
Abstract
Aims/Hypothesis:
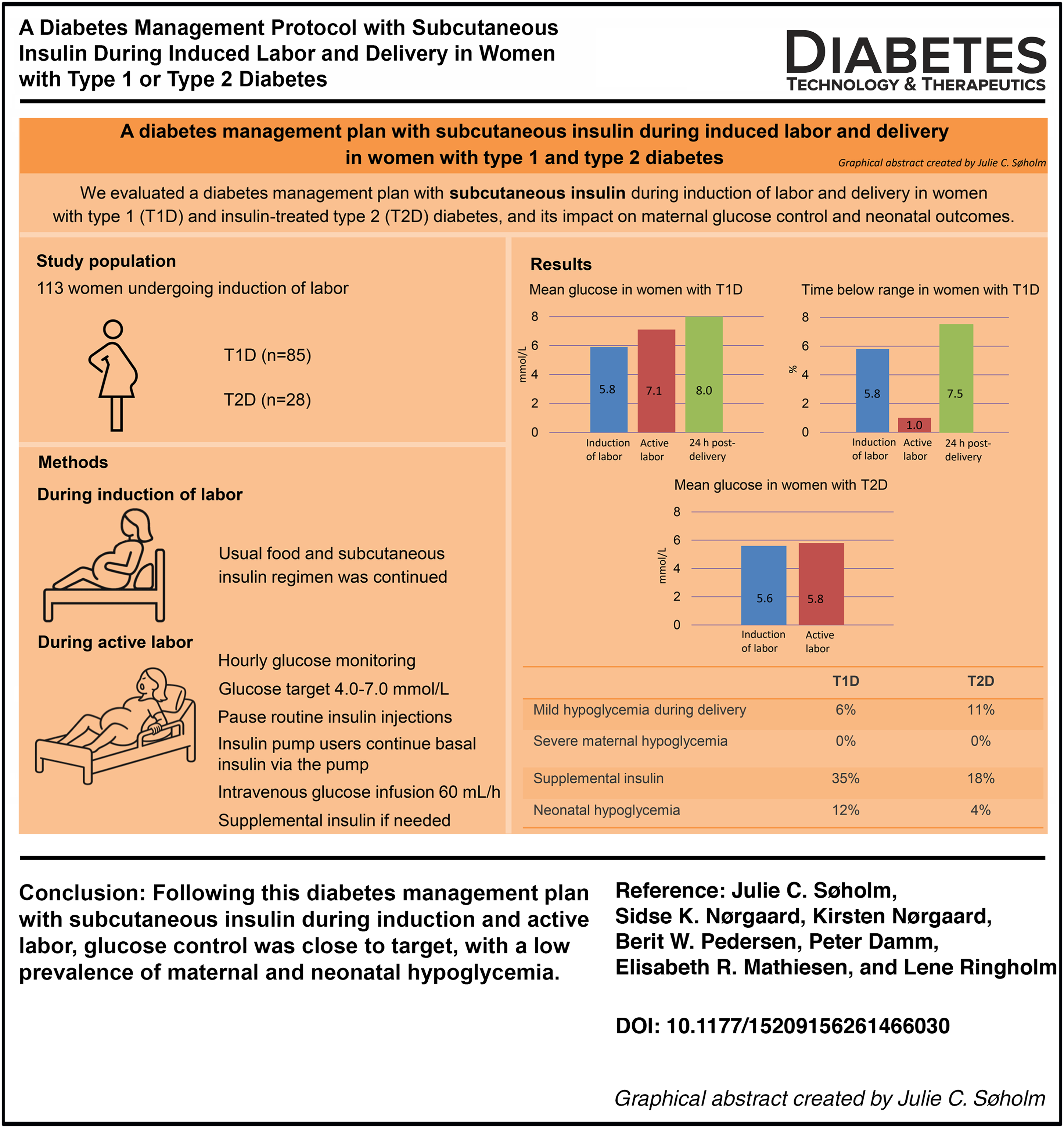
To evaluate a diabetes management protocol with subcutaneous insulin during induction of labor and delivery in women with type 1 diabetes (T1D) and insulin-treated type 2 diabetes (T2D).
Material and Methods:
A secondary analysis of the CopenFast trial, including women undergoing induction of labor. According to the diabetes management protocol, usual diet and insulin were initially continued. From the onset of active labor, target glucose was 4.0–7.0 mmol/L, and intravenous glucose infusion (3 g/h) was given. Women using multiple daily injections discontinued routine insulin injections, and nonautomated insulin pump users continued subcutaneous basal insulin via the pump. Supplemental insulin was given if glucose levels exceeded target levels. Continuous glucose monitoring was used in T1D and hourly capillary blood glucose monitoring (BGM) with a glucometer in T2D. Study endpoints were maternal glucose control and neonatal outcomes.
Results:
In total, 113 women (85 T1D and 28 T2D) were included. HbA1c was 42 ± 5 and 41 ± 10 mmol/mol (6.0 ± 2.0% and 5.9 ± 2.0%) [mean ± standard deviation (SD)]) at 35 weeks. Glucose infusion was given for 4.8 (2.0–7.0) and 5.5 (4.0–8.0) (median [interquartile range (IQR)]) hours. During induction and active labor, mean sensor glucose in T1D was 5.9 ± 1.8 and 7.1 ± 1.8 mmol/L (106 ± 32 and 128 ± 32 mg/dL), respectively, and mean BGM in T2D was 5.6 ± 2.8 and 5.8 ± 1.2 mmol/L (101 ± 50 and 104 ± 22 mg/dL). During active labor, maternal hypoglycemia (≤3.9 mmol/L [70 mg/dL]) occurred in 6% and 11%. Supplemental insulin was administered in 35% (4.0 IU [2.0–7.5]) and 18% (2.0 IU [2.0–4.0]). Neonatal hypoglycemia (<2.2 mmol/L [40 mg/dL]) occurred in 12% and 4%.
Conclusions/Interpretation:
Following a diabetes management protocol with subcutaneous insulin during induction and active labor, glucose control was close to target, with low prevalence of maternal and neonatal hypoglycemia. These findings support the feasibility of subcutaneous insulin during labor and delivery.
Keywords
Introduction
Pregnancy and childbirth in women with type 1 diabetes (T1D) and type 2 diabetes (T2D) remain associated with substantially increased risks of severe late-pregnancy and perinatal complications.1,2 Approximately half of women with T1D and one third of women with T2D deliver large for gestational age infants, and the prevalence of birth complications, such as perineal laceration, shoulder dystocia, neonatal hypoglycemia, and, ultimately, stillbirths is 2–5 times higher compared with pregnant women without diabetes.3–7 Induction of labor is therefore commonly recommended around 38 gestational weeks to reduce the risk of these birth complications.8,9
The primary objective of diabetes management during labor and delivery is to achieve stable maternal glucose levels with minimal hypoglycemia and hyperglycemia to ensure maternal and fetal well-being and to prevent neonatal hypoglycemia. 10 Severe hypoglycemia (requiring assistance from another person) 11 and diabetic ketoacidosis are rare but serious complications during labor.2,12
Traditionally, the standard of care for women with T1D during labor and delivery has involved the coadministration of intravenous insulin and glucose infusion.13,14 This conventional approach is notoriously burdensome as it requires continuous, labor-intensive intravenous management via two peripheral intravenous catheters, frequent insulin dose titrations to maintain tight glycemic targets and prevent maternal hypoglycemia, fluid overload, and electrolyte derangement.10,15,16
Subcutaneous insulin administration, either by multiple daily injections (MDIs) or insulin pump, may be used as an alternative to intravenous insulin administration. This approach has been evaluated in small retrospective studies including 27–47 women with T1D or T2D using subcutaneous insulin13,16–18 and one randomized controlled trial (RCT) with 70 women with T1D allocated to either subcutaneous (n = 35) or intravenous insulin infusion (n = 35). 14 These studies reported comparable or improved maternal glucose control with subcutaneous insulin compared with intravenous insulin and no increased risk of adverse maternal or neonatal outcomes.13,14,16–18
Diabetes management protocol with subcutaneous insulin during labor and delivery in women with T1D and T2D have, to the best of our knowledge, not been described.
In accordance with our practice, a diabetologist develops a diabetes management protocol in late pregnancy. In essence, women with T1D or T2D continue usual subcutaneous insulin until active labor after which women using MDIs discontinue insulin injections, while women using insulin pump continue subcutaneous basal insulin via the pump.
The aim of this study was to evaluate our diabetes management protocol with subcutaneous insulin during induction of labor and delivery in women with T1D and T2D, and its impact on maternal glucose control and neonatal outcomes.
Methods and Material
Study design and population
This was a descriptive secondary analysis of diabetes management during induction of labor and delivery in women with T1D and T2D who, from November 2019 to May 2022, were included in the CopenFast trial, an RCT evaluating the effect of faster-acting insulin aspart compared with insulin aspart during pregnancy, delivery, and post-delivery.19,20
In the original CopenFast trial, 203 women with T1D or T2D delivered an infant with a gestational age beyond 22 gestational weeks. Of these, 113 (56%) women, 85 with T1D and 28 with T2D, underwent induction of labor and were included in this analysis. The remaining women were excluded due to elective cesarean section (n = 61), acute cesarean section prior to onset of labor induction (n = 18), or spontaneous onset of labor (n = 10).19,20
Among women with T1D, 66 (78%) used MDI and 19 (22%) used nonautomated insulin pumps. All 28 women with T2D used MDI.
Routine diabetes care
All women followed the standard diabetes care program for women with T1D and T2D during pregnancy, with regular consultations by a diabetologist approximately every 2 weeks as previously described. 20 Briefly, at the first visit, all women received standardized recommendations on medical nutrition therapy and carbohydrate counting. Women were advised to follow a low glycemic index diet with a daily carbohydrate intake of at least 150 g distributed as 20, 50, and 50 g at the main meals, with the remaining carbohydrates from snacks.
Women already using continuous glucose monitoring (CGM) at the first visit routinely continued its use, and the remaining women with T1D were offered intermittently scanned CGM (isCGM), whereas women with T2D primarily used capillary blood glucose monitoring (BGM). 20 Glucose targets were 4.0–5.5 mmol/L (72–99 mg/dL) before meals and 4.0–7.0 mmol/L (72–126 mg/dL) 90 min after meals. Women using isCGM were advised to aim for a mean sensor glucose of 5.0–6.0 mmol/L (90–108 mg/dL), time in range in pregnancy (TIRp, 3.5–7.8 mmol/L [63–140 mg/dL]) >70%, time above range (TARp, >7.8 mmol/L [140 mg/dL]) <25%, and time below range (TBRp, <3.5 mmol/L [63 mg/dL]) <4%. 21 HbA1c targets were <48 mmol/mol before 20 gestational weeks and <38 mmol/mol from 20 gestational weeks onward. Blood pressure (BP) targets during pregnancy were office BP ≤135/85 mmHg, and when available, home BP ≤130/80 mmHg.22,23
Recommended gestational weight gain was based on prepregnancy BMI as follows: 10–15 kg if BMI <25 kg/m2, 5–8 kg if BMI 25–29.9 kg/m2, and 0–5 kg if BMI ≥30 kg/m2.24,25
At approximately 33 gestational weeks, a diabetologist documented a diabetes management protocol estimating each woman’s subcutaneous insulin dosing during induction and active labor and immediately after delivery (Fig. 1), 26 based on the national guideline.26,27 This protocol took into account that during active labor and immediately after delivery, insulin requirements typically decrease to approximately 70% of the prepregnancy dose, corresponding to about 30% of the insulin dose administered on the day prior to delivery. The individual diabetes management protocol was documented in the patient record.
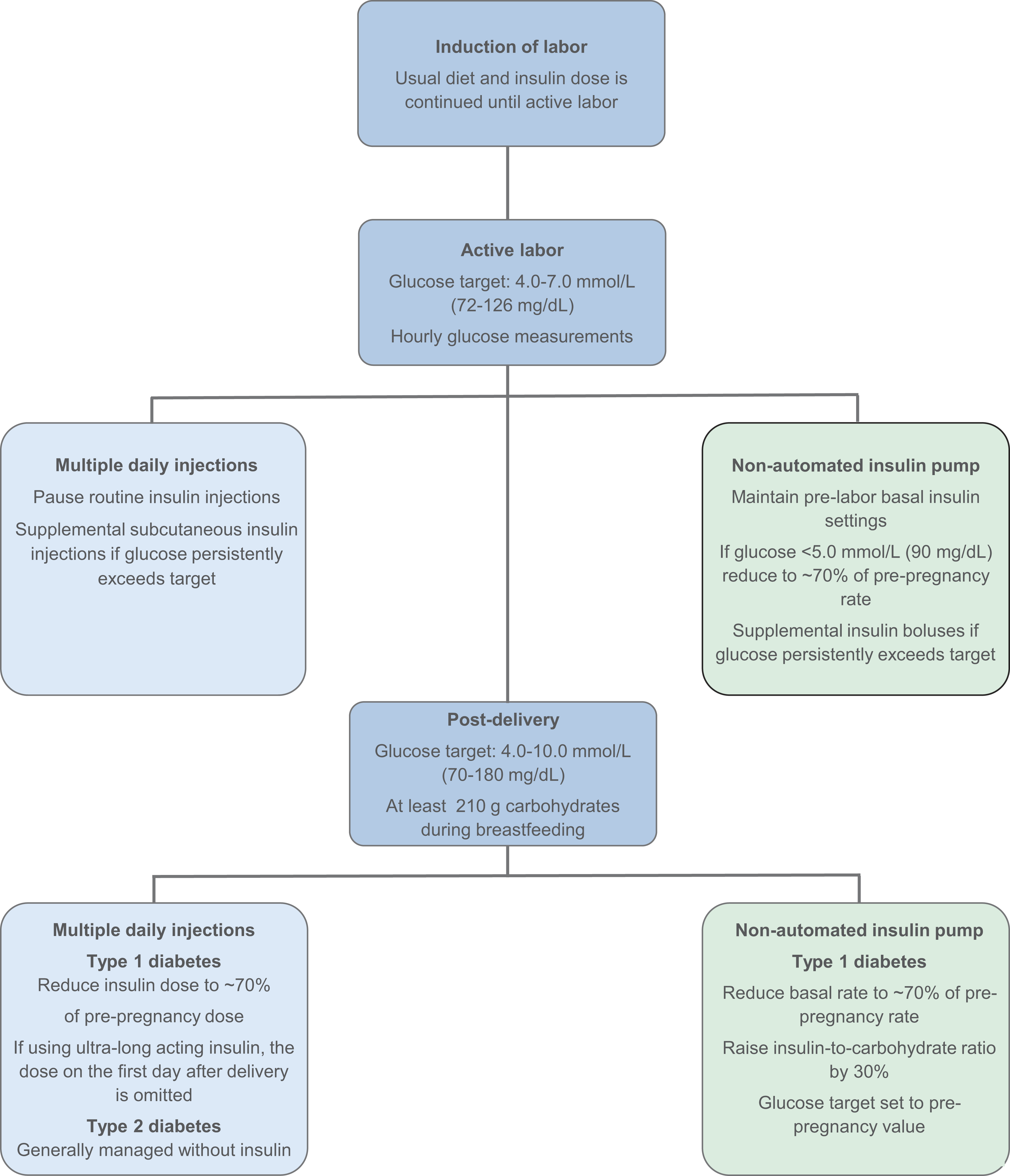
Chronological sequence of the diabetes management protocol for women with type 1 and type 2 diabetes from the onset of induction of labor, during active labor, and the immediate post-delivery period, including specific recommendations according to diabetes type and insulin treatment modality.
At approximately 36 gestational weeks, the mode and timing of delivery were planned and agreed upon by the woman and an obstetrician based on an individualized evaluation of overall obstetric risk assessment. In accordance with national recommendations for women with T1D and T2D, induction of labor was generally recommended at the latest between 38 + 0 and 40 + 0 gestational weeks, with the exact timing based on fetal and maternal risk factors and complications. 28
The principles of the diabetes management protocol covering induction of labor, active labor, and the period immediately after delivery were as follows: The usual diet and subcutaneous insulin regimen used in late pregnancy was continued until onset of active labor or until cesarean section. Upon admission to the delivery room, glucose monitoring was performed at least hourly, either by CGM or capillary BGM, with a target glucose of 4.0–7.0 mmol/L (72–126 mg/dL).
Women using CGM and/or insulin pumps were advised to place sensors, and infusion sets away from the upper abdomen and the anticipated surgical field in case of cesarean section. Alternative insertion sites during labor included the lateral abdomen, upper arms, thighs, and buttocks.
From the onset of active labor, women were generally advised to pause oral food intake and an intravenous isotonic 5% glucose infusion at 60 mL/h (3 g glucose per hour) was initiated. All women using MDI were advised to pause routine insulin injections. Women using insulin pump were advised to initially maintain prelabor basal insulin settings. When glucose levels were below 5.0 mmol/L (90 mg/dL), basal insulin rates were reduced to approximately 70% of prepregnancy rates according to the documented diabetes management protocol. Supplemental insulin was administered as subcutaneous insulin injections or, in insulin pump users, additional insulin pump boluses if glucose levels persistently exceeded the recommended threshold.
After delivery, all women were recommended a minimum daily carbohydrate intake of 210 g during breastfeeding, 29 and a target glucose level of 4.0–10.0 mmol/L (72–180 mg/dL). Women with T1D using ultra-long-acting insulin analogs were advised to omit the injection on the first day after vaginal delivery to minimize the risk of maternal hypoglycemia. Basal insulin dose was resumed the following day at approximately 70% of the prepregnancy insulin dose, in accordance with the diabetes management protocol. Insulin pump users continued basal insulin rates at approximately 70% of prepregnancy rates as initiated during delivery. Meal-time insulin doses were reduced by raising the insulin-to-carbohydrate ratio by approximately 30%, insulin sensitivity was raised by 30%, and glucose target was set to the value prior to pregnancy. 30
Women with T2D diabetes were generally managed without insulin or any other glucose-lowering drugs during breastfeeding.
Data collection and definitions
The 113 women’s records were reviewed independently by two of the authors (J.C.S. and L.R.), focusing on diabetes management from time of induction of labor, during active labor, and until 4 h post-delivery.
Induction of labor was initiated with oral prostaglandin E1, by artificial rupture of membranes or with a balloon catheter. When intravenous oxytocin was administered as part of the induction process, time of administration and discontinuation were recorded.
Women were considered to be in active labor based on a clinical assessment by the midwife documented in the medical record, including strong and regular contractions and cervical dilation ≥4 cm.
The following data were collected from the records:
Timing and method of induction of labor, timing of onset of active labor, and initiation and discontinuation of intravenous glucose infusion.
During active labor and until 4 h post-delivery, hourly glucose values were obtained by CGM in women with T1D and by capillary BGM in women with T2D. An episode with a glucose level ≤3.9 mmol/L (70 mg/dL) was categorized as hypoglycemia, and an episode with a glucose level >7.0 mmol/L (126 mg/dL) was categorized as hyperglycemia. The need for supplementary subcutaneous insulin injections was recorded.
From the onset of induction of labor until 7 days post-delivery, episodes of severe hypoglycemia and diabetic ketoacidosis were recorded.
Glucose monitoring
Raw isCGM data, covering the period from the onset of induction until 7 days post-delivery, were downloaded from LibreView (Abbott Diabetes Care, Alameda, California, USA). isCGM data were available for 58 (75%) of the 85 women with T1D during labor and delivery, and for 55 (65%) women from delivery until 7 days post-delivery.
The remaining 27 women with T1D were not included in the CGM-based analysis due to real-time CGM use (n = 13), incomplete isCGM data (n = 8), and use of capillary BGM only (n = 6). All 28 women with T2D used capillary BGM.
Pregnancy and neonatal outcomes
Pre-eclampsia was defined as office BP ≥140/90 mmHg after 20 gestational weeks with co-existing proteinuria or new-onset symptoms from other organs. 31 Preterm delivery was defined as delivery before 37 gestational weeks. The following neonatal outcomes were registered: gestational age at delivery given as weeks + days, birthweight, offspring sex, and neonatal hypoglycemia (plasma glucose <2.2 mmol/L [40 mg/dL] 2 h after birth). Large- and small-for-gestational age infants were defined as birthweight >90th and <10th percentiles, respectively, adjusted for gestational age and sex. 32
Statistical analysis
Continuous data were given as mean (SD) or median (interquartile range) and categorical variables as numbers (%). For maternal characteristics at baseline presented in Table 1, differences between women with T1D and T2D were assessed using Student’s t-test for continuous variables and chi-square test for categorical variables.
Maternal Characteristics in 113 Pregnant Women with Type 1 or Type 2 Diabetes Undergoing Induction of Labor
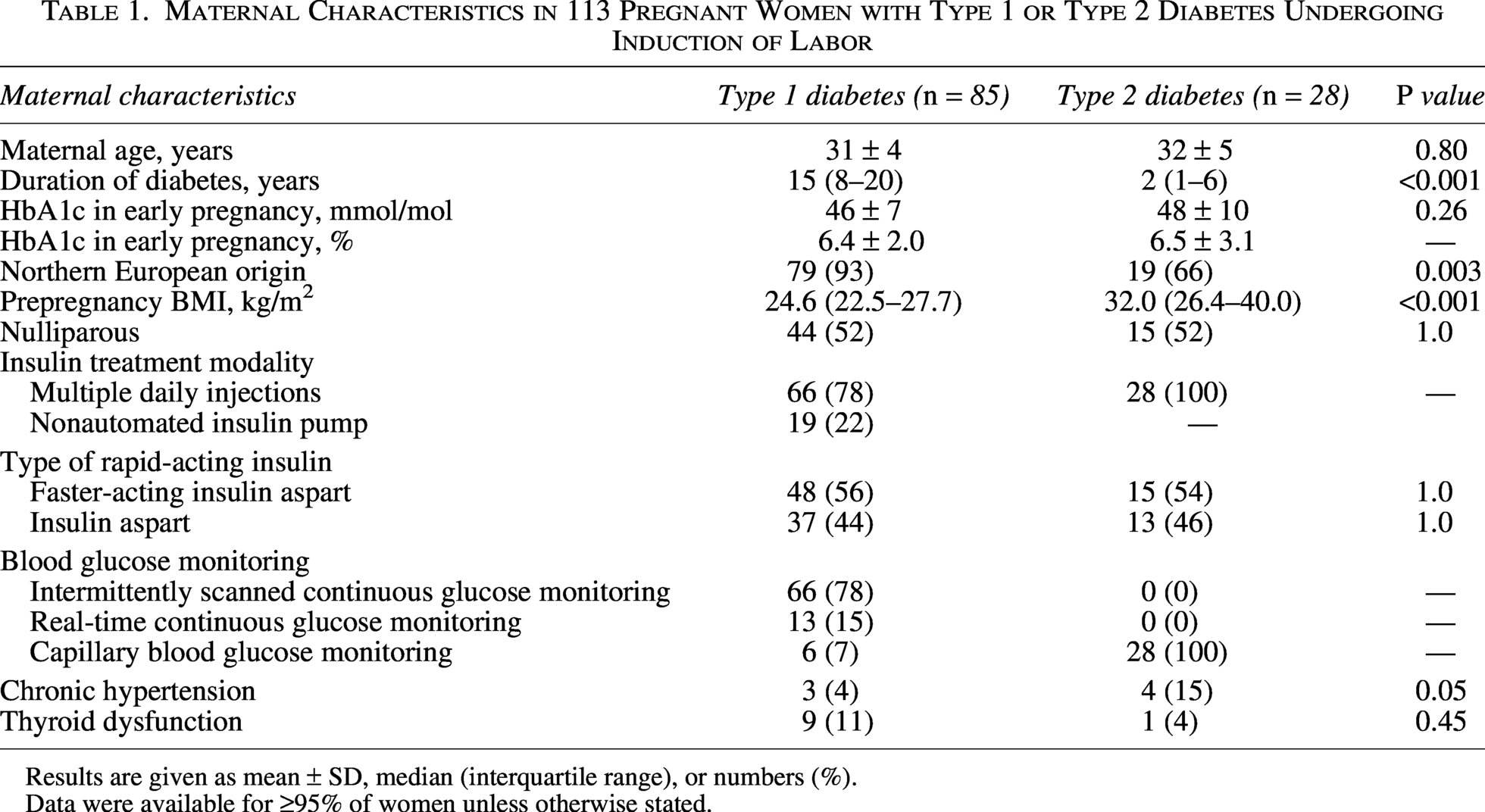
Results are given as mean ± SD, median (interquartile range), or numbers (%).
Data were available for ≥95% of women unless otherwise stated.
Blood glucose values were assessed for the following four intervals: (1) from onset of induction to onset of active labor, (2) from onset of active labor to delivery, (3) from delivery until 24 h post-delivery, and (4) from 24 h post-delivery to 7 days post-delivery.
For women with T1D, glycemic metrics including mean glucose, TARp, TIRp, and TBRp were calculated for intervals 1 and 2. Post-delivery, the reference range for TIR was adjusted to 4.0–10.0 mmol/L (70–180 mg/dL) and applied for analyses of intervals 3 and 4.
In all women, mean blood glucose values were estimated using linear mixed-effects models with a random intercept for each woman to account for repeated measures. When data were aggregated into hourly means, each hour was weighted by the proportion of the hour covered by available measurements.
Analyses were performed using R version 4.5.0 (R Core Team, 2021, R Foundation for Statistical Computing, Vienna, Austria, was used for all the data analyses). 33 A two-sided P value of <0.05 was considered statistically significant.
Ethics
Written consent was obtained from all women, including the partners, regarding infant data collection. The trial protocol was approved by the Danish Medicines Agency (2018-004680-31) and the Regional Ethics Committee (H-19029966). The trial was registered with ClinicalTrials.gov, NCT03770767.
Results
Women with T1D had longer diabetes duration, lower BMI, and were more often of Nordic origin compared with women with T2D. All other maternal characteristics were similar between women with T1D and T2D (Table 1).
Induction of labor was on average initiated at term and primarily medically with prostaglandin E1 (Table 2). The time from onset of induction to onset of active labor was 25.0 (9.0–47.0) (median [IQR]) hours in women with T1D and 33.5 (18.0–46.0) hours in women with T2D (Table 2). From induction until active labor, mean glucose was 5.9 ± 1.8 (mean ± SD) mmol/L (106 ± 32 mg/dL) in women with T1D and 5.6 ± 2.8 mmol/L (101 ± 50 mg/dL) in women with T2D, respectively.
Induction of Labor and Diabetes Management During Active Labor in 113 Women with Type 1 or Type 2 Diabetes
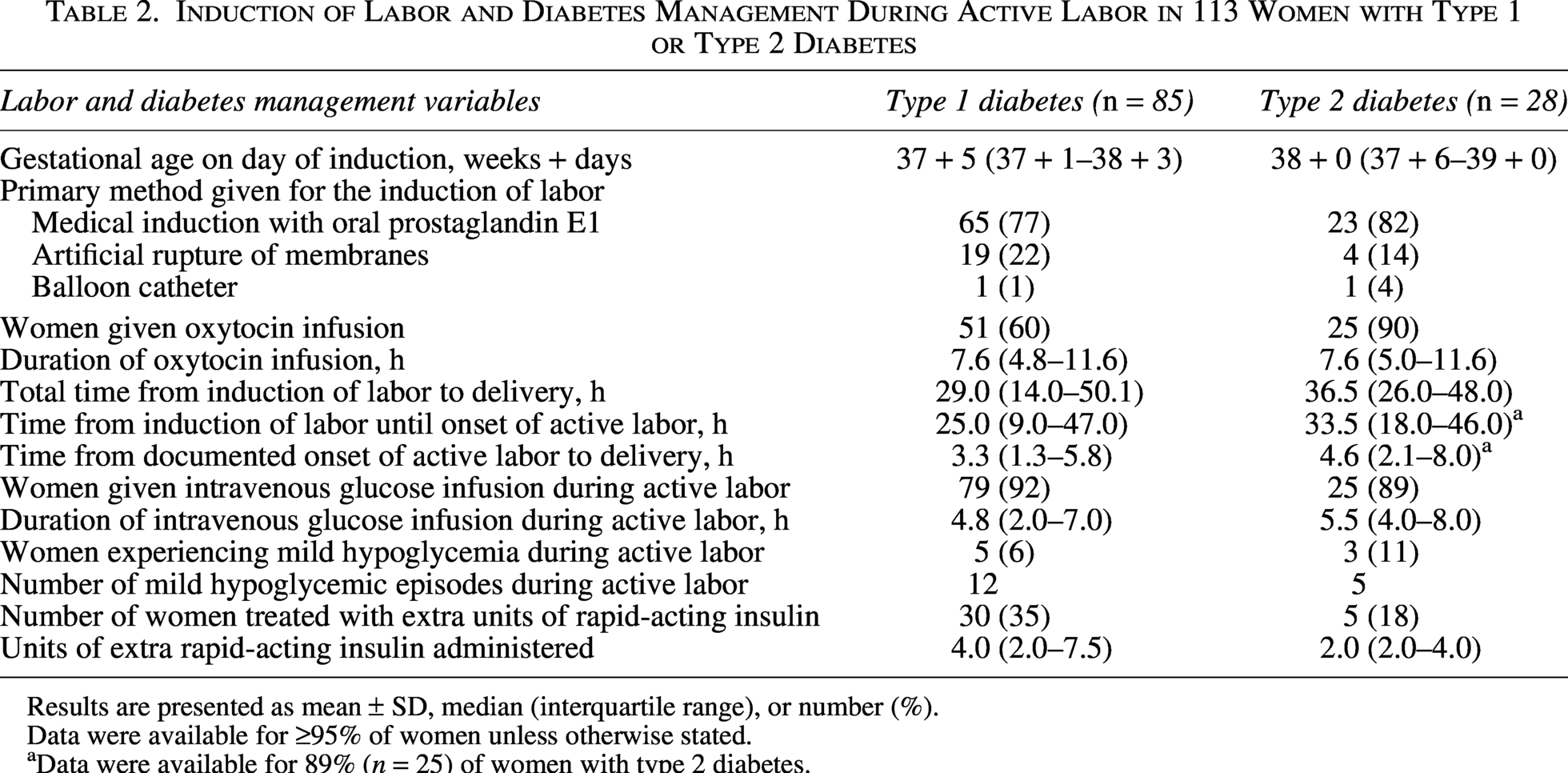
Results are presented as mean ± SD, median (interquartile range), or number (%).
Data were available for ≥95% of women unless otherwise stated.
Data were available for 89% (n = 25) of women with type 2 diabetes.
Intravenous glucose infusion was given for 4.8 (2.0–7.0) and 5.5 (4.0–8.0) hours in the majority (92% and 89%) of women with T1D and T2D, respectively. The median time from onset of active labor until delivery was 3.3 (1.3–5.8) and 4.6 (2.1–8.0) hours for women with T1D and T2D, respectively (Table 2). The longer duration of intravenous glucose infusion reflects continuation of the infusion into the immediate post-delivery period in some women.
Mean glucose was 7.1 ± 1.8 mmol/L (128 ± 32 mg/dL) and 5.8 ± 1.2 mmol/L (104 ± 22) during active labor in women with T1D and T2D, respectively. Episodes of hypoglycemia (glucose levels ≤3.9 mmol/L [70 mg/dL]) occurred in 6% and 11% of women.
Supplementary subcutaneous insulin, as insulin injections or, in insulin pump users, additional insulin pump boluses, in addition to the diabetes management protocol, was given in 35% of women with T1D (4.0 IU [2.0–7.5]) and 18% of women with T2D (2.0 IU [2.0–4.0]) (Table 2). During active labor, 33 (57%) of women with T1D and 18 (69%) of women with T2D achieved overall mean glucose levels within the target range of 4.0–7.0 mmol/L (72–126 mg/dL).
Fourteen women (16%) with T1D underwent an emergency cesarean section, of whom five had the procedure before the onset of active labor and nine during active labor. Five women (18%) with T2D underwent an emergency cesarean section, of whom two had the procedure before the onset of active labor and three during active labor (Table 2).
The prevalence of neonatal hypoglycemia was 12% and 4% in infants born to women with T1D and T2D, respectively (Table 3).
Maternal and Neonatal Outcomes in 113 Women with Type 1 or Type 2 Diabetes Undergoing Induction of Labor
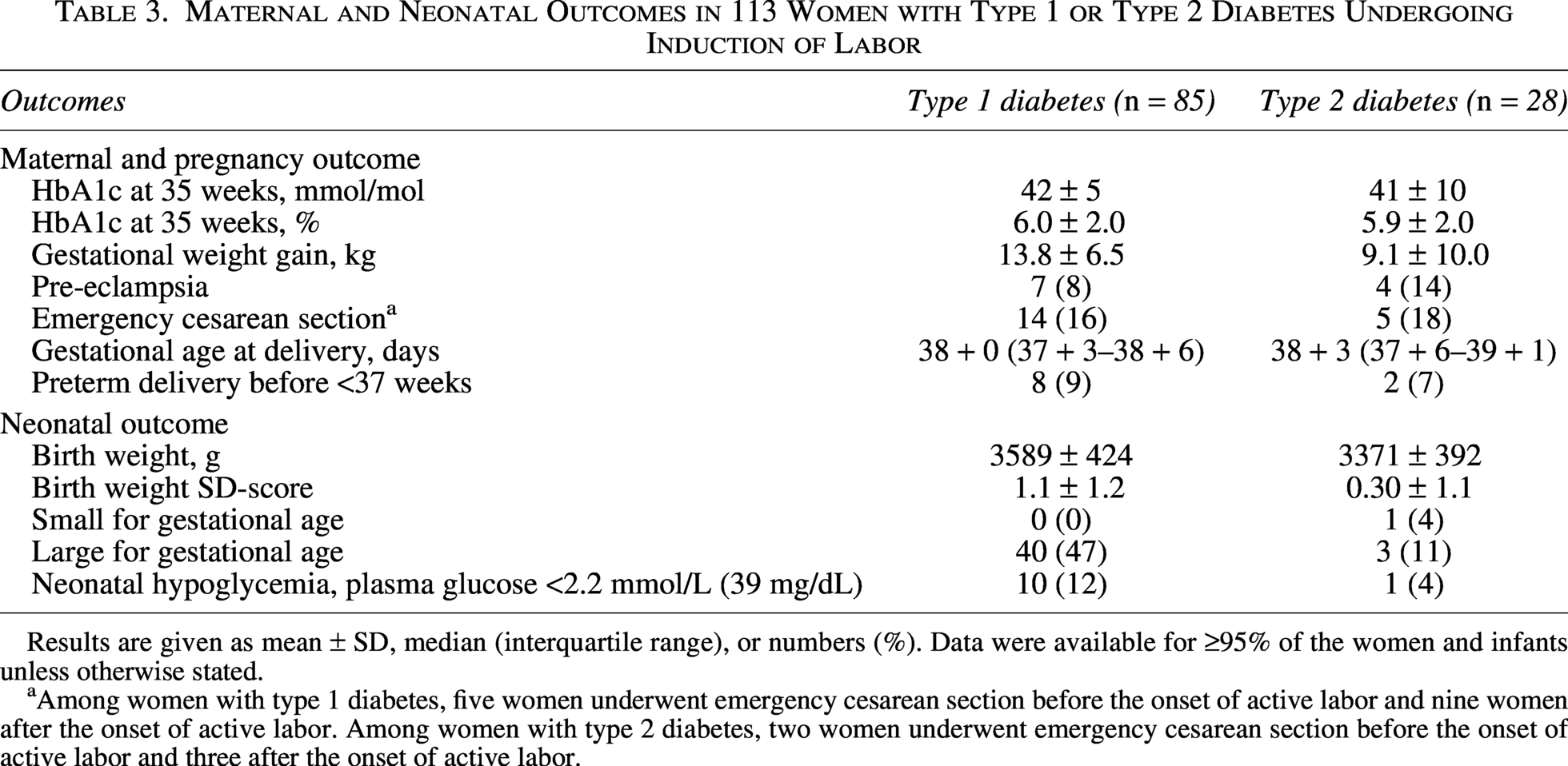
Results are given as mean ± SD, median (interquartile range), or numbers (%). Data were available for ≥95% of the women and infants unless otherwise stated.
Among women with type 1 diabetes, five women underwent emergency cesarean section before the onset of active labor and nine women after the onset of active labor. Among women with type 2 diabetes, two women underwent emergency cesarean section before the onset of active labor and three after the onset of active labor.
Within the first 4 h post-delivery, 28 (33%) women with T1D and 9 (33%) with T2D had at least one glucose value documented in the record. Only one of these glucose values was ≤3.9 mmol/L (70 mg/dL).
Sensor-derived glycemic metrics are presented in Table 4. During induction and active labor, TBRp was 5.6% and 1%, respectively. After delivery, time below range was 7.5% the first 24 h and 8.2% during the subsequent days.
Glycemic Metrics in 58 Women with Type 1 Diabetes Using Intermittently Scanned Continuous Glucose Monitoring from Onset of Induction of Labor until 7 Days Post-Delivery
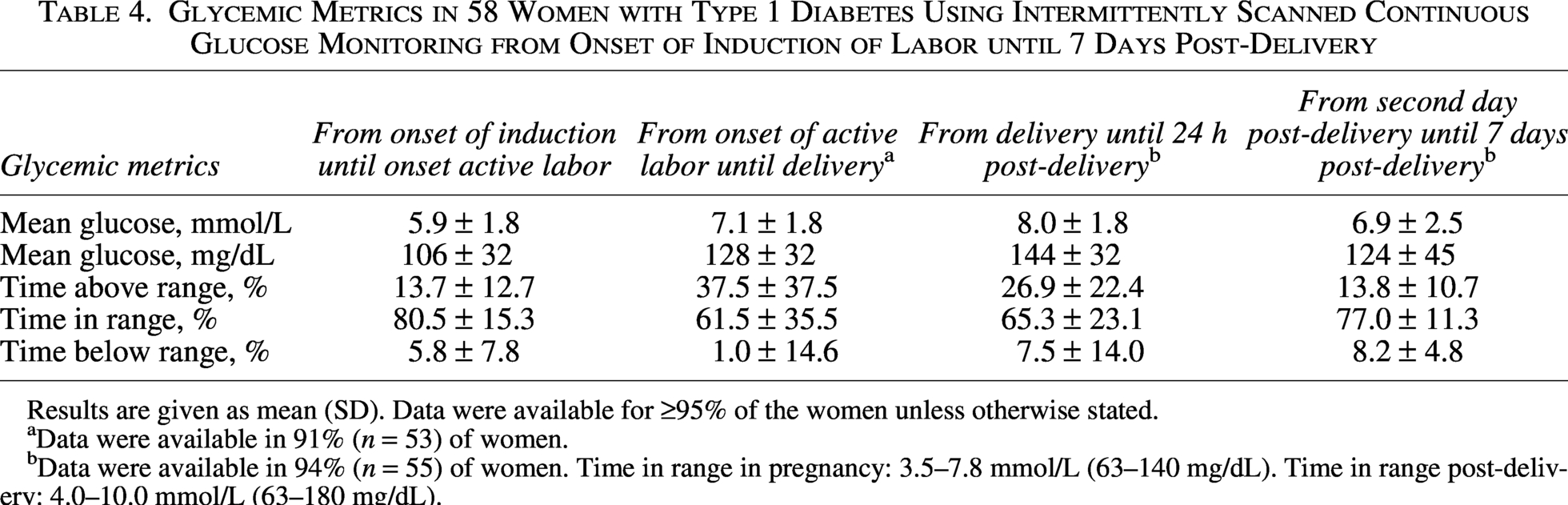
Results are given as mean (SD). Data were available for ≥95% of the women unless otherwise stated.
Data were available in 91% (n = 53) of women.
Data were available in 94% (n = 55) of women. Time in range in pregnancy: 3.5–7.8 mmol/L (63–140 mg/dL). Time in range post-delivery: 4.0–10.0 mmol/L (63–180 mg/dL).
From the onset of induction of labor until 7 days post-delivery, there were no episodes of severe maternal hypoglycemia or diabetic ketoacidosis and no maternal or perinatal deaths.
Discussion
In this descriptive cohort study evaluating a diabetes management protocol with subcutaneous insulin in women with T1D and T2D undergoing induction of labor, maternal glucose levels remained in or close to the recommended target during induction and active labor. The number of hypoglycemic episodes was low, with no episodes of severe hypoglycemia, and the prevalence of neonatal hypoglycemia was low. Among women with T1D using isCGM, the percentage of TBRp was 1% during active labor.
Our diabetes management protocol considered that, during active labor and immediately after delivery, insulin requirements decrease to approximately 70% of prepregnancy requirements.10,34 To minimize the risk of maternal hypoglycemia and ketosis during active labor, a basal supply of carbohydrate was secured via isotonic (5%) glucose infusion at 60 mL/h.
Neonatal hypoglycemia affected 12% of infants born to women with T1D and 4% of infants born to women with T2D, rates that are substantially lower than previously reported.13,14,16,17,35 This may reflect well-controlled diabetes during pregnancy, with HbA1c close to target at 35 weeks and maternal glucose levels in or close to target during induction and active labor, which may have limited excessive maternal-fetal glucose transfer and subsequent fetal hyperinsulinemia in late pregnancy, labor, and delivery. 10 The selected study population, including women participating in the original RCT and undergoing induction of labor, may also have contributed to the low prevalence of neonatal hypoglycemia. In addition, differences in the definitions of neonatal hypoglycemia across studies may have influenced the reported prevalence as well.
The use of CGM during labor and delivery has previously been described only in small sample sizes (n ≤ 27 women).18,36,37 Two of these studies evaluated CGM use during labor in women with T1D using subcutaneous insulin and demonstrated improved overall glucose levels, but no impact on the prevalence of neonatal hypoglycemia compared with use of capillary BGM.18,36
Immediately after delivery and during the first 7 days post-delivery, TBR was around 8.0%, possibly reflecting the well-known challenges of maintaining stable glucose levels in the immediate post-delivery period, particularly during the establishment of breastfeeding.38–40 In addition, the use of isCGM in pregnant women with T1D has been associated with higher TBRp at low glucose levels compared with real-time CGM, which may have contributed to the observed level of TBR. 41 Reassuringly, no episodes of severe hypoglycemia occurred during this period despite the rapid decline in insulin requirements after delivery.38–40 All women were recommended a daily carbohydrate intake of 210 g during breastfeeding to prevent hypoglycemia and ketosis.34,39 Although data on breastfeeding were not collected during the first 7 days post-delivery, 20 we have previously reported that 86%–93% of women with T1D and 86% of women with T2D at our center were breastfeeding at the time of discharge after delivery.42,43
The high time in range and relatively limited time spent in hypoglycemia observed during the first 7 days post-delivery in women with T1D may be attributed to appropriate insulin dose reduction and adequate carbohydrate intake as outlined in the diabetes management protocol.
Target glucose of 4.0–7.0 mmol/L (72–126 mg/dL) during labor and delivery is recommended by the 2015 NICE guidelines and aims to balance the risk of maternal and neonatal hypoglycemia. 9 In this analysis, the maternal and neonatal outcomes were achieved as part of routine clinical care, suggesting that this glucose target during labor and delivery can be safely maintained when supported by a diabetes management protocol with subcutaneous insulin. Our observations, therefore, do not support the recent Joint British Diabetes Societies for Inpatient Care guideline suggesting a higher glucose target of 5.0–8.0 mmol/L (90–144 mg/dL) during labor to prevent maternal hypoglycemia. 10
Strengths of this secondary analysis include the relatively large, prospectively collected cohort of women with both T1D and T2D originating from an RCT, with detailed information on subcutaneous insulin and glycemic data during induction of labor until 7 days post-delivery. To the best of our knowledge, this represents the largest dataset to date examining the use of subcutaneous insulin during labor and delivery. The use of a standardized diabetes management protocol ensured consistent documentation of insulin dosing and glucose monitoring and was applied across a broadly representative cohort, enhancing the generalizability of the findings to other populations. isCGM data were available for 58 women with T1D during labor and delivery and for 55 women during the first 7 days post-delivery, providing a unique CGM dataset with detailed glucose values during induction and active labor until the immediate post-delivery period.
This analysis also has certain limitations. As this study was a secondary analysis, the randomized allocation from the original trial was not preserved. The study population was limited to women undergoing induction of labor, and the findings may therefore not apply to women delivering by elective cesarean section or with spontaneous onset of labor. The number of women with T2D was relatively small, and glucose monitoring data beyond 4 h post-delivery were not available. In addition, data on post-delivery hemorrhage were not collected. Consequently, the effect of women with T2D discontinuing insulin after delivery, as part of the diabetes management protocol, could not be evaluated. Furthermore, isCGM data were only available in a subgroup of women with T1D and reflect older CGM technology, although the observed glycemic patterns and metrics during labor and post-delivery are likely applicable to women with T1D and may be transferable to more modern CGM systems. Automated insulin delivery systems were not approved for use during pregnancy during the study period, and the diabetes management protocol therefore does not address their use during labor and delivery.
Future studies should assess the applicability of this management protocol in women with spontaneous onset of labor and in larger cohorts of women with T2D.
In conclusion, women with T1D and T2D following this diabetes management protocol with subcutaneous insulin during induction and active labor achieved mean glucose levels within or close to the recommended target range, with a low number of hypoglycemic episodes, no episodes of severe hypoglycemia or ketoacidosis, and a low prevalence of neonatal hypoglycemia. Among women with T1D using isCGM, the percentage of time spent below the target range in the early post-delivery period is limited. These findings support the safety and feasibility of maintaining relatively tight glucose control during labor, delivery, and the immediate post-delivery period using this diabetes management protocol with subcutaneous insulin.
Authors’ Contributions
The original trial was initiated by the principal investigator, L.R., in collaboration with senior investigators, E.R.M. and P.D. J.C.S., S.K.N., E.R.M., and L.R. collected the data. J.C.S. performed all statistical analyses and wrote the first draft of the article. S.K.N., K.N., P.D., E.R.M., and L.R. critically read and revised the article. All authors have approved the article and consented to publication before submission. L.R. is the guarantor of this study.
Footnotes
Data Availability
The dataset analyzed during the study is available from the corresponding author on reasonable request.
Acknowledgments
The authors kindly thank all participants in the trial and the nurses Ann-Sofi Lunde, Birgitta Ellingsgaard, Charlotte Barfred, Helle Løvschall, Olga M. Lindeberg Green, Signe Lou-Møller, and Vibeke Ladefoged at the Center for Pregnant Women with Diabetes. The authors also acknowledge Julie Lyng Forman from the Statistical Advisory Section of Biostatistics at the University of Copenhagen and Rigshospitalet and Mads Albrecht Andersen for statistical support.
ChatGPT (OpenAI) was used to assist in the development of visual elements for the graphical abstract. The authors reviewed and approved the final version and take full responsibility for all scientific content.
Author Disclosure Statement
S.K.N. commenced a position at Novo Nordisk on September 1, 2024. K.N. has received funding from Novo Nordisk (grant number U1111-1209-6358) for an investigator-initiated trial with faster-acting insulin aspart in insulin pump-treated adults with T1D and is an advisory board member, for which an honorarium was given to her institution, Steno Diabetes Center Copenhagen. K.N. owns stocks in Novo Nordisk. P.D. has participated in clinical studies on the use of insulin in pregnant women with pre-existing diabetes in collaboration with Novo Nordisk, but no personal honorarium was involved. E.R.M. has received speaker’s fees from Novo Nordisk, received financial support from Novo Nordisk for traveling to one international scientific meeting in the field of diabetes, and has participated in steering committee tasks and guidance involving writing protocols for Novo Nordisk. L.R. has received a grant for AID-DM, an investigator-initiated national multi-center RCT on the use of automated insulin delivery before and during pregnancy in women with T1D. This does not include funding for own salary. Abbott provides Freestyle Libre 3 + CGM devices free of charge for the AID-DM RCT. Ypsomed Diabetes Care AG provides devices for the CamAPS FX system, including mylife Ypsopumps and nonmedical device accessories, free of charge for the AID-DM RCT. LR participated in the European Association for the Study of Diabetes annual meeting 2023 as an invite by Novo Nordisk, serves as the chairperson of the Diabetic Pregnancy Study Group (unpaid), and heads the writing group on the National Treatment Guideline for pre-existing diabetes in pregnancy (unpaid).
Funding Information
The trial was funded by