
Abstract
Background:
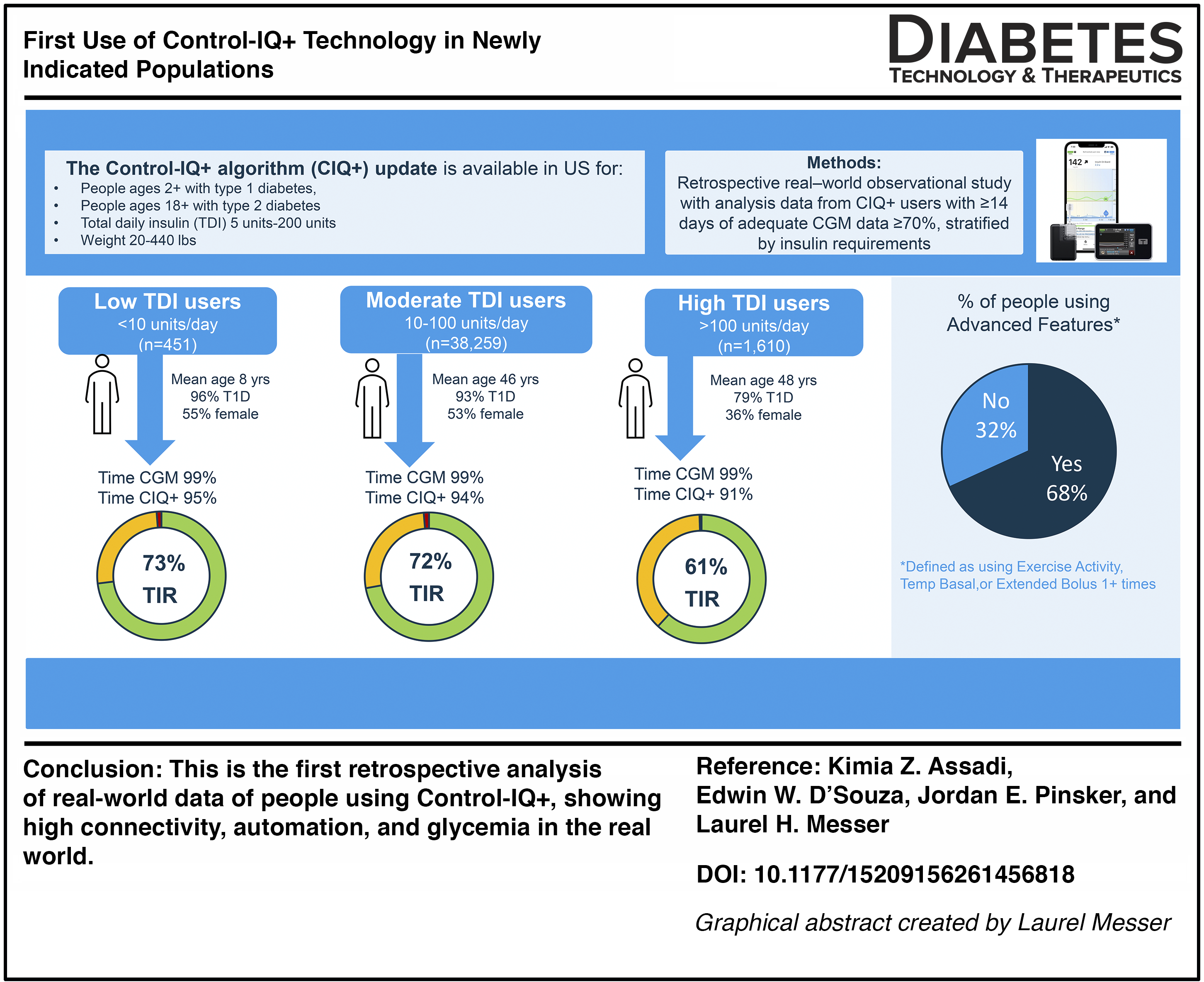
Control-IQ+ technology (Control-IQ+) is available to Tandem t:slim X2 and Tandem Mobi insulin pump users in the United States. This algorithm update enhances support for individuals with a broader range of insulin needs and offers additional new features: extended bolus and temp basal rates during automation. This study aimed to describe early real-world use of Control-IQ+ in newly indicated populations.
Methods:
Data from users of Control-IQ+ (t:slim X2 or Tandem Mobi) with ≥14 days and ≥70% continuous glucose monitoring availability in the Tandem Source web application from March 2025 to June 2025 were retrospectively analyzed. Results were stratified according to total daily insulin (TDI) use: <10 units/day (low), 10–100 units/day (moderate), or >100 units/day (high).
Results:
A total of 40,320 Control-IQ+ users met criteria for analysis (51.7% female, median age 45.6 years, 92.8% type 1 diabetes), with 451 (1%) classified as low TDI, 38,259 (95%) classified as moderate TDI, and 1610 (4%) classified as high TDI. Median percent time in automation was >90% across all subgroups. Median time in range (TIR) for the overall cohort was 71.4%, with similar values observed in low (72.7%) and moderate (71.7%) TDI users. Hypoglycemia rates were low across all groups regardless of TDI. Proactive advanced features such as extended bolus and temp basal were utilized by the minority of the cohort, with the low-TDI group using these features the most (12.2% using temp basal and 26.4% using extended bolus).
Conclusions:
In this first report, Control-IQ+ users experience high time in automation, and those with low and moderate insulin needs exceeded consensus glycemic goals. The majority of users do not use the advanced features routinely, indicating proactive engagement may be useful but is not necessary with Control-IQ+.
Introduction
Automated insulin delivery (AID) continues to be the standard of care for people living with type 1 diabetes (T1D)1–4 and more recently has been recommended for people with type 2 diabetes (T2D) who require insulin. 2 The t:slim X2 with Control-IQ technology received U.S. Food and Drug Administration clearance in 2019 for people with T1D ages 6 years and up and has demonstrated glycemic and quality-of-life benefit to people across a variety of demographics both in randomized controlled trials (RCTs)5–7 and in real world use.8–13 In 2024, the algorithm also became available on the Tandem Mobi insulin pump in the United States, a smaller insulin pump with a 200 unit insulin cartridge that offers multiple wear options including an on-body patch and full phone control. 14 The Control-IQ algorithm automates insulin delivery every 5 min while also delivering an automatic correction bolus (Autobolus) up to once per hour for predicted hyperglycemia. In addition to its standard operating mode, Control-IQ has a sleep activity feature with a more aggressive automation treatment range (112.5–120 mg/dL) that can be programmed to activate overnight and an optional exercise activity feature with a higher treatment target (140–160 mg/dL) that can be manually activated for exercise or anticipated hypoglycemia. Both systems have remote bolusing capabilities via their pump’s smartphone application (t:slim and Mobi mobile apps) and can continuously upload data to the cloud-based data server, Tandem Source.
An updated version of the AID algorithm, Control-IQ+ technology, was released in 2025 for both t:slim X2 pump users and Tandem Mobi users in the United States. The algorithm update included optimizations to support use across expanded weight parameters (from 25–140 to 9–200 kg) and total daily insulin (TDI) requirements (from 10–100 to 5–200 units/day) (Fig. 1). Control-IQ+ also adds temporary (temp) basal rates and extended boluses that can be activated while automation is turned on. 15 The Temp Basal Rate feature allows the user to activate a basal rate from 0% to 200% in increments of 15 min up to 72 h, whereas the Extended Bolus feature allows users to extend 0%–100% of a bolus over a period up to 8 h. Features such as Temp Basal Rate, Extended Bolus, and Exercise Activity are often considered “advanced features” because they require active user engagement at the time of use, such as before exercise, during a meal, or when insulin needs change. Currently, minimal data exist to suggest how frequently advanced features requiring additional user engagement are used in AID systems.
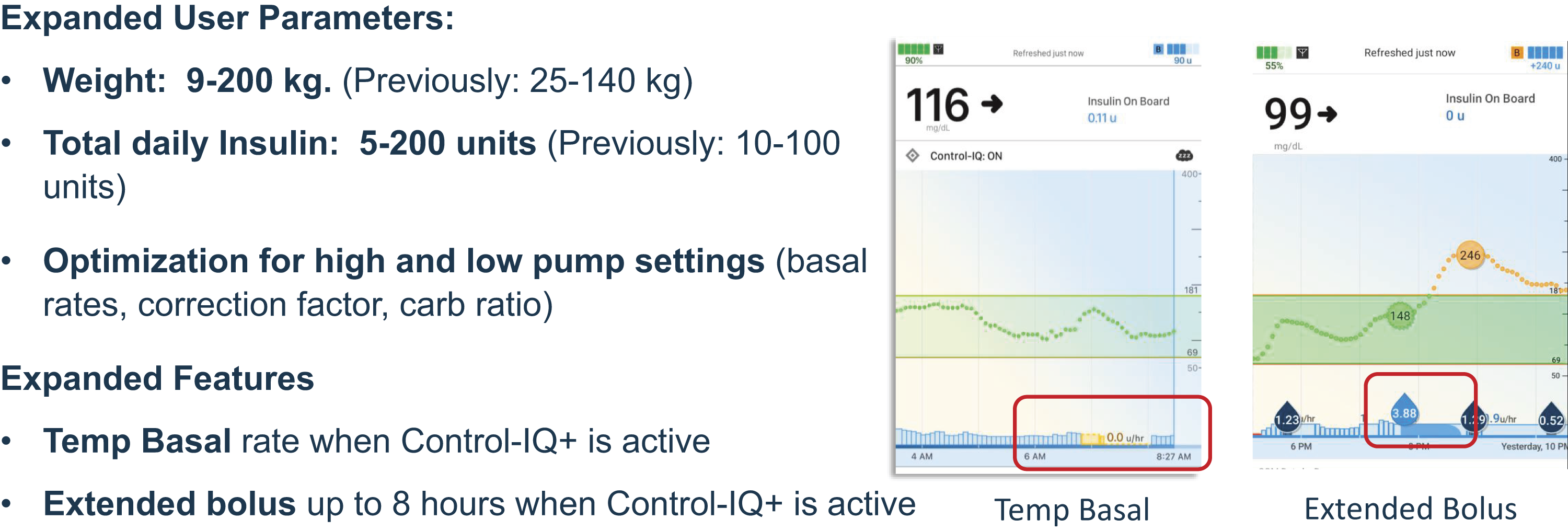
New features of Control-IQ+ technology algorithm update.
Although Control-IQ+ has demonstrated safety and efficacy in new user groups in clinical trial settings,16–18 real-world data describing the use of the system across these newly eligible populations have yet to be reported. With the addition of new features and indications, we aimed to analyze and describe outcomes from the first users of this system in the real world, with particular attention to individuals with low and high insulin requirements and use of advanced features.
Methods
Study design and population
We conducted a retrospective analysis of real-world pump and continuous glucose monitoring (CGM) data uploaded to Tandem Source, the cloud-based data platform used with Tandem insulin pumps. Ethics approval was not sought for this postmarket analysis as all patient data extracted was de-identified, and use of data was disclosed and acknowledged by Tandem users at Source account creation. The dataset included individuals using either a t:slim X2 or a Tandem Mobi pump with Control-IQ+ enabled. To be included, users were required to have at least 30 days of Control-IQ+ use between March 18, 2025 (the date of commercial availability in the United States), and June 30, 2025 and at least 14 days of CGM use with ≥70% data availability.
Classification by insulin requirements
TDI was calculated as the mean of all recorded basal and bolus insulin delivered on eligible days. To explore glycemic and behavioral patterns across typical insulin-use ranges, we stratified individuals into three subgroups: low-insulin users (TDI <10 units/day), moderate-insulin users (TDI 10–100 units/day), and high-insulin users (TDI >100 units/day). These categories reflect clinically relevant differences in insulin requirements and population heterogeneity commonly observed among pump users.
Pump interaction and system-use measures
We characterized overall system use by examining performance metrics commonly reported for AID systems, including time in automation (percentage of time Control-IQ+ was active) and CGM availability (percentage of time with valid CGM data), TDI use, mean hours of use of sleep activity and exercise activity, use of temp basal rate and extended bolus, and insulin delivery characteristics (percentage of basal and bolus insulin). With respect to bolusing behaviors, we analyzed the average number of user-initiated boluses, carbohydrate boluses, correction boluses without carbohydrate entries, Autoboluses delivered by Control-IQ+, and bolus overrides entered by the user.
Although Tandem Mobi relies on full control from a smartphone, the t:slim X2 is primarily controlled from the pump itself, with an optional mobile app feature that can be used to deliver boluses, view pump and CGM data, and automatically upload data to the cloud. As such, not every t:slim user utilizes the mobile app and instead relies on the pump itself for all functions. We therefore calculated the proportion of t:slim X2 users using the t:slim mobile app for data uploads and mobile bolusing versus those who did not use the mobile app and instead only relied on the pump for all functions. All variables were summarized at the participant level using aggregated per-day means.
Glycemic outcomes
Glycemic metrics were calculated according to standard international consensus targets for CGM reporting, 19 including time in range (TIR) 70–180 mg/dL, time in tight range (TITR) 70–140 mg/dL, time >180 mg/dL, time >250 mg/dL, time <70 mg/dL, time <54 mg/dL, mean blood glucose, and % coefficient of variation, as an indicator of glycemic variability.
Statistical analysis
All descriptive analyses were conducted in Python (Version 3.12) using standard scientific libraries for data processing. Because distributions of insulin delivery, bolusing behaviors, and CGM metrics are typically right-skewed in large real-world datasets, continuous variables are summarized using medians and interquartile ranges (IQRs). Categorical variables are presented as counts and percentages.
Summaries were produced separately for each TDI group and for the overall cohort. For descriptive comparisons across the three TDI groups, the Kruskal–Wallis test was used for continuous variables to assess differences in distributions. The chi-square test for independence was used for categorical variables. All P-values are reported for descriptive purposes.
Results
In total, 40,320 individuals met the inclusion criteria for analysis. The median age was 45.6 (IQR: 29.5–61.9) years, with 92.8% of participants having T1D. The low-TDI group was the youngest, with the median age of 8.0 (IQR: 4.2–43.9) years, whereas the moderate-TDI and high-TDI groups had median ages of 45.6 (IQR: 29.7–62.1) and 47.9 (IQR: 34.8–59.1) years, respectively (Table 1).
Demographic, System Use, and Glycemic Outcomes for People Using Low, Moderate, and High Total Daily Insulin with Control-IQ+ Technology
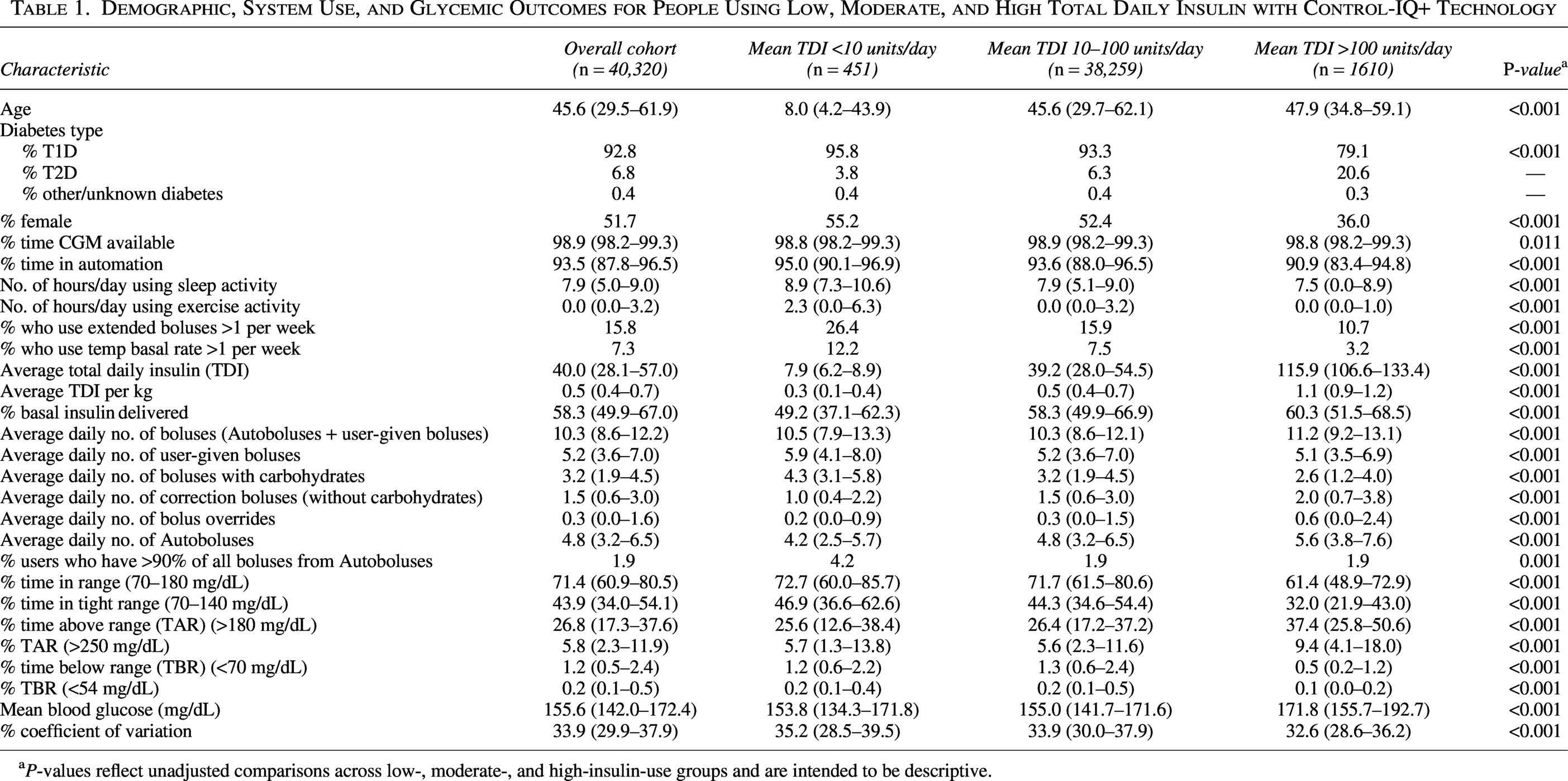
P-values reflect unadjusted comparisons across low-, moderate-, and high-insulin-use groups and are intended to be descriptive.
Device use
The majority of the low-TDI participants were using the Tandem Mobi AID system (62.8%), whereas the t:slim X2 system was more commonly used in the moderate- and high-TDI groups (72.8% and 91.1%, respectively). In all three groups, the majority of t:slim X2 users were using the Mobile app to upload data to the cloud on a regular basis (71.4% for low-TDI, 89.9% for moderate-TDI, and 87.5% for high-TDI groups). About half of the low-TDI users delivered boluses from the t:slim app (56.5%), whereas 76.3% of the moderate-TDI users and 76% of the high-TDI users delivered boluses from the app (all Tandem Mobi users bolus from the Mobile app, as the system interface is app based). Across all three groups, there was high time in CGM use (>98%) and high time in automation (>90%).
Low-TDI users
Low-insulin users were notably younger than other user groups and primarily had T1D (Table 1). Compared with other groups, the low-TDI users spent more time per day using sleep activity (median 8.9 h/day), exercise activity (median 2.3 h/day), and 26.4% used extended boluses at least once per week. They also had the lowest weight-adjusted insulin use and a lower proportion of basal insulin delivery (49.2% of TDI). The low-TDI users had the highest median user-initiated boluses per day (5.9) compared with the other insulin groups, and 4.2% of them received >90% of their bolus insulin from Autoboluses, indicating that these individuals initiated boluses rarely. For glycemic outcomes, the low-TDI group exceeded consensus statement guidelines by achieving >70% TIR (70–180 mg/dL) and maintaining 1.2% time <70 mg/dL. This user group also had the lowest mean glucose (median 153.8 mg/dL [IQR: 134.3, 171.8], P < 0.001).
Moderate-TDI users
The moderate-TDI users had system use outcomes between the low-TDI and high-TDI groups (feature use, TDI, number of boluses, etc.). Their median age was closer to the high-TDI user group (45.6 vs. 47.9 years), and 58.3% of TDI was delivered as basal. Glycemic outcomes in the moderate-TDI group were clinically similar to those in the low-TDI user group, with a median TIR of 71.7% (IQR: 61.5–80.6) and low hypoglycemia (1.3% [IQR: 0.6–2.4]), exceeding guideline recommendations for >70% TIR and <4% time <70 mg/dL. 19
High-TDI users
Compared with the other two groups, a higher proportion of high-insulin users had T2D (20.6%) and were male (64%). They had the highest weight-adjusted insulin requirements (1.1 units/kg/day), substantially more than the other two groups. They also had the lowest use of sleep activity, exercise activity, extended bolus, and temp basal rate features. High-insulin users had the highest proportion of basal insulin delivery (60.3%), administered fewer user-initiated boluses during the day but more correction boluses, and had the highest number of daily Autoboluses. For glycemic outcomes, the high-TDI group had a lower median TIR of 61.4% (IQR: 48.9–72.9) and time <70 mg/dL (median 0.5% [IQR: 0.2–1.2], P < 0.001). They also had the highest mean glucose (median 171.8 mg/dL [IQR: 155.7–192.7], P < 0.001).
Discussion
This is the first report of Control-IQ+ technology outcomes in the real world, including people with both T1D and T2D, a wide range of ages, and a range of insulin needs. This study found high time in automation and CGM use, consistent across all three strata of insulin users. The low-TDI and moderate-TDI groups met recommended glycemic targets for >70% TIR 70–180 mg/dL, 19 and all groups reported low hypoglycemia (time <70 and <54 mg/dL). There are limited AID systems indicated for use in individuals as young as 2 years old and with TDI requirements as low as 5 units, underscoring the importance of safety and efficacy data across a broad range of people with diabetes.
The overall high time in automation and CGM use observed in this study matches previous reports of Control-IQ use in the real world. 9 Automation with Control-IQ+ remains active as long as CGM data are available, identical to the former Control-IQ algorithm.
The low-TDI users in this study were notably younger than the other cohorts, with a median age of 8.0 [IQR: 4.2–43.9] years and included young children in the newly indicated age group of 2–5 years old. It is not surprising that this group utilized advanced features more than the moderate- and high-TDI groups who were much older, as younger children are managed with enhanced parental supervision and support, and may require additional feature utilization to manage challenging eating behaviors such as grazing or snacking.3,15,20 Younger children also typically require a lower proportion of insulin delivered by basal as compared to bolus, 3 and this group showed the lowest percentage of basal across the three TDI strata. Although the duration of diabetes is unknown, it is possible that many of the older participants in the low-TDI group were early in their diabetes diagnosis and still in the honeymoon phase, which could explain why their insulin requirements by body weight were low, and they required <10 units/day. 21 Adjunctive glucose-lowering therapies (e.g., glucagon-like peptide 1 (GLP-1) receptor agonists or sodium-glucose cotransporter 2 (SGLT2) inhibitors) may also have contributed to lower TDI requirements; however, use of contaminant medications was not captured in the available dataset. All of these factors may also have contributed to the median TIR of 72.7% for this cohort.
The high-TDI users in our study included a greater proportion of individuals with T2D (20.6%) and had higher weight-adjusted insulin requirements compared to the other groups. In an RCT of 319 individuals with T2D, Control-IQ+ use over 13 weeks was associated with a 0.9% reduction in HbA1c compared with a 0.3% reduction in those using their pre-study insulin regimen with CGM (mean adjusted group difference: −0.6%). 17 The TIR for people with T2D using Control-IQ+ was 64%, and the glycemic improvements were seen regardless of age, sex, race/ethnicity, education level, and baseline HbA1c. 22 In a separate study, Control-IQ+ was studied in people with T1D with high insulin requirements (1.2 units/kg/day) over 13 weeks and similarly found an average TIR of 64.8%. 18 The TIR reported for high-TDI users in this real-world study is comparable, if not slightly lower. The users in this study, while requiring large amounts of insulin, had the lowest bolus frequency, the lowest average number of carbohydrate entries per day, and the highest number of Autoboluses of all the groups analyzed. This lower engagement may contribute to the lower glycemic outcomes, although insulin resistance itself is also a likely factor.
It is noteworthy that proactive, advanced features such as exercise activity, temp basal rates, and extended bolus were minimally utilized overall. We know from previous studies that automation improves glycemia irrespective of engagement, 23 which may explain why users decide not to use advanced features in the majority of situations. Characterization of individual feature use on AID systems is not often studied. Exercise activity is a feature that had previously existed in the Control-IQ algorithm and has been suggested for use during aerobic exercise in published AID guidelines.24,25 A real-world study conducted in Belgium reported exercise activity being used by 35% of children after 1 year of Control-IQ use, which is substantially higher than the use of exercise activity in this analysis. 10 This is the first article to report on the use of the temp basal and extended bolus features during automation with the use of Control-IQ+. Future studies will be able to determine optimal use of these features or delineate appropriate use cases for subpopulations.
This study is the first to describe real-world use of the Control-IQ+ algorithm in the United States. Strengths of the study include the large sample size, the robust volume of CGM data points, and detailed characterization of system use. Data were collected across a variety of ages, diagnoses, insulin needs, and pump and CGM systems. There are also limitations to this database analysis. First, there are many unknown variables that could not be analyzed, such as other demographic characteristics of the participants, pump therapy settings, and use of adjunctive medications (e.g., GLP-1 receptor agonists) that may influence glycemic outcomes and insulin requirements. Furthermore, these are cross-sectional data, which cannot lead to conclusions of algorithm efficacy compared to the previous insulin delivery modality. Future studies are needed to further characterize therapy settings and feature use across new segments of the population of people using Control-IQ+ technology.
Conclusions
In the real world, Control-IQ+ demonstrates high time in automation and CGM use, with low- and moderate-TDI user groups meeting TIR goals, and low hypoglycemia across all strata of insulin users. Future studies will help to further characterize therapy settings and feature use across newly indicated populations using Control-IQ+ technology.
Authors’ Contributions
K.Z.A., E.W.D., J.E.P., and L.H.M. were involved in the conception and design of the study. E.W.D. performed the glycemic and survey results analysis. All authors were involved in the planning of the analysis and interpretation of the results. K.Z.A. and L.H.M. wrote the first draft of the article. K.Z.A. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. All the authors edited, reviewed, and approved the final version of the article.
Footnotes
Acknowledgments
The authors wish to thank Lars Mueller and the data science teams at Tandem Diabetes Care.
Author Disclosure Statement
All authors are employees and shareholders of Tandem Diabetes Care, Inc.
Funding Information
This study was funded by Tandem Diabetes Care, Inc.