
Abstract

Approximately 27 million adults in the United States have a diagnosis of type 2 diabetes (T2D). 1 For many years, metformin, sulfonylureas, and insulin were the mainstays of pharmacologic management. More recently, treatment options have expanded to include many additional drug classes, including thiazolidinediones, dipeptidyl peptidase 4 (DPP-4) inhibitors, incretin receptor agonists (including glucagon-like peptide-1 receptor agonists and dual glucagon-like peptide-1 receptor and glucose-dependent insulinotropic peptide agonists, which will be referred to as GLP-1ra drugs), and sodium–glucose cotransporter-2 inhibitors (SGLT2i). Data on the frequency of use of glucose-lowering medications for T2D become outdated quickly.
Analysis of the Epic Cosmos database provides an opportunity to assess up-to-date prescribing patterns. This database includes longitudinal records of data collected across U.S. health systems utilizing the Epic electronic health record for approximately 300 million patients receiving care at 2051 hospitals and 46,300 clinics 2 (as of March 17, 2026). The patients in the database closely mirror U.S. Census data for age, race, ethnicity, insurance coverage, and social vulnerability index. 2 We utilized the Epic Cosmos database to evaluate treatment patterns for T2D in the U.S. during 2025.
Methods
Cosmos data were obtained for the analyses, using structured query language queries of the Expertly Determined De-Identified data. Adults with a diagnosis code of T2D were identified in the database who were ≥18 years old, resided in the U.S., had at least two outpatient visits between January 1, 2023, and December 31, 2025, with at least one office or telemedicine visit in 2025, and had a prescription for a glucose-lowering medication during 2025. Patients who were pregnant during 2025 were not included. Glucose-lowering medications prescribed as an outpatient during 2025 (excluding medications prescribed during an inpatient hospital stay or on hospital discharge) were identified in the database and tabulated.
Results
There were 1,928,614 adults with a diagnosis code of T2D who had an encounter and at least one outpatient prescription for a glucose-lowering medication in 2025 (Supplementary Table S1). Metformin was prescribed for 59.6% and used as the only treatment in 20.3%. GLP-1 drugs were prescribed for 40.7%, SGLT-2i drugs for 28.4%, and sulfonylureas for 16.1%. Other non-insulin glucose-lowering drugs were prescribed for 10% or fewer patients (Table 1). Insulin was prescribed for 26.1% of the cohort. A long-acting basal insulin without short or rapid-acting insulin was prescribed for 11.4% and a long-acting basal insulin plus a rapid-acting analogue insulin in 10.2%. Except for lower frequencies of insulin and GLP1ra drugs and higher frequency of metformin in Asian patients, differences in prescribing patterns among races and Hispanic ethnicity were small (Supplementary Table S2). There were some differences in prescribing patterns according to payor type, most notably GLP-1ra being higher and insulin lower with commercial insurance and GLP-1ra being lower and metformin and sulfonylureas higher in self-pay (Supplementary Table S3). Only 15.5% of the patients were seen by an endocrinologist during 2025.
Glucose-Lowering Treatments Prescribed in 2025 (N = 1,928,612)
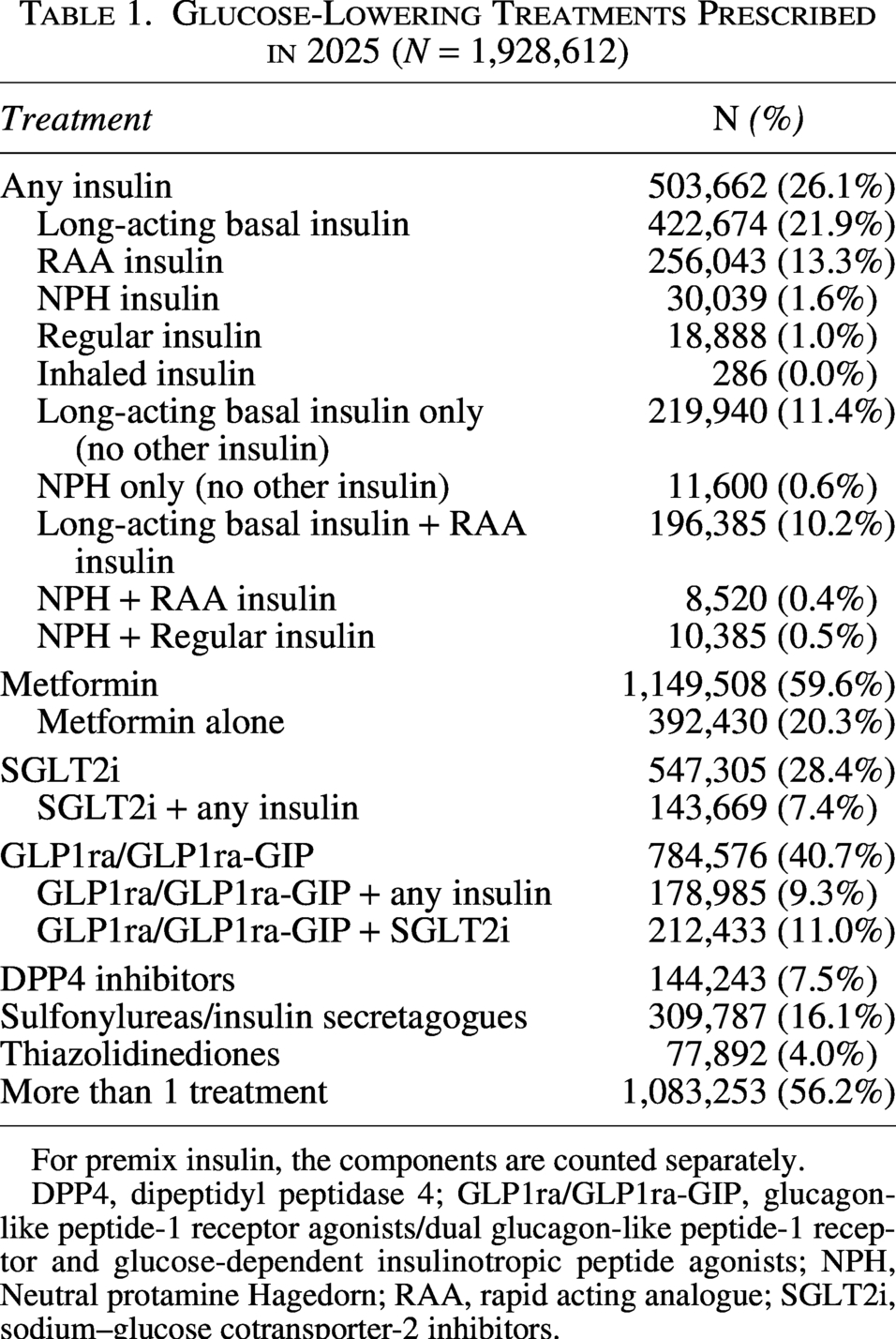
For premix insulin, the components are counted separately.
DPP4, dipeptidyl peptidase 4; GLP1ra/GLP1ra-GIP, glucagon-like peptide-1 receptor agonists/dual glucagon-like peptide-1 receptor and glucose-dependent insulinotropic peptide agonists; NPH, Neutral protamine Hagedorn; RAA, rapid acting analogue; SGLT2i, sodium–glucose cotransporter-2 inhibitors.
Conclusions
The Epic Comos data provide current information on how T2D is being treated in a representative population of adults in the US. Insulin use in 2025 was less than in 1994, when it was estimated to be 38%, but about the same as it was in 2007, when it was estimated to be 28% in a study that utilized the National Disease and Therapeutic Index. 3 That study also found that in 2007 metformin use was 54%, sulfonylureas 34%, thiazolidinediones 28%, and DPP-4 inhibitors 8%. The NHANES data showed insulin use to be 18.4% in 1999–2002 and 25.7% in 2015–2018. 4 Other glucose-lowering medication use in the 2015–2018 survey was 59.5% metformin, 24.4% sulfonylurea, 10.8% DPP-4 inhibitor, 7.1% GLP-1ra or SGLT2i, and 3.3% thiazolidinediones. More recent data show the expansion of use of GLP-1ra drugs, with a frequency of 26.5% in the 2024 National Health Information Survey data. 5 The GLP-1ra frequency in the 2025 Epic Cosmos data is even higher at 40.7%. Concomitant with the increase in GLP-1ra and SGLT2i drugs, there has been a decrease in the prescribing of sulfonylureas compared with the 2015–2018 survey.
The data presented herein demonstrate the power of using the Epic Cosmos database to provide data on current treatment patterns of T2D in a patient population representative of US adults. The data are also informative in showing that an endocrinologist was seen during 2025 by only a small proportion of these patients, and GLP-1ra and SGLT-2i drugs were prescribed in less than half of patients despite the known benefit of these drugs on cardiovascular and renal disease.
Authors’ Contributions
T.L.B., I.B.H., and R.W.B. developed the design for the study. T.L.B. performed the analyses. T.L.B., I.B.H., and R.W.B. wrote the article. All authors approved the final version of the article. All authors are guarantors of the article content.
Data Sharing Statement
The authors are not able to share the data used in the analyses as they are part of the EPIC database.
Footnotes
Author Disclosure Statement
T.L.B. reports no personal financial disclosures. I.B.H. reports grant funding to his institution from Sequel Med Tech and Mannkind and consulting fees from Abbott, Roche, and Hagar. R.W.B. reports no personal financial disclosures but reports that his institution has received funding on his behalf as follows: grant funding, study supplies, and consulting fees from Insulet and Tandem Diabetes Care; grant funding and study supplies from Dexcom and Abbott; grant funding from Bigfoot Biomedical, Sequel Med Tech, and MannKind; study supplies from Medtronic; consulting fees and study supplies from Novo Nordisk; and consulting fees from BetaBionics, Hagar, DreaMed, Ypsomed, Eli Lilly, and Zucara.
Funding Information
The study was conducted without a funding source.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.