
Abstract
We present the process of developing a social marketing campaign to promote HIV testing with Black and Latina women living in neighborhoods with high rates of HIV. We developed partnerships with organizations serving women at high risk for contracting or transmitting HIV as well as with experts in prevention, marketing, and research. Focus groups with community organizations’ staff members helped create motivational messages. These data led us to focus on health promotion attitudes toward enhancing well-being rather than on fear-based messages about disease and risk behaviors. Additionally, we determined that to shape norms and self-efficacy, messenger images should be women that the focus audience would identify with as a model of their “best self”—attainable and positive. A series of messages were then pretested to Latina and Black women receiving services at the partner organizations. They confirmed that they did not want to read negative messages or see portraits of women representing their community in a stigmatizing way. Women also related barriers to testing such as fear of medical providers, stigma, and child welfare intervention, which would impact the costs and benefits of testing. Motivations to get tested included availability of health-care services in addition to testing and a “strong/positive” messenger for testing. Materials were distributed in locations that would be coordinated with HIV prevention services of testing, education, and linkage to care. A small-scale evaluation indicated that 14% of women recognized the campaign and 33% of those women said it influenced their behavior.
In the United States, there are large racial and economic disparities among women living with HIV and those at high risk for contracting HIV. In 2013, the national rate of new HIV diagnoses among Black women was 18 times higher than the rate for White women, and the rate for Latinas was 4 times higher than that for White women (Centers for Disease Control and Prevention [CDC], 2015). Black women (62%) also accounted for the greatest proportion of deaths among women with HIV, followed by White women (18%) and Latinas (14%; CDC, 2015). The HIV epidemic in New York City (NYC) shows a similar pattern to national trends. In 2013, there were 552 NYC women newly diagnosed with HIV and most were Black (57%) or Latina (31%), 24% of whom had concurrent AIDS diagnoses (NYC Department of Health and Mental Hygiene [DOHMH], 2014).
In 2013, a quarter (25.5%) of all HIV diagnoses in NYC and almost a third (31.3%) of diagnoses among women in NYC were in Brooklyn. Many of the ZIP codes with high diagnosis rates were also among those with the highest poverty rates, including areas in Central Brooklyn (Williamsburg-Bushwick and Bedford Stuyvesant-Crown Heights). As of 2013, Brooklyn was home to 28,860 people living with HIV/AIDS (PLWHA), 34% of whom were women; among women, 93% were Black or Latina (NYC DOHMH, 2014). Among women who reside in Brooklyn, 27% of those diagnosed with HIV were concurrently diagnosed with AIDS. Among Brooklyn neighborhoods, the NYC DOHMH has highlighted the health needs of Central Brooklyn, where 20% or more of the population lives in high or very high poverty. In Central Brooklyn, the rates of HIV diagnosis and related deaths are among the highest in NYC (NYC DOHMH, 2014; King et al., 2015). Moreover, other sexually transmitted infections (STIs) may be opportunistic for PLWHA or create greater susceptibility to a new HIV infection among those who are HIV negative (CDC, November 2014). Women in Central Brooklyn also have some of the highest rates of gonorrhea and chlamydia diagnoses among women in NYC (DOHMH, 2012).
To help address these disparities, Project Street Beat of Planned Parenthood of New York City (PPNYC) developed a social marketing campaign specifically for women of color to promote HIV/STI testing. In this article, we describe the process of creating this campaign, with a focus on formative research with a unique and high-risk population of women in Brooklyn, NY, for development and pretesting of messages, materials, and placements. We also present data about the dissemination and evaluation of the campaign.
Social Marketing to Women for HIV Prevention
To begin the development of social marketing materials, a team of advertising and public health researchers and program experts collaborated to assess the marketing mix for HIV testing among women in Brooklyn, taking product, price, place, and promotion into account, as suggested by Grier and Bryant (2005). In this case, the product is HIV and STI testing among high-risk women, treatment if testing positive, and continued maintenance of health if negative. Research was conducted to acquire information about aspirations, fears, and social barriers and facilitators. The price of testing in the target neighborhoods is free. Nonetheless, fear, time, and lack of privacy that women may associate with HIV testing in their neighborhoods may create a personal or social cost. Our research gained feedback about these factors and informed placement and promotional products for the campaign.
A preliminary product scan of the environment nationally and, in NYC, specifically in Brooklyn, revealed that social marketing campaigns to prevent HIV have primarily targeted men. Two large-scale reviews of U.S. HIV testing campaigns found that almost none was designed specifically for women (Davis, 2006; Noar, Palmgreen, Chabot, Dobransky, & Zimmerman, 2009). If included at all, women were most often only a minor focus. This indicates a gap, given that one in four people living with HIV are women, and one in five new infections are among women (CDC, March 2014). Further, the social contexts, health-care needs, and perspectives on HIV among women are different from those of men—creating a gap between their unique needs and the focus of most HIV preventive messaging. For example, 84% of women are infected with HIV through heterosexual contact (CDC, March 2014). Furthermore, women face barriers to prevention and treatment such as poverty, cultural inequities, sexual violence, and placing the needs of their families over their own (Denning & DiNenno, 2010; Health Resources and Services Administration, 2012; White House, 2014). Women also experience different clinical symptoms and complications related to HIV infection and most are not in regular care or virally suppressed (CDC, July 2012).
We also conducted a search for HIV prevention campaigns that had been developed to uniquely focus on women in the United States, and we found five. Published evaluation outcomes were available for two; none had published information about formative research. Take Charge, Take the Test was developed by the CDC (http://www.cdc.gov/actagainstaids/campaigns/tctt/) and rigorously evaluated with a randomized and longitudinal sample. Research findings showed greater knowledge about HIV and STIs, intentions to get tested, website visits, and peer-to-peer communication about testing among the intervention group compared to the controls (Davis, Uhrig, Bann, Rupert, & Fraze, 2011; Uhrig & Davis, 2012). The evaluation of the Tu No Me Conoces/You Don’t Know Me campaign (http://www.socialmarketing.com/campaign/tu_no_me_conoces_you_don_t_know_me) showed increases in HIV testing, website visits, and campaign recall (Olshefsky, Zive, Scolari, & Zuniga, 2007). Campaigns that have not yet published their findings include the My Body My Rules campaign from the NYC DOHMH(http://www.nyc.gov/html/doh/html/pr2012/pr027-12.shtml;http://www.pinterest.com/pin/161918549077794369/), the We’re Not Taking It Lying Down campaign for the Women’s Institute at Gay Men’s Health Crisis in NYC (http://www.socialmarketing.com/campaign/we_re_not_taking_it_lying_down), and the Be EMPOWERED campaign that was part of a broader national We Are Greater Than HIV social marketing program that included campaigns for specific groups like this one for women (http://greaterthan.org/campaign/empowered/).
Theory and Background
Fishbein’s (2000) integrative model posits that any given behavior is determined by a combination of a person’s intention, skills, and environment. Further, intentions are influenced by attitudes, norms, and efficacy beliefs. The model predicts that a person will act on his or her intentions if she or he has the necessary skills and abilities, and if environmental barriers are low and facilitators are high. We wanted our social marketing campaign to address these major theoretical components of behavior change, as it recognizes that any behavioral outcome is not just the action itself but the result of a combination of influences, including the action, the target, the product, and the social context.
The main behavioral outcomes we wanted to influence were HIV and STI testing. Using this model to guide our research process, we sought to address both personal intentions and environmental factors relevant to our target population (Black and Latina women in Brooklyn) through this campaign. We set the (1) campaign goal to promote healthy behaviors to address attitudes and norms associated with the intention to get tested, (2) call to action (behavior) to get tested for HIV and STIs (product), and (3) population as Black and Latina women ages 20–44, segmented to those living in Brooklyn neighborhoods, with high prevalence of HIV to investigate the environmental barriers specific to these women. It was important for our campaign to also address environmental barriers and facilitators, thus we collaborated with community partners. HIV and STI testing attributes specific to our research partners and other health-care providers who would host the campaign where women would be referred for services were confidential, no cost, rapid testing (oral swab, urine, and blood) in clinics, mobile medical units (MMUs), and other street-based outreach.
In our focus groups, we discussed topics that may be associated with attitudes about testing, efficacy beliefs, and social norms within that population. Willingness to test was discussed, including knowledge of transmission risk and testing access and emotional and social factors. A secondary action was the use of condoms; however, getting tested was the primary action because it was the most specific behavioral outcome under the control of women themselves, while getting men to use a condom is more of a goal for women (Fishbein & Cappella, 2006). We conceptualized the context more broadly than the sexual relationship, which is often the focus of HIV prevention campaigns, since our goal was health promotion. We chose the Brooklyn neighborhoods of East New York, Bedford Stuyvesant, Crown Heights, Brownsville, and Bushwick because they were designated as priority area zip codes by the NYC DOHMH for high prevalence of HIV and STIs with associated cofactors of poverty and substance abuse (NYC DOHMH, 2014). Women in these contexts have less control over sexual risks due to economic dependency on and violence by men (White House, 2014).
Program Planning and Stakeholder Engagement
Developing a social marketing campaign involves a program-planning process that applies advertising concepts to promote behavior changes that benefit both individuals and society (Grier & Bryant, 2005). We wanted to develop a campaign to encourage HIV and STI testing as well as promote overall health care for both women living with HIV and those who are HIV negative. The overarching goal was to decrease HIV transmission and improve health outcomes among women already living with HIV, and we followed strategies that had been effective in other HIV prevention campaigns (Dearing et al., 1996; Noar et al., 2009; Tucker, Fenton, Peckham, & Peeling, 2012).
In order to incentivize health behaviors and reduce barriers associated with testing, we planned to connect the campaign to community resources for HIV/STI screening and prevention, education, and linkage to health-care services. To do this, we segmented the audience to Central Brooklyn and created partnerships with community-based organizations (CBOs), serving the highest risk women in these neighborhoods. Three large CBOs and their clients participated in campaign development: a methadone maintenance clinic, a homeless shelter for mentally ill and chemically addicted women, and Project Street Beat. The first two were selected because their provision of HIV and STI services was limited, and therefore the campaign would mobilize these settings to work closely with the third partner, Project Street Beat, which specializes in HIV preventive services for women.
PPNYC launched Project Street Beat in high HIV prevalence neighborhoods of the Bronx in 1988 and expanded services to Brooklyn in 1990. Project Street Beat specializes in HIV preventive services for women. It is a nonprofit organization that regularly engages in community mobilization activities, which include integrating clients into program planning and implementation, networking with HIV and non-HIV organizations serving a variety of social needs, and providing leadership at the city and state levels for HIV awareness, social activism, and public policy. Traveling in minivans and an MMU, the Project Street Beat reaches individuals who live or work on the street, are distrustful of traditional health and social service venues, and therefore do not seek the care they need. Project Street Beat primarily serves individuals who have little or no income and whose HIV risk factors include sexual activity without condoms; injection drug or other substance use; and a history of trading sex for money, drugs, food, or shelter. Many clients are unstably housed or homeless. Clients are 96% Black (including consumers who identify as both Latino and Black) and 52% are female. They have a wide age span but most are 20–49 years old (57%). Project Street Beat provides street-based outreach and prevention education; basic medical and reproductive health care including STI screening and treatment on its MMU; support groups, case management, and comprehensive risk counseling; evidence-based interventions; mental health counseling; syringe access and opioid overdose prevention training; HIV rapid testing, confirmatory testing, and linkage to HIV primary care at partner providers; and referrals to other services that are not offered by Project Street Beat such as the housing and addiction treatment provided by our community partners for this social marketing project.
The next step in the campaign was to plan formative research to collect data from staff and client stakeholders at each of the three community partners. Research methods and findings are described below and were used for development and pretesting of messages, images, products, and placements for the campaign. For this stage, we added researchers and communication experts from PPNYC and Better World Advertising (BWA) to work with the community partners. We then launched the campaign in the selected neighborhoods through events, posters, pamphlets, promotional materials, street outreach, and HIV testing. Dissemination was tracked with standardized measures, and outcome data were collected through street interceptor interviews. The evaluation was a partnership between NYC DOHMH and PPNYC.
Method
Design and Sampling for Formative Research
We collected qualitative data from focus groups by using Fishbein’s (2000) integrative model as a deductive foundation for creating discussion guides, which were focused primarily on motivations, norms, and environmental constraints for getting tested for HIV and other STIs and for utilization of health care. For the development of initial concepts and messages, we conducted three groups with direct service staff employed at one of the three partner organizations (N = 24: 7, 8, and 9 per group). Each group was conducted at the respective organization from which staff were recruited (i.e., at Project Street Beat, at the methadone maintenance clinic, and at the homeless shelter). Organizations were paid US$500 for use of space, assistance with recruitment, and lost staff time for the 90 min of group discussion. Food was provided for the staff during the discussion time. No individual incentives were paid. Organizational administrators invited direct service staff who worked primarily with adult women at high risk for contracting HIV or who were already HIV positive. Staff were allowed to participate in the discussion during work time but were not required to do so (i.e., participation was voluntary with informed consent). No administrators or staff supervisors participated in or observed the focus groups. We began with staff rather than consumers because these initial sessions were more open, less structured, and focused on personal messages they had used to motivate clients to increase healthy behaviors. Further, we discussed barriers they perceived for clients’ utilization of health care. A series of messages and images were designed by BWA and PPNYC based on these data.
We then pretested messages and images with three new focus groups of English-speaking-and-comprehending Black and Latina women, ages 20–44 who were receiving services from one of the three partner organizations (N = 21: 8, 6, and 7 per group). We tested different messages and images and asked for input about community venues and promotional materials (e.g., palm cards, posters, coin purses, shoulder bags, etc.). Each group was conducted at the respective organization from which clients were recruited. Women were recruited by the same administrators who recruited staff participants. Participating women were given food during the 90-min discussion, a round-trip NYC transit card (US$5), and a US$25 gift certificate to a food and clothing store. Participation was voluntary with informed consent without relation to the receipt or denial of any other organizational services. No staff from the host organization participated in or observed these client focus groups.
All focus groups were cofacilitated by a researcher and an HIV services expert and observed by a communications expert. Groups were audiotaped and transcribed verbatim into Word documents. Institutional review board approval was obtained for the use of human subjects in research. Groups were held in private conference rooms at each organization. Staff development focus groups were held in the summer of 2013, and client pretesting groups were held in the fall of 2013. The campaign was launched in 2014.
Measures
A semistructured focus group guide was developed to inform initial concept and message development and to gain information related to attitudes, knowledge, and environmental constraints related to the target behavior. The focus group guide was organized around the following areas: (1) messages and motivational strategies used when talking to clients about preventive health care, in general, and willingness to test for HIV and STIs and adhere to medical treatment, in particular; (2) clients’ barriers to preventive health behaviors; (3) knowledge of health-care services related to testing and treatment; and (4) trusted messengers about health-care information.
As a result of the initial focus groups, four social marketing concepts were created, which comprised eight different images of women with different color backgrounds. A focus group guide for pretesting the messages and images was structured to gather feedback in a systematic way about four social marketing concepts, specifically related to motivational messages and images that would be relatable and support a social norm for testing. First, we tested main messaging only and then messages plus subtext, without any images associated with the words. We did this to gain reactions to messages and images separately, so as not to confound exactly what the women were reacting to with too much stimulus presented at one time. The order in which we presented the messages was randomized for each focus group. The main messages tested were as follows:
Your Body Needs You It’s Your Time Be Negative Stay Negative
The subtexts tested were the following:
To Get Checked for Sexually Transmitted Diseases (STDs) To Get an HIV Test To Stay STD Free Use Condoms/Get Tested for HIV/Stay STD Free
Second, we paired the messages with different images of women and background colors. We asked women, one by one, to give a simple rating of each concept from 1 = I do not like at all to 5 = I like it very much. Then we facilitated a thorough group discussion about what aspects they liked, did not like, and would change. Finally, we solicited feedback about where they would like to see posters and palm cards (dissemination and product placement), and what types of promotional materials with prevention messages would be desirable (e.g., safer sex supplies, hats, bracelets, coin purses, etc.).
Formative Research Results
Group discussions were audiotaped and transcribed verbatim. Two researchers coded transcripts using a grounded theory approach to identify categories and themes emerging across the groups. Categories and themes were then compared for validation and determination of final results. Final themes were determined to be those that emerged across all six groups (for both development and pretesting) and then used to create concepts that would have common appeal across our partners and neighborhoods. Fishbein’s (2000) model was used to guide categorical coding to focus on attitudes about receiving testing and medical care in general, norms regarding who should serve as messengers (images) to promote testing, and environmental and social stigma barriers to testing.
Concept Development
Table 1 presents categories and themes that emerged from the message development focus groups with direct service staff across the three partner organizations.
Categories and Themes Emerging From Message Development Focus Groups.
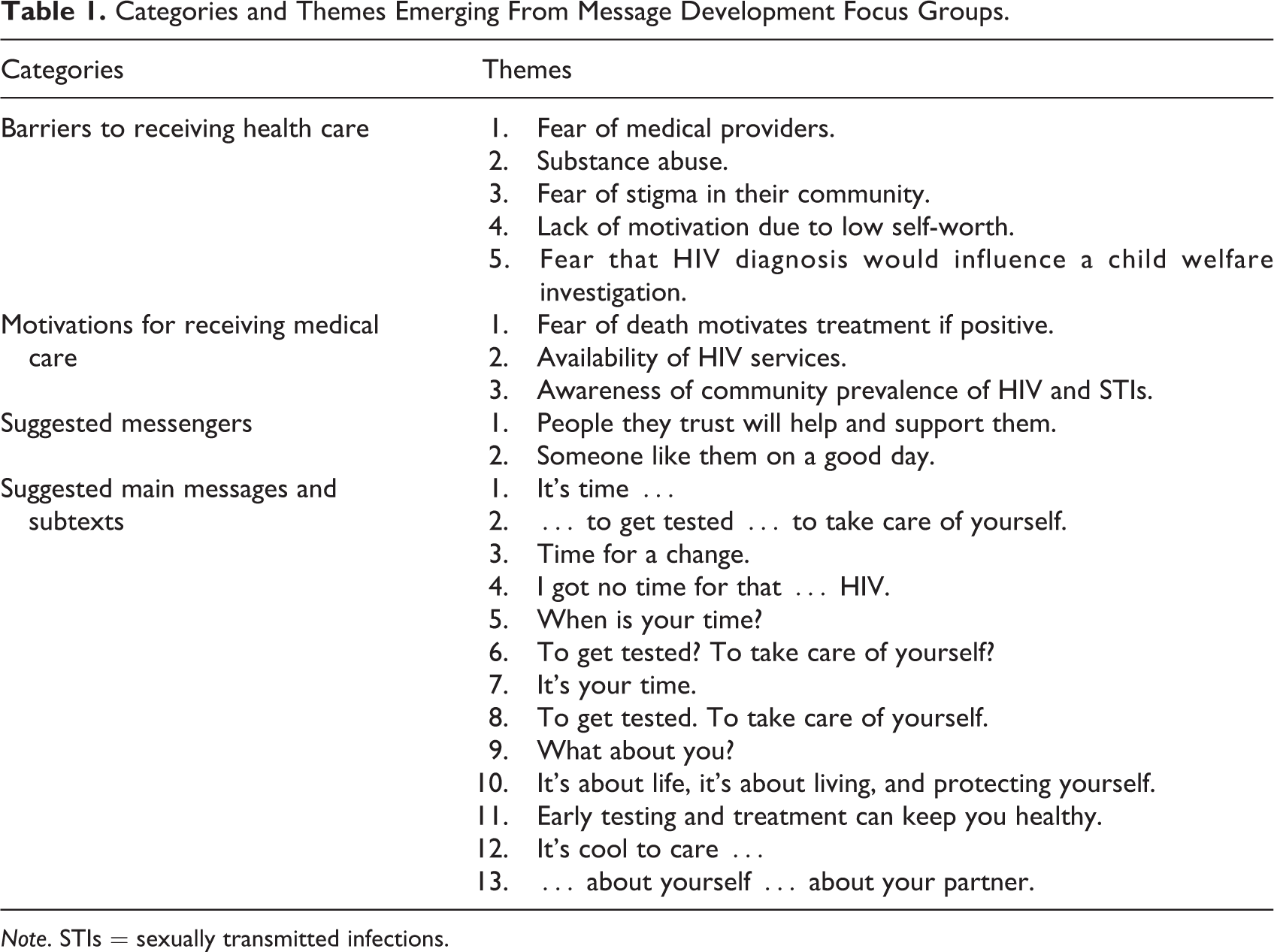
Note. STIs = sexually transmitted infections.
Barriers to screening
Five themes emerged that related to barriers to screening. First, staff said that their clients express fear of medical providers, which prevents them from disclosing their sexual health behaviors and needs. They fear that if they disclose the need to be tested for HIV or STIs to providers, they will be emotionally and medically mistreated through moral judgment and disregard of their well-being. Second, substance abuse created barriers to remembering health appointments and caring about their overall health. One staff person said, “Being more motivated to get high than go to the doctor is a real problem for women who are addicted to drugs.” Another commented that, “substance use is often a coping mechanism for dealing with an existing HIV diagnosis or other illnesses. They don’t want to think about it.” Similarly, another staff member added, “HIV is a motivator to take better care of their health, but most want to get high so that they don’t think about it.” Third, staff reported that clients fear being stigmatized in their community. If they are seen in the shelter or at a nearby MMU waiting for HIV/STI screening, people will gossip about them and presume there is something wrong with them. Fourth, lack of self-worth was discussed as a barrier to taking care of themselves in many ways, including medically. One staff person related, “They feel like nobody cares about them, so why should they care about themselves.” It was suggested that the campaign not make women feel judged or fearful that they have HIV or another disease, but that they are important, that someone (i.e., via the campaign) is concerned about their health, and that they should care about it too. The fifth was fear of losing children to child welfare; for example, a staff person commented, “They believe that if they are diagnosed with HIV, it will be used against their ability to parent their children in an already difficult [social] context.” Staff stated that if their clients were not already involved in an open-case investigation, they knew women who were and feared that a medical provider would report them if they tested HIV positive. Further, many of their clients were already involved in the child welfare system, often trying to regain custody of a child, and feared that being HIV positive would be used against them by government workers or their families as a reason why they could not be good parents.
Motivations for screening and health care
Three themes emerged that related to motivations for screening and follow-up medical care. First, staff participants felt that fear of death was a motivator for medical care for women who are HIV positive and for those who are negative but at high risk for contracting HIV. It was noted that their clients were concerned about who would take care of their family members if something happened to them or if they were sick. For social messaging, though, staff recommended staying focused on living a healthy life rather than messaging about death. Further, most people felt that HIV should not be a prominent part of any message because it created too much fear and stigma and would be a “turn off” to the women they serve. Further, they felt that associating HIV directly with women of color would make them feel “targeted and diseased.” There was discussion about taking care of the needs of oneself and the needs of others and the motivation to stay alive in order to do that. Second, staff thought it would be helpful to raise awareness of the availability of medical and social services for PLWHA, commenting “If they knew help would be available, they would be more motivated to get tested.” A staff member noted that many of her clients do not know that medication can manage the disease and reduce the likelihood of onward transmission and becoming infected with other STIs. The clients did not know that other food, housing, and social support were available for HIV-positive women. One staff member reported motivating her HIV-positive clients to receive medical care and adhere to medication by saying, “Perhaps there will be a cure someday and you can stay healthy until then.” Another staff commented that, “For many HIV-positive women, the virus has stabilized their lives through access to medical care, food stamps, housing, and social services. More women should understand this is possible.” Third, staff members believed that having more knowledge about the prevalence of HIV, STIs, and viral hepatitis in their community would motivate them to get tested. One stated, “Many believe that these infections will not happen to them, they should know it’s all around them.” Another noted that, “women still think this is a gay man’s disease and don’t know how they might be at risk.”
Messengers
Two themes emerged related to who would be effective messengers for the campaign. First, staff agreed that women trust those who they perceive as “helpers,” that is, “service providers who they trust or believe would not judge them,” “people they view as wanting to help them,” and “people who will listen to them, support them, encourage, and convince them.” Medical providers were not seen as helpers per se, and they advised staying away from images of doctors or nurses. Second, staff believed that, “They would listen to someone like them.” They said a campaign image should be “like they’re the ones giving the advice to someone like themselves.” However, it was strongly noted by most participants that it would need to be an “inspirational peer … like their best self—like the person they want to be.” Staff explained that this would not be a person who reflects clients’ highest life aspirations, but one they thought was “like me on my best day.” There was discussion of whether men/male images as messengers would be effective, and most participants said that the women they serve “fear men” or “don’t expect them to do what’s in their best interest.” They thought that the best option would be images of women with whom their clients would relate.
Messages
Quotes of specific message suggestions are presented in Table 1. Although there were some suggestions about using images or messages about infection to grab attention or create fear, overwhelmingly staff members suggested showing positive images of women and messages that were health promoting and esteem enhancing within the context of their lives. Participants emphasized speaking “in their language” without medical details, jargon, or statistics. They emphasized strong use of color and simple images with few words, noting that many clients had low literacy skills. The campaign should suggest that “you matter” and “we’re talking to you.” Also, it should focus on what to do, rather than what not to do, and on what was in their control.
Message Testing
Table 2 presents a summary of results from the message testing focus groups with agency clients. Four main messages, four subtexts, and eight images were tested. Main messages were created to be the motivational message, the subtexts to be the call to action, and the image to be the messenger. Of the four main messages tested, one stood out as the clear favorite: “Your Body Needs You.” Most women across all three groups responded positively to this as noticeable and motivating. One person noted that, “We see negative [social marketing] messages all the time in our community about sickness, crime, and drugs. I want to see someone say something positive about our health. Make us care about it. Make us feel like somebody cares.” Other comments included, “It opens your eyes,” “you can see this and go, oh yeah!” “I like this, without your body [being healthy] you are lost,” and “It is letting us know we should get tested for our health.”
Summary of Main Message Testing.
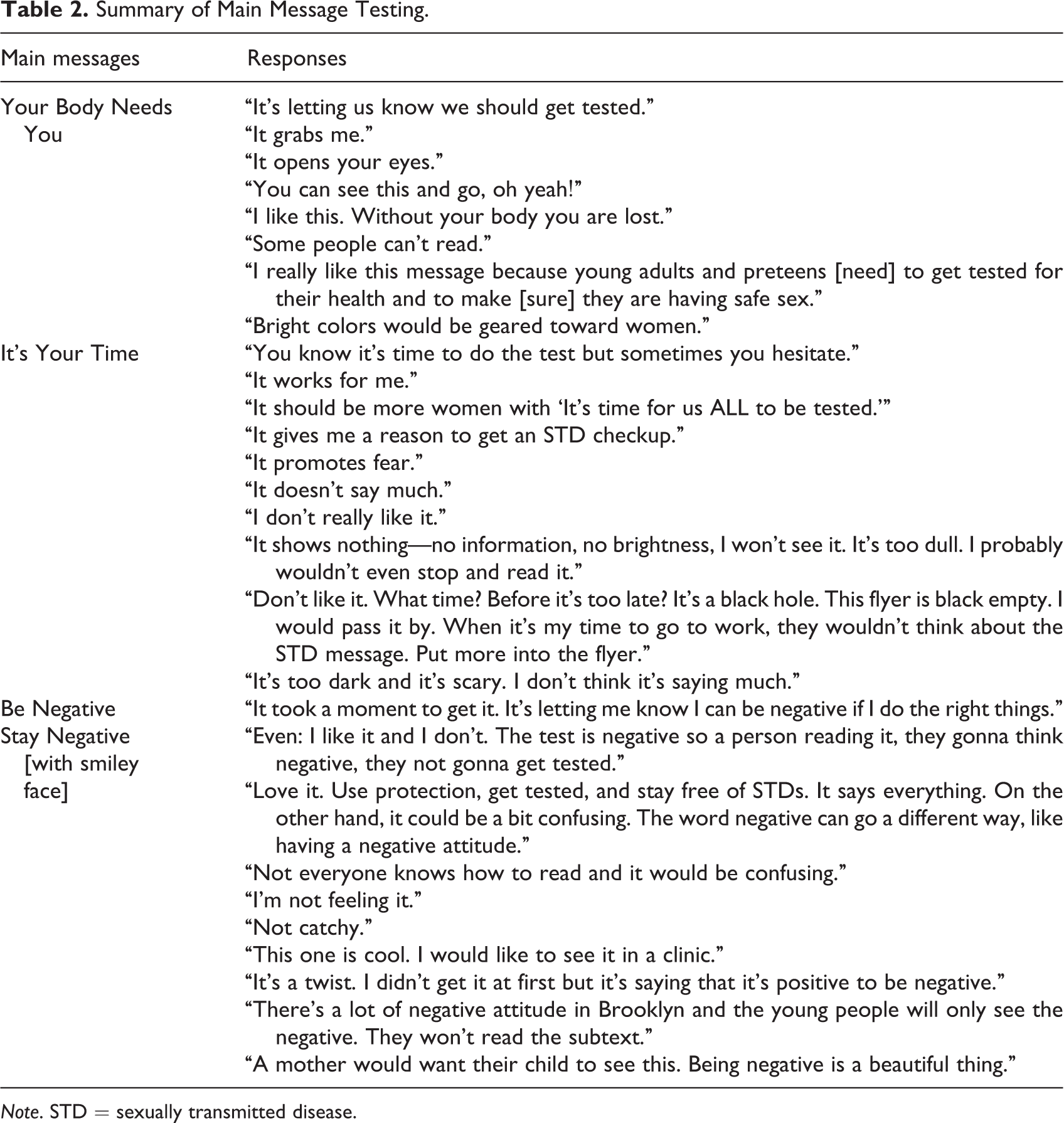
Note. STD = sexually transmitted disease.
There was considerable fear-based reaction to the message, “It’s Your Time,” but it did generate a lot of attention and discussion from women in the groups. One woman said, “It makes me feel like something bad is going to happen or if I get tested it will only be bad news.” Other comments were “It’s what time? Before it’s too late? It’s like a black hole,” and “It’s a dark message that doesn’t say much.” Participants suggested changing the message to, “It’s time for women’s health.”
“Be Negative” and “Stay Negative” were two similar versions of a message paired with a smiley face drawing to connote positivity and happiness by taking actions to achieve negative HIV and STI test results. Women liked the concept and thought it was funny, but that it required too much time to think about its meaning. Some found it confusing, saying, “It would work well in a testing clinic, but on a sign, I wouldn’t understand what it meant,” and “People in our community have very negative attitudes about things in general, I don’t think it will get a healthy message across.”
Regarding the subtexts, women did not like “get checked” as a directive, nor did they want to see “HIV” on any messages, especially not by itself without additional context. Comments included, “It shouldn’t say anything about HIV because when people see the word ‘HIV’ they get scared.” “Don’t focus on Black women and HIV, it’s stigmatizing.” “When you go to a clinic and they ask you if you want an HIV test, you just say ‘no, I don’t need that.’ But it’s important.” Most women liked the concept of staying disease “free” and thought that it paired well with the “Your Body Needs You” message to stay healthy. When we put all three together with condom use as a subtext, “Use Condoms/Get Tested for HIV/Stay STD Free,” women had positive responses: “It’s broader than one thing.” “HIV is less scary when you put it with other messages.” “It tells you several things you can do.”
Images
A series of female images was reviewed by focus group participants. We asked the women to give open-ended responses to each image and to vote for the one they liked the best. The final two images were selected because the women had the most positive responses to them, including, “I could be her … when I’m feeling good.” “I think younger and older women would relate to her.” “She looks like she just got tested, and can handle it!” Comments about images that were not selected for the campaign included, “She looks like a party girl, not someone who would get tested.” “She looks like a victim.” “She looks like me when I was sick, and that’s not motivating … like she’s strung out.” “She looks afraid.” “She looks like a sucker.”
Materials and venues
We asked the women what types of materials would remind them to get tested and engage in healthy behaviors, such as posters, postcards, and branded items. We asked what kinds of items they would carry around and would cause their friends to ask about or where they got it, such as coin purses, bags, and so on. We also asked where they and others in their community would see posters, pamphlets, public advertising, or other materials about the campaign. Table 3 lists suggested materials and distribution venues.
Suggested Campaign Materials and Distribution Venues.
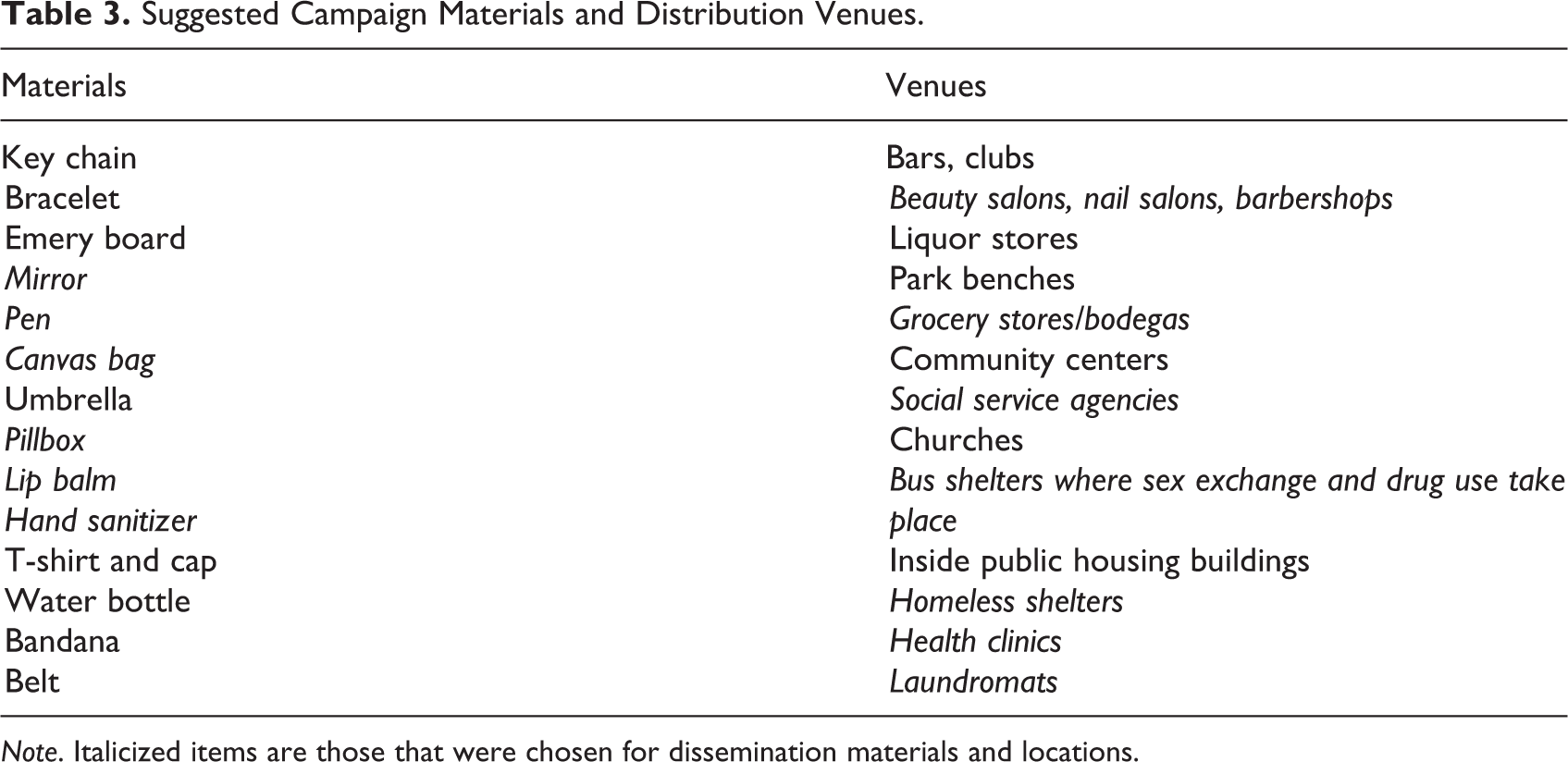
Note. Italicized items are those that were chosen for dissemination materials and locations.
Campaign Dissemination
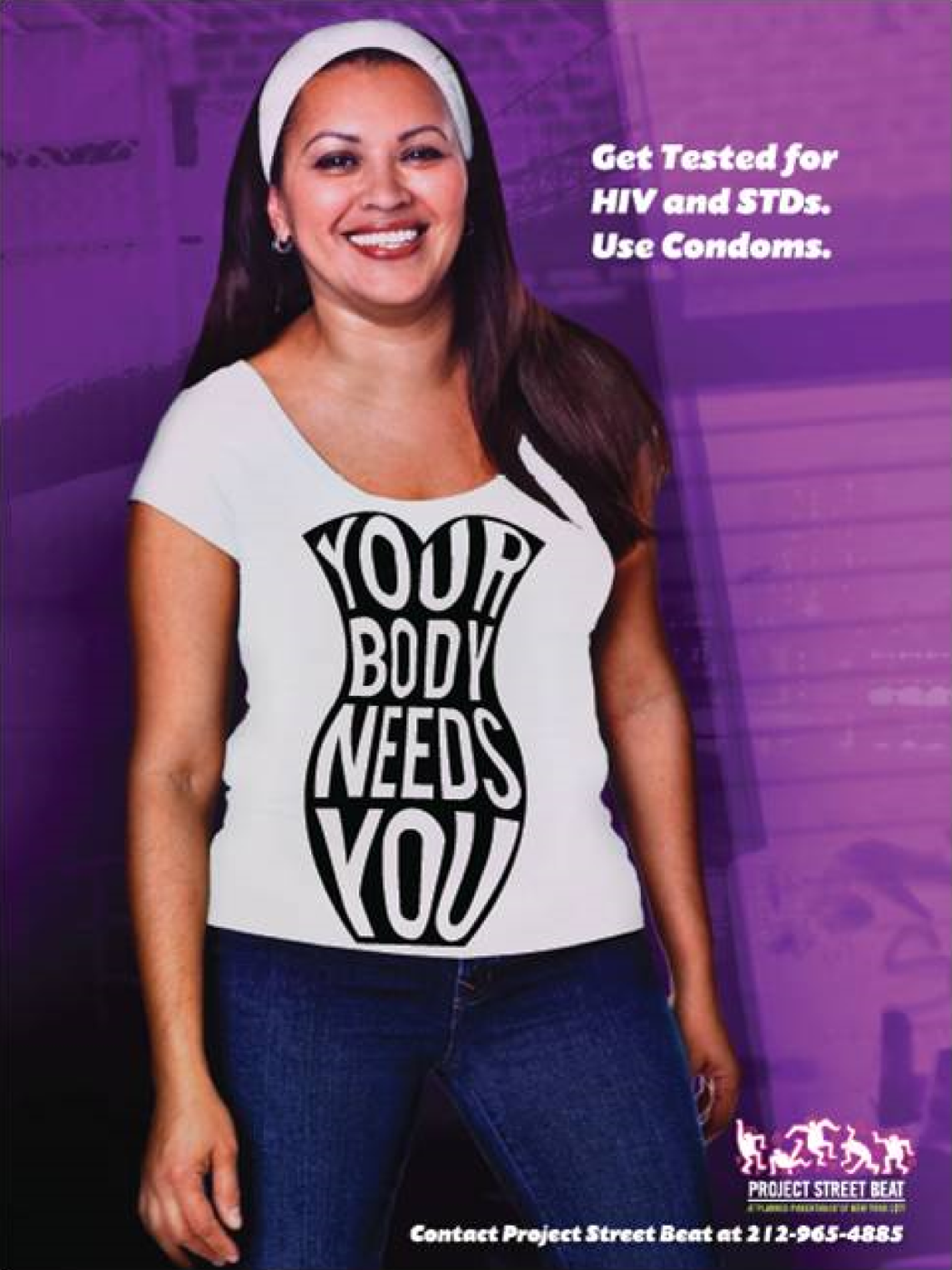
Two images were selected for the campaign concept, “Your Body Needs You.” The call to action messages were “Get tested for HIV and STDs. Use Condoms” (Figures 1 and 2). A small logo was also created for use across different branded items (Figure 3). The final campaign materials include 12 × 18-in. posters and bus shelter advertising. A 4 × 6-in. postcard carried the image on one side, and Project Street Beat’s list of services and contact information on the other side. Branded products with the logo and messages (no images) include lip balm, compact mirrors, tote bags, and a coin purse. Posters for display and postcards for pick up are distributed periodically to CBOs and health centers (where helpers could support our message) and businesses such as beauty parlors and bodegas. Branded products are distributed at street outreach testing and educational events, with the larger items (i.e., tote bags and coin purses) sometimes distributed as incentives for receiving a service and smaller items (i.e., postcards, lip balms, mirrors) packaged together with other incentives (i.e., food and personal hygiene supplies) or safer sex supplies (i.e., male and female condoms, lubricant). The main message, Your Body Needs You, speaks to our health promotion goal with women, which sets a positive tone for testing and condom use calls to action. The promotional materials convey positive, nonfear based modes of carrying the messages within community venues that women perceive as supportive (educational, social service, and social sites) and nonmedical, but where communication about aspects of HIV/STI testing (access/referral, cost, methods, and timing) can take place in a nonstigmatized way.
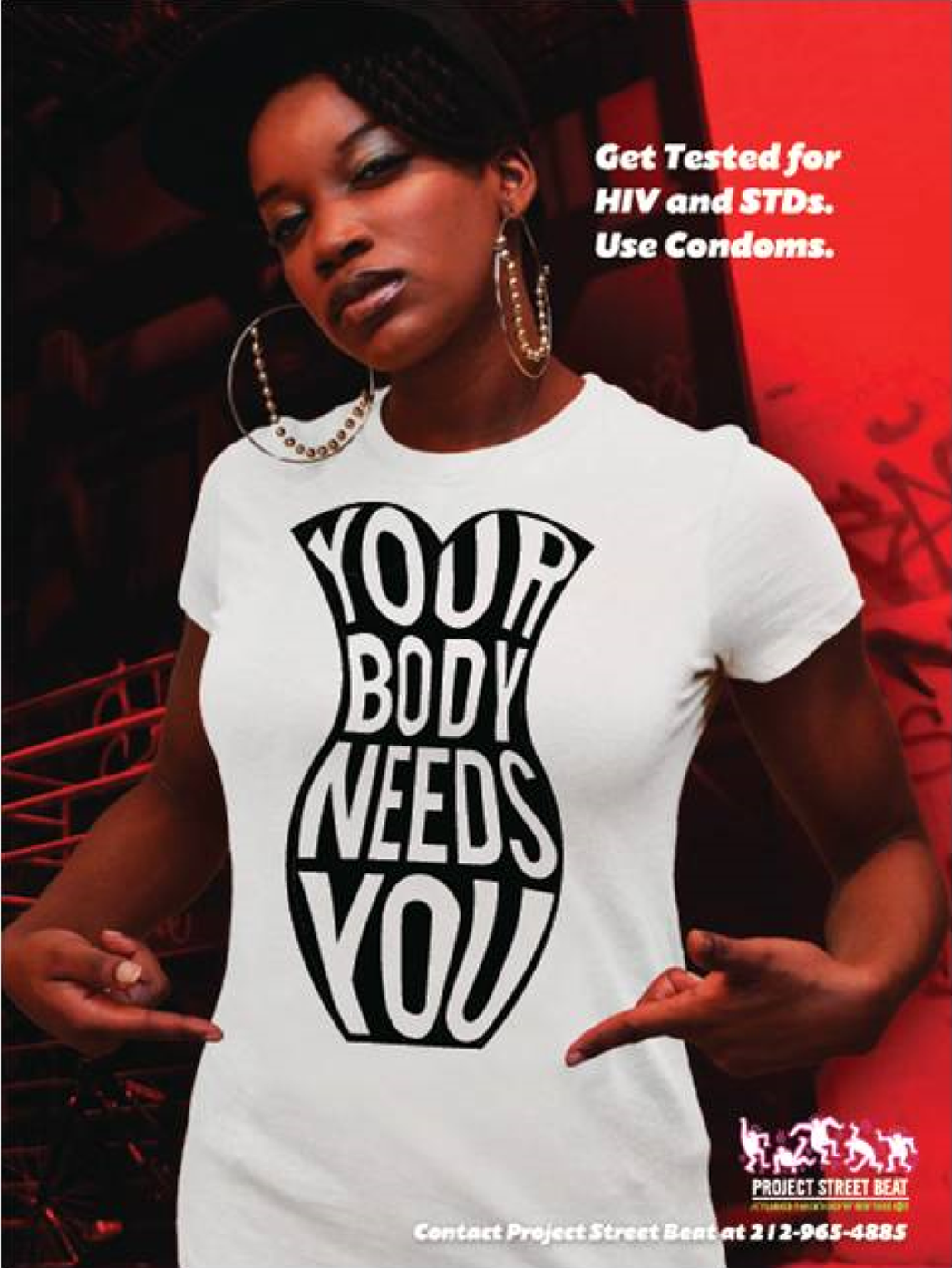
Campaign concept image 1.
Campaign concept image 2.

Logo.
Additionally, to respond to the data indicating the need to raise awareness about the prevalence of HIV and STIs among women in the focus communities, we developed a fact sheet for distribution at CBOs to inform staff members and the clients they serve. Further, a number of HIV and STI prevention and treatment educational sessions tailored to staff members at our partner organizations and to their clients were conducted by Project Street Beat health educators. The campaign was paired with information about HIV and STI testing services via clinics, MMUs, and other street-based outreach within the neighborhoods that provide confidential, no cost, rapid testing.
Dissemination of campaign products was tracked on standardized reporting forms. Project Street Beat’s outreach manager recorded counts of materials distributed during the course of street-based outreach and HIV testing by location (address or intersection) on daily work logs, which a researcher compiled into monthly summaries of materials distributed by ZIP code. Materials distributed to local businesses, other community organizations, and at campaign testing and educational events were tracked (i.e., material type, quantity distributed, location) by program staff members and recorded by the researcher on forms created for these purposes. An overview of materials disseminated during the first 17 months of the campaign is provided in Table 4.
Summary of Campaign Dissemination Activities, Brooklyn, April 1, 2014, to August 31, 2015.
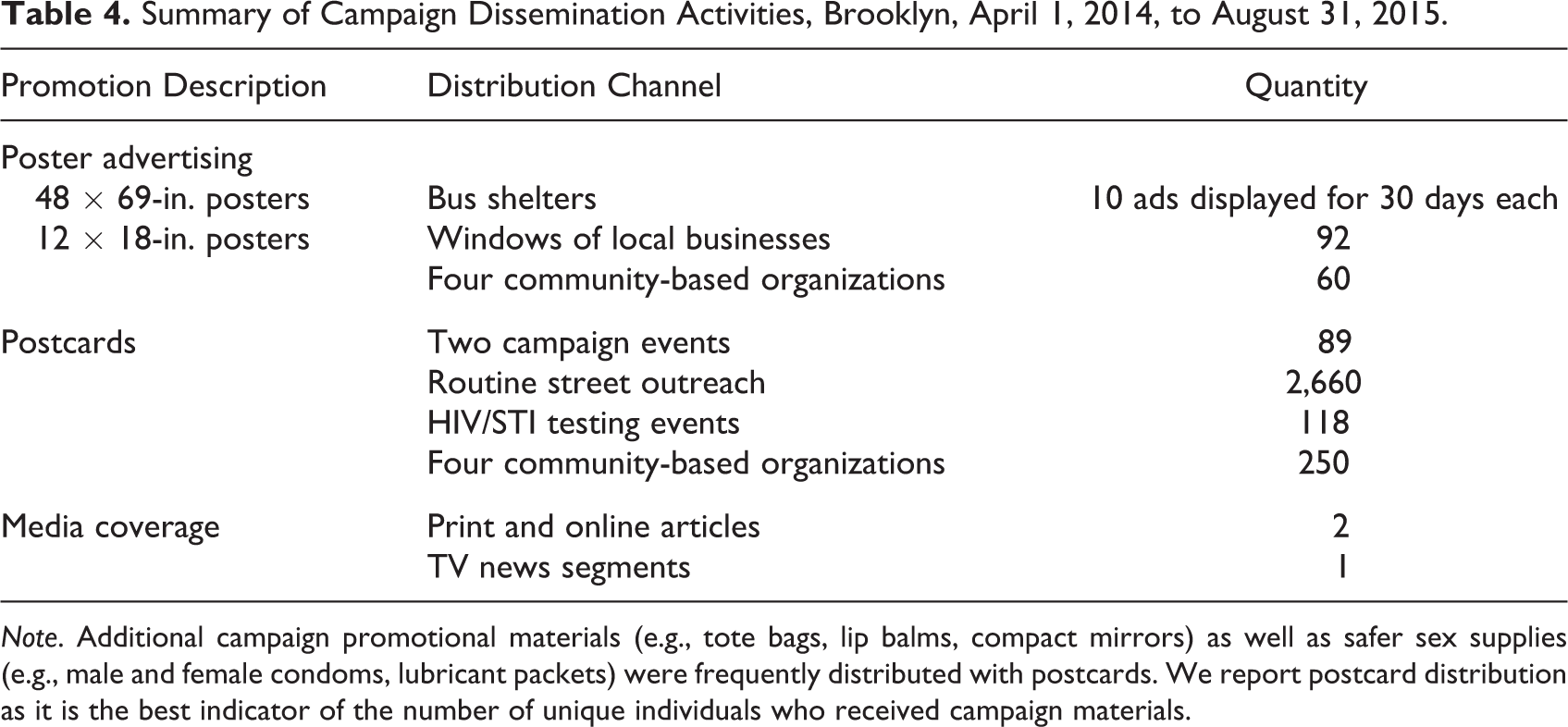
Note. Additional campaign promotional materials (e.g., tote bags, lip balms, compact mirrors) as well as safer sex supplies (e.g., male and female condoms, lubricant packets) were frequently distributed with postcards. We report postcard distribution as it is the best indicator of the number of unique individuals who received campaign materials.
Evaluation
The evaluation was a partnership between NYC DOHMH and PPNYC (K. Scanlin & N. Mensah, personal communication, January 11, 2016). We allowed 14 months of exposure in the selected neighborhoods before collecting outcome data through street interceptor surveying. Recruitment locations were chosen street corners where the social marketing materials, especially bus shelter ads, had been disseminated and HIV educational and testing outreach had taken place. These were predicted to be areas where Black and Latina women who are at higher risk for HIV could be found, including food pantries, shelters, and neighborhoods with high disease burden.
The structured survey consisted of 31 questions, which addressed demographic characteristics, recent HIV testing, attitudes about HIV, and exposure to the Your Body Needs You campaign and its motivational impact. Data were collected during eight 4-hr-long data collection sessions, on weekday afternoons and evenings between June and August 2015. The data collection target was 300 surveys.
The street intercept survey was administered in English and Spanish by surveyors trained by the NYC DOHMH and required 5–6 min to complete. All participants provided informed consent, and no incentives were offered for participation. Of the 2,005 persons approached, 384 were willing to talk to a surveyor and 276 met eligibility criteria of 18–64 years of age, female sex at birth, NYC residence, and consented to participate in the survey.
Of the 276 women completing the survey, 98% spoke English; 60% identified as African American/Black, 29% as Latina/Hispanic, 7% as White, and 10% as Other (participants could choose multiple categories); 29% were foreign born; 11% had not received a high school diploma or Graduate Equivanlency Diploma (GED); and 68% reported sex with a man in the prior 6 months (the primary mode of HIV transmission to women). When shown photos of the marketing materials, 14% (n = 39) of women said they had seen the campaign. A third of the women who saw the campaign (33%; n = 13) said that it motivated them to take at least one action. Most frequently reported actions were using a condom, getting an HIV or STI test, asking a sexual partner about their HIV status, and/or using an Internet search to find information about sexual risk.
Discussion
Social marketing to promote HIV testing among women has largely been ancillary to male-focused campaigns. Yet, recommendations for best practices have pointed out the need for careful development planning to clarify segmented audience needs (Maibach, Kreps, & Bonaguro, 1993) and the integration of public health and advertising to create a marketing mix that will promote both the individual and the social good (Andreasen, 1995). This includes input on product design and messaging, price, placement and promotion, or distribution. Further, successful campaigns should start from a theoretical framework and use accepted methodologies for (1) conducting formative research, (2) pretesting of messages, (3) audience segmentation into meaningful subgroups, (4) determining channels of dissemination, and (5) dissemination and outcome evaluation (Noar et al., 2009).
We presented formative research based on Fishbein’s (2000) integrative model outlined for HIV prevention campaigns. First, we selected the audience of women living in central Brooklyn, NY—a public health priority area for prevention, given its high incidence and prevalence of HIV and AIDS among Black and Latina women. Second, we developed partnerships with community stakeholders (direct service staff of CBOs providing services to high-risk women as well as the service recipients themselves) and HIV specialists across prevention, marketing, and research. Third, we conducted focus groups with staff members to help us create motivational messages. These data led us to develop messages to increase self-efficacy by focusing on promotion of health and positive messaging about how to enhance well-being rather than on fear-based messages about disease and risk behaviors. Further, group participants helped us to determine that the messenger images should be women that the audience would identify with as a model of their “best self”—attainable and positive. This would serve as a social norm that is immediately attainable rather than an aspiration for the more distant future. Fourth, a series of messages were pretested on clients at the partner organizations. They indeed confirmed that they did not want to read negative messages or see portraits of women representing their community in a stigmatizing way. They also confirmed that the images should look like “someone I could be on a good day,” confident and able to “handle getting tested.” Women also suggested materials and distribution venues in their neighborhoods. Finally, we believe that if these norms are paired with increases in environmental facilitators, the behavior would be strongly supported. We planned for resource management and program development to produce and distribute materials in locations that would be coordinated with free, preventive community services of testing, education, and linkage to care via clinics, MMUs, and other street-based outreach.
The campaign was launched in 2014 and an implementation evaluation tracked dissemination of materials across venues on a monthly basis with standardized forms. Funding for the campaign following its launch supported relatively limited dissemination in public spaces (i.e., bus shelter ads in the targeted neighborhoods, distribution of print materials to businesses and service providers such as shelters and soup kitchens), therefore the emphasis was placed on materials dissemination in conjunction with delivery of HIV/STI testing and educational services, where it could elicit conversations between health workers and women at high risk for HIV acquisition and address women’s immediate service needs. Results from a small outcome evaluation conducted in 2015 showed that a modest percentage of women surveyed in the targeted neighborhoods recognized the campaign and said it had positively influenced their behavior. These results are not surprising, given the scope of campaign dissemination and the amount of competing visual information New Yorkers encounter on the street, which can make distinct ads hard to recall.
Challenges to creating a campaign for a unique audience included the time it takes to conduct several stages of research to develop and test messages as well as to develop community partnerships that are meaningful and will follow the campaign into dissemination and coordinated educational and testing services. Additionally, there are many financial costs involved in creating such a campaign from research incentives to marketing design to staff time for a multidisciplinary team of specialists. We believe the investment captures the unique perspectives of communicating about HIV prevention with very high-risk women of color in NYC—a population often overlooked in social marketing.
Footnotes
Acknowledgment
We would like to thank Jamal Peterkin, Pamela Skinner, Sherrill Cohen, Veronica Momjian, Kim Sanders, and Marcella Tillett from Planned Parenthood of New York City; and Kathleen Scanlin and Nana Mensah from the New York City Department of Health and Mental Hygiene (NYC DOHMH) for their assistance and consultation on the project. The opinions expressed in this article do not necessarily reflect those of Planned Parenthood Federation of America, Inc. or the NYC DOHMH.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the New York City Department of Health and Mental Hygiene, Bureau of HIV/AIDS Prevention and Control.