
Abstract
Objective:
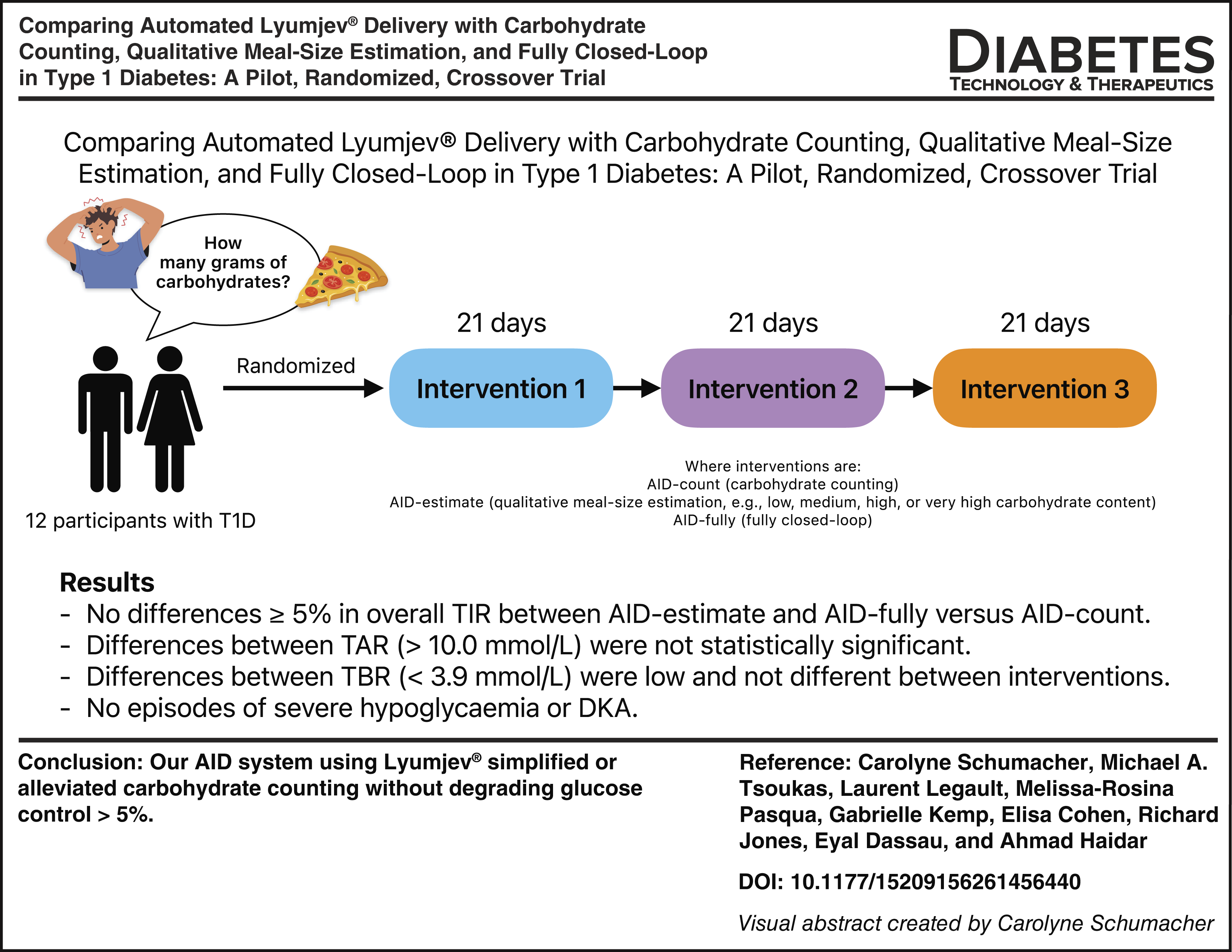
Determining prandial insulin needs by carbohydrate counting is a challenging task for many people with type 1 diabetes (PwD). We developed a novel automated insulin delivery (AID) system using ultrarapid lispro insulin (Lyumjev®), replacing carbohydrate counting with qualitative meal-size estimation and meal detection.
Research Design and Methods:
We performed a randomized crossover pilot trial comparing 3 weeks of AID with carbohydrate counting (AID-count) with (i) AID with qualitative meal-size estimation (i.e., defining a meal as low, medium, high, or very high in carbohydrate content; AID-estimate) and (ii) AID with meal detection (i.e., fully closed-loop; AID-fully) in adults with type 1 diabetes (T1D). The trial was registered (NCT06021158).
Results:
Twelve participants completed the study (eight females; mean [SD]: age 38 [16] years, HbA1c 7.0% [0.7], total daily insulin dose 0.64 [0.22] U/[kg·d]). There were no differences greater than 5% in the overall time in range between AID-estimate and AID-fully compared with AID-count, and thus the differences were not considered clinically significant based on the international consensus on time in range (AID-count vs. AID-estimate: 75.4% [16.3] vs. 72.9% [13.2], P = 0.191; AID-count vs. AID-fully: 75.4% [16.3] vs. 71.0% [10.6], P = 0.192). The differences in time spent in hyperglycemia were not statistically significant, and the times spent in hypoglycemia were low and not different between interventions. There were no episodes of severe hypoglycemia or diabetic ketoacidosis in any intervention.
Conclusions:
In this pilot study, the AID system using Lyumjev simplified or alleviated carbohydrate counting without degrading glucose control more than 5%. Larger studies are warranted.
Keywords
Introduction
One of the primary challenges in maintaining strict glucose control for people with type 1 diabetes (PwD) occurs at mealtimes. Most commercial automated insulin delivery (AID) systems require prandial insulin boluses based on the carbohydrate content of each meal to be consumed. 1 However, accurately quantifying carbohydrates is a challenging and burdensome task for many. Two out of three PwD underestimate their prandial insulin needs, leading to postprandial glucose excursions. 2 A meal’s fat and protein content also influences postprandial glucose levels, making precise prandial insulin dosing even more complicated. 3 Furthermore, PwD often standardize their meals to simplify carbohydrate counting, which can negatively affect their food choices. 4 The emphasis on carbohydrate counting complicates diabetes management because it is time-consuming and stressful, prompting many to pursue innovative technologies that simplify the carbohydrate-counting process. 5
Ultrarapid lispro insulin (Lyumjev®; Eli Lilly and Company, IN, USA) is the fastest-acting lispro insulin available today and the closest to mimicking endogenous insulin activity. 6 With an onset of 5 min, it offers tighter glucose control in PwD by shortening postprandial glucose excursions without an increase in hypoglycemia. 7 A randomized, double-blind crossover study compared hyperglycemia recovery after Lyumjev versus rapid-acting lispro insulin (Humalog®) injection in 32 adults on insulin pump therapy, and the results from both interventions indicate that, compared with Humalog, Lyumjev reduced maximum postprandial glucose levels, produced a faster postprandial glucose decline, and a shortened recovery from hyperglycemia. 8 Lyumjev was also tested with AID systems such as CamAPS FX and Control-IQ technology, and showed a slight but statistically significant improvement in glucose control compared with Humalog.9–11
We have developed an AID system that replaces traditional carbohydrate counting with qualitative meal-size estimation (i.e., selecting a category of low, medium, high, or very high corresponding to the estimated carbohydrate content of the meal) and meal detection (i.e., consuming food without notifying the system about a meal). This system utilizes Lyumjev. Here, we present the results of a pilot, randomized, crossover trial that assesses this system by comparing it with an AID system with carbohydrate counting in 12 adult individuals with T1D.
Research Design and Methods
Study design
This was a randomized, three-way, crossover outpatient pilot trial assessing (i) an AID system with carbohydrate counting (AID-count), (ii) an AID system with qualitative meal-size estimation (AID-estimate), and (iii) an AID system with meal detection (AID-fully). Each arm lasted 21 days, and Lyumjev was used in all interventions. The interventions were separated by a washout period of 3 to 14 days, during which participants returned to their usual insulin therapy.
Participants were recruited at the McGill University Health Centre in Montreal, Canada. Eligible adults (≥18 years) were those with T1D for at least 12 months, had used an insulin pump for at least 3 months, had not used oral antihyperglycemic agents for at least 2 weeks, avoided glucocorticoids and hydroxyurea (due to its potential to interfere with the accuracy of CGM readings), had no planned or ongoing pregnancy or breastfeeding, experienced no severe hypoglycemia or diabetic ketoacidosis in the past month, and had no clinically significant retinopathy, nephropathy, or neuropathy. They also did not have any acute macrovascular events in the last 6 months and had no known hypersensitivity to the study drug or its excipients. Participants provided written informed consent.
This trial received approval from the local research ethics board and followed the ICH Guideline for Good Clinical Practice and the Declaration of Helsinki.
Randomization
Blocked randomization of size six was used to generate the allocation sequences, which were revealed to the study coordinator and the participant upon confirmation of study enrollment.
Masking
The research staff and participants were not blinded.
Study procedures
During each 21-day intervention, participants utilized an AID system consisting of an investigational YpsoPump® insulin pump (Ypsomed AG, Burgdorf, Switzerland), a Dexcom G6® continuous glucose monitor (Dexcom, Inc., CA, USA), and McGill University’s euClide application installed on a Google Pixel® 2 cellphone (Google LLC, CA, USA).
The euGlide application included a dosing algorithm that adjusted basal rates every 10 min and was initialized with the participants’ usual basal rates, total daily insulin dose (TDD), insulin sensitivity factors, and carbohydrate ratios. Glucose targets were set at 5.5 mmol/L (99 mg/dL) unless the participant temporarily enabled the exercise function, which raised the targets to 8.5 mmol/L (153 mg/dL). Participants could administer correction boluses at any time. Based on premeal glucose levels and insulin on board, the system increased or decreased insulin doses at mealtimes. It did not provide automated correction boluses outside mealtimes; instead, it managed glucose levels by adjusting the basal rates (e.g., 6 U/h for 10 min delivers 1 U).
During the AID-count intervention, participants manually entered the carbohydrate content of their meals into the system, and the algorithm calculated prandial boluses based on their insulin-to-carbohydrate ratios. This intervention resembles the first-generation AID systems currently available in the market.
During the AID-estimate intervention, participants were directed to select from a drop-down menu a meal-size category (ranging from low, medium, high, to very high in carbohydrate content) that corresponded to the estimated carbohydrate content of their meal. These meal-size categories were prematched to numerical values that were personalized (e.g., medium-size meal is 50 g of carbohydrate for a particular participant) to reflect the participant’s typical eating habits, informed by a 24-h food recall, where participants were asked about their carbohydrate intake in grams at breakfast, morning snack time, lunch, afternoon snack time, dinner, and dessert. The same bolus calculator as in the carbohydrate counting intervention was used, except that the carbohydrate input values were predefined and restricted to four values (corresponding to four meal-size categories) for each participant.
During the AID-fully intervention, participants were instructed to eat without informing the system of their meal. The AID system administered one to three partial meal boluses upon detecting rising glucose levels approximately 20–50 min after meal ingestion. The partial boluses were separated by 30 min. Boluses were calculated in two steps. First, the probability that a meal was consumed was calculated based on current blood glucose levels, the amount of insulin on board, the time elapsed since the last bolus, and the rate of blood glucose change.12,13 If the meal probability crossed a predefined threshold, the three boluses were calculated using insulin-to-carbohydrate ratios and insulin sensitivity factors. 14 The first bolus was calculated to cover 20 g of carbohydrates, and to correct the glucose level to 6.0 mmol/L, and the second and third boluses were calculated to correct the glucose level to 6.0 mmol/L, considering insulin on board from previous boluses.
The study team conducted remote follow-ups and data reviews on days 2, 3, and 7 (±2 days) of each intervention to address potential technical issues with the system, document adverse events, and adjust therapy parameters (e.g., carbohydrate ratios, insulin sensitivity factors, basal rates) for safety reasons, if necessary. The study coordinator (C.S.) remained on call throughout the interventions to provide technical support.
Outcomes
Glycemic outcomes are reported using the last 14 days of each intervention. The two predefined comparisons were AID-count versus AID-estimate and AID-count versus AID-fully. The primary endpoint was the percentage of time spent in the target glucose range (3.9–10.0 mmol/L). Secondary endpoints included the percentage of time spent in various glucose ranges, glucose variability, and insulin delivery.
Sample size and statistical analyses
This pilot study was not powered to demonstrate statistically significant superiority or noninferiority. A sample size of 12 per intervention is a commonly accepted guideline for pilot studies when no prior information is available to determine an appropriate sample size. 15
Statistical analyses were conducted on a modified intention-to-treat basis: participants who did not complete all interventions were excluded from the primary and secondary outcome analyses, but they were included in the adverse events reporting. Glycemic and insulin outcomes were assessed for normality, and in cases of skewness, the Wilcoxon signed-rank test was used to assess statistical differences. If the data were not skewed, a paired t-test was used to assess statistical differences. P-values <0.05 were regarded as significant. Results are presented as mean (SD) or median [IQR].
The trial was registered at ClinicalTrials.gov (NCT06021158).
Data and resource availability
The raw data, including insulin delivery, glucose levels, and individual participant data, along with the informed consent form, can be shared by the corresponding author for academic purposes. This is contingent on a material transfer agreement and the approval of McGill University Health Center’s Research Ethics Board. All shared data will be deidentified.
Results
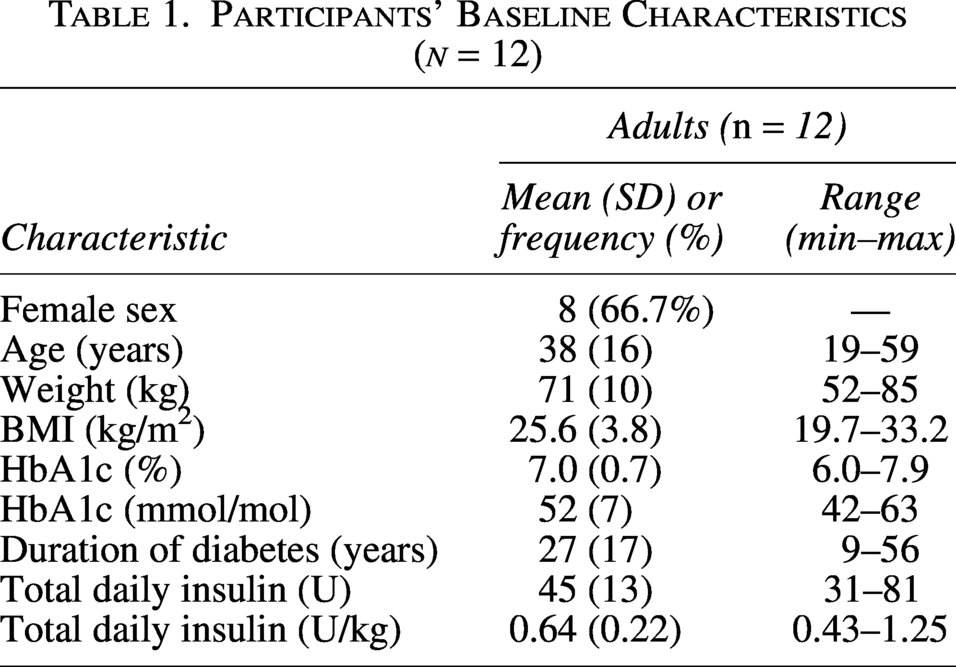
Fourteen participants were enrolled from December 20, 2023, to November 7, 2024 (Fig. 1). A total of 12 adults (eight females; mean [SD]: age 38 [16] years, HbA1c 7.0% [0.7], TDD 0.64 [0.22] U/[kg·d]) completed the study and were included in the analysis (Table 1). One participant withdrew on day 5 of the first intervention due to a possible adverse reaction to Lyumjev insulin, and another withdrew on day 3 of the first intervention due to discomfort using the experimental AID system.
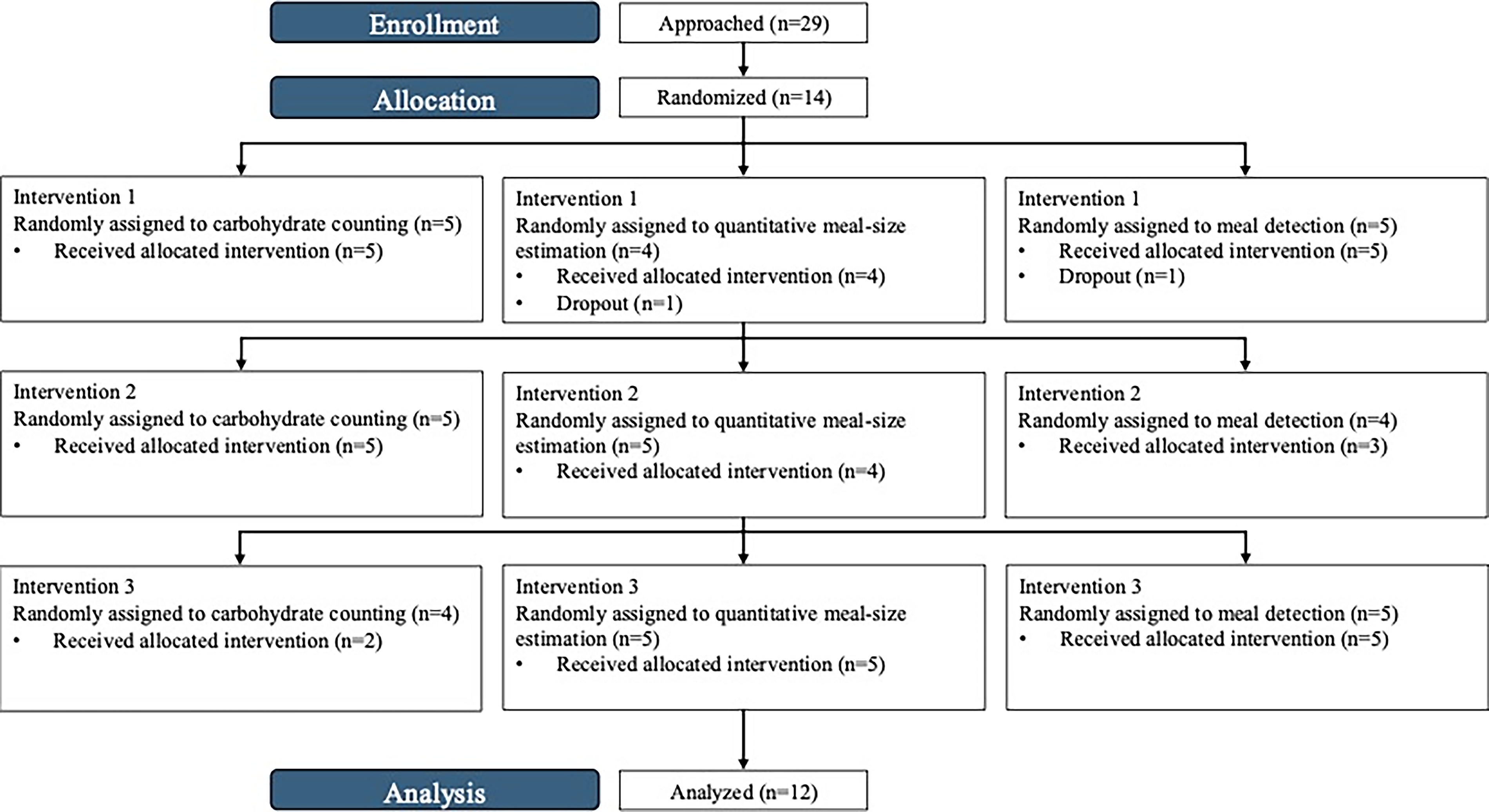
Trial profile.
Participants’ Baseline Characteristics (n = 12)
The AID system operated in closed-loop mode almost 100% of the time during each intervention (AID-count: 99.5% [99.4–99.9], AID-estimate: 99.2% [98.0–99.8], AID-fully: 99.6% [98.7–99.8]), with no difference observed (P > 0.05).
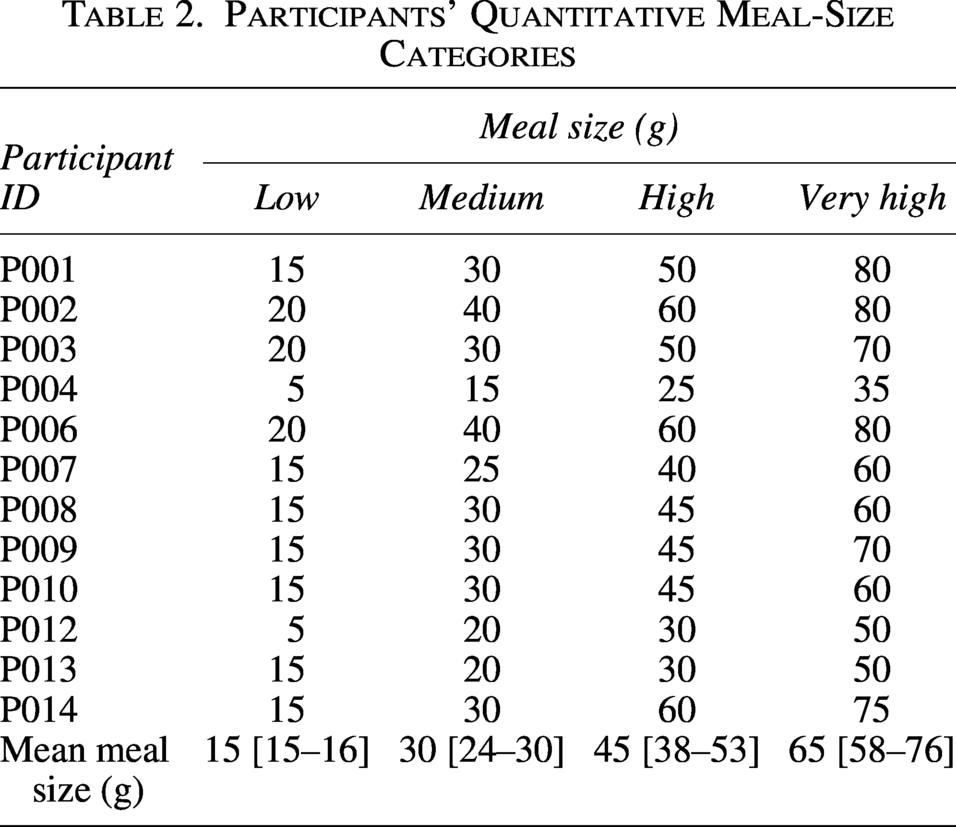
Table 2 presents the meal-size categories personalized for each participant in AID-estimate. The average value of a low, medium, high, and very high carbohydrate-content meal was 15 [15–16], 30 [24–30], 45 [38–53], and 65 g [58–76], respectively (Table 2).
Participants’ Quantitative Meal-Size Categories
The absolute differences in the overall time spent within the target glucose range between AID-count and AID-estimate (75.4% [16.3] vs. 72.9% [13.2], P = 0.191) and AID-count and AID-fully (75.4% [16.3] vs. 71.0% [10.6], P = 0.192) were not statistically significant and were not different by more than 5% (mean difference of 2.5% (6.1) vs. 4.4% (11.0), respectively). The percentage of time spent below 3.9 and 3.0 mmol/L was low in all interventions (medians <2.0% and <0.2%, respectively). The percentage of time spent above 10.0 mmol/L did not differ significantly between interventions (AID-count vs. AID-estimate: 23.2% [16.2] vs. 25.5% [13.2], P = 0.212; AID-count vs. AID-fully: 23.2% [16.2] vs. 27.0% [10.4], P = 0.269). Complete outcomes are provided in Table 3.
Comparison of Glucose and Insulin Outcomes Between Interventions
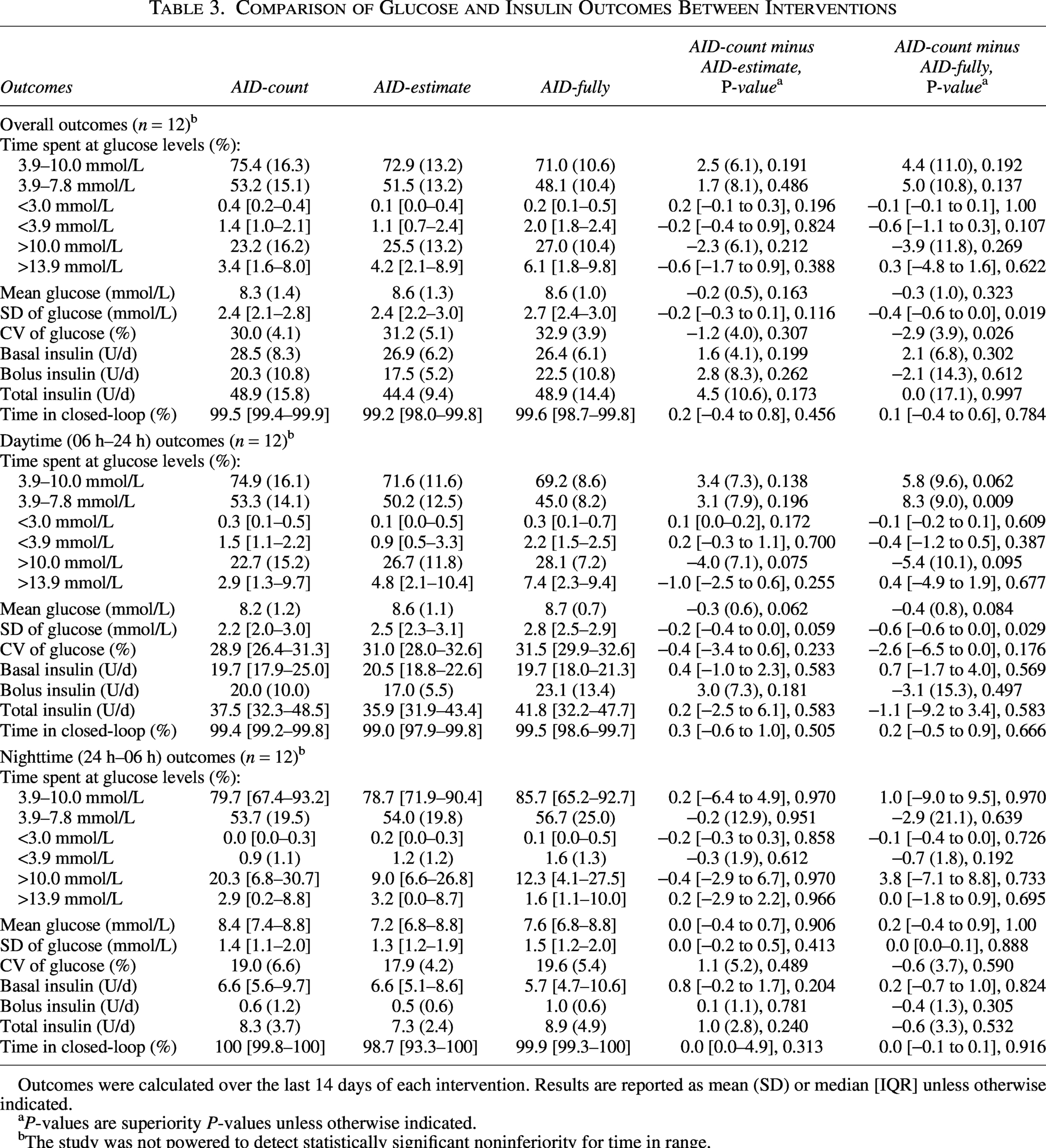
Outcomes were calculated over the last 14 days of each intervention. Results are reported as mean (SD) or median [IQR] unless otherwise indicated.
P-values are superiority P-values unless otherwise indicated.
The study was not powered to detect statistically significant noninferiority for time in range.
During the daytime, the differences in time spent in range between AID-count versus AID-estimate (74.9% [16.1] vs. 71.6% [11.6], P = 0.138) and AID-count versus AID-fully (74.9% (16.1) vs. 69.2% (8.6), P = 0.062) were not greater than 5%. During the nighttime, there were no differences in time spent in range between AID-count and AID-estimate (0.2 [−6.4 to 4.9], P = 0.970) and AID-count and AID-fully (1.0 [−9.0 to 9.5], P = 0.970). The percentage of time spent below 3.9 mmol/L and 3.0 mmol/L during the daytime and nighttime was low and comparable between interventions. Complete daytime and nighttime outcomes are provided in Table 2.
There was a small decrease in overall insulin dosage during AID-estimate (mean difference of 4.5 [10.6] U/d, P = 0.173) and no change in insulin dosage during AID-fully (mean difference of 0.0 [17.1] U/d, P = 0.997), although none of these differences was statistically significant. The reduction in total insulin dosage during AID-estimate was mostly attributed to a reduction in bolus insulin (reduction in bolus 2.8 [8.3] U/d, P = 0.262; reduction in basal 1.6 [4.1] U/d, P = 0.199). The average number of manual (participant-initiated) correction insulin boluses was 0.83 (0.69) with AID-count, 1.20 (0.92) with AID-estimate (P = 0.02 vs. AID-count), and 0.89 (1.62) with AID-fully (P = 0.34 vs. AID-count).
No serious adverse events were reported in any intervention. A total of 17 adverse events were reported; all but one (classified as moderate) were classified as mild. Five participants (36%) experienced stinging at the infusion site during mealtimes, three (21%) reported stinging at the infusion site when large boluses were administered (>4 U), one (7%) reported pain at the infusion site for 24 h following every catheter insertion, and one (7%) reported bleeding at the infusion site. One participant (7%) indicated allergic contact dermatitis likely related to the insulin and withdrew from the trial. One participant (7%) experienced gastrointestinal symptoms. There were no occurrences of severe hypoglycemia or diabetic ketoacidosis.
Conclusions
The automated Lyumjev delivery system with qualitative meal-size estimation and meal detection displayed small but no statistically significant differences in time in range compared with the automated Lyumjev delivery system with carbohydrate counting. This indicates that adequate glucose control with Lyumjev may be attained through meal strategies that simplify or alleviate the necessity for carbohydrate counting. However, as this trial is unpowered and pilot, a larger trial with a sample size chosen to achieve power to assess statistical significance is needed to adequately estimate the effect sizes of these differences. Moreover, evaluating the impact on quality of life using an automated Lyumjev delivery system, which incorporates qualitative meal-size estimation and meal detection with ultrarapid lispro insulin, is warranted.
Leohr et al. demonstrated that Lyumjev reduces recovery time from hyperglycemia compared with Humalog in PwD using continuous subcutaneous insulin infusion therapy. 8 Other studies have also shown the improved pharmacokinetics and glucodynamics of ultrarapid lispro insulin in patients with T1D7,16,17 and T2D. 18 This more rapid pharmacokinetics of Lyumjev could be incorporated in the closed-loop dosing algorithm explicitly through a mathematical model with a pharmacokinetic parameter (e.g., time to peak insulin action) or implicitly through a more aggressive dosing algorithm design or a more aggressive tuning of AID system parameters (e.g., insulin sensitivity factor determining correction boluses). In our study, the AID algorithm accounted for Lyumjev implicitly by delivering three postprandial boluses, separated by only 30 min, and, additionally, the study team adjusted systems parameters as needed on the follow-ups and data review remote visits. A quicker return to euglycemic levels is essential in a fully AID system that facilitates more liberal eating. Our data add to this body of literature and support the use of Lyumjev to timely correct hyperglycemia following meals with no prandial insulin boluses.
A 2.5% absolute reduction in time in range was observed between AID-count and AID-estimate. Whereas AID-estimate limited participants to four categories that differed by 15–20 g, AID-count allowed for more precise prandial bolus administration. A 4.4% absolute reduction in time in range was observed with AID-fully compared with AID-count. This was likely caused by the reactive nature of the meal detection algorithm, which administered up to three meal boluses in response to rising glucose levels typically detected 20–50 min after eating. Another reason for this reduction in time in range is that the participants could eat freely; as a result, they may not have made the most carbohydrate-conscious meal choices.
Several studies have evaluated simplified qualitative meal-size estimation and compared it with carbohydrate counting. Petrovski et al. demonstrated in two studies with 34 adolescents using the MiniMed™ 780 G system that while simplified qualitative meal-size estimation maintained glycemic control, precise carbohydrate counting resulted in superior time in range, even at a 12-month follow-up.19,20 The iLet bionic pancreas commercial system prompts users to announce meals as usual or more or less than usual, showed improved glycemic control compared with overall usual care, but no direct comparison was made to carbohydrate counting embedded in the bionic pancreas. 21 Haidar et al. and the accompanying commentary by Blervaque et al. investigated qualitative meal-size estimation in adults, revealing that while it also showed promise with high time in range, it was slightly inferior to carbohydrate counting.22,23 Our study corroborates with their findings, as we observed a slight reduction in time in range during AID-estimate compared with AID-count. A recent study by Laesser et al. found that simplified qualitative meal-size estimation was noninferior to carbohydrate counting in 46 adolescents and young adults using the CamAPS HX system and fast-acting insulin aspart (Fiasp®). 24 That their results contrast with the aforementioned studies could be due to a difference in dosing algorithms, insulin used, or sample size.
Another recent study assessed a fully closed-loop insulin system in outpatient free-living settings. Boughton et al. evaluated the CamAPS HX system with Lyumjev over 8 weeks in 26 adults with suboptimal glycemic control, showing that fully closed-loop improved time in the target glucose range compared with standard pump therapy with continuous glucose monitoring (50.0% (9.6) vs. 36.2% (12.2)). 25 Our fully closed-loop system showed a slight decrease in time in range without an increased risk of hypoglycemia compared with the closed-loop system with carbohydrate counting. However, because the CamAPS HX study did not compare their fully closed-loop system to a closed-loop system with carbohydrate counting, we cannot discern if their outcomes are comparable with ours.
A strategy using meal announcement alone, without any information on carbohydrate ingestion, which is not particularly burdensome, has the potential to outperform AID-fully. Thus, priming a fully closed-loop algorithm with a meal announcement would render the algorithm more reactive, thereby lowering the incidence of postprandial glucose excursions.
Adjunctive therapies such as glucagon-like peptide-1 receptor agonists, sodium/glucose transport protein 2 inhibitors, pramlintide, and glucagon have been studied in AID systems to simplify or alleviate carbohydrate counting, with promising results.26–32 However, their widespread use is limited by regulatory barriers, as they are not approved for use in PwD.
The study has several limitations. First, the short duration of each intervention does not adequately reflect the participants’ long-term adoption of the novel meal strategy. Second, the study was not sufficiently powered to determine noninferiority. Third, most participants recruited were highly motivated patients and frequent participants in insulin pump trials, which may introduce a bias toward more proficient carbohydrate counting. Therefore, a smaller difference in AID-count versus AID-fully may be observed in a real-world patient. On the contrary, the number of participant-initiated manual boluses in AID-estimate, but not AID-fully, was slightly higher than in AID-count. This raises the possibility that this group of highly motivated participants may have mitigated the information loss typical of fully closed-loop systems, which may not be representative of real-world patients who are less inclined to interact with the system. The study’s strengths included the randomized crossover design. The broad age cohort and balanced sex distribution provided diverse glycemic and behavioral profiles for a comprehensive analysis.
This study suggests that an automated Lyumjev delivery system equipped with qualitative meal-size estimation and meal detection could simplify or alleviate the need for carbohydrate counting, without observing a clinical decrease in time in range of more than 5%. Larger and longer studies both using these meal strategies and collecting patient-reported outcomes are warranted.
Authors’ Contributions
M.A.T., L.L., M.-R.P., and A.H. supervised the study. A.H., E.C., and E.D. designed the study. C.S., M.A.T., L.L., M.-R.P., and A.H. conducted the study. G.K. performed data reviews. C.S. performed the statistical analyses. A.H. and R.J. created the dosing algorithms and the system. Both A.H. and C.S. accessed and verified the underlying data reported. All authors had full access to the data, read and approved the final version of this article, and accepted responsibility for the decision to submit it for publication.
Guarantor Statement
A.H. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
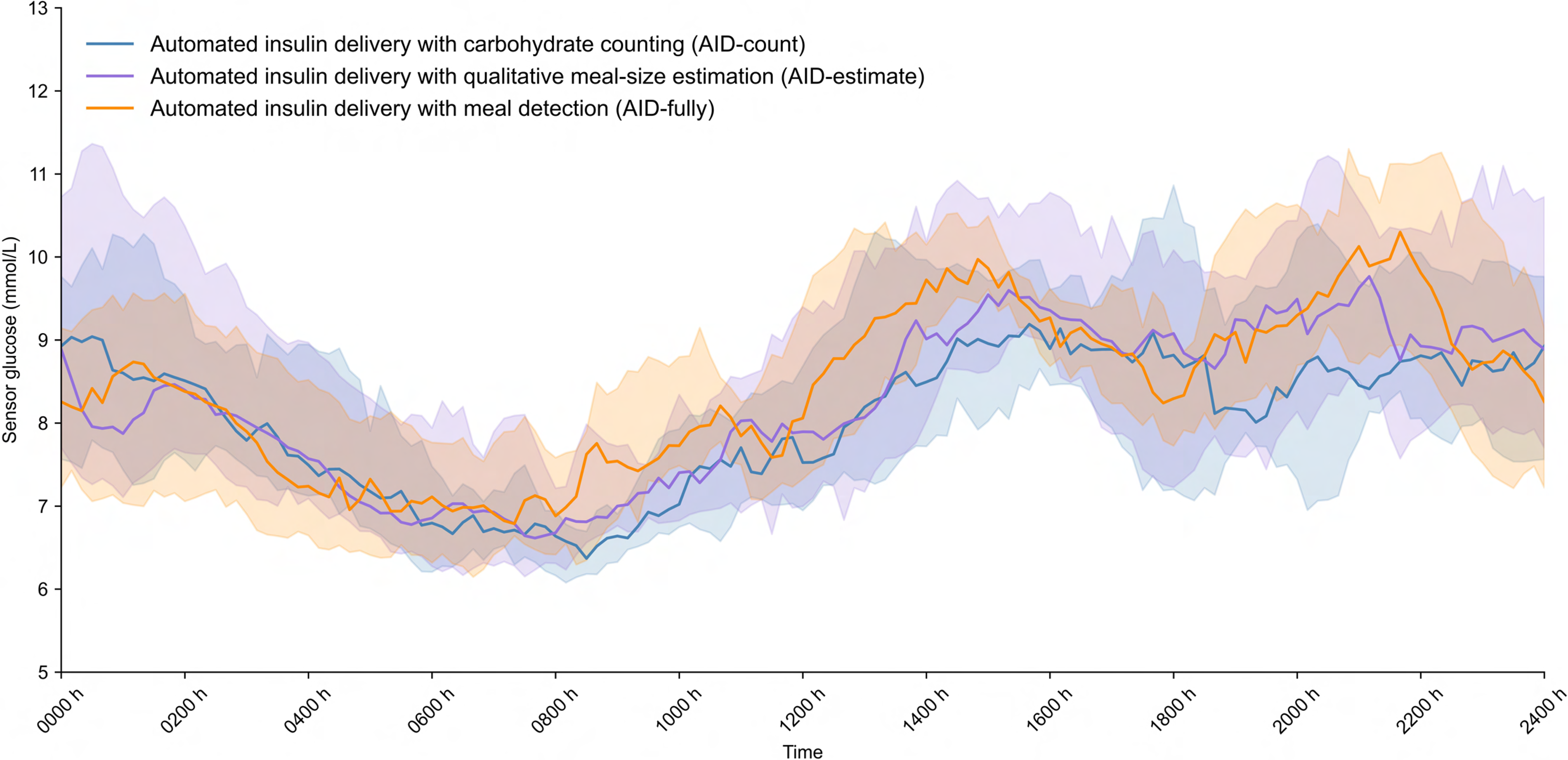
The median [IQR] profiles of mean sensor glucose levels with automated insulin delivery using carbohydrate counting (blue), qualitative meal-size estimation (purple), and meal detection (orange) (n = 12). At each time point, mean values were calculated for each participant, and the median [IQR] was determined across participants.
Footnotes
Author Disclosure Statement
M.A.T. received speaker honoraria from Boehringer-Ingelheim, Eli Lilly and Company, Janssen, Novo Nordisk, and Sanofi. L.L. received consultant fees from Abbott Diabetes Care, Dexcom, Insulet, and Novo Nordisk, payment/honoraria and support for attending meetings and/or travel from Novo Nordisk, and participated on a Data Safety Monitoring Board/Advisory Board for the NIH Artificial Pancreas program. M.-R.P. received support from Sanofi, Medtronic, and Abbott Diabetes Care. R.J. and E.D. are employees and shareholders of Eli Lilly and Company. A.H. received research support from Adocia, Dexcom, Eli Lilly and Company, Beta Bionics, and Tandem Diabetes Care, consultant fees from Eli Lilly and Company and Abbott Diabetes Care, speaker fees from SiBionics, IP acquisition fees from Eli Lilly and Company and Bigfoot Biomedical, and holds the Canada Research Chair in Artificial Pancreas Systems.
Funding Information
This research was supported by Eli Lilly and Company.