
Abstract
The flu causes a significant number of largely vaccine-preventable hospitalizations and deaths each year. Previous studies show that efficacy beliefs about other flu prevention strategies may be barriers to flu vaccine uptake. The purpose of this study was to assess attitudes and behaviors regarding flu vaccination and other flu prevention strategies and to examine the decision to get a flu vaccine within a competitive context. Two independent surveys were administered in 2013 (general population, n = 1,158) and 2015 (millennial panel, n = 1,574) among adults in the United States, which generated propensity models to get flu vaccines. Compared to the vaccine, participants considered many strategies to be more effective at preventing seasonal flu, particularly behaviors related to maintaining a strong immune system. Propensity models demonstrate that perceived effectiveness of some alternative “healthy behaviors” in a competitive set were associated with a lower likelihood of vaccine uptake. Results suggest that adults’ engagement in alternative strategies may be at the expense of getting vaccinated. Social marketers should consider competition not just from unhealthy behaviors but from alternative healthy behaviors when designing programs and campaigns to ensure effectiveness of their messages.
Introduction
According to the Centers for Disease Control and Prevention (CDC), the annual estimates of deaths from complications stemming from seasonal flu in the United States range from 3,000 to 49,000 cases (M. G. Thompson et al., 2010) and on the average 200,000 individuals are hospitalized (W. W. Thompson et al., 2004) per year. Experts agree that the best way to prevent the flu is to get a flu vaccine each season, but most adults do not get vaccinated. For the 2014–2015 flu season, flu vaccine coverage among adults aged ≥18 years was 43.6%, diminishing to 39.3% among adults aged 18–49 years (Santibanez et al., 2016).
The explanation and prediction of vaccination behavior has historically relied on value expectancy models. For example, the Health Belief Model is often used to explain vaccine uptake, stressing the individual assessment of the susceptibility toward and severity of the flu itself as well as the potential benefits of the vaccine and the belief in the likelihood of adverse reactions to the vaccine (Chapman & Coups, 1999; Frank, Henderson, & McMurray, 1985; Poland, 2010; Setbon & Raudez, 2010). Explanations relying on Theory of Reasoned Action or Theory of Planned Behavior highlighted attitudes toward flu vaccination as well as social influence and social norms (Gargano et al., 2011; Myers, 2016).
However, literature suggests that flu vaccinations may be competing with other health behaviors that audiences think are sufficient substitutes for an annual flu vaccine. Even among healthcare workers, beliefs in the effectiveness of actions such as exercise and good nutrition, thought to boost well-being and the health of the immune system, were cited as reasons for not accepting a seasonal flu vaccination (Manuel, Henry, Hockin, & Naus, 2002; Steiner, Vermeulen, Mullahy, & Hayney, 2002). Beliefs in the effectiveness of “healthy living” and social isolation were also stated as reasons for not accepting influenza vaccination among the elderly (Telford & Rogers, 2003). These findings suggest that the decision to get a seasonal flu vaccine may occur in a competitive context where the decision-maker is faced with several choices of behaviors that are perceived to be equally effective in preventing the flu.
Background and Literature
Competition in Social Marketing is often defined in terms of the competition between recommended behaviors and non-recommended behavioral alternatives (Grier & Bryant, 2005). The competition to recommended health behaviors is thus typically conceptualized in terms of the “bad guys.” It is the lure of the couch or screen time that interferes with promotion of physical activity, the food industry’s near constant inundation of advertisements for unhealthy snacks that undermines efforts to promote healthy eating, or the tobacco industry’s promotion of products attractive to children that social marketers have trouble combating. In other words, competition is the barrier to individuals adopting the promoted behaviors posed by what is typically considered unhealthy practices (Hasting, 2003).
These reasons for flu vaccination refusal suggest a different conceptualization of competition, one which is more in line with how the competition is defined in the commercial sector. In the commercial sector, survival of the brand depends on the consumers choosing it over other brands in the same product category, where the product category is typically defined by brands that meet similar goals, needs, or desires. Understanding the consumer choice as it pertains to the competition between brands is of utmost practical and existential importance for businesses (Weitz, 1985). Brand competition is implicit in social marketing of products such as condoms, where social marketed brands compete with commercial brands for a share of consumer wallets. However, it has not often been addressed in the context of idea marketing and behavior change. Rather, the typical conceptualization of behavior change tends to look at behaviors in isolation, where the outcome of the intervention is either adopting the promoted behavior or continuing with existing risk behavior. However, if we factor in the competitive context, behavior change can theoretically be influenced by alternative behaviors considered by the individual. The outcome is not just the adoption or rejection of the promoted behavior but potentially the adoption of possible alternative behaviors among those considered by an individual. The key is that the individual perceives the alternative behaviors to be equally or more beneficial or less costly than the promoted behavior to achieve the health goal.
The competitive set of behaviors and/or associated products may be wide or narrow depending on the health problem and context. Considering that to some extent behaviors such as proper hygiene practices, good nutrition, and stress reduction are promoted by reputable sources as ways to prevent flu, along with several other approaches promoted by less credible sources (i.e., blogs, Internet forums, social media), the information context may inadvertently, and sometimes deliberately, create a diverse consideration set of strategies to prevent the flu. Therefore, the uptake of the flu vaccine can be conceptualized as a choice between the flu vaccine and the alternatives that are thought to meet the same health outcome of preventing influenza infection. The analyses presented in this study posit the following hypothesis: If the decision to get a flu vaccine occurs in a competitive context where the competitive set is comprised of behaviors the audience believes will lead to the same outcome as the flu vaccine, a decision to get a flu vaccine may be dependent on the audience’s assessment of the flu vaccination itself in relationship to possible alternative prevention strategies.
The analytical challenge in testing this hypothesis is that consumer ratings of individual products in a competitive set are poor predictors of the consumer choice. For instance, weighted sums of ratings across attributes of different brands do not accurately predict a choice between products in a competitive set (Bass & Talarzyk, 1972). Similarly, weighted sums of attitudes toward particular nutritional recommendations based on Fishbein and Ajzen’s (1975) Theory of Reasoned Action or Ajzen’s (1991) Theory of Planned Behavior were weak in predicting food choices when several options are presented (Brinberg, Axelson, & Price, 2000). Hofmeyr, Goodall, Bonger, and Holzman (2008) argued that direct measures of consumers’ disposition toward the brands in a competitive set (as opposed to summary scores based on brand attributes) were also not strong predictors of consumer choice.
The solution offered by Bass and Talarzyk (1972) was to first rank-order individuals’ weighted sums of ratings of brand attributes and use rank-order values as the predictor of consumer choice. We used a similar approach based on the work of Hofmeyr et al. (2008). Namely, raw ratings on effectiveness of flu vaccine and other prevention strategies were rank ordered for each respondent. Procedures for calculating the perceived effectiveness score and resolving ties in raw measures are described in the Method section. The resultant score thus captured the perceived effectiveness of each prevention strategy in relationship to the perceived effectiveness of all other strategies.
Method
Sample
In November 2015, an online survey was administered to a panel of respondents recruited from the EurekaFacts millennial panel. Of 5,000 respondents randomly selected from the panel, 1,574 participated in the survey. Eligibility criteria included being between the ages of 18 and 34 (i.e., definition of the millennial cohort). We further excluded respondents who were strongly opposed to all vaccinations or reported medical conditions that precluded them from getting a flu vaccine, resulting in 1,175 participants who were included for analysis.
The Ipsos Omnibus survey, referred to as the general population survey in this article, was administered to a general population sample in September 2013. The sample was recruited using a blended sample approach which combined samples from multiple online panels with web intercepts. The questionnaire was administered as part of an Ipsos Omnibus tracking survey. In all, 1,158 participants completed the survey and 853 were included for analysis. Exclusions were based on a participant’s opposition to vaccinations or medical conditions that prevented them from getting a flu vaccine.
Both surveys were administered online and were available in desktop and mobile platforms. Because of the procedures used to recruit the general population sample, response rate is not available. The cooperation rate for the millennial panel sample was 31%.
Instruments
The main constructs measured in both survey instruments were flu vaccine uptake, perceived effectiveness of flu vaccination and other flu prevention strategies, engagement in flu prevention strategies, perceived susceptibility toward contracting flu, perceived severity of flu, attitudes toward the vaccine itself, exposure to flu vaccine advertising and promotions, and perceived availability and cost of the vaccine. In addition to the measure of effectiveness of the flu vaccine, both surveys included a 5-point Likert-type scale question in which respondents were provided the stem “On the scale of 1 to 5, where 1 is very ineffective and 5 is very effective, how you would rate the following in terms of their effectiveness in preventing you getting the flu?” and a series of scenarios to evaluate, including washing hands, using hand sanitizer, maintaining a healthy diet, being physically fit, eating certain foods, taking vitamins or supplements, dressing warmly, and avoiding crowds. The millennial survey differed slightly from the general population survey in that it included the additional scenarios of “wiping off surfaces” and “avoiding touching surfaces in public places.” These items were added in light of advertising campaigns for surface disinfection products that specifically mentioned flu virus. Furthermore, the millennial survey included measures of effectiveness for “getting enough sleep” and “reducing stress,” which were based on recommendations commonly conveyed by more reputable medical advice sites like Mayo Clinic. Response options for measures of effectiveness, attitudes, and engagement in prevention behaviors were randomized to minimize order effects.
Items assessing vaccine uptake also differed slightly. The millennial survey asked respondents whether they had received a flu vaccine, either by shot or nasal mist, during the current season and the past three flu seasons. Those who had not received a flu vaccine were asked to rate their likelihood of getting a flu vaccine this fall or winter on a 4-point Likert-type scale, anchored by response options “definitely planning to get a flu vaccine” and “definitely not planning to get a flu vaccine.” The general population survey assessed vaccine uptake and intention in a single item, presenting the following options: “Already got a flu vaccine this season,” “I plan to get a flu vaccine this season,” “I may or may not get a flu vaccine this season,” “I probably will not get a flu vaccine this season,” and “I definitely will not get a flu vaccine this season.”
Survey instruments also assessed demographic characteristics including gender, race/ethnicity, household income, and education. All respondents were also asked about their motivation to live a healthy lifestyle and health-seeking behaviors, as indicated by searching for information online, contributing to a health discussion on social media, reading about health or fitness in a book, and similar behaviors. Whereas the models described below included demographic variables, we did not include health lifestyle and health-seeking measures in the analyses as they are subject for further research.
Criterion Variable
The definition of the flu vaccination status differed between the two samples. For the millennial survey, vaccine uptake and intention to vaccinate (response of definitely planning to get a flu vaccine) were combined to indicate positive vaccination status. For the general population sample, agreement with the statements, already got a flu vaccine this season or I plan to get a flu vaccine this season, indicated positive vaccination status. For both samples, vaccination status was significantly related to whether participants got a flu vaccine during the previous flu season.
Calculation of Perceived Effectiveness Scores
Respondents were asked to rate a set of strategies in terms of their effectiveness in preventing them from contracting the flu. First, raw effectiveness scores were rank ordered. In the case of a tie (e.g., same raw effectiveness score for two or more measures), an average ranking of the effectiveness of each behavior was computed. For example, a score of 4 put three behaviors in the second ordinal position in relationship to all other behaviors (i.e., those three behaviors were rated as the second most effective). In this case, the ordinal positions of 2, 3, and 4 are first assigned to each behavior and each behavior’s rank score is computed by taking the average of the ordinal positions (i.e., 3). Then, the Zipf transformation is applied to each individual ranking. The formula for Zipf transformation is presented below, where s is an empirically derived constant of 2.2 and m is the number of alternative behaviors for which ratings were given (Hofmeyr, Goodall, Bonger, & Holzman, 2008).
Findings
Respondent Demographics
Full demographics for the two samples can be seen in Table 1. The millennial sample was 76% female and 24% male. It was predominantly “White only” at 71.8%, followed by “Others” at 14%, and “Black only” and “Hispanic” both reporting at 7.1%. A majority of the sample was between the ages of 18 and 24 at 65.9%, with 34.1% being between 25 and 34 years old. The millennial sample was highly educated, with 61.4% having a college degree or more, 34.6% having had some college, and 4.1% having not gone to college. The incomes reported were spread across the spectrum, with the majority earning between $US25,000 and just below $US52,000 at 34.1%, followed by under $US25,000 at 27.2% and between $US52,000 and just below $US75,000 at 16.6%. Overall, in comparison to U.S. demographic characteristics of the millennial population, the sample overrepresented women and individuals with college degrees and underrepresented Hispanic and Black populations.
Demographics of Samples (Unweighted).
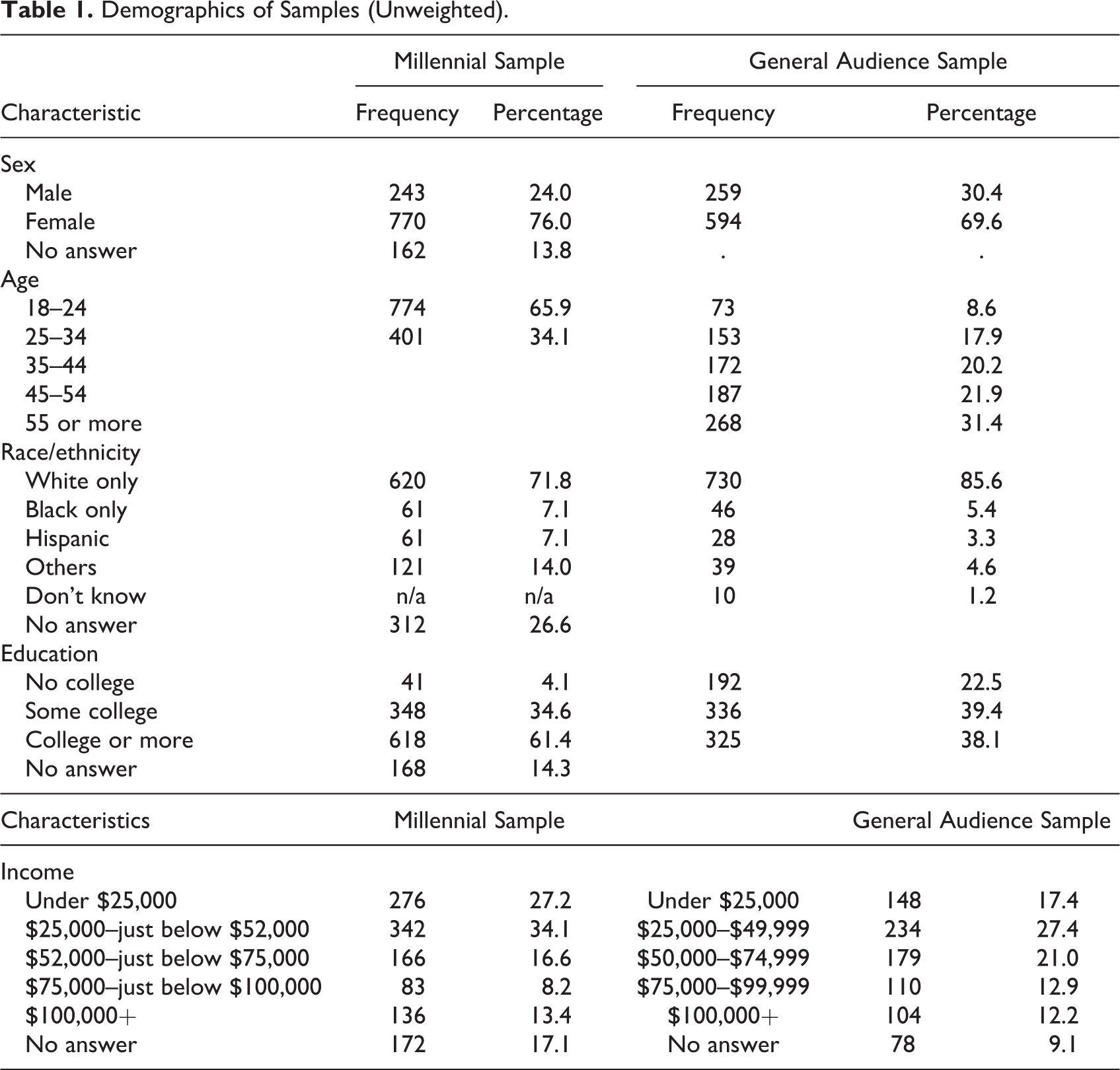
The general population sample had 69.6% women and 30.4% men. It was also predominantly White only at 85.6%, followed by Black only at 5.4% and Others at 4.6%. The majority of this sample was aged 55 and up at 31.4%, followed by 45 through 54 at 21.9% and 35–44 years at 20.2%. There was an even mixture of levels of education for this sample, with 22.5% having had no college, 39.4% some college, and 38.1% college or more. Most of the people in this sample earned between $US25,000 and $US49,999 at 27.4%, followed by $US50,000 and $US74,999 at 21.0% and under $US25,000 at 17.4%. Overall, in comparison to the demographic characteristics of the U.S. population, the sample overrepresented women and individuals with college degrees and those with higher incomes. The sample underrepresented younger cohorts, Hispanic, and Black populations.
Both data sets were weighted to reflect U.S. population proportions. The general sample was weighted using estimates from the 2013 Current Population Survey on age, gender, U.S. census region, race/ethnicity, and income. The millennial sample was weighted using estimates from 2015 American Community Survey on gender, age stratum (18–24/25–34), and race/ethnicity.
Models of Propensity to Get a Flu Vaccine
For each sample, we fit a binary logistic regression of the likelihood to get a flu vaccine using a forward selection of predictors with a likelihood ratio test. This selection method starts with an intercept-only model and at each step adds the predictor with the largest score statistic whose significance value is less than 5%. The likelihood ratio test compares the fit of two successive models to assess whether the new model fits the data better than the previous one. The final model retained is the one that fits the data the best with the optimal number of predictors. The model was thus used to ascertain the influence of the following attributes on propensity to get a flu vaccine: perceived effectiveness of flu prevention behaviors, perceived safety of the flu vaccine, perceived severity of the flu, and the belief that a strong immune system protects one from contracting the flu. Demographic variables (age, gender, and race/ethnicity) as well as perceived availability and cost of the vaccine were included in the set of variables. As noted in the Method section, the model for the millennial survey sample included additional measures for perceived effectiveness of wiping surfaces, avoiding touching surfaces in public places, getting enough sleep and reducing stress, which were included in the predictor set. Analyses were conducted using IBM SPSS Statistics Version 21.
The models for the millennial survey sample demonstrate that perceived effectiveness of eating healthy foods to prevent catching the flu, and a belief that vaccines are not safe had a negative effect on the propensity to get a flu vaccine (see Table 2). The participants, on average, believed that eating a well-balanced diet was effective in preventing the flu (M = 3.92, standard deviation, not shown in table [SD] = 1.00) and showed moderately low levels of support on flu vaccines not being safe (M = 1.97, SD = 0.90). On the other hand, a belief in the effectiveness of the flu vaccine and concern about contracting the flu had a positive effect on the propensity to get a flu vaccine. The participants displayed a high level of support for the effectiveness of the flu vaccine (M = 3.83, SD = 1.10) and were undecided on whether to be concerned about contracting the flu (M = 2.81, SD = 1.18). The findings show that for each 1-point increase in the vaccine effectiveness score, participants were slightly over 9 times more likely to obtain a flu vaccine. Yet, for each 1-point increase in the belief in effectiveness of eating a well-balanced diet, participants were 22 times less likely to get a flu vaccine. Interestingly, greater perceived likelihood of contracting the flu had a negative effect on the propensity to get a flu vaccine. This might have been due to a statistical artifact or interpretation of the questions by some participants that strategies they have employed to prevent the flu have reduced their chances of catching the virus.
Summary of Logistic Model for the Millennial Survey Sample.
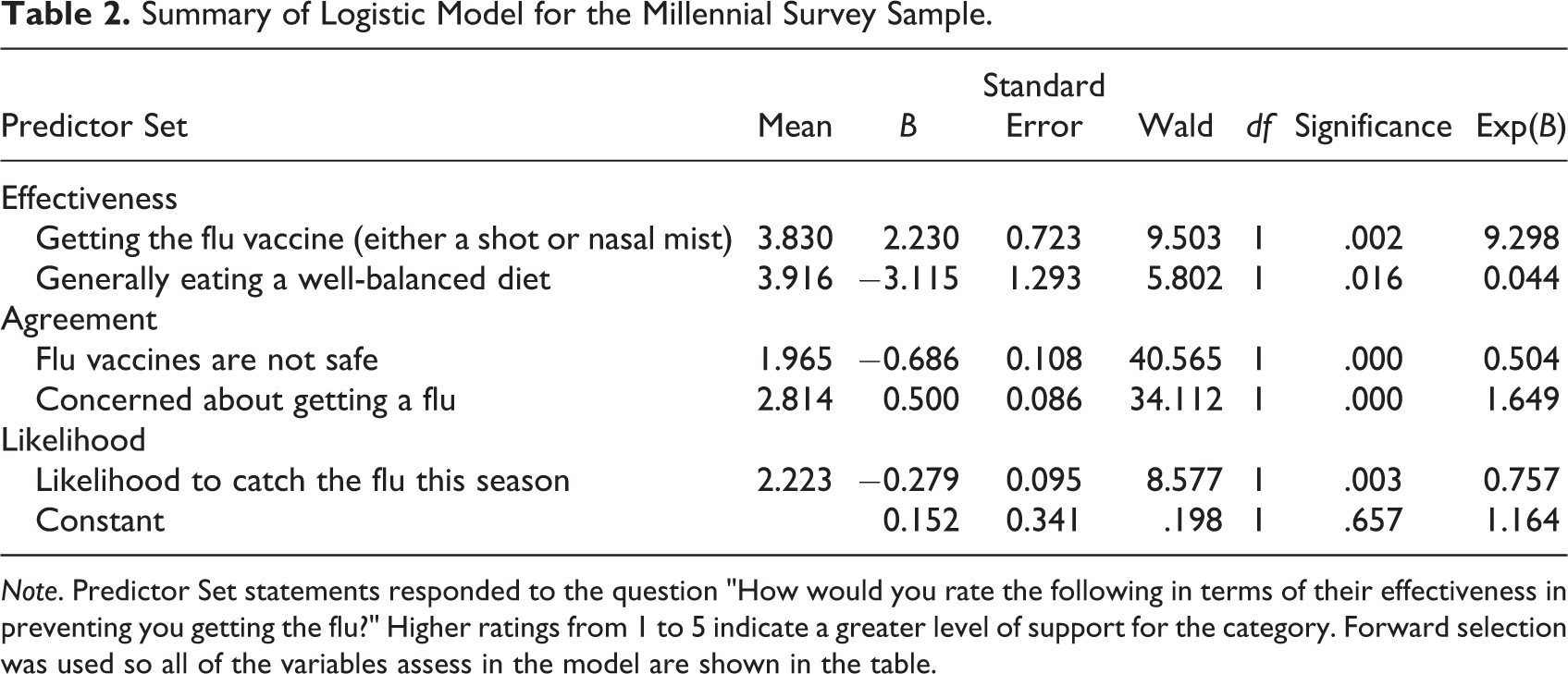
Note. Predictor Set statements responded to the question "How would you rate the following in terms of their effectiveness in preventing you getting the flu?" Higher ratings from 1 to 5 indicate a greater level of support for the category. Forward selection was used so all of the variables assess in the model are shown in the table.
Overall, the model was 71.9% accurate in predicting vaccination status. The model was better at predicting cases who did not get a flu vaccine (84.0%) compared to those who did get a flu vaccine (54.3%).
Among the general population sample, perceived effectiveness of the flu vaccine and overall concern about getting the flu were positively related to propensity to get a flu vaccine (see Table 3). Despite these variables being significantly related to flu vaccination, participants showed, on average, a moderately low level of support regarding the effectiveness of flu vaccines (M = 2.32, SD = 1.41) and were undecided on whether to be concerned about contracting the flu (M = 2.99, SD = 1.11). Belief in a strong immune system, belief that vaccines are not safe and belief that one is unlikely to contract the flu were negatively related to propensity to get a flu vaccine. Note that the item concerning likelihood to contract the flu was worded in the opposite direction, meaning that those who did not believe they were susceptible to getting the flu were less likely to get a flu vaccine. Overall, participants displayed moderately low levels of support on whether having a strong immune system is enough to protect you from the flu (M = 2.43, SD = 1.23). Additionally, the sample was undecided on whether they were unlikely to catch the flu this season (M = 2.90, SD = 1.16) and showed moderately high levels of support for the flu vaccines not being safe (M = 3.89, SD = .94). These findings are opposite of what was found from the millennial survey sample.
Summary of Logistic Model for General Population Sample.
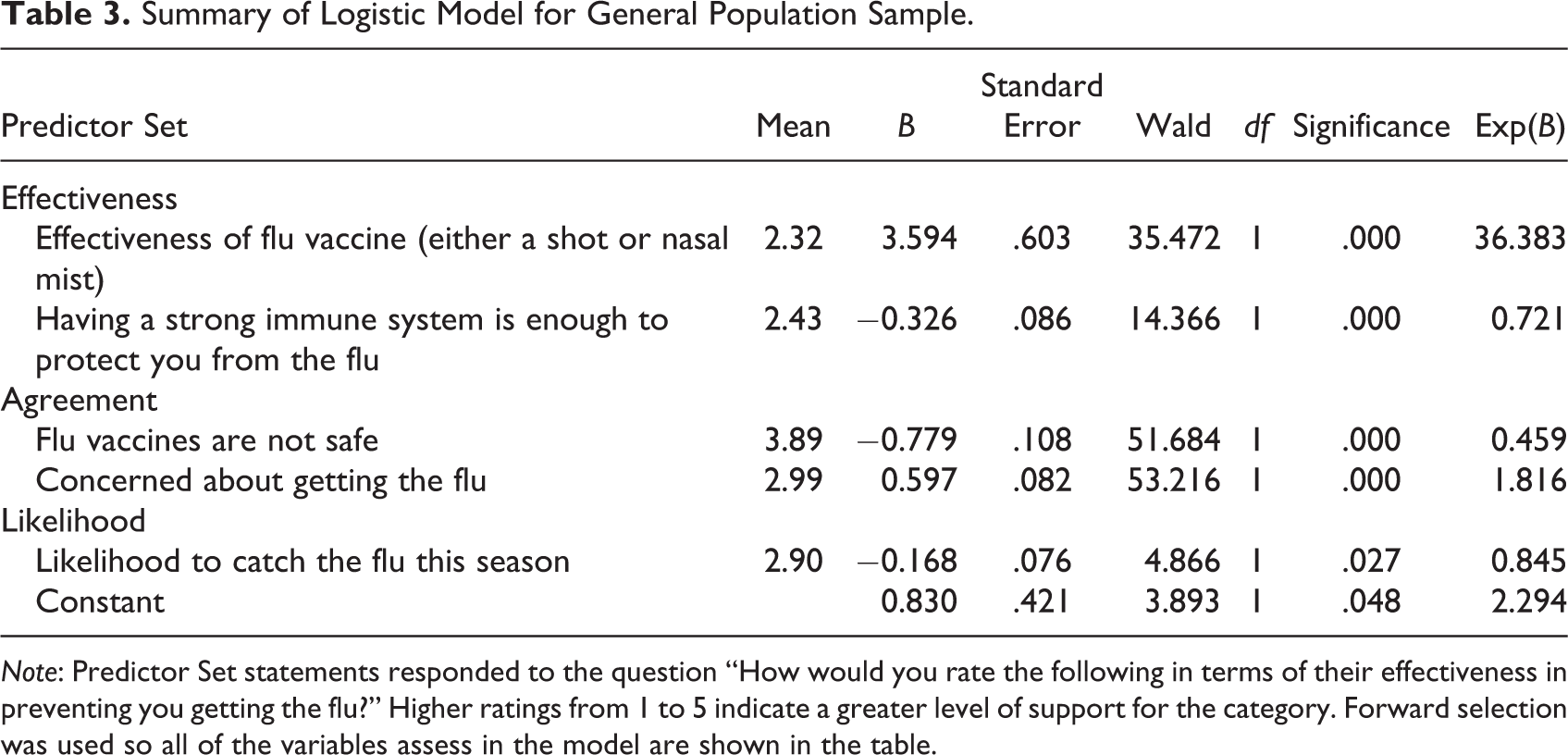
Note: Predictor Set statements responded to the question “How would you rate the following in terms of their effectiveness in preventing you getting the flu?” Higher ratings from 1 to 5 indicate a greater level of support for the category. Forward selection was used so all of the variables assess in the model are shown in the table.
Overall, the model was 73.5% accurate in predicting vaccination status, with similar accuracy in predicting those who got or intended to get a flu vaccine (72.6%) versus those who did not get a flu vaccine or did not intend to (74.4%).
Follow-Up Analyses
Both the previous literature and the model for the general population sample indicate that the belief in a strong immune system as protection against the flu may be a barrier to getting a flu vaccine. Thus, we conducted follow-up analyses to examine the relationship between the belief in a strong immune system and perceived effectiveness of different flu prevention strategies. Table 4 presents a summary of Pearson correlations between the belief in a strong immune system as a protective factor and the perceived effectiveness of each potential preventive strategy. For both samples, the belief in a strong immune system was negatively related to perceived effectiveness of flu vaccination. Although the magnitude of the relationships was relatively weak, in both samples, the belief in a strong immune system was significantly and positively related to behaviors that support a healthy immune system, such as eating well and being physically active. In addition, for both samples, the belief in a strong immune system was significantly and positively related to perceived effectiveness of dressing warmly and eating certain foods as a means of flu prevention. Among respondents in the millennial survey, the same belief was related to other behaviors promoted as strategies for a “healthy” immune system, namely, getting enough sleep and keeping stress levels low. The hygiene and avoidance strategies (i.e., washing hands and avoiding crowds) were either significantly negatively related to the belief that a strong immune system prevents flu or had no relationship with the construct.
Relationship Between the Belief in a Strong Immune System to Prevent Flu and Perceived Effectiveness of Flu Prevention Strategies.
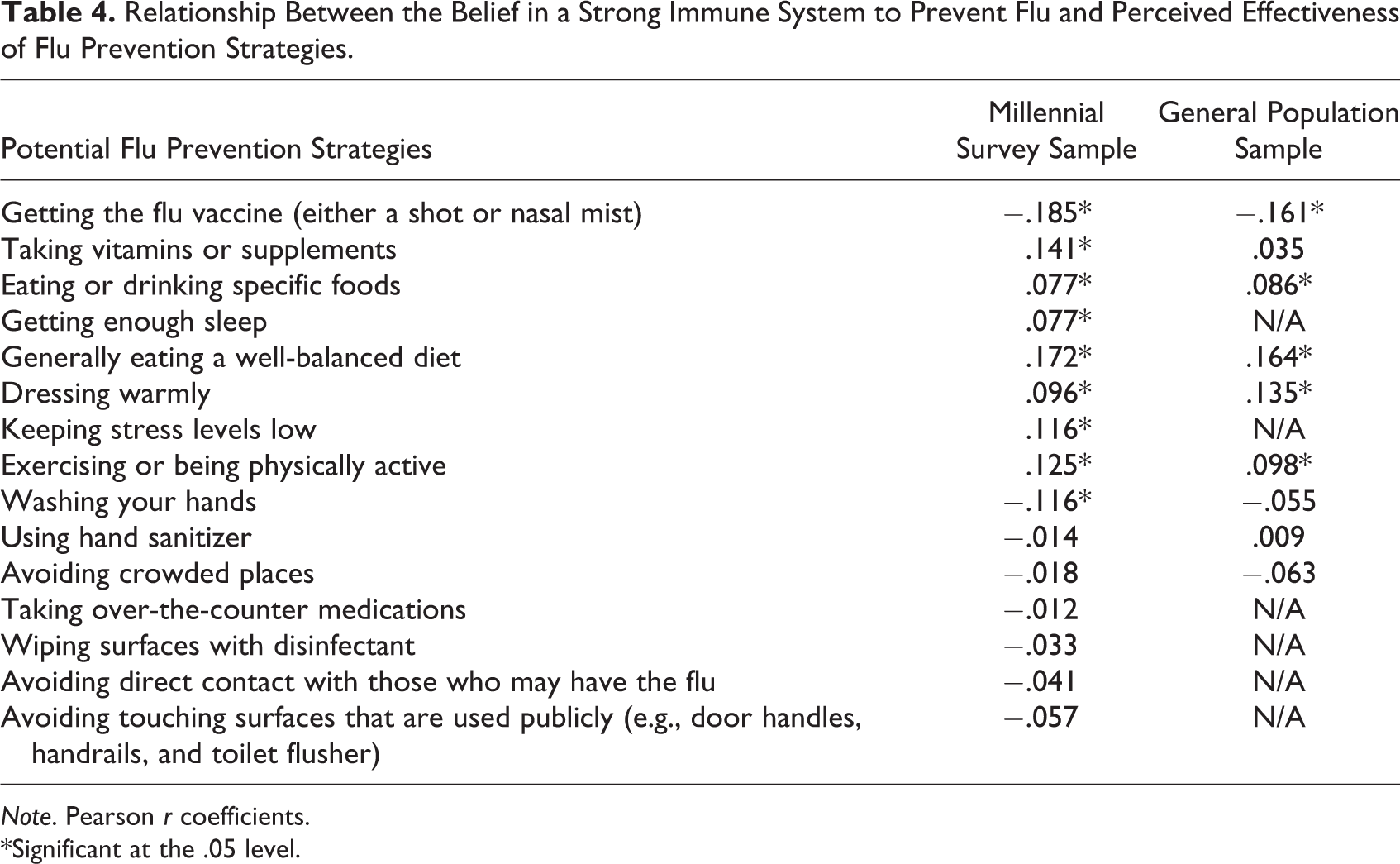
Note. Pearson r coefficients.
*Significant at the .05 level.
Previous Behaviors
A set of logistic regressions looking at the association between the belief that immune system protects one from the flu (i.e., “agree” and “strongly agree” indicated strong belief vs. other response categories) and self-reported engagement in preventive behaviors showed that millennials who held a strong belief in immune system protection were more likely to eat a well-balanced diet (β = .435, standard error [SE] = .159, odds ratio [OR] = 1.545, p<-.006) and dress warmly (β = .507, SE = .161, OR = 1.66, p = .002) as strategies to prevent getting the flu.
Analyses of the general population sample revealed findings consistent with the millennial survey. Participants who held a strong belief that the immune system protects one from contracting the flu were more likely to report eating a well-balanced diet (β = .552, SE = .164, OR = 1.73, p = .001), eating specific foods or beverages (β = .453, SE = .202, OR = 1.57, p = .025), staying fit (β = .867, SE = .172, OR = 2.34, p < .0001), and dressing warmly (β = .359, SE = .167, OR = 1.43, p = .028). In contrast, they were less likely to report avoiding crowds (β = −.534, SE = .177, OR = 0.586, p = .002) to prevent contracting flu.
Discussion
The results of this study support the hypothesis that the perceived effectiveness of alternative behaviors in a competitive set can negatively influence uptake of the promoted behavior. For the millennial survey sample, when participants held strong beliefs that healthy eating is an effective strategy to prevent flu infection, they were less likely to get a flu vaccine. The negative influence of the belief in the effectiveness of healthy eating as a flu prevention strategy was evident in the model that accounted for the influence of the attitudes toward safety of the vaccine, perceived susceptibility, and perceived severity of the flu virus.
For the general population sample, the belief that a strong immune system protects one from the flu was negatively related to the propensity to get a flu vaccine. Results of the follow-up analyses showed that the belief in the effectiveness of certain behaviors such as eating well, staying fit, eating certain foods, and dressing warmly were significantly related to this belief. On the other hand, hygiene-related practices (i.e., washing hands or using hand sanitizer) were not related or demonstrated a negative relationship with the belief that a strong immune system protects one from contracting the flu. This pattern of results is similar to previous analyses of the millennial survey data that showed the belief in the effectiveness of immune boosting strategies such as eating well, exercising, reducing stress, and so on, loaded on a common factor (Ulasevich, Jacobs, van Over, & Mbangdadji, 2016a). Hence, the belief that a strong immune system protects one from the flu is related to the belief in the effectiveness of what we can consider to be “immune boosting strategies.” Furthermore, those who held a strong belief in the effectiveness of the immune system as a protective factor were more likely to report engaging in these immune boosting strategies during the previous flu season and were less likely to report getting a flu vaccine. These findings are consistent with our previous findings reported for the millennial survey sample (Ulasevich, Jacobs, van Over, & Mbangdadji, 2016b).
Given the relationships between the belief that a strong immune system can prevent the flu, and the perceived effectiveness of and engagement in what can be considered immune boosting strategies, the findings from the general population sample appear to cross-validate the findings from the millennial survey sample. It is likely that differences in methodology (e.g., different number of competitive measures and wording of some survey items) and the timing of survey administration influenced the results. However, the apparent consistency in results across the difference between the samples are informative. Recent marketing research demonstrates that millennials are more likely to endorse healthy eating as an overall health benefit and are willing to pay a premium for healthier foods (“Younger Consumers Endorse Health,” 2015). Eating healthy is a strong cultural norm that is conveyed as a moral imperative that one “ought to” strive for, although practicing this behavior consistently is a challenge for many adults. It is therefore likely that healthier eating is the more salient immune boosting strategy to millennials. On the other hand, the general population sample that included a wider range of ages may be more varied in terms of which immune boosting behaviors are effective or may in fact rely on several strategies to prevent flu infection in lieu of a vaccine. The belief in a strong immune system might have subsumed the variance associated with individual immune boosting strategies.
The findings presented here are thus consistent with literature that demonstrates that immune boosting strategies are potential competitors to flu vaccination (Manuel et al., 2002; Steiner et al., 2002). However, our approach modeled the relationship between alternative strategies and the propensity to get a flu vaccine rather than inquiring about reasons why nonvaccinators refused the flu vaccine. All of these findings potentially reflect the current Zeitgeist described by Greenhalgh and Wessely (2004) in which the lay understanding of vulnerability to disease has been internalized and attributed to the functioning of the immune system. Although, clinically, vaccinations work through inciting an immune response to specific pathogens, our analyses suggest that audiences do not see flu vaccine in terms of “immune boosting” strategies and, in fact, behaviors thought to strengthen the immune system are seen as antithetical to vaccination.
Implications for Social Marketing
These findings thus present a social marketing conundrum: how should public health professionals promote flu vaccination, when the audience has a clear preference for other behaviors over the flu vaccine, which in fact have some merit? Results of this study suggest that a solution to this specific problem may lie in both acknowledging that a substantial audience segment believes in the effectiveness of the behaviors thought to “boost” the immune system, while framing flu vaccination in terms of its positive effect on the immune system. The messaging strategy should emphasize the unique features of the flu vaccine, namely, that vaccination leads to a very specific immunological response that prevents influenza. The relative advantage of the specificity of the immune response produced by the flu vaccine can be contrasted with the more general positive effect of behaviors such healthy eating, physical activity, and getting enough sleep on immune health. In other words, audiences need to be convinced that by design, vaccination is the ultimate “immune boost,” and even a healthy immune system can use help targeting a pathogen as specific as the flu virus.
The cobranding approach suggested here has the potential of overcoming what can be considered a deficiency of current public health approaches, which tend to list several recommended behaviors that may be tangentially related to disease prevention or health promotion. For example, the flu virus is primarily contracted through the air, but strategies such as washing hands and using hand sanitizer are not entirely irrelevant, as transmission may occur if droplets are absorbed into the respiratory tract after touching infected surfaces. Not to mention, hygiene practices are particularly salient with the audience, as they are recommended to prevent the spread of many illnesses. Although the effectiveness of the flu vaccine is often emphasized as the empirically “best” option, as we noted in the Introduction section, the presentation of the list itself may inadvertently create a consideration set of possible strategies to prevent one from contracting the flu. Our findings show that endorsement of some behaviors on the list may in fact lead to lower flu vaccination uptake. The suggested cobranding approach can potentially tie flu vaccination to other recommended behaviors, creating a coherent strategy for influenza prevention that intrinsically includes flu vaccination.
The success of the suggested cobranding approach will depend on the extent to which communication strategies addresses the demonstrated distinction between immune boosting strategies and the flu vaccine. We can suspect that among some segments, the distinction between immune boosting strategies and flu vaccine lies along the “natural” versus “artificial” dimension. Hence, if this is the case, the emphasis that vaccines produce a natural body response to pathogens may be necessary. We also do not know how the audiences’ mental models work with regard to how the natural immune boosting strategies prevent disease. In regard to vaccines, some segments may think that ingredients in vaccines directly attack the pathogen (Jee, Uttal, Spiegel, & Diamond, 2013); hence, vaccines are perceived more as antiviral medications than stimulators of the immune response. These are topics for further investigation, which are necessary to refine communication approach.
Additionally, the communication strategy should address the safety of the vaccine. We should note that although the perceived safety of the influenza vaccine was a significant factor in predicting flu vaccination for both samples, the mean score for vaccine safety was below the midpoint, thus suggesting that most respondents saw vaccines as relatively safe. Increasing beliefs in susceptibility to flu or the overall concern about flu infection can be potentially effective messages in terms of increasing motivation to protect oneself from flu. However, our analyses suggest that these messages should be implemented in the context of the proposed cobranding approach, since it is possible that an increase in perceived susceptibility or severity would simply lead some members of the audience to turn to the alternative strategies to prevent the flu, such as eating healthy.
Whereas some behaviors related to the belief that a strong immune system will prevent one from catching the flu (e.g., eating healthy, exercise, and getting enough sleep) are often promoted by reputable sources along with flu vaccination, our findings also show that strategies of more dubious effectiveness are also part of the consideration set. For example, participants who held the belief in a strong immune system were also more likely to think that eating certain foods and dressing warmly were effective for flu prevention and were more likely to report engaging in these behaviors. A simple Internet search for flu prevention yields advice to ranging from loading up on zinc tablets to massage therapy as a means to get rid of bad energy. For some audience segments, a countermarketing campaign against ineffective strategies to prevent influenza infection may be warranted, especially where knowledge is low.
Implications of Findings to Other Public Health Issues
Findings presented in this article focused specifically on the perception of competitive behaviors as they relate to flu vaccination, yet the idea that a preference for alternative behaviors, including other valid healthy behaviors, may in fact be barriers to promoted behaviors. We know, for instance, that risk reduction strategies such as strategic sexual positioning based on HIV status has been used by men who have sex with men as alternatives to condom use to prevent HIV infection (Van de Ven et al., 2005). Similarly, due to the widespread awareness of and commercial availability of Truvada®, pre-exposure prophylaxis (PrEP) is already a preferred alternative to condom use among certain populations (Mansergh et al., 2010). While these strategies are indeed valid for reducing risk of HIV transmission, condom use is still promoted as the gold standard for comprehensive disease prevention. On the topic of nutrition and physical activity, qualitative findings show that children clearly prefer physical activity and think that physical activity counteracts the negative effects of bad nutrition (Hesketh, Waters, Salmon, & Williams, 2005; Zawislanki & Ulasevich, 2003). These findings that children may prefer physical activity over healthy nutrition practices provide a plausible explanation of the results that showed that the programs promoting both nutrition and physical activity among school-age children succeeded only in increasing physical activity but not nutrition (Shilts, Townsend, & Horowitz, 2002). On the other hand, analyses of quantitative data suggest that adults seem to prefer dieting to physical activity as a means of maintaining or losing weight (Mokdad et al., 2001), suggesting that “picking and choosing” among compatible behaviors is common. Therefore, competition among healthy behaviors may factor in other domains other than flu behavior and may need to be addressed by social marketers. For example, presenting several behavioral recommendations to achieve a particular health outcome may in fact inadvertently create a competitive set, leading the audience to choose one recommendation over another. A solution suggested here is that cobranding recommendations as a coherent approach to achieve a health outcome may diminish the perceived competition among them, thus increasing compliance with all recommendations.
Limitations and Strengths
Findings for the millennial survey sample are based on opt-in panel, whereas findings for the general population sample are based on a more robust online sampling methodology that included multiple panels and web intercepts. Therefore, generalization to the population should be made cautiously. Besides the sampling methodology, the instruments varied both in content and in wording of some survey items. However, the two studies found relatively consistent results in terms of influences of the belief in a strong immune system and associated behaviors leading to lower uptake of the flu vaccine. In other words, regardless of sample differences and specific wording of the survey items, the two analyses found a convergence of results.
Conclusion
The broader theoretical implication of our findings is that knowing what audiences think and feel about behaviors that they consider as alternatives to one promoted behavior may be as important as knowing what they think and feel about the behavior being promoted. We need to ask not just why our audience adopt or fail to adopt the behaviors we promote but also ask what the audiences possibly do instead. Behavior change is probably best conceptualized in terms of a decision model in which the audience potentially considers several alternatives to reach the health outcomes goals. In case of the flu vaccination, the alternative strategies for influenza prevention include health behaviors promoted by trusted sources. Social marketing strategies may thus need to leverage healthy practices already endorsed by the audiences and position flu vaccination as an integral part of individual flu prevention.
We should note that the present analyses focused narrowly on the competition hypothesis. There is still much to be learned. At the very least, future research should explore the segmentation of the audiences in terms of the factors that may influence greater acceptance of alternative strategies of flu prevention. In fact, factors such as health information seeking may be an important segmentation variable. Since one of our samples was, by definition that of younger people, the present study did not have statistical power to explore the phenomenon of competition among medically vulnerable populations. Future research may wish to examine the specific vaccination and alternate behavioral mental models of these populations to further success in social marketing efforts.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.