in pregnancy is associated with improved glycemia. The treatment effect of CGM in this real-world study is similar to that observed in the CONCEPTT study, thus supporting CGM use in pregnant women with T1D.
Introduction
Most pregnant women with type 1 diabetes (T1D) do not achieve optimal glycemic targets and have worse pregnancy outcomes than the general population.1,2 However, evidence from clinical trials suggests that diabetes technology such as continuous glucose monitoring (CGM) improves glycemia and pregnancy outcomes.3–5
The 2017 multicenter international randomized controlled trial “Continuous glucose monitoring in pregnant women with type 1 diabetes” (CONCEPTT) compared glycemic control in prepregnant and pregnant women with T1D who used CGM versus women who did not use CGM. 6 In pregnant women using CGM from randomization (<13 + 6 weeks of gestation) to 34 weeks of gestation, CGM use was associated with improved glycemic control (HbA1c mean difference −0·19%; 95% confidence interval [CI]: −0·34 to −0·03; P = 0·0207). Women who used CGM also had improved neonatal outcomes with a lower incidence of large-for-gestational-age (LGA) offspring (odds ratio [OR]: 0.51, 95% CI: 0.28–0.90; P = 0.0210), neonatal intensive care admissions lasting more than 24 h (OR: 0.48; 95% CI: 0.26–0.86; P = 0.0157), and neonatal hypoglycemia (OR: 0.45; 95% CI: 0.22–0.89; P = 0.0250), as well as 1-day shorter length of hospital stay (P = 0.0091). 6
Based on the results of CONCEPTT, the Australian Government subsidized CGM products for prepregnant and pregnant women living with T1D through a national scheme in 2018. 7 Although multiple studies have demonstrated the benefits of CGM in improving clinical outcomes in large prospective randomized clinical trials and in smaller observational studies,4,6,8–10 there are few real-world studies that demonstrate benefit across whole populations. In this study, we aimed to determine the benefits of CGM on glycemic control and pregnancy outcomes in a population-based real-world Australian cohort.
Methodology
Study design
This multicenter cohort study involved the collection of clinical data from pregnant women with T1D attending both large public maternity hospitals and a smaller number of public and private maternity care providers across Australia. Three models of data collection were used. An opt out consent model was used in some centers. In these centers, a participant information statement was provided to women, including the details of the principal investigator or a delegated staff member to answer questions about the nature and purpose of the study and all women were given the opportunity to opt out. In those centers where an informed consent model was required, all participants provided informed consent to opt in before data collection. Third, through a collaboration with the Environmental Determinants of Islet Autoimmunity (ENDIA) study (ANZCTR registration number: ACTRN12613000794707),11,12 some women contributed deidentified data through their participation in this study. The ENDIA study was reviewed and approved by the Women’s and Children’s Hospital Human Research Ethics Committee (HREC) acting as the lead under the Australian National Mutual Acceptance Scheme (2020/HRE01400), and by the Women and Newborn Health Service HREC (RGS0000002639) and the Child and Adolescent Health Service HREC (RGS0000002402) in Western Australia. For all women, deidentified demographic data and clinical metrics were collected from the start of pregnancy until 6 weeks postpartum. There was no impact on standard clinical care. The study was prospectively approved by the Melbourne Health HREC (HREC/95601/MH-2023-372828).
Study subjects
This study consisted of pregnant women living with T1D who attended an Australian hospital for maternity care between January 2015 and January 2025. This time frame included the introduction of a national subsidy for CGM products initially for pregnant women with T1D, and then for all persons with T1D. The timing of implementation of the subsidy and of access to CGM education varied across Australian centers. All women with T1D attending Australian maternity centers are routinely offered information about CGM at a preconception care appointment or at the first antenatal appointment. For the purposes of this study, CGM users were defined as women who were using CGM by 12 + 6 weeks of gestation. CGM nonusers were defined as women who had not used CGM by 12 + 6 weeks of gestation.
Demographic data and clinical data were obtained from the medical record of the mother and linked offspring. Extracted data included maternal age, first visit body mass index (BMI), ethnicity, postcode, diabetes duration, and HbA1c. Diabetic nephropathy was defined as persistent micro- or macroalbuminuria most likely secondary to diabetes. 13 Diabetic retinopathy was defined as retinopathy secondary to diabetes, including nonproliferative retinopathy (mild, moderate, or severe), proliferative retinopathy, or macular edema. 14 If linked offspring data were not available, maternal data were still included. CGM data metrics were not uniformly collected at all participating sites, so these data were not analyzed. All data were stored in a deidentified format in a secure REDCap database, housed at Melbourne Health.
Continuous subcutaneous insulin infusion device and CGM eligibility
Continuous subcutaneous insulin infusion devices (insulin pumps) are not subsidized in Australia and are largely obtained through private health insurance or less commonly through philanthropic organizations. Since 2018, Australian women with T1D have been able to access fully subsidized CGM products in pregnancy through the National Diabetes Services Scheme (NDSS). The NDSS is an Australian government program that provides support to people living with diabetes. Individuals are required to register with the NDSS to receive subsidized diabetes supplies, including glucose monitoring strips, needles, insulin, and CGM products. Eligible products at the time of the study included Abbott Freestyle Libre and Freestyle Libre2, Dexcom G4, G5, and G6, and Medtronic Guardian Connect and Guardian Sensor 3 and 4.
Outcome measures
The primary outcome was the change in HbA1c from baseline (defined as mean HbA1c measured in the first trimester of pregnancy) to the third trimester of pregnancy. Prespecified secondary outcomes included mean HbA1c in the first, second, and third trimesters, mean HbA1c for the pregnancy overall, and the odds of women who achieved an HbA1c of ≤6.5% and ≤7.0% in the third trimester of pregnancy. Maternal outcomes included gestational hypertension, preeclampsia, maternal length of stay, and cesarean section delivery stratified by parity. Given that the delivery method in prior pregnancies was not collected, cesarean sections in primiparous women were primary cesarean sections, but cesarean sections in multiparous women may have been either primary or repeat procedures. Gestational hypertension was defined as new-onset hypertension (systolic BP ≥140 mm Hg and/or diastolic BP ≥90 mm Hg) after 20 weeks of gestation, and preeclampsia was defined as new-onset hypertension after 20 weeks of gestation with new-onset renal, liver, hematological, neurological, or placental involvement. 15 Maternal length of stay was defined as the total number of days the birth mother was hospitalized for the admission, including the birth.
Neonatal outcomes included gestational age at delivery, birthweight, preterm birth (<37 completed weeks of gestation), LGA (birthweight ≥90% centile using national growth charts), small-for-gestational-age (SGA, birthweight ≤10% centile using national growth charts), macrosomia (birthweight ≥4000 g), neonatal hypoglycemia requiring intravenous dextrose, neonatal respiratory distress, neonatal intensive care unit (NICU) length of stay, and neonatal hospital length of stay. We prespecified the use of both national growth charts and GROW (gestation-related optimal weight)-customized birthweight centiles to report the proportion of SGA and LGA offspring. National growth charts are based on Australian population birthweight data excluding iatrogenic preterm deliveries for SGA, which therefore increases the median birthweight in these charts. 16 Both national growth charts and GROW charts adjust for neonatal sex and gestational age at birth, but GROW charts also adjust for maternal height and weight, parity, and ethnicity, 17 which may be important determinants of neonatal birthweight in a multiethnic Australian cohort. Neonatal respiratory distress was defined as one or more signs of increased work of breathing, such as tachypnea, nasal flaring, chest retractions, or grunting requiring respiratory observation or support. 18 Neonatal length of stay was defined at the total length of hospital admission, including the days spent in the NICU and special care nursery (SCN).
Statistical analysis
Based on the mean (standard deviation [SD]) decrease in HbA1c between randomization (<13 + 6 weeks of gestation) and 34 weeks of gestation in CONCEPPT of 0.54% (0.62) in the CGM group and 0.35% (0.65) in the control group, to achieve 90% power at a two-side significance level, 470 participants (230 in each group) would be required.
Baseline data are presented as mean (SD), median (interquartile range, IQR), or number of participants (percentage within the group, %) unless indicated otherwise. Changes in HbA1c from the first to the third trimester were compared between CGM users and non-CGM users using the Wilcoxon rank-sum test. Adjusted associations between CGM use and change in HbA1c were examined using linear regression models accounting for first-trimester HbA1c and insulin regimen. Logistic regression adjusted for first-trimester HbA1c and insulin regimen was used to estimate adjusted ORs with 95% CIs for achieving third-trimester HbA1c targets (≤6.5% and <7.0%) in CGM users compared with non-CGM users. Multivariable logistic regression models were used to estimate adjusted ORs with 95% CIs for binary maternal and neonatal outcomes, including LGA, SGA, macrosomia, and cesarean section. These models adjusted for first-trimester HbA1c, first-trimester BMI, insulin regimen, parity, and year of delivery. Adjusted differences in mean birthweight were assessed using multivariable linear regression with the same covariates. Proportions between groups were compared using Fisher’s exact test or Pearson’s chi-squared test, as appropriate. The median (quantile) regression was used to analyze length-of-stay data as they were skewed.
Results
Of the 951 women recruited to the study, 456 (48%) were CGM users. Overall, 841 (88.4%) women provided written informed consent, while 110 (11.6%) were included via an approved opt out consent process. Baseline characteristics are shown in Table 1. There was no difference between CGM users and CGM nonusers in the mean (SD) maternal age (31.6 [4.6] vs. 31.3 [4.7] years, P = 0.32) and BMI (27.1 [5.9] vs. 27.0 [5.7] kg/m2, P = 0.79). There was also no difference in the median (IQR) duration of T1D (17.4 [12.9] vs. 16.9 [13.3] years, P = 0.66). The cohort was predominately Australian born (80.7%) and multiparous [median (IQR] 2.0 [2.0]).
Baseline Characteristics of Pregnant Women with Type 1 Diabetes Using Continuous Glucose Monitoring Versus Those Not Using Continuous Glucose Monitoring
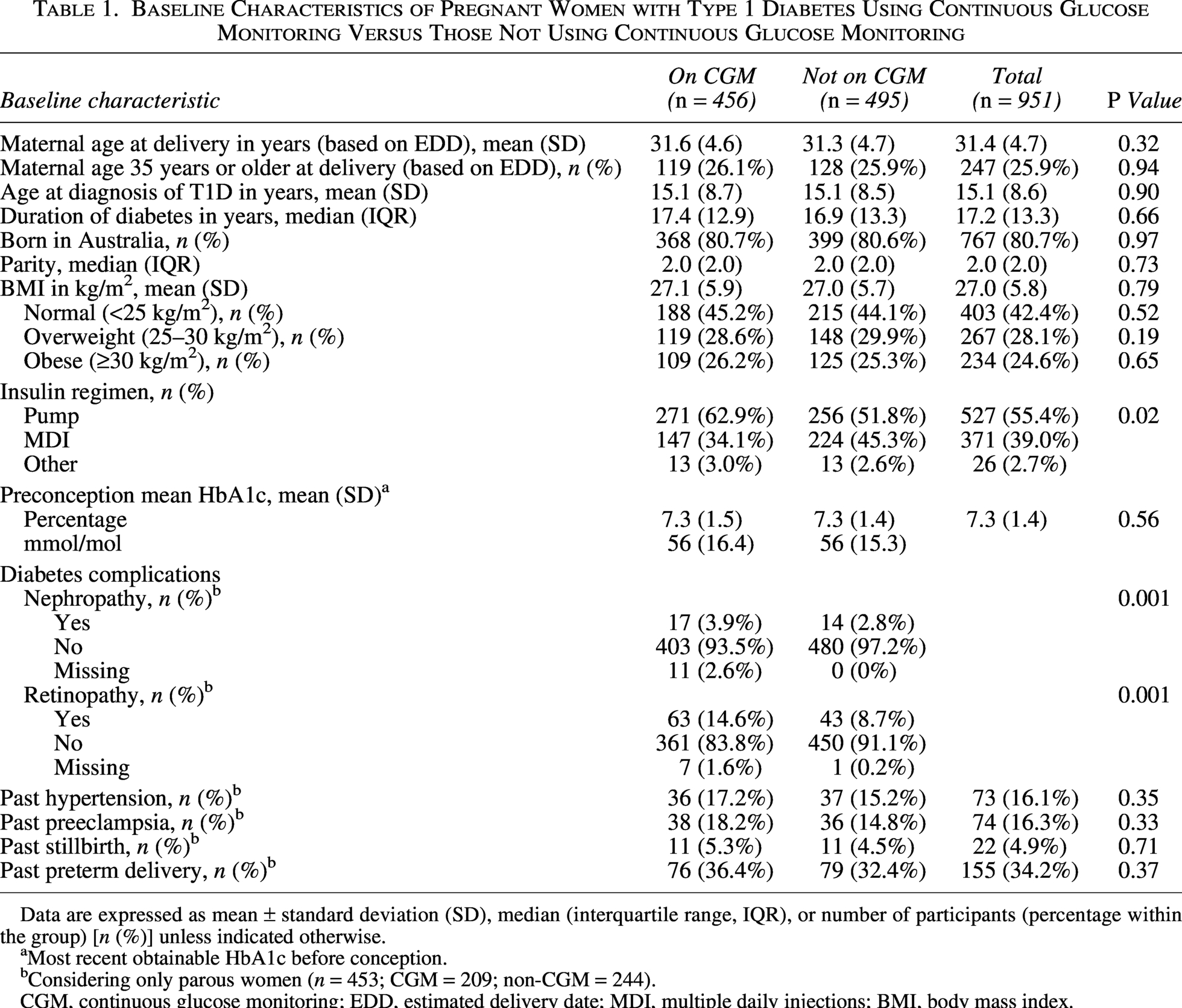
Data are expressed as mean ± standard deviation (SD), median (interquartile range, IQR), or number of participants (percentage within the group) [n (%)] unless indicated otherwise.
Most recent obtainable HbA1c before conception.
Considering only parous women (n = 453; CGM = 209; non-CGM = 244).
CGM, continuous glucose monitoring; EDD, estimated delivery date; MDI, multiple daily injections; BMI, body mass index.
Considering the most recent obtainable HbA1c before conception, there was no difference in mean (SD) preconception HbA1c between CGM users and nonusers (7.3 [1.5] vs. 7.3 [1.4]%, P = 0.56). Significantly more CGM users than non-CGM users used an insulin pump for insulin administration (62.9% vs. 51.8%, P = 0.02). Significantly more CGM users than non-CGM users had preexisting diabetes microvascular complications, including nephropathy (3.9% vs. 2.8%, P = 0.001) and retinopathy (14.6% vs. 8.7%, P = 0.001). There was no difference between the groups in the presence of preexisting hypertension (17.2% vs. 15.2%, P = 0.35) or previous adverse pregnancy events such as preeclampsia, stillbirth, and preterm delivery.
In adjusted linear regression models accounting for first-trimester HbA1c and insulin regimen (pump vs. multiple daily injection [MDI]), CGM use remained independently associated with a greater reduction in HbA1c over pregnancy (adjusted mean difference −0.20%, 95% CI: −0.40 to 0.00, P = 0.037). First-trimester HbA1c was the strongest predictor of HbA1c change (−0.57%, 95% CI: −0.59 to −0.54, P < 0.001), while pump use (pump vs. MDI) was associated with a smaller reduction in HbA1c (adjusted mean difference −0.10%, 95% CI: 0.03–0.17, P = 0.008) (Supplementary Table S1).
In multivariable analyses adjusting for first-trimester HbA1c and pump use (pump vs. MDI), CGM use was not associated with achieving HbA1c ≤6.5% (adjusted OR 1.008, 95% CI: 1.000–1.015, P = 0.055) nor was it associated with achieving HbA1c ≤7.0% (adjusted OR 1.001, 95% CI: 0.993–1.009, P = 0.766). First-trimester HbA1c remained the strongest predictor of achieving these targets (adjusted OR 0.313. 95% CI: 0.272–0.360, P < 0.001). Pump use (vs. MDI) was associated with lower odds of achieving HbA1c ≤6.5% (adjusted OR 0.752, 95% CI: 0.575–0.984, P = 0.037) but was not significantly associated with achieving ≤7.0% (adjusted OR 0.748, 95% CI: 0.551–1.015, P = 0.062) (Supplementary Tables S2–S3).
CGM use increased over time during the 10-year study period. This change occurred in both pump users and those using multidose injections (Supplementary Table S4A–B). As shown in Supplementary Table S4C, the observed improvements in HbA1c were attributable to CGM use rather than other changes in clinical diabetes management.
As shown in Table 2, mean HbA1c levels decreased progressively across pregnancy in both CGM users and nonusers with more than half of both groups achieving HbA1c ≤6.5% by the third trimester of pregnancy. There was no difference between CGM users and nonusers in the proportion of women who developed gestational hypertension (17.1% vs. 16.4%, P = 0.74) or preeclampsia (19.7% vs. 16.6%, P = 0.21). Among primiparous women, 140/207 (67.6%) of CGM users underwent cesarean section compared with 191/249 (76.7%) of nonusers. The unadjusted analysis suggested lower odds of cesarean section among CGM users (OR 0.63, 95% CI: 0.42–0.96), and this association was strengthened after adjustment for first-trimester HbA1c, first-trimester BMI, insulin regimen, and year of delivery (adjusted OR 0.22, 95% CI: 0.08–0.58, P = 0.002). In contrast, there was no difference in the cesarean section rate between groups in multiparous women (160/209 [76.6%] vs. 170/244 [69.7%], adjusted OR 2.01, 95% CI: 0.91–4.43, P = 0.08) (Supplementary Table S5). There was no difference in the median (IQR) maternal hospital length of stay between groups (6.0 [4.5] vs. 6.0 [4.2] P = 0.80). Multivariable factors affecting maternal length of stay included prepregnancy hypertension (1.20, 95% CI: 0.42–1.97, P = 0.003) and gestational age at delivery in weeks (−0.70, 95% CI: −0.93 to −0.48, P < 0.001) (Supplementary Table S6).
Comparison of Maternal Outcomes in Pregnant Women with Type 1 Diabetes Using Continuous Glucose Monitoring Versus Those Not Using Continuous Glucose Monitoring
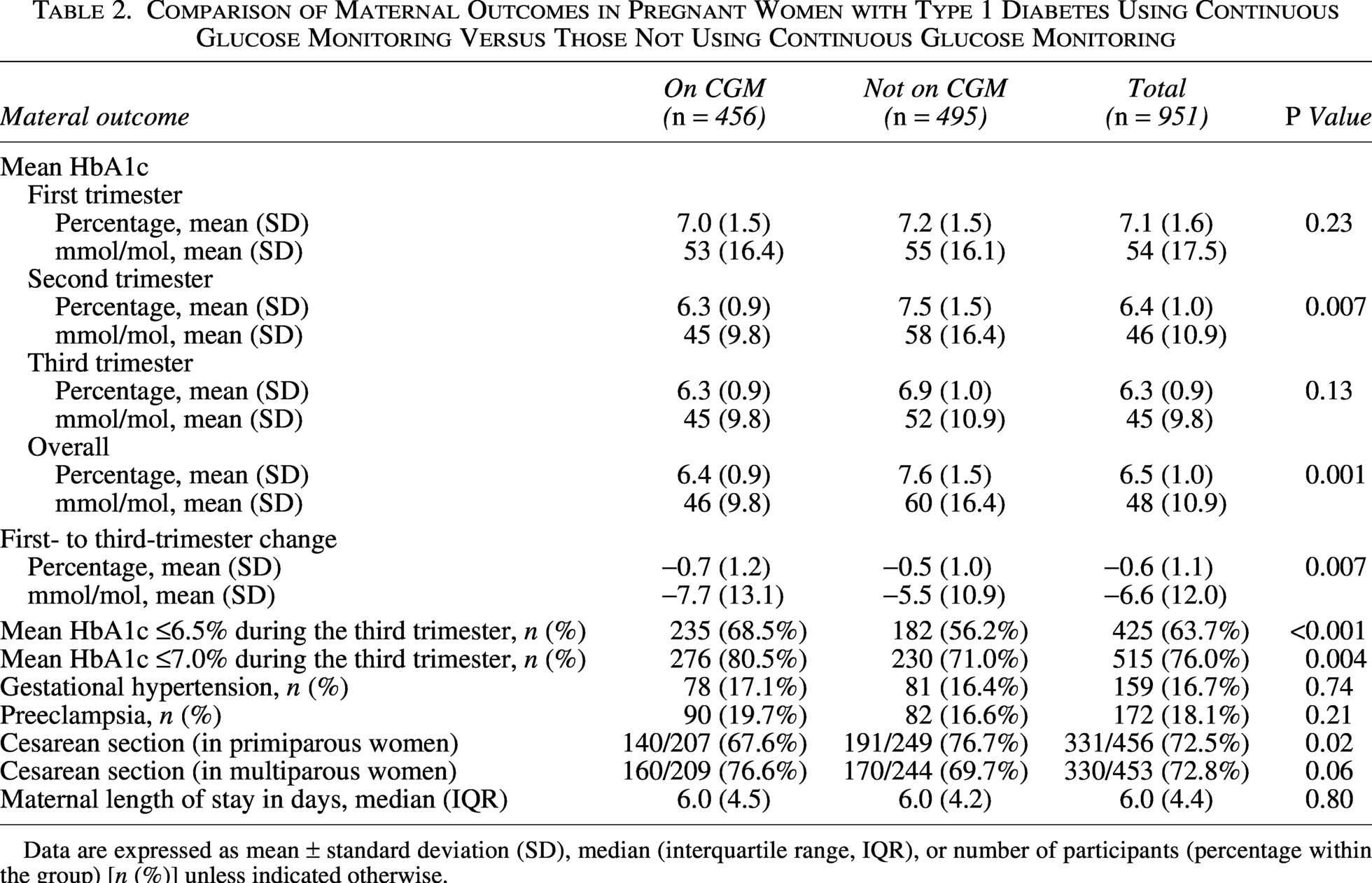
Data are expressed as mean ± standard deviation (SD), median (interquartile range, IQR), or number of participants (percentage within the group) [n (%)] unless indicated otherwise.
As shown in Table 3, there was no difference in mean (SD) birthweight between CGM users and nonusers (3506 [700] vs. 3598 [739] g, P = 0.05). In multivariable logistic regression analysis adjusting for mean first-trimester HbA1c, first-trimester BMI, insulin regimen (pump vs MDI), parity, and year of delivery, the adjusted mean difference in birthweight was −132 g (95% CI: −303 to 39 g, P = 0.13) (Supplementary Table S7). Using GROW customized centiles, median (IQR) birthweight centiles were similar between groups (96.1 [30.5] vs. 97.2 [21.3], P = 0.20). CGM use was not associated with lower odds of LGA based on national birthweight centiles (33.3% vs. 38.2%; adjusted OR 0.99, 95% CI: 0.50–1.95, P = 0.97) or GROW-customized centiles (adjusted OR 0.73, 95% CI: 0.43–1.24, P = 0.25). There was no difference in SGA between CGM users and nonusers using national growth charts (1.1% vs. 1.6%, adjusted OR 1.12, 95% CI: 0.17–7.61, P = 0.91) or GROW-customized centiles (3.4% vs. 3.4%, adjusted OR 1.25, 95% CI: 0.33–4.75, P = 0.75). There was also no significant difference in the rate of macrosomia (birthweight >4000 g) (adjusted OR 0.84, 95% CI: 0.45–1.57, P = 0.58). Overall, these findings indicate that while CGM use was associated with improved glycemic control, there was no measurable effect on birthweight, LGA, SGA, or macrosomia (Supplementary Table S8A–E).
Comparison of Neonatal Outcomes in Pregnant Women with Type 1 Diabetes Using Continuous Glucose Monitoring Versus Those Not Using Continuous Glucose Monitoring
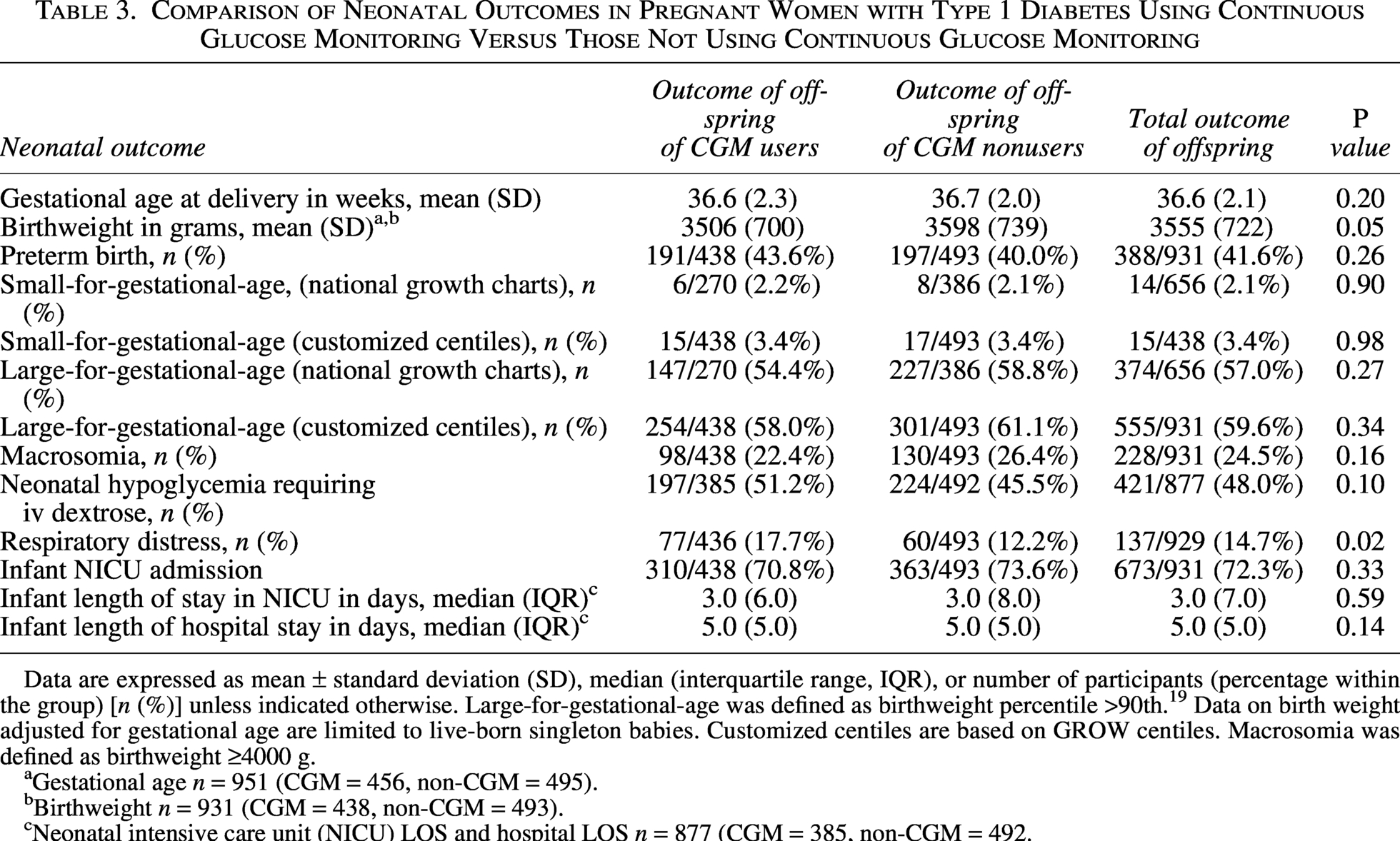
Data are expressed as mean ± standard deviation (SD), median (interquartile range, IQR), or number of participants (percentage within the group) [n (%)] unless indicated otherwise. Large-for-gestational-age was defined as birthweight percentile >90th. 19 Data on birth weight adjusted for gestational age are limited to live-born singleton babies. Customized centiles are based on GROW centiles. Macrosomia was defined as birthweight ≥4000 g.
Gestational age n = 951 (CGM = 456, non-CGM = 495).
Birthweight n = 931 (CGM = 438, non-CGM = 493).
Neonatal intensive care unit (NICU) LOS and hospital LOS n = 877 (CGM = 385, non-CGM = 492.
The mean (SD) gestational age at delivery did not differ between CGM users and nonusers (36.6 [2.3] vs. 36.7 [2.0] weeks, P = 0.20), nor did the proportion of offspring born preterm (43.6% vs. 40.0%, P = 0.26). There was no difference between CGM users and nonusers in the proportion of neonates with hypoglycemia requiring treatment with intravenous dextrose (51.2% vs. 45.5%, P = 0.10). CGM users had a higher proportion of infants with neonatal respiratory distress (17.7% vs 12.2%, P = 0.02). Median (IQR) length of stay (in days) in the NICU was not different between groups (3.0 [6.0] vs. 3.0 [8.0] P = 0.59), nor was the neonatal length of hospital stay (5.0 [5.0] vs. 5.0 [5.0] days, P = 0.14). Multivariable analysis demonstrated that the neonatal length of stay was significantly impacted by gestational age at delivery (−3.33, 95% CI: −3.90 to −2.76 weeks, P < 0.001) (Supplementary Table S9). When those born preterm (<37 weeks of gestation) were excluded, there was no difference in the median (IQR) NICU length of stay between neonates born to CGM users and nonusers (1.0 [3.0] vs. 2.0 [4.0] days, P = 0.41), but the neonates born to CGM users had a significantly shorter hospital length of stay (4.0 [2.0] vs. 4.0 [2.0] days, P = 0.04). Although the median and IQR were similar between groups, the difference remained statistically significant, indicating a shift in the overall distribution of lengths of stay with fewer prolonged admissions among CGM users.
Discussion
To our knowledge, this is the first population-based study in Australia evaluating the real-world impact of CGM on pregnancy outcomes in women with T1D. Of the 135,000 Australians living with T1D, around 1000 women have a pregnancy resulting in a live birth per year. 19 Based on these numbers, this study captured ∼10% of the pregnancies in Australian women with T1D within the period of interest.
In CONCEPTT, CGM users had a greater decrease in mean (SD) HbA1c between early pregnancy and 34 weeks of gestation than non-CGM users after adjustment for insulin regimen (pump or MDI) and baseline HbA1c (adjusted mean difference −0.19%; 95% CI: −0.34 to −0.03; P = 0.0207). In this study, CGM use remained independently associated with a greater reduction in HbA1c between the first and third trimesters of pregnancy after adjustment for insulin regimen (pump vs. MDI) and first-trimester HbA1c, with a magnitude of difference that was almost identical to CONCEPTT (adjusted mean difference −0.20%, 95% CI: −0.40 to 0.00, P = 0.037).
The baseline characteristics of this study were similar to CONCEPTT with respect to mean maternal age, duration of T1D, parity, ethnicity, and BMI. 6 For the baseline mean (SD) HbA1c, the large SDs in both CGM users and nonusers in this study (7.0% [1.5] vs. 8.1% [1.8]) compared with CONCEPTT (6.8% [0.7] vs. 7.0% [0.7]) suggest a wider variation of glycemic control. This may be due to differences in the cohorts recruited to clinical trials and real-world studies, with clinical trials having stricter inclusion criteria and real-world studies being more diverse in participants’ socioeconomic status, educational attainment, and medical comorbidities. Recognition of these differences is important in ensuring that real-world studies that are designed using data from clinical trials recruit sufficiently large cohorts to be adequately powered.
Multiple improvements in diabetes management occurred over the 10-year study period, but these data suggest that CGM use does contribute to improved glycemic control in pregnancy. Despite this, CGM use was not independently associated with achieving the glycemic targets of HbA1c ≤6.5% or ≤7.0% in this study. These HbA1c thresholds are roughly equivalent to the pregnancy-specific time in range (pTIR 3.5–7.8 mmol/L) 74% and 69%, respectively, 20 where pTIR ≥70% is recognized as the therapeutic target for glycemia in pregnancies complicated by T1D. 21 This suggests that CGM use in pregnancy may not fully offset the impact of higher first-trimester HbA1c on later glycemic outcomes. The predominant determinant of whether a woman achieves the glycemic targets in the third trimester of pregnancy is the first-trimester HbA1c. This further reinforces the potential importance of CGM in optimizing glycemic control before conception.
In an adjusted analyses accounting for first-trimester HbA1c, first-trimester BMI, insulin regimen, parity, and year of delivery, CGM use was not associated with lower odds of LGA using national birthweight centiles or GROW-customized centiles. This finding is discordant with CONCEPTT where the rate of GROW-defined LGA was significantly lower in CGM users than nonusers (53% vs. 69%, P = 0.02). The difference in study outcomes may reflect the more variable first-trimester glucose control and greater proportion of women with obesity in the CGM study arm (26% vs. 20%) in this real-world cohort compared with CONCEPTT, 6 with both factors being known to drive fetal overgrowth. Importantly, among CGM users in this study and CONCEPTT, the rates of LGA were 56% and 53%, respectively. This is more than five times the rate of the background population in Australia 19 and demonstrates substantial ongoing neonatal morbidity despite the glycemic improvements obtained with CGM use.
In both the present study and CONCEPTT, 6 there was no difference in the incidence of gestational hypertension or preeclampsia between CGM users and non-CGM users. While CONCEPPT data suggest that increasing time below range (<3.5 mmol/L) in the first trimester is associated with a higher risk of developing preeclampsia, 22 other data suggest that preeclampsia risk is associated with a higher periconception HbA1c. 23 As supported by this study and a recent Swedish cohort study, 24 the development of preeclampsia may not relate to glycemia per se but instead to a preexisting endothelial dysfunction, which is more common in women with long-standing T1D.
Although there was no difference in the proportion of offspring with neonatal hypoglycemia requiring intravenous dextrose administration between CGM users and nonusers, the rate of neonatal hypoglycemia in the present study was more than double than observed in CONCEPTT (51% vs. 15%). 6 This may reflect international differences in the management of hypoglycemia, with Australia more frequently using intravenous glucose to treat hypoglycemia than Europe and North America.6,25 Similarly, the admission criteria for SCN and NICU admission are variable across Australia. 25 This may partially explain why the present study found no difference in NICU admission rates between CGM users and nonusers, which differed from the findings of CONCEPTT. Although this study observed a significantly higher rate of respiratory distress among infants born to CGM users compared with nonusers (17% vs. 12%), this finding should be interpreted cautiously given that it is biologically improbable and a large number of exploratory secondary outcomes were examined.
In this real-world study, CGM use may have been influenced by a range of factors, including real and perceived clinical benefit, cost, and access to appropriate education.26,27 Women in this study who used CGM were more likely to be insulin pump users, likely reflecting better access to diabetes technology due to higher socioeconomic status and health literacy. 27 Women with diabetes complications were also more likely to use CGM, 28 potentially due to an awareness of the association between diabetes complication and adverse pregnancy outcomes.
The strengths of this study include its large sample size, which provides statistical power for a range of clinically important outcomes. The study cohort included women with T1D attending a large number of public maternity centers across Australia. 26 CGM users and nonusers were well-matched with respect to maternal age and diabetes duration. Given that CGM use was determined by patient preference, the results of this study likely reflect clinical outcomes expected with standard clinical care.
This real-world data study has a number of important limitations. It is highly likely that changes in both diabetes technology and clinical practice occurred over the study period time. The period of data collection included the introduction of a national subsidy for CGM. It is not possible to determine who accessed CGM using the subsidy, or the exact CGM start date. Self-management skills and uptake of diabetes education were not assessed, and we did not have data about medication use (including aspirin and betamethasone) or gestational weight gain. While HbA1c is not the preferred measure of glycemia in pregnancy due to increased erythrocyte turnover, the high prevalence of iron-deficiency anemia, and variable iron supplementation,29–31 it allows comparison of glycemic control between CGM users and nonusers. Women were considered CGM users or nonusers based on CGM use before 12 + 6 weeks of gestation. In those using CGM, the CGM use-time was not considered. Given that the CGM data metrics (pTIR, mean glucose, coefficient of variation) were not uniformly collected in CGM users at all the participating sites, these data were not analyzed.
To our knowledge, this is the first population-based real-world study to report the impact of CGM on glycemic and pregnancy outcomes in women with T1D. Reassuringly, the “real-world” outcomes are largely consistent with the published data from observational and randomized controlled trials. This study reinforces the critical role of CGM in improving glycemic and pregnancy outcomes.
Authors’ Contributions
S.A.L.P., M.C., and T.J. conceptualized the study. S.A.L.P., T.J., and M.C. designed the methodology. R.L.T., M.A.S.P., and J.J.C. collected the ENDIA data. S.A.L.P., M.C., and A.E. curated the data and conducted the formal analysis. S.A.L.P. wrote the original draft. All authors participated in the review and editing of the draft.
Author Disclosure Statement
No relevant disclosures to declare.
Footnotes
Acknowledgments
The authors gratefully acknowledge the funders of this project (Breakthrough T1D). The ENDIA Study Group comprises Pat Ashwood, Simon Barry, Maria E Craig, Peter G Colman, Elizabeth A Davis, Emma E Hamilton-Williams, Leonard C Harrison, Aveni Haynes, Tony Huynh, Ki Wook Kim, Kelly J McGorm, Grant Morahan, William D Rawlinson, Georgia Soldatos, Jason Tye-Din, Peter J Vuillermin, and John M Wentworth. The ENDIA Study Group thanks the institutions and individuals outlined in ![]() . The authors acknowledge the Australasian Diabetes in Pregnancy Society for supporting the recruitment of maternity sites across Australia to the study. They also acknowledge the women and families who generously contributed data to this project.
. The authors acknowledge the Australasian Diabetes in Pregnancy Society for supporting the recruitment of maternity sites across Australia to the study. They also acknowledge the women and families who generously contributed data to this project.
Funding Information
Research reported in this publication was funded by
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.