
Abstract
Sexual violence (SV) represents a serious public health problem with high rates and numerous health consequences. Current primary prevention strategies to reduce SV perpetration have been shown to be largely ineffective—not surprisingly, since as others have pointed out current prevention largely fails to draw on existing knowledge about the characteristics of effective prevention. In this article, we examine the potential of K–12 comprehensive sexuality education (CSE), guided by the National Sexuality Education Standards (NSES), to be an effective strategy. Our discussion uses socioecological and feminist theories as a guide, examines the extent to which NSES-guided CSE could both meet the qualities of effective prevention programs and mitigate the risk factors that are most implicated in perpetration behavior, and considers the potential limitations of this approach. We suggest that sequential, K–12 program has potential to prevent the emergence of risk factors associated with SV perpetration by starting prevention early on in the life course. CSE has not yet been evaluated with SV perpetration behavior as an outcome, and this article synthesizes what is known about drivers of SV perpetration and the potential impacts of CSE to argue for the importance of future research in this area. The primary recommendation is for longitudinal research to examine the impact of CSE on SV perpetration as well as on other sexual and reproductive health outcomes.
There is growing awareness in the United States about the nation’s high rates of sexual violence (SV). SV is defined by the Centers for Disease Control and Prevention as a sexual act committed against someone without that person’s freely given consent—including completed forced penetration (rape), attempted forced penetration, coerced penetration, unwanted sexual contact, and noncontact sexual experiences such as harassment. A 2010–2012 nationally representative survey of adults found that approximately one in three (36.3%) women and one in six (17.1%) men reported experiencing some form of SV during their lifetime, with 19.1% of women and 1.5% of men experiencing completed or attempted rape and 13.2% of women and 5.8% of men experiencing sexual coercion at some time in their lives. Among women who have been raped, 41.3% first experienced that rape before the age of 18 and an additional 36.5% were first raped between ages 18 and 24 (Smith et al., 2017). There is strong evidence that SV affects individuals throughout the life course (Basile, Smith, Breiding, Black, & Mahendra, 2014).
These alarming statistics underline the dire need to implement, evaluate, and scale up primary prevention—that is, effective programming to prevent SV before it happens. In a public health framework, primary prevention entails “looking upstream” at the underlying risk factors and mitigating those risk factors before they come to fruition and result in violent behavior (Harvey, Garcia-Moreno, & Butchart, 2007). The Centers for Disease Control and Prevention has recommended that research and programs to prevent SV be grounded in the socioecological approach to prevention (Basile et al., 2016), which addresses risk factors at the individual, interpersonal, community, and social-structural levels across the life course that may lead someone to perpetrate SV. This ecological approach conceptualizes violence as an interplay among these multiple levels of influence (Casey & Lindhorst, 2009; Heise, 1998; Krug, Mercy, Dahlberg, Zwi, & Lozano, 2002).
Drawing on that ecological life-course perspective, this article examines one promising strategy for the primary prevention of SV perpetration that would operate by modifying the known risk factors associated with perpetration. A primary prevention of perpetration approach, instead of a focus on the risk factors that make someone likely to be victimized, places the onus for SV prevention on perpetrators. While victimization prevention approaches should be part of a larger SV prevention strategy, the historical emphasis on preventing victimization neglects the role of the perpetrator in violence; this can fuel victim-blaming narratives, self-blame, and a focus on whether victims could have done something differently to prevent an attack (DeGue et al., 2012). Furthermore, a prevention focus on those at risk of being assaulted does not necessarily reduce attempts to perpetrate SV nor does it address the social norms that lie on the outer level of the ecological model that allows SV to continue. In order to achieve measurable reductions in violence, perpetration needs to be the focal point of intervention (DeGue et al., 2012).
There are few programs with demonstrated effectiveness at mitigating perpetration behavior (DeGue et al., 2014). A 2014 review found only three programs shown by rigorous, controlled evaluation to prevent perpetration behavior (DeGue et al., 2014). Furthermore, it found that the vast majority of programs target college-level students but that none of the effective programs were in this age-group. Instead, program effectiveness was found earlier on in the life course, during adolescence (DeGue et al., 2014). Given the substantial limitations of the literature on effective perpetration prevention, the current article draws on Banyard’s (2013) commentary encouraging sexual violence researchers to “locate and use opportunities for bridging across areas of prevention…and across the life span (e.g., finding ways to connect skill building in childhood and adolescence with prevention education in early adulthood)” (p. 115).
The specific step this article takes to advance SV prevention is to examine the potential for K–12 comprehensive sexuality education (CSE), guided by the National Sexuality Education Standards (NSES)—and henceforth referred to as NSES-CSE—to effectively prevent perpetration behavior. Currently, most school-based SV programs are independent from any CSE program, and many CSE programs fall short of their potential to comprehensively address SV perpetration. An NSES-CSE program can effectively merge the two and address SV while simultaneously fulfilling its more traditional goals of preventing unplanned teen pregnancy, HIV/sexually transmitted infections (STIs) acquisition, and other adverse health outcomes. There are several reasons for this, all of which are discussed at greater length below, but in brief: (1) research across multiple areas of behavioral prevention highlights a number of criteria for effectiveness, all of which can be met by high-quality NSES-CSE; (2) a number of well-documented risk factors for SV perpetration are addressed in a NSES-CSE curriculum; (3) these risk factors have individually been shown to be amenable via small group or educational interventions, and sex education creates an opportunity to comprehensively address many of them in one intervention; and (4) a sequential, K–12 program begins early on in the life course when many risk factors are only just beginning to develop, and by reaching young children while they are still in development, it presents the best opportunity to address the problem before it occurs. The field of SV prevention is in desperate need of population-level solutions. The interventions currently being implemented in the field primarily target an age-group in which intervention is past the point of being “primary” prevention. NSES-CSE may present one promising strategy to address this critical public health issue. Figure 1 visually depicts the mechanism through which NSES-CSE could be effective.
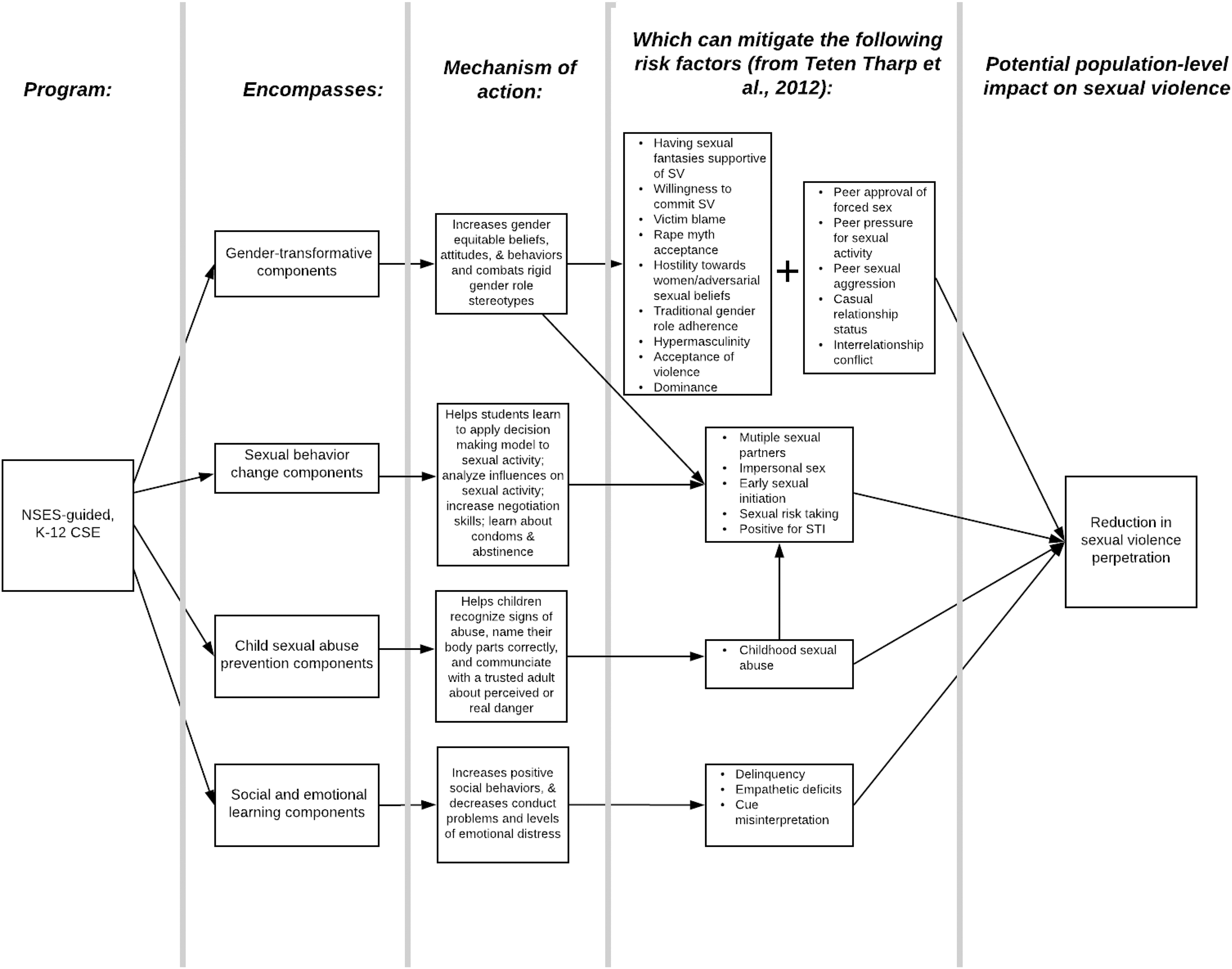
Conceptual model of pathways through which comprehensive sexuality education based on National Sexuality Education Standards could prevent sexual violence perpetration.
Method
Because, as noted above, there is so little in the way of published literature on effective primary prevention for SV, we did not take a systematic literature review approach. Rather, cued by Banyard (2013) to mine other areas in which successful and relevant prevention programs have been developed, our literature search, conducted on EBSCOHost using all databases, sought relevant literature for each section in this article. We first searched for current SV primary prevention literature to understand the current state of the field. We then searched for an existing systematic review of risk factors for SV perpetration. We clustered the risk factors found in this review into themes (see Figure 1) and conducted a search for all clusters to find existing reviews of each.
Because this article is not intended to be a systematic review, not every article yielded in the search is included. This article synthesizes evidence from review articles in several different areas to examine the potential of CSE as an effective population-level strategy for the prevention of SV perpetration. Search terms used for these different research areas are displayed in Table 1.
Search Terms and Key Articles Used.
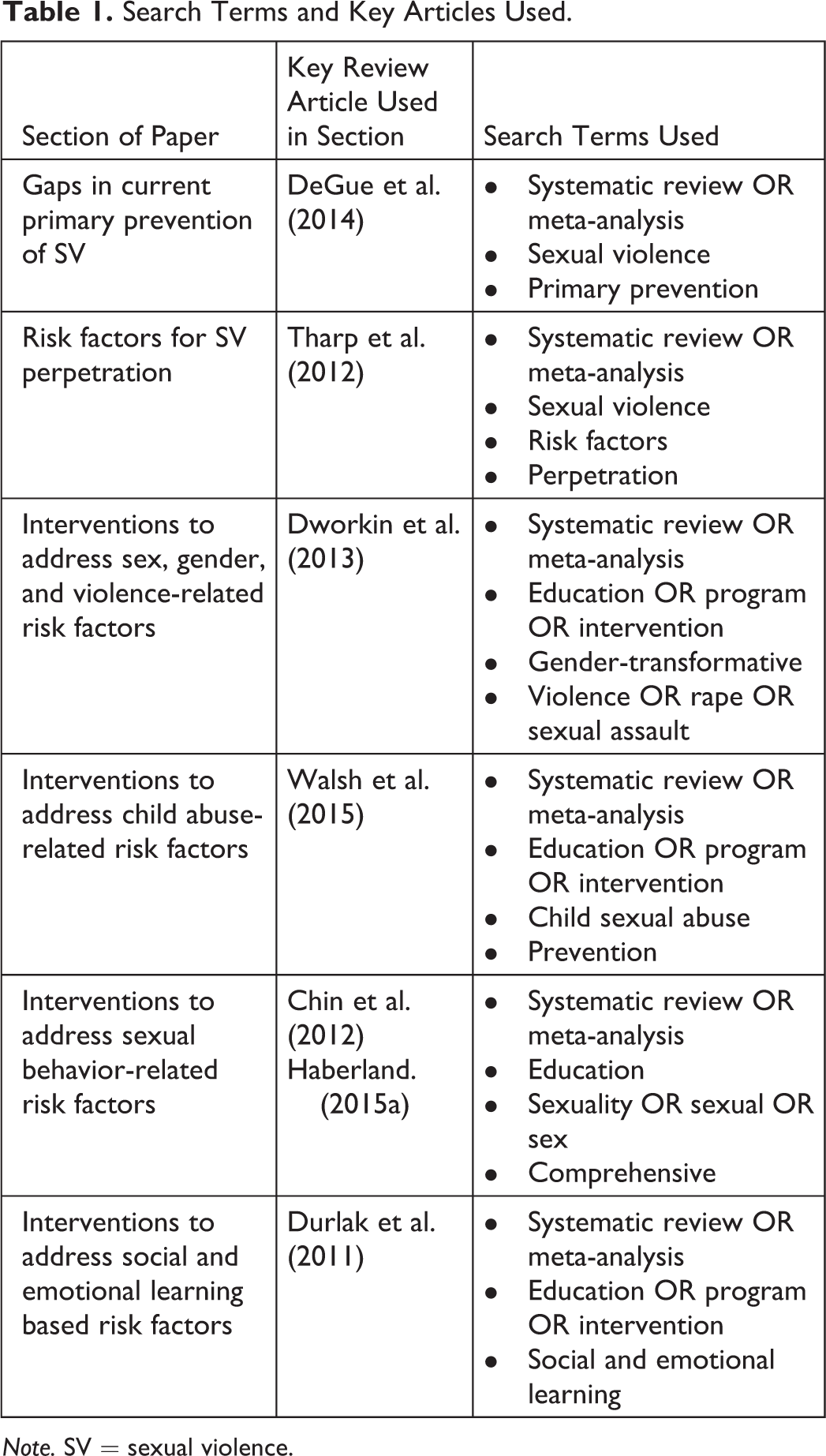
Note. SV = sexual violence.
SV as a Public Health Problem
Preventing SV is an important public health priority for a multitude of reasons. In addition to the obvious human rights violations described by the statistics above, experiencing SV has both immediate and long-term health consequences. Physical consequences include pregnancy (over 32,000 of which occur every year as a result of rape) as well as STI/HIV acquisition, chronic pain, gastrointestinal disorders, gynecological complications, migraines, cervical cancer, and genital injuries (Centers for Disease Control and Prevention, 2017). Immediate psychological consequences of SV include shock, denial, fear, confusion, anxiety, withdrawal, guilt, shame, distrust of others, and post-traumatic stress disorder, and longer term psychological consequences include depression, generalized anxiety, attempted or completed suicide, diminished interest or avoidance of sex, and low self-esteem (Centers for Disease Control and Prevention, 2017).
Research also shows a variety of subsequent health risk behaviors associated with having experienced SV including earlier sexual debut, unprotected sex, having multiple sexual partners, cigarette use, drunk driving, and illicit drug use. These behaviors put victims at risk of unplanned pregnancies, STIs, HIV, and cigarette, drug, and alcohol-related injuries and illnesses (Centers for Disease Control and Prevention, 2017). Furthermore, the estimated lifetime cost of rape is US$122,461 for the victim, with a population economic burden of $3.1 trillion over the victims’ lifetimes. These cost estimates include medical costs (39%), lost work productivity (52%), criminal justice–related activities (8%), and among other costs such as property loss and damage (1%; Peterson, DeGue, Florence, & Lokey, 2017).
The Current State of the SV Field
The state of the SV field is not adequate to successfully prevent perpetration. Instead, the field features a plethora of different programs including one-off, on-line sessions intended to prevent perpetration and promote bystander behavior (DeGue et al., 2014) or secondary and tertiary prevention programs that work with survivors of violence to prevent revictimization and help the criminal justice system successfully prosecute perpetrators (The White House Council on Women and Girls, 2014). For example, The Violence Against Women Act (VAWA), which is the backbone of the nation’s SV response (The White House Council on Women and Girls, 2014) and which was reauthorized in 2013 through fiscal year 2018 (Sacco, 2015), funds 28 grant programs, the vast majority of which are geared toward victim services and enhancing the criminal justice response to violence (Sacco, 2015). This reauthorization brought with it set-aside funding and new purpose areas for multidisciplinary sexual assault response teams, sexual assault nurse examiners, specialized law enforcement units, and training for criminal justice professionals (The White House Council on Women and Girls, 2014). It also includes new provisions to help previously overlooked survivors of SV including immigrants and the lesbian, gay, bisexual, transgender, queer, and questioning (LGBTQ) community. The 2013 reauthorization doubled funding for the Sexual Assault Service Formula Grant Program, which exclusively funds initiatives that help survivors on various steps in their road to recovery (The White House Council on Women and Girls, 2014). Unquestionably, these are all crucial aspects of a comprehensive approach to violence, yet these programs reflect a predominant focus on care and response rather than on primary prevention.
DeGue et al. (2014) conducted a systematic review of 140 outcome evaluations to describe the current primary prevention interventions being employed in the field and to assess the effectiveness of these programs for SV perpetration. Two thirds of the studies they reviewed consisted of brief, one-session interventions with college populations (n = 84). Only 11 of those measured sexually violent behavioral outcomes, none of which were found to consistently affect those behaviors. Rather, the majority of these intervention evaluations measured knowledge or attitudinal change as program outcomes; these are certainly related to behavior but are not necessarily sufficient to change behavior and may not be sustained over time. The review found only three primary prevention strategies in total for which there was sufficient evidence that they reduced SV perpetration behavior in a rigorous outcome evaluation, two of which were implemented among adolescent populations and one based on funding associated with the 1994 U.S. VAWA. Their review makes clear that the vast majority of efforts being made to curb perpetration are being implemented among college groups and that none of these interventions have been found to be effective; together, these two conclusions suggest that a paradigm shift is warranted to focus on younger groups and to emphasize primary prevention. The recent finding from a population-based survey of undergraduates in one campus context that more than one quarter of women and nearly one tenth of the men surveyed had experienced some form of prematriculation sexual assault (Mellins et al., 2017, p. 12) only underlines the importance of targeting primary prevention efforts at precollege students.
Moving Toward Effectiveness: Prevention Science
The field of prevention science has identified nine characteristics of effective prevention: (1) comprehensiveness, (2) varied teaching methods, (3) sufficient dosage, (4) theory-driven, (5) fosters positive relationships, (6) appropriately timed, (7) sociocultural relevance, (8) well-trained staff, and (9) outcome evaluations (Nation et al., 2003). DeGue et al. (2014) analyzed whether and to what extent the programs in their review met these criteria—and they by and large did not, which indicates why they may have collectively been so unsuccessful at reducing SV perpetration. Table 2 provides further detail about the ways in which the 140 outcome evaluations reviewed by DeGue et al. failed to meet the qualities of effective prevention. Table 2 also shows by comparison how a program that adheres to the NSES—which serves as the foundation for this article’s argument on best practices CSE—fulfills many of these same characteristics of effective prevention.
Qualities of Effective Prevention: Comparison of Studies Reviewed in DeGue et al. and of the National Sexuality Education Standards (NSES).
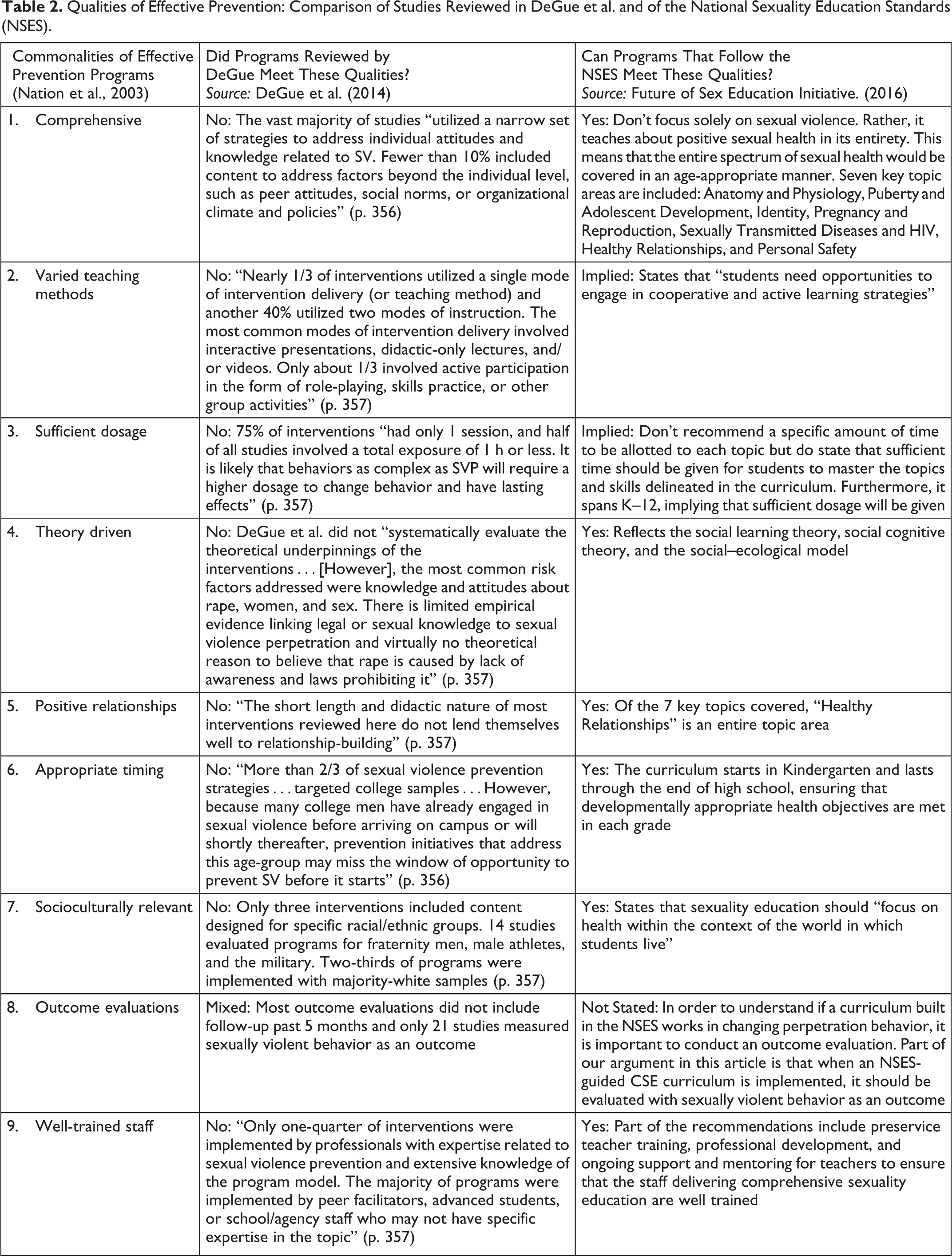
Experts in the field of sex education created the NSES in 2012 to serve as a guideline for the base minimum that all sexuality education programs should follow (Future of Sex Education Initiative, 2012). The Standards’ aim is to “provide clear, consistent and straightforward guidance on the essential minimum, core content for sexuality education that is developmentally and age-appropriate for students in grades K–12” (Future of Sex Education Initiative, 2012). The NSES were informed by the National Health Education Standards (Joint Committee on National Health Education Standards, 2007), the Centers for Disease Control and Prevention’s Health Education Curriculum Analysis Tool (Centers for Disease Control and Prevention, 2007), existing state and international education standards that include sexual health content (Future of Sex Education Initiative, 2012), and the Guidelines for Comprehensive Sexuality Education: Kindergarten-12th Grade (Sexuality Information and Education Council of the United States, 2004).
An NSES-guided CSE program meets the qualities of effective prevention in multiple ways. As the name implies, the standards are comprehensive, spanning a wide range of topics related to sexuality, sexual health, and overall well-being: anatomy and physiology, puberty and adolescent development, identity, pregnancy and reproduction, sexually transmitted diseases and HIV, healthy relationships, and personal safety (Future of Sex Education Initiative, 2012). The standards are theory-driven, drawing on social learning theory, social cognitive theory, and the social–ecological model (Future of Sex Education Initiative, 2016). Positive relationships are stressed as a key component of the standards. They emphasize age-appropriateness of the topics covered, spanning kindergarten through 12th grade, with different learning objectives in each grade level, thereby ensuring that students are reached before the onset of any risk behaviors and at a developmental moment where the information provided is relevant and appropriate. The standards recommend preservice teacher training, professional development, and ongoing support and mentoring to ensure that staff are well trained (Future of Sex Education Initiative, 2016). The standards also recommend the use of varied teaching methods. Lastly, the Standards cover multiple topics and thus intrinsically require a much higher “dosage” than the typical SV prevention program, with the NSES outline of the entire curriculum spanning K–12 with a multitude of learning objectives and topics to be included (Future of Sex Education Initiative, 2012). Table 2 maps out the NSES with the qualities of effective prevention in more detail.
Risk Factors for SV Perpetration
The fact that an NSES-guided curriculum meets the qualities of effective prevention in general, however, is only one piece of conceptualizing why it makes sense to explore it as a strategy for primary prevention of SV. Indeed, CSE traditionally aims to prevent health outcomes such as unplanned teenage pregnancy and HIV/STI acquisition, not SV (Chin et al., 2012; Haberland, 2015a; Kirby, Laris, & Rolleri, 2007; Lindberg & Maddow-Zimmet, 2012). The authors were not able to identify any published work to date evaluating the impact of CSE on SV behavior as a dependent variable. Healthy relationships are a component of sexuality education curricula that meet NSES standards, and yet the impact of CSE on unhealthy relationship behaviors such as SV or teen dating violence has not been evaluated as outcome measures, or at least not evaluated in a way that has been disseminated through the searchable peer-reviewedCSE scientific literature. The goal of this article is to map out conceptually the potential of CSE, in order to encourage research that examines the hypothesis that CSE could be effective prevention for SV perpetration behavior in addition to the more traditional health outcomes, and thus that it should be evaluated as a dependent variable of an NSES-guided K–12 CSE program. The other crucial elements in proposing evaluation of the impact of best practices CSE on SV are (1) to examine whether known risk factors for SV perpetration have been shown to be amenable to modification through educational intervention in the past and (2) to assess the extent to which these risk factors would be addressed through NSES-CSE.
Tharp et al.’s (2012) systematic review of risk and protective factors for SV perpetration summarized 191 published empirical studies that examined perpetration by and against adolescents and adults. Two societal and community factors, 23 relationship factors, and 42 individual-level factors were identified (n = 67). Of these 67 factors, 35 of them displayed consistently significant association with SV. All 35 of these factors, which were at the individual, interpersonal, or relationship level of the social–ecological model, are presented in Table 3. That these factors exist across multiple levels of the ecological model underline the need for a prevention approach that works across the models’ different levels. (Some of those risk factors, such as previous suicide attempt, sports and fraternity participation, or having experienced physical or emotional abuse as a child, fall substantively outside of the goals of NSES-CSE, underlining that even if it is found to be effective at reducing SV by addressing some of the underlying risk factors, a truly comprehensive approach will be comprised of layered strategies across the ecological level over multiple points in the life course.) The risk factors can be grouped into four overarching categories: sex, gender, and violence-related risk factors; child abuse–related risk factors, sexual behavior–related risk factors, and social and emotional intelligence–related risk factors.
Sexual Violence Perpetration Risk Factors Found to be Significant (Adapted from Tharp et al. [2012]) and Potential for CSE to Mitigate Those Risk Factors.
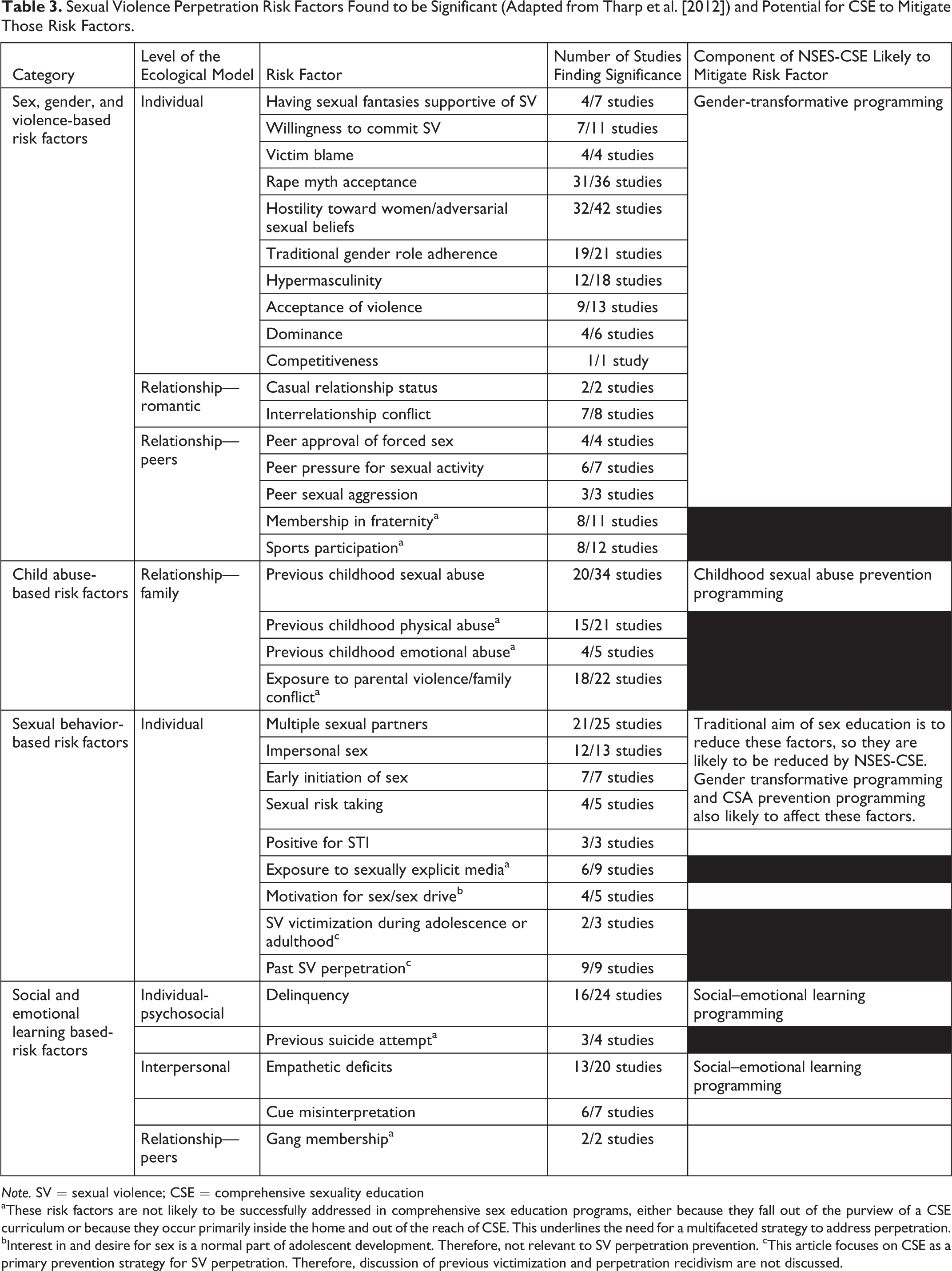
Note. SV = sexual violence; CSE = comprehensive sexuality education
aThese risk factors are not likely to be successfully addressed in comprehensive sex education programs, either because they fall out of the purview of a CSE curriculum or because they occur primarily inside the home and out of the reach of CSE. This underlines the need for a multifaceted strategy to address perpetration. bInterest in and desire for sex is a normal part of adolescent development. Therefore, not relevant to SV perpetration prevention. cThis article focuses on CSE as a primary prevention strategy for SV perpetration. Therefore, discussion of previous victimization and perpetration recidivism are not discussed.
Sex, Gender, and Violence
The largest category of risk factors found to be significant in Tharp et al.’s (2012) review fall under sex, gender, and violence (Table 3). At the individual level, these include having sexual fantasies supportive of SV, willingness to commit SV, engaging in victim blaming, rape myth acceptance, hostility toward women/adversarial sexual beliefs, traditional gender role adherence, hypermasculinity, acceptance of violence, dominance, and competitiveness. At the peer-relationship level, these include peer approval of forced sex, peer pressure for sexual activity, peer sexual aggression, membership in a fraternity, and sports participation. At the romantic-relationship level, these include having a casual relationship status and having interrelationship conflict. These risk factors are fundamentally tied to gender and sexual norms and cognitions (Casey & Lindhorst, 2009; Heise, 1998).
Tharp’s review failed to find the structural-level risk factor for gender as significant for SV perpetration, despite the intrinsic relationship between the broader social organization of gender and these relationship and individual-level manifestations of gendered practices and beliefs. This failure to find empirical evidence for the structural concept of gender as a risk factor may reflect the review’s exclusion of qualitative and ethnographic research and their focus on biomedical rather than social scientific research. Ethnographic and qualitative empirical work (e.g., Armstrong, Hamilton, & Sweeney, 2006; Sanday, 1981, 1996) grounded in social scientific theory certainly demonstrates that the social organization of gendered power is a critical underlying social driver of the sexual assault of women, as does both foundational work in gender theory (Connell, 1987) and quantitative social scientific research that looks comparatively at social organization and gender power (Whaley, 2001). An extensive discussion of the range of research not included in the Tharp et al. (2012) is beyond the scope of this article, but because our argument for NSES-CSE as a strategy to prevent SV relies on the ecological model, this question about the role of broader community and social norms is critical because of their framing, in the ecological model, as shaping factors at the individual, family, peer, and relationship levels (Casey & Lindhorst, 2009; Fulu et al., 2013; Heise, 1998; Jewkes, Flood, & Lang, 2015). An understanding of inequitable gender relations as a foundational structural driver of SV is thus necessary in any discussion of SV perpetration prevention (Fulu et al., 2013; Jewkes et al., 2015).
There is without question evidence from other sources that unequal gendered access to power is an underlying cause of SV (Breger, 2014; Casey & Lindhorst, 2009; Courtenay, 2000; Fulu et al., 2013; Heise, 1998; Jewkes et al., 2015; Kågesten et al., 2016). These manifestations include many of the risk factors identified in this review clustered within the sex, gender, and violence risk factors category. Feminist theory offers at least two ways of thinking about the social processes through which gender, masculinity, and violence are related (Anderson, 2005). The first is that violence is a mechanism through which men can prove their masculinity, and thus, performing acts of violence causes or leads to a societally accepted depiction of masculinity (Anderson, 2005). The second is that gender is a social structure that influences opportunities and rewards for violent behavior. Men who fit the acceptable ideal of masculinity—or hegemonic masculinity—are rewarded for their behavior by maintaining power and control within society (Anderson, 2005). Hegemonic masculinity in much of the world, and especially in the United States, encompasses heterosexual success, dominance and control over women, sexual entitlement, and strength and toughness (Jewkes et al., 2015). When combined in a society that allows men to perpetrate with fairly little consequences, these qualities can contribute to a dangerous formula for SV perpetration.
The ecological model is conceptualized as embedded levels of causality (Heise, 1998), and thus, shifting the societal, inequitable gender norms that sit in the outer level of the model will in turn affect relationship, peer, and individual gendered relations, cognitions, and behaviors. “Gender-transformative” interventions are defined as those that aim to “reconfigure gender roles in the direction of more gender equitable relationships” (Dworkin, Treves-Kagan, & Lippman, 2013, p. 2846). Furthermore, they “view masculinities as a set of social norms that are modifiable in order to attain reduced rates of violence, decreased levels of unsafe sex, and improvements in inequitable gender relations” (p. 2846) These interventions acknowledge gender as the central component in the perpetration of SV and thus place it at the epicenter of the theory of change.
Based on this definition, NSES-CSE would be defined as gender-transformative (Table 4). A mere glance at the standards delineates this clearly: By the end of second grade, programs provide children with the critical thinking capacity to discuss the similarities and differences in how boys and girls may be expected to act; provide examples of how friends, family, media, and culture can influence the ways girls and boys think they should act; and learn about gender and gender roles. By the end of fifth grade, students can define sexual orientation and demonstrate ways to show respect and treat others with dignity. By the end of eighth grade, students explore gender expression and analyze the potential impact of individual, family, and cultural expectations on gender, gender roles, and gender stereotypes; they begin to analyze the impact of gender inequities on relationships including on power dynamics, communication, and decision-making; they can differentiate between sexual orientation and gender identity; and they can demonstrate respectful communication with people of all gender identities, gender expressions, and sexual orientations (Future of Sex Education Initiative, 2012).
How NSES-CSE Addresses the Majority of Risk Factors for SV Perpetration.
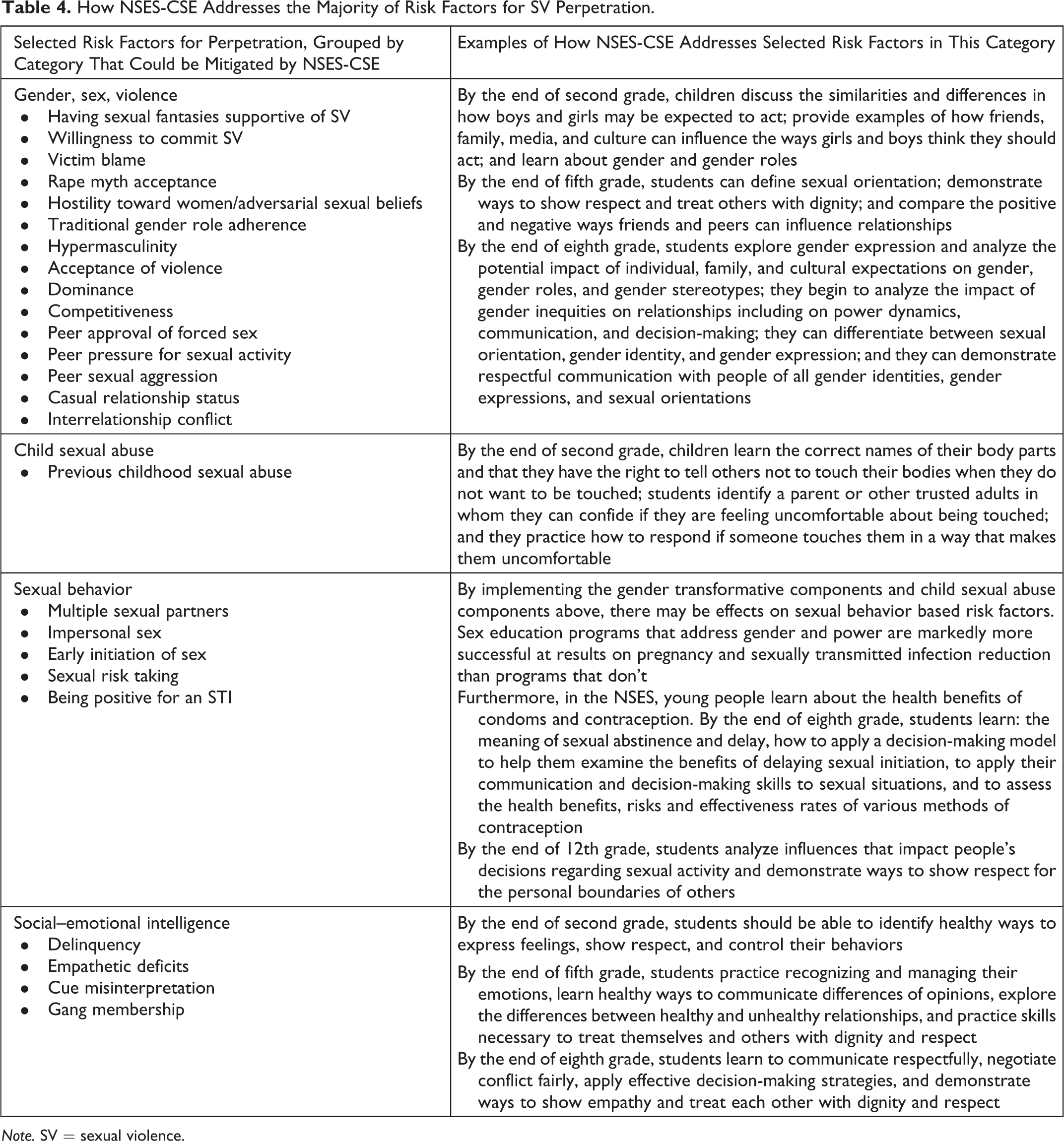
Note. SV = sexual violence.
To examine what is known about whether effective interventions exist to transform gender norms, Dworkin et al. (2013) conducted a systematic review of gender-transformative programming in relation to HIV. The review included 15 research articles. To be included, articles had to measure either a reduction in HIV/STI incidence, sexual risk behaviors, violence against women, or normative change in attitudes as outcomes. Of the 15 studies included, nine evaluated a change in gender norms through small group educational interventions with adolescents and young adults. There was a high degree of variability in indicators measuring a change in gender norms including attitudes about gender and masculinity; discussing sex, HIV prevention, condom use, and HIV testing with a main or casual partner; recognition of abuse; and acceptance of violence toward women. Eight of these showed statistically significant results on at least one indicator of gender norms. This review delineates that gender-transformative interventions employed in small group educational settings can be successful at changing gender norms with adolescents and young adults, indicating that NSES-CSE could also successfully change gender norms, leading to a potential reduction in SV perpetration through mitigation of this risk factor. Furthermore, CSE programs that address gender and power have had markedly better results on pregnancy and STI reduction than sex education programs that fail to do so (Haberland, 2015b). Different types of sexual and reproductive health programs, such as reproductive health interventions for married girls, men in maternity projects, and microcredit programs for marginalized women, have also found that programs that address gender and power yields much more significant results than programs that don’t, indicating that gender is a core component of sexual and reproductive health generally (Haberland, 2015b). As SV is a component of sexual and reproductive health, this is likely to hold true in the SV prevention arena as well.
Child Abuse
The prevention of child abuse—which includes not just sexual abuse but also physical abuse more broadly as well as emotional abuse—is important for several reasons, the foremost being to stop the current abuse being faced by the child. Secondarily, child abuse prevention may halt the cycle of abuse that occurs when people who have been formerly abused become perpetrators as adults. Child abuse and witnessing family violence are both risk factors for perpetration later in life (Tharp et al., 2012). Abuse can leave emotional, psychological, and developmental scars and children who are exposed to abuse in early childhood can become prone to aggression, impulsivity, and an absence of empathy or remorse (Heise, 1998; Jewkes et al., 2015). Furthermore, social learning theory adds that children may learn that violence can be used as a mechanism to get one’s way and adopt this behavior as an adult (Heise, 1998).
Both conceptual and empirical work suggest that NSES-CSE can help prevent child sexual abuse (CSA). Research shows that ability of a child to prevent or report child abuse is dependent, in part, on their understanding of their bodies, including the correct names of body parts, the recognition that they have bodily autonomy, and the skills to communicate with a caring adult regarding perceived or real danger (Future of Sex Education Initiative, 2016).
The American Academy of Pediatrics (2011) recommends that children learn the names of genitals along with other body parts to understand that “the genitals, while private, are not so private that you can’t talk about them.” In the NSES (Table 4), by the end of second grade, children learn the correct names of their body parts and that they have the right to tell others not to touch their bodies when they do not want to be touched, students identify a parent or other trusted adults in whom they can confide if they are feeling uncomfortable about being touched, and they practice how to respond if someone touches them in a way that makes them uncomfortable (Future of Sex Education Initiative, 2012).
A recent systematic review (Walsh, Zwi, Woolfenden, & Shlonsky, 2015) compiled evidence of the effectiveness of a school-based program to prevent CSA. The review included 24 studies, with 10 aimed at younger participants from kindergarten through third grade, eight aimed at fourth grade and older, and six studies had both younger and older participants. Programs ranged from a single 45-min session to eight 20-min sessions on consecutive days. This review was conducted to assess whether programs are effective in improving students’ protective behaviors and knowledge about sexual abuse prevention; if behaviors and skills are retained over time; and whether participation results in disclosures of sexual abuse, produces harms, or both. Protective behaviors were enhanced at immediate posttest, the intervention group had gains in factual and applied knowledge up to 2 weeks postintervention with studies having a 1- to 6-month follow-up showing maintenance of knowledge, and odds of disclosure were as much as 3.5 times higher in the intervention participants.
These results suggest that schools can be an effective vehicle for CSA prevention and intervention, as well as underlining the need for complementary strategies that focus on the prevention of emotional and physical abuse. The studies included in the review all had the primary goal of reducing CSA and were not significantly long in duration or fully comprehensive. Including CSA prevention within a larger CSE framework, as is done in the NSES, may produce better results because it would feature the qualities of effective prevention described at length above. Furthermore, it is important to note that education tailored to the child should be part of a larger strategy to prevent CSA and the onus of prevention should not be placed on the child. However, being able to recognize signs of abuse, name body parts, develop bodily autonomy, and tell a trusted adult can help a child get out of a sexually abusive situation.
Sexual Behavior
Tharp et al. (2012) identify a number of sexual behavior–related factors that consistently demonstrate a strong association with perpetrating SV: having multiple sexual partners, impersonal sex, early initiation of sex, sexual risk taking, and being positive for an STI. One factor that the literature has attributed this association to is that enacting these behaviors are mechanisms to negotiate power, demonstrate masculinity, and display an emphasized heterosexuality (Courtenay, 2000; Grazian, 2007; Jewkes, 2012; O’Sullivan, Hoffman, Harrison, & Dolezal, 2006; Ott, 2010; Pleck, Sonenstein, & Ku, 1993; Santana, Raj, Decker, Marche, & Silverman, 2006; Shearer, Hosterman, Gillen, & Lefkowitz, 2005), all of which fall under the domain of gender inequity across the social ecology and have already been discussed as risk factors for SV perpetration above. Another factor that can help to explain this association is that early (consensual) initiation of sexual activity and increased high-risk sexual behaviors are associated with childhood sexual abuse (Jewkes, 2012), which has also already been discussed as a major risk factor in perpetration. Proposed pathways from childhood sexual abuse to high-risk sexual activity include the development of maladaptive sexual scripts, avoidant coping mechanisms such as alcohol and drug use which could lead to sexual risk behavior, difficulties with attachment and trust which can lead to a series of short or concurrent sexual relationships, and self-efficacy issues that inhibit formerly abused individuals from being able to control sexual situations as adolescents (Senn, Carey, & Vanable, 2008). The fact that these sexual behaviors and SV perpetration share a host of risk factors may contribute to the strong association between the two.
Our discussion has already explained the ways in which NSES-CSE can potentially affect gender-related risk factors, as well as its potential to intervene in and prevent childhood sexual abuse. As these are two prominent explanations linking sexual risk behaviors to SV perpetration, it is likely that the gender-transformative components and childhood sexual abuse components of NSES-CSE can also have effects on the sexual behavior-related risk factors identified in Tharp et al. (2012). The traditional aim of CSE is to impact sexual risk behaviors such as early sexual initiation, impersonal sex, and multiple sexual partners, as well as their associated outcomes such as pregnancy and HIV/STI acquisition, and there is substantial evidence that it is successful in doing so (Chin et al., 2012; Haberland, 2015a; Kirby et al., 2007; Lindberg & Maddow-Zimmet, 2012). As has been previously noted, evidence also suggests that CSE programs that address gender and power are more successful at achieving its intended results than conventional sex education programs that do not address these risk factors (Haberland, 2015b). As the NSES takes a gender-transformative approach to CSE, it is likely that it will be successful in reducing sexual risk behaviors as well as these shared risk factors.
Social–Emotional Skills
The last group of risk factors for SV perpetration falls under “social–emotional” skills that young children acquire and develop through adolescence, which include the ability to recognize and manage emotions, establish and maintain positive relationships, make responsible decisions, appreciate the perspective of others, and handle interpersonal situations constructively (Elias et al., 1997). Manifestations of poor social–emotional skills include several risk factors for SV perpetration including a lack of empathy, cue misinterpretation, and delinquency. Social–emotional learning (SEL) programs aim to enhance the social–emotional skills of students, with the proximal goals being to foster “the development of five interrelated sets of cognitive, affective, and behavioral competencies: self-awareness, self-management, social awareness, relationship skills, and responsible decision-making” (Durlak, Weissberg, Dymnicki, Taylor, & Schellinger, 2011, p. 406)
The NSES include a core set of learning objectives explicitly aimed at enhancing the social–emotional skills of students (Table 4). By the end of second grade, students should be able to identify healthy ways to express feelings, show respect, and control their behaviors. By the end of fifth grade, students practice recognizing and managing their emotions, learn healthy ways to communicate differences of opinions, explore the differences between healthy and unhealthy relationships, and practice skills necessary to treat themselves and others with dignity and respect. By the end of eighth grade, students learn to communicate respectfully, negotiate conflict fairly, apply effective decision-making strategies, and demonstrate ways to show empathy and treat each other with dignity and respect (Future of Sex Education Initiative, 2012). This instruction falls directly under the purview of an SEL program.
A 2011 meta-analysis of SEL programs (Durlak et al., 2011) delineated the effects that SEL can have on a variety of skills, attitudes, and behaviors in children and adolescents relevant to SV perpetration risk factors. The meta-analysis combined findings from 213 studies. More than half of the programs were administered to elementary school students (56%) and about a third to middle school students (31%). Compared to control groups, students in the SEL intervention displayed enhanced SEL-related skills, attitudes, and positive social behaviors, demonstrated fewer conduct problems, had lower levels of emotional distress, and had improved academic performance. These programs thus show efficacy in affecting risk factors for SV perpetration, indicating that a school-based SEL program, like the NSES, can be successful.
K–12 Justification
One of the potentially most controversial dimensions of the prevention approach proposed here is that SV prevention begins in kindergarten. While some advocate strongly for this, others have argued just as strongly against the idea of providing “sex education” to kindergarteners (de Melker, 2015; Rohter, 2008), who will not begin engaging in perpetration behavior or sexual activity for some time. However, in line with the public health approach to prevention, it is crucial to look upstream at when in the developmental process the risk factors for perpetration begin to form (Harvey et al., 2007). As this article has shown, a plethora of risk factors that can lead to perpetration do in fact begin to form early on in the life course, and thus, engaging in prevention during this window is crucial. There are at least three important reasons for beginning prevention early.
The first and most obvious of the risk factors that need to be addressed early on is the prevention of CSA. The substantial burden of suffering associated with CSA underlines the importance of addressing SV prevention early on. One in nine girls and 1 in 53 boys under the age of 18 experience sexual abuse or assault at the hands of an adult (RAINN, 2018). From 2009 to 2013, child protective services data show that 63,000 children a year were victims of sexual abuse—a statistic that is most likely an underestimate due to lack of reporting (RAINN, 2018). Of the 63,000 cases, 80% of perpetrators were parents and 6% were other relatives, and 88% of CSA cases involve a male perpetrator (RAINN, 2018). Taking a life-course approach to prevention and attending to the substantial evidence linking experiences of CSA to future perpetration of SV (Greathouse, Saunders, Matthews, Keller, & Miller, 2015) emphasizes the importance of integrating CSA prevention into a wider CSE curriculum as a strategy to reduce later perpetration.
The second and less obvious reason to begin early is that the formulation of gender roles and cognitions begins in childhood. While a comprehensive overview of feminist developmental psychology is beyond the scope of this article, one key insight from that work is the idea that the gender inequities in power and status which exist in society influence children’s development (Leaper, 2000). A host of socialization practices exist that can conform children to gender roles and stereotypes very early on in the life course that go on to create their gender schemas in adolescence and adulthood. Children learn gender through their social interactions and daily activities, for example, when toys, sports, and activities are gender-typed, which can groom boys to compete for dominance. Children also learn gender by observing their own and the other genders and inferring patterns of appropriate behavior. From there, they begin socializing one another to conform to gender norms as part of peer group behavior. This can often manifest in “masculine protest,” the complete avoidance and devaluation of feminine-stereotyped qualities very early on (Leaper, 2000). These gender-shaping processes that often lead to male adherence to gender roles happen in early childhood development, and schools are often a vehicle through which this occurs (Adler, Kless, & Adler, 1992; Connell, 1996; Jordan, 1995; Messner, 2000; Renold, 2000, 2001; Swain, 2000). It is therefore critical to intervene in the gender-stereotyping process as early on as possible. Furthermore, teaching children about what it means to give and receive permission to do something and how to share and play with others can offer early, age-appropriate instruction about what it means to elicit or convey consent. Starting instruction as early as possible could help mitigate rigid and harsh gender stereotypes from forming, reducing potential perpetration behavior that stems from these risk factors later on in life. Intervening beginning in kindergarten, before children have engrained gender norms that guide their self-concepts, motivations, and expectations of others, could mitigate the potential harm that comes from rigid- and hypermasculinity. Furthermore, early instruction to address gender-stereotyping might create safer climates for LGBTQ and gender nonconfirming students as they grow up, who experience much higher rates of sexual harassment and violence than heterosexual and cisgender populations (Ford & Soto-Marquez, 2016; Katz-Wise & Hyde, 2012; Mitchell, Ybarra, & Korchmaros, 2014).
Lastly, as DeGue et al. (2014) delineated, most of the work in SV prevention thus far has focused on college students (70%), with the next highest number of interventions focusing on students in high school (14.3%). This may be in response to the legal requirements at the federal and state level (Lebioda, 2015; Morse, Sponsler, & Fulton, 2015; Office of Civil Rights, 2011) for institutions of higher education to offer or require some form of prevention education. However, the overwhelming focus on higher education as a site for SV prevention is intrinsically in tension with the underlying notion of primary prevention grounded in an understanding of the risk factors discussed throughout this article. Even if college programs had been shown to be effective, many people experience sexual assault before entering college (Smith et al., 2017), and only roughly 59% of the adult population ever attends “some college” (Ryan & Bauman, 2016). Between half and three quarters of the men who commit rape first do so as teenagers (Jewkes et al., 2015). Therefore, while college-level interventions are most definitely part of the solution, there is a need to start primary prevention earlier in the life course to reach individuals before they start perpetration behavior.
College-level interventions are most certainly necessary in an overarching SV prevention plan but should not be the first interaction that individuals have with SV prevention. The whole conceptualization of a life-course approach to primary prevention of SV presented in this article, as well as the discussion of preventing the initial perpetration of SV by targeting the risk factors that are most implicated in the behavior, underlines the limits of having a first encounter with prevention concepts at the college level.
Limitations
Without question, while NSES-CSE holds the potential to successfully mitigate many of the risk factors implicated in SV perpetration and—if implemented widely—subsequently curb the high rates of societal SV, it cannot do so alone. Child abuse provides a good example of both the promise and the limits of NSES-CSE as a prevention strategy; while evidence exists that it can have an impact on CSA, there are clearly a host of risk factors that CSE does not reach, such as events and interactions that happen in the home, and there is little evidence that NSES-CSE would be an appropriate or effective strategy for preventing the emotional or physical abuse of children. We have explored the role that NSES-CSE can play in preventing and stopping CSA, but there are other strategies that must also be employed to reach within the family where CSE cannot. Enhanced primary care and behavioral parent training programs are two such approaches (Fortson, Klevens, Merrick, Gilbert, & Alexander, 2016).
Furthermore, gender stereotypes that go on to create hypermasculinity complexes and entrench traditional gender roles often begin before a child is born—at “gender reveal” parties and via painting bedrooms pink or blue. NSES-CSE alone will not undo the inequitable societal gender norms that permeate every level of society. It cannot undo the gendered structure of the labor market, for example, or the gendered stereotypes disseminated through popular culture. It does, however, have the power to buffer and help students develop critical attitudes toward beliefs, attitudes, and behaviors about gender, and in that way mitigate the gender-related risk factors that can lead to perpetration.
A multipronged strategy is necessary to curb rampant SV. Primary prevention of perpetration must be complemented by strategies that include secondary and tertiary prevention, such as initiatives that address perpetration recidivism, as well as strategies that help prevent victimization and work with survivors in the aftermath of their attack in a trauma-informed way, through the criminal justice system and elsewhere. For example, rape crisis centers and women’s shelters play a critical role in keeping women safe from violent household situations or in getting help after being attacked, and this article does not aim to diminish those services in any way.
The work that we present here is not a systematic review because there is very little in the way of evidence for effective prevention of SV perpetration. Instead, we selected literature, including review articles that already synthesized various bodies of literature, to knit together knowledge across topic areas to suggest a new approach to prevention—one that is urgently in need of research and evaluation. This included summarizing the state of the field of SV perpetration, the risk factors for SV perpetration, interventions that have been shown to reduce these risk factors, and how NSES-CSE can effectively mitigate those risk factors. The authors conceptualized this endeavor as piecing together a puzzle: The pieces to the puzzle already exist (systematic reviews of perpetration risk factors, of the evidence regarding perpetration intervention effectiveness, and of how different risk factors can be mitigated by different types of interventions) but they needed to be assembled, so that future researchers could then take this as a charge to examine empirically the impact of NSES-CSE on SV perpetration (Figure 1). This article’s aim is to stimulate research in sex education and SV perpetration by connecting these previously separate bodies of research (Figure 1), all of which already had systematic reviews and analyses.
A further limitation is the focus here on cisgender, heterosexual men and women. Numerically, data suggest that the preponderance of assaults are perpetrated by cisgender heterosexual men and experienced by cisgender heterosexual women. However, the rates of SV have been shown to be very high among LGBTQ populations (Ford & Soto-Marquez, 2016; Katz-Wise & Hyde, 2012; Mitchell et al., 2014). It is vital therefore for other work to fill the gap that we have left here, mapping the potential impact of CSE for those groups, and for subsequent evaluation research to explicitly examine the impact of CSE on rates of sexual assault among LGBTQ populations.
Another limitation is that K–12 CSE guided by the NSES has neither been widely implemented nor evaluated. The evidence chosen to support our argument was based on similar interventions—tailored to certain perpetration risk factors—in educational and small group settings that NSES-CSE would most likely resemble. It may be that the enormous recent popular media attention to sexual harassment and assault in the United States (Baumgartner & McAdon, 2017; “Beyond Harvey Weinstein,” 2017; Fantz, 2016; Gabler, Twohey, & Kantor, 2017; Martin & Stolberg, 2017; Savransky, 2017; Zacharek, Dockterman, & Edwards, 2017) will provide an impetus to reexamine opportunities for population-level prevention, and CSE certainly offers one such opportunity.
Finally, it may seem politically unrealistic in the current federal environment to implement CSE, especially when funding streams are more closely tied to abstinence-only, or “sexual risk avoidance” programs than to comprehensive sexuality programs. However, despite federal funding having emphasized abstinence-only programs since the mid-1990s, states and municipalities have acted to increase access to comprehensive programs. California passed the Healthy Youth Act in 2015, which requires all public schools to teach CSE in Grades 7–12 with the option to start earlier (California Department of Education, 2017), and New York City mandated in 2011 that public schools teach CSE as well (NYC Department of Education, 2011). There are also other avenues outside of government to implement CSE, such as through private foundation funding. In 2009, The Grove Foundation, a private philanthropic foundation that strives to improve adolescent health, launched the Working to Institutionalize Sex Education (WISE) initiative (Butler, Sorace, & Beach, 2018). WISE’s mission is to provide support to school districts to advance CSE programs and to document how implementation can be advanced and institutionalized. Rather than endorse a specific curriculum, WISE works with school districts to choose curricula that fit their needs. Implementation plans vary in scope from one grade level to K–12 programs, but at a minimum are all age-appropriate, evidence-informed, and compliant with state laws and standards. Since its launch, $7 million have been invested in 13 states; 88 school districts reached their implementation goals and institutionalized sex education and 788,865 unique students received new or improved sex education in school. The evaluation of WISE found that “resources and expertise help schools advance and meet their sex education institutionalization goals and that barriers that impede sex education can be mitigated, leading to increased quality and quantity of sex education in ready school districts” (Butler et al., 2018).
Conclusion
Without question, a plethora of risk factors are implicated in SV perpetration. Addressing one risk factor alone is unlikely to substantially reduce the incidence of SV. A comprehensive strategy is needed to affect multiple risk factors across the social ecology. Individual, interpersonal, community, environmental, and societal level risk factors all contribute to health and social problems including SV. As noted in Table 5, NSES-CSE is potentially one powerful component of a multipronged strategy to lower the unacceptably high rates of SV seen in the United States. Its unique value is implicit in the name itself: It is comprehensive (Figure 1). While sex education has been traditionally designed, implemented, and evaluated to reduce unplanned teenage pregnancies, HIV/STI acquisition, and the health risk behaviors that lead to these outcomes, it holds the potential to address SV perpetration as well. As a high-dosage sequential program, it not only addresses these sexual risk behaviors, but it also embodies gender transformative programming, social and emotional learning, and child abuse prevention, and it adheres to the commonalities of effective prevention programs, which have been widely cited in the literature. Most importantly, it begins to address the risk factors for perpetration behavior long before the onset of that behavior. Primary prevention is the most effective way of fully preventing poor health outcomes by mitigating risk factors from developing.
Critical Findings.
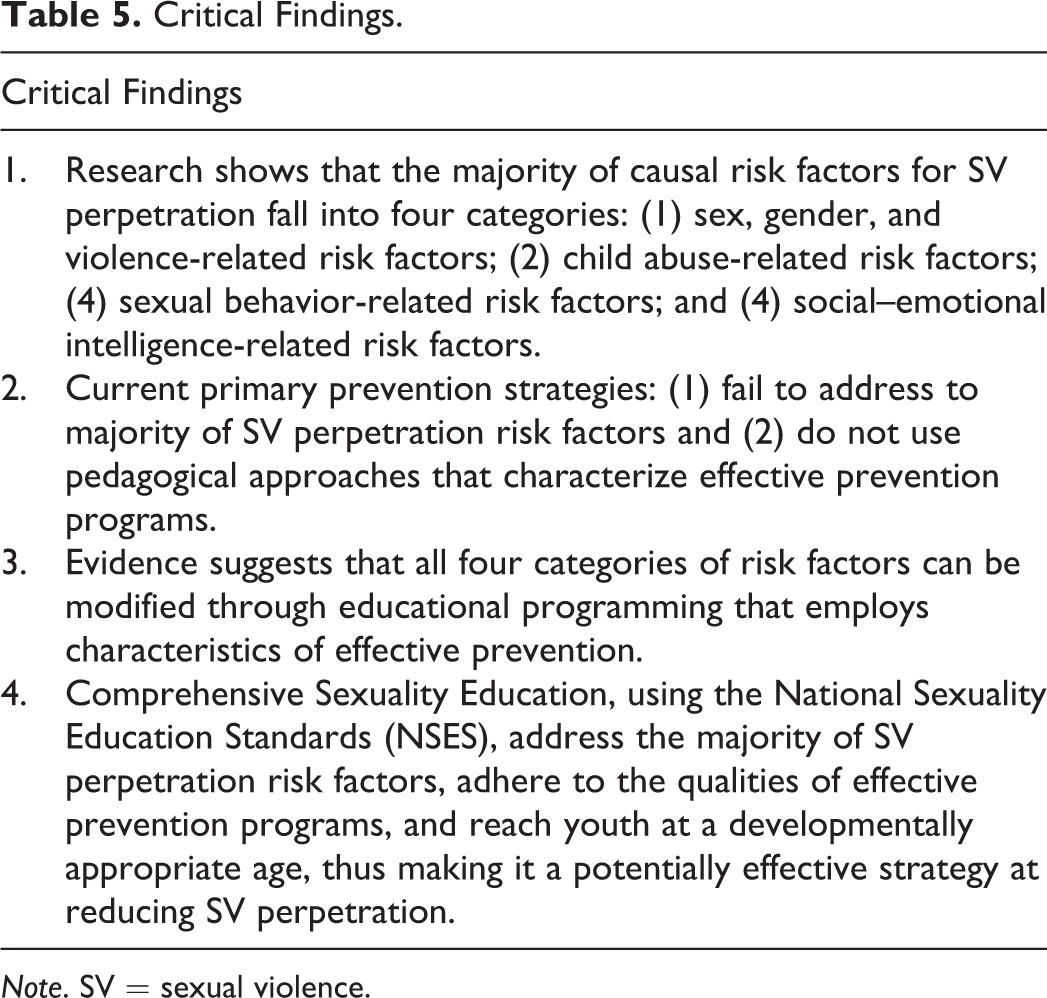
Note. SV = sexual violence.
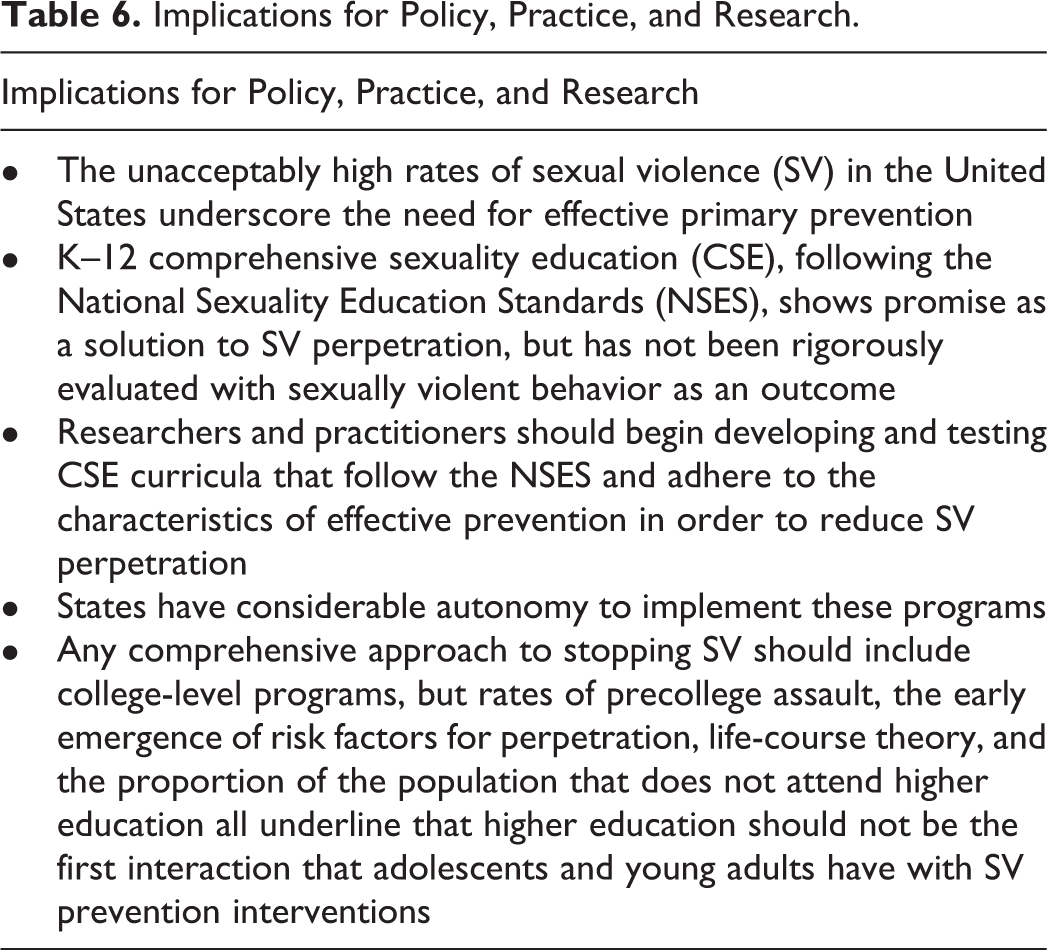
When implemented according to best practices and over a sustained period, NSES-CSE holds tremendous potential as an intervention approach; the implications of this argument for policy and practice are summarized in Table 6. No published peer-reviewed research to date evaluated the impact of NSES-CSE on sexually violent behavior, and this article presents evidence for its potential to affect this outcome. The authors recommend that where NSES-CSE is implemented, it should be assessed for impact longitudinally by following students as they are exposed to CSE and looking at their behaviors over time. The social climate is certainly ripe for this work, with public figures being called out as sexual predators as a near-daily occurrence and a sustained public discussion about what, beyond holding the individuals accountable for their behavior, might produce a broader change in the climate. Remedial education on SV in late adolescence and in college cannot by itself be the solution; CSE that gets to the root of the problem before the problem begins may be one key component of a comprehensive strategy to end SV.
Implications for Policy, Practice, and Research.
Footnotes
Acknowledgments
The authors would like to thank the Department of Sociomedical Sciences, the Columbia Population Research Center (P2CHD058486), and the Sexual Health Initiative to Foster Transformation for their support. They would also like to thank Dr. John Santelli for his comprehensive review of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.