
Abstract
The aim of the systematic review described in this article was to determine the outcomes for individuals exposed to severe neglect in congregate care institutions such as orphanages. In this context, severe neglect refers to failure to meet children’s basic physical, developmental, and emotional needs due to inadequate resources. In this systematic review of previous systematic reviews and meta-analyses, searches of 10 databases were conducted, 18 papers that met inclusion and exclusion criteria were selected for review, their quality was assessed, and data were extracted and synthesized. The 550 primary studies included in the 18 systematic reviews and meta-analyses were relatively well designed, allowing confidence to be placed in their results. Severe neglect was associated with a wide range of problems in the domains of physical development, cognitive development, attachment, and mental health. The severity of adverse outcomes was partly influenced by the duration and severity of deprivation and a constellation of risk and protective factors. Prevention policies should aim to eliminate large underresourced congregate care institutions for infants. In taking steps toward this, policies should aim to adequately resource congregate care institutions to meet children’s developmental needs for nutrition, stimulation, and attachment to a stable primary caregiver with adequate parenting skills and training. Early placement in adoptive or foster families, with access to routine physical and mental health-care service available in developed countries, is the most viable effective intervention for child survivors of severe neglect.
This article is a review of review papers on the outcome of severe neglect in orphanages that care for large groups of children, with inadequate and unstable staffing, and limited physical resources. It is the second in a series of three on the outcome of child maltreatment. The first article is a review of review papers on the outcome of child abuse in noninstitutional contexts (Carr, Duff, & Craddock, 2018a). The third article is a review of studies of outcomes for survivors of child abuse that occurred in long-term residential care (Carr, Duff, & Craddock, 2018b).
Severe neglect, which is also referred to in the literature as structural neglect, refers to failure to meet children’s basic physical, developmental, and emotional needs within the context of orphanages that care for large groups of children, with inadequate and unstable staffing, and limited physical resources (van IJzendoorn et al., 2011). Distinctions may be made between the failure of institutions to meet three broad types of childhood needs (Gunnar, Bruce, & Grotevant, 2000). These include (1) physical needs such as nutrition, medical care, and hygiene essential for healthy physical growth; (2) developmental needs for stimulation to promote sensory motor, cognitive, and language development; and (3) the need for stable and meaningful interpersonal relationships with a primary caregiver to facilitate the development of secure attachment and the capacity to make and maintain social relationships.
The prevalence of severe neglect associated with placing children in institutions is difficult to determine. Using 2002 government statistics, Browne, Hamilton-Giachritsis, Johnson, and Ostergren (2006) estimated that 43,842 (14.4/10,000) children under 3 years of age were in institutional care within 46 European and Asian countries. Surprisingly, within Europe, institutional care of young children was not restricted to developing countries but occurred throughout the entire region. Using 2001 U.S. Department of Health statistics, Browne et al. (2006) estimated that 11,777 children in the United States were in childcare institutions. In Europe, Asia, and the United States, most children were placed in care due to maltreatment, abandonment, or because of a disability. In the developing world (e.g., Africa and South America), vast numbers of young children are in institutional care, but prevalence statistics are unavailable.
In industrialized countries in the second half of the 20th century, there has been a gradual reduction in the use of large congregate settings to care for orphans (Hamilton-Giachritsis & Browne, 2012). Large orphanages came to be replaced by the provision of care by foster families and smaller family-like care centers. Policies underpinning this trend were influenced by Bowlby’s (1951) seminal research on the critical role of parent–child attachment and the vast body of research which this spawned. This research showed that children raised in large institutions developed a wide range of problems in the domains of physical health including growth failure and impaired neurobiological development, mental health difficulties including behavior problems and impaired cognitive development, and problematic social adjustment including attachment difficulties and problems making and maintaining relationships (Bakermans-Kranenburg et al., 2011; McCall, 2013; Nelson, Bos, Gunnar, & Sonuga-Barke, 2011; Van IJzendoorn et al., 2011).
Many primary studies have been conducted on the effects of severe neglect, especially on orphans adopted from developing countries. A number of systematic reviews and meta-analyses have been published, which synthesize the results of these studies. In the current study, a systematic review was conducted, limited to the identification of these previous systematic reviews and meta-analyses.
The aim of the systematic review described in this article was to determine the outcomes for individuals exposed to severe neglect in institutions, especially orphanages, in terms of adjustment across the life span. In this context, adjustment referred to physical health including growth failure and impaired neurobiological development, cognitive development, attachment, and mental health.
Method
Guidelines for conducing systemic reviews of systematic reviews were followed in developing a protocol for this review (Smith, Devane, Begley, & Clarke, 2011). The protocol specified the aim, databases to be searched, search terms, study selection criteria, supplementary manual search strategies, data extraction system, study quality assessment procedures, and data synthesis methods. The review was registered with PROSPERO at the Centre for Reviews and Dissemination, University of York (https://www.crd.york.ac.uk/PROSPERO/registerReview.php#index.php). The registration number is CRD42017065095.
Search Terms
Record titles, abstracts, and key words were searched in the electronic databases listed in the next section. Using appropriate Boolean operators, terms denoting institutional care were combined with terms reflecting a range of possible negative developmental outcomes in the areas of physical health, cognitive development, attachment, and mental health. These were combined with the terms systematic review and meta-analysis. Where appropriate, Medical Subject Heading (MeSH) terms were used relating to adoption and human development as well as other relevant MeSH terms, which varied depending on the database. The search was conducted in July 2017. The following search string was used: ((looked after OR looked-after OR residential care) AND (child OR children)) OR (Institutionalize* OR institutionalise* OR Orphanage* OR Orphan OR “child in care” OR “children in care”) OR [Adoption Mesh term(s)] AND (delay OR cogn* OR IQ OR reading OR attainment OR education OR school OR ADHD OR inattention OR attention OR ASD OR autis* OR attach* OR growth OR weight OR height OR circumference OR health OR illness OR psych* OR behavio? r* OR emotion* OR self-esteem OR clinic OR disorder) OR [Human development Mesh term(s)] AND (“systematic review” OR meta-analysis).
Databases
The following 10 databases were searched: PsycINFO, Medline, Academic Search Complete, Excerpta Medica database (EMBASE), Sociological Abstracts, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Web of Science, Applied Social Sciences Index and Abstracts (ASSIA), Education Resource Information Centre (ERIC), and Cochrane Library.
Inclusion and Exclusion Criteria
Inclusion and exclusion criteria were used to identify high-quality systematic reviews and meta-analyses relevant to the research question. Papers were included if they reported systematic reviews and meta-analyses of longitudinal or cross-sectional controlled studies or single-group cohort primary studies of the effect of early institutional neglect or deprivation (without explicit reference to physical or sexual abuse) prior to adoption on physical health and growth, cognitive development, attachment, and mental health across the life span. For multiple publications of the same review, the one with the most complete data was included.
Systematic reviews and meta-analyses that did not meet three of the following four basic AMSTAR (Shea et al., 2009) systematic review quality criteria were excluded: (1) described an a priori design with a research question and inclusion criteria, (2) conducted a comprehensive literature search of at least two databases with appropriate search terms, (3) provided a table of characteristics of included studies (author, date, participant age and gender, type of maltreatment, and type of outcome), and (4) took the quality of studies into account in drawing conclusions. AMSTAR contains 11 criteria. A very high degree of confidence may be placed in conclusions from reviews and meta-analyses that meet all 11 criteria. The four basic AMSTAR criteria included in study selection criteria for the current review were chosen because conclusions from review papers and meta-analyses that do not meet these basic criteria have limited validity.
Narrative, integrative, nonsystematic reviews, discursive papers, theoretical papers, papers describing individual quantitative or qualitative studies (rather than reviews of multiple studies), editorials, and letters were excluded. Papers not published in peer-reviewed journals were also excluded.
Search Process
Records identified in electronic searches were downloaded to EndNote (http://endnote.com). Covidence (https://www.covidence.org/) was used for record screening, data extraction, and quality assessment. In addition to the electronic database search, a supplementary manual search was conducted. Bibliographies of review papers and tables of contents of relevant journals (Trauma, Violence, and Abuse, Child abuse and Neglect, Child Abuse Review, Child Maltreatment, Child Welfare, and Adoption and Fostering) were searched. Established researchers in the field were also contacted.
Figure 1 contains a PRISMA (Moher, Liberati, Tetzlaff, Altman, & The PRISMA Group, 2009) flow diagram of the search process. Through electronic and manual searches, 921 separate records were identified after duplicates were removed. When the titles and abstracts of these were screened, 48 relevant papers were downloaded for full-text screening. A final set of 18 papers, which met inclusion and exclusion criteria, were selected for review. The quality of these papers was assessed with AMSTAR (Shea et al., 2009).
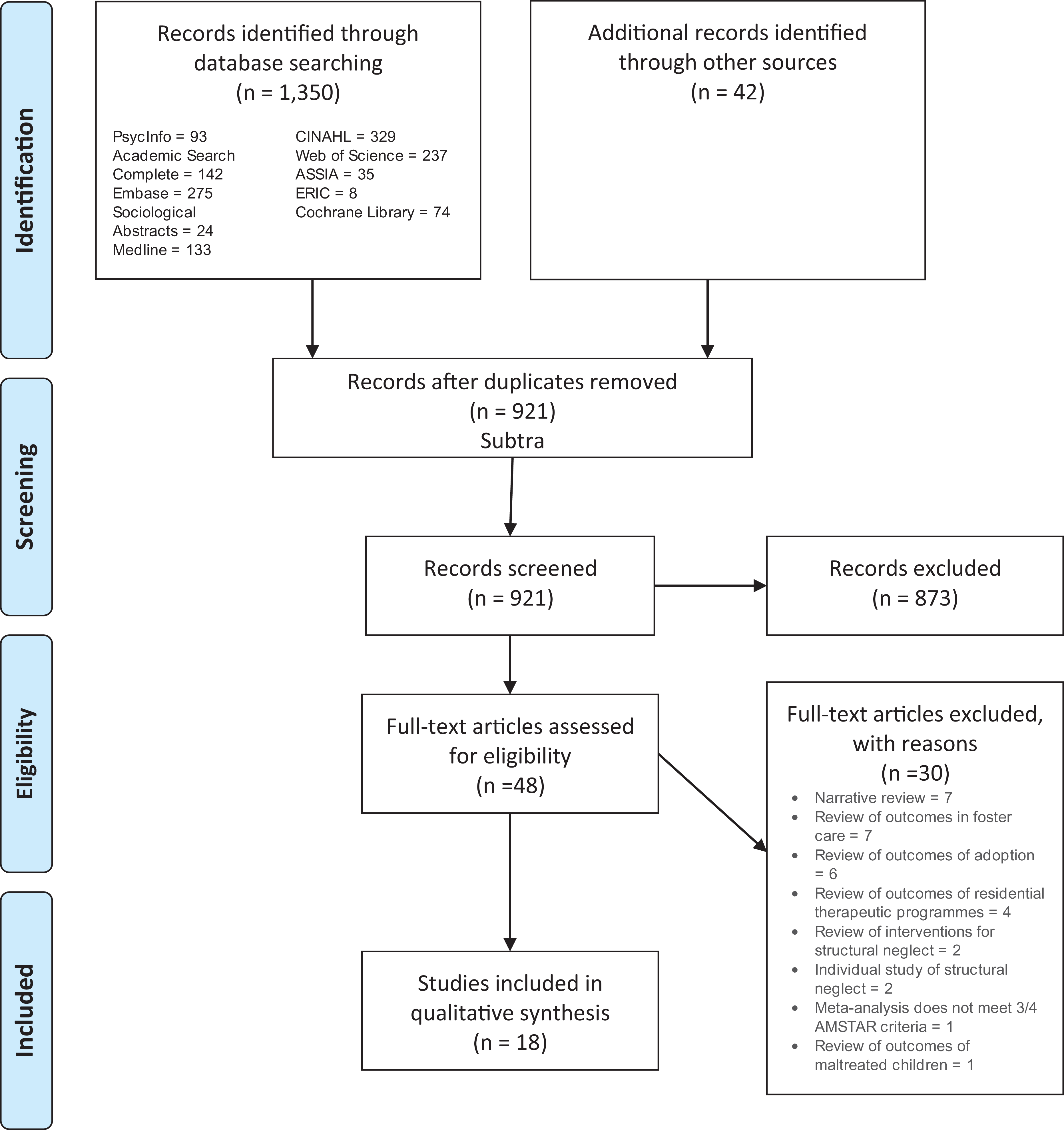
PRISMA flow diagram of literature search on outcomes of severe neglect.
Results
Interrater Agreement
Two research assistants were trained in using the systematic review protocol. Both research assistants independently conducted searches, study selection, data extraction, and study quality assessments. Disagreements were identified on the “resolve conflicts” page of Covidence, and these were resolved by discussion. Percentage agreement and Krippendorff’s α (Hayes & Krippendorff, 2007) were used to determine interrater agreement and reliability. For screening records and full-texts agreement, rates were 98% and 92%, respectively. For quality assessment agreement, rates ranged from 78% to 100% for AMSTAR items. There was 93% agreement for total AMSTAR scores and the Krippendorff’s α value was 0.86. For data extraction agreement, rates ranged from 67% to 100%, and the Krippendorff’s α values ranged from 0.88 to 1.00.
Study Sequence in Tables
Study quality ratings and data extracted from review papers were summarized in three tables. AMSTAR study quality scores are presented in Table 1. Study design features and sample characteristics are given in Table 2. Key findings are set out in Table 3. To aid synthesis of the large amount of information contained in 18 complex and comprehensive review papers, they have been grouped thematically in the same order within Tables 1–3. They have been grouped by the main type of outcome assessed (physical health, cognitive development, attachment, and mental health). It is noteworthy that in some studies which assessed cognitive development and mental health, multiple outcomes were assessed, as shown in the fourth column of Table 2. Within each group, papers have been sequenced, predominantly by the year of publication, although in some instances, sequences have been based on other features (such as author, specific outcomes assessed, where multiple outcomes were measured, or specific findings) to form a more coherent narrative.
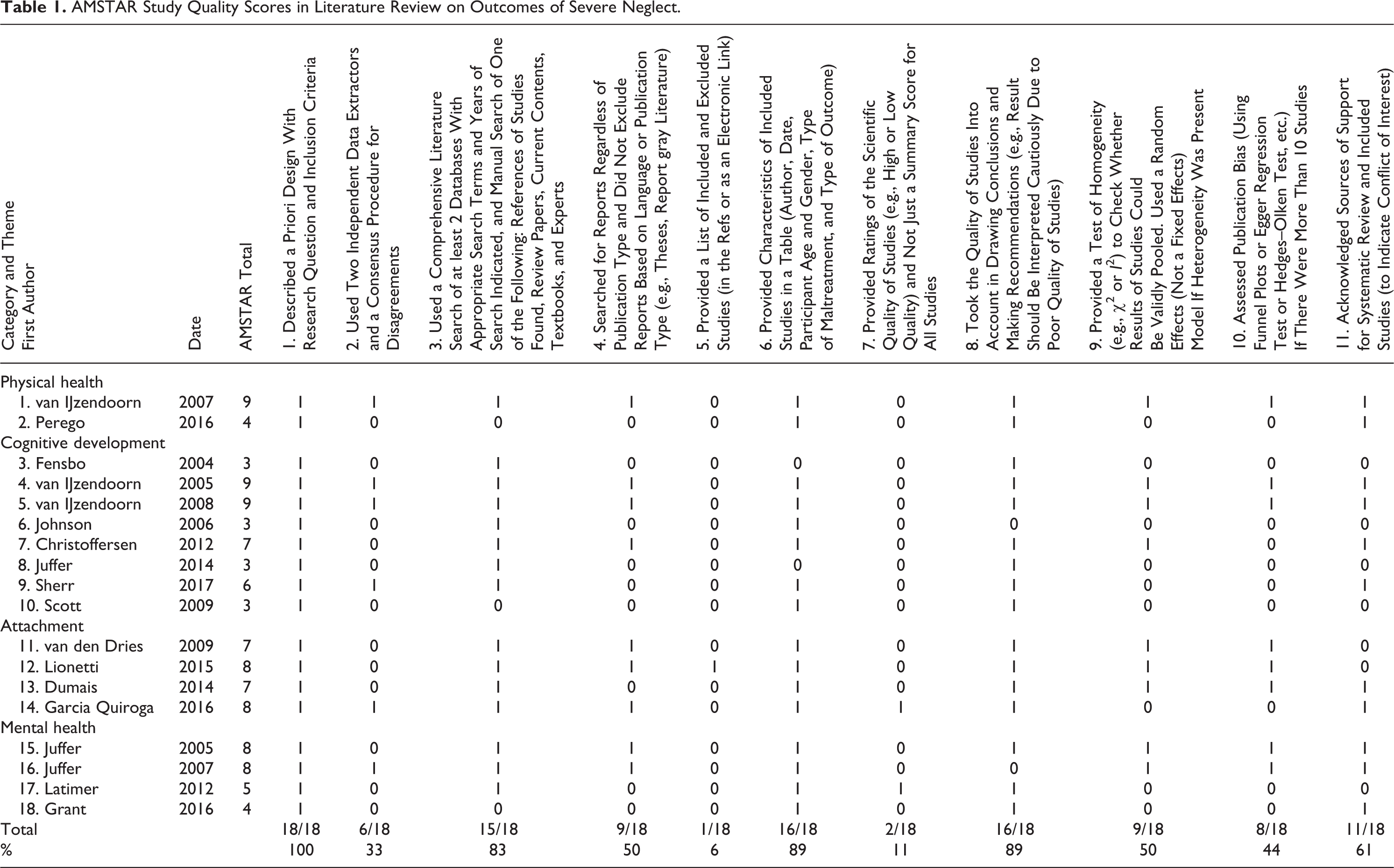
AMSTAR Study Quality Scores in Literature Review on Outcomes of Severe Neglect.
Study Design Features and Sample Characteristics in Literature Review on Outcomes of Severe Neglect.
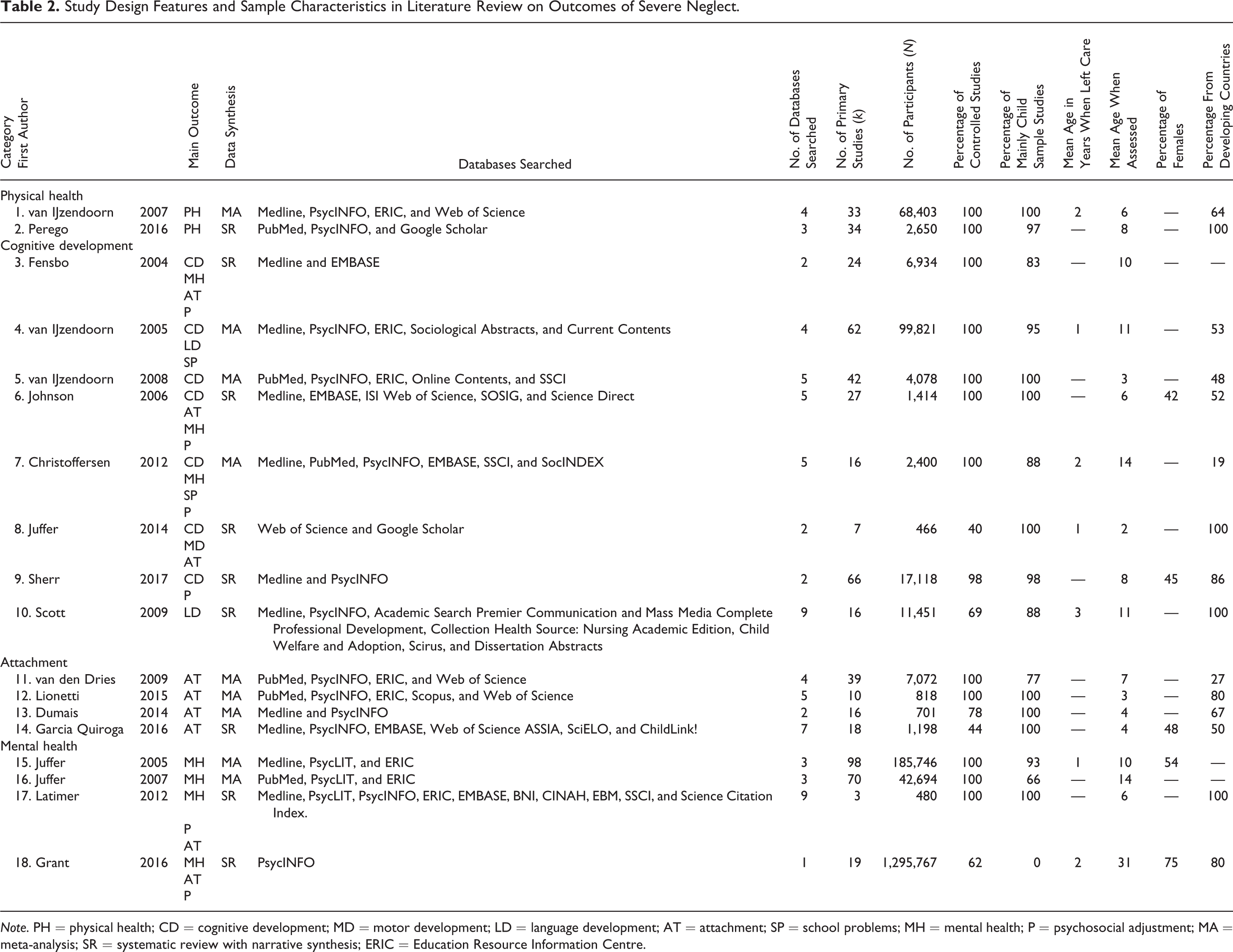
Note. PH = physical health; CD = cognitive development; MD = motor development; LD = language development; AT = attachment; SP = school problems; MH = mental health; P = psychosocial adjustment; MA = meta-analysis; SR = systematic review with narrative synthesis; ERIC = Education Resource Information Centre.
Key Findings from Literature Review on Outcomes of Severe Neglect.
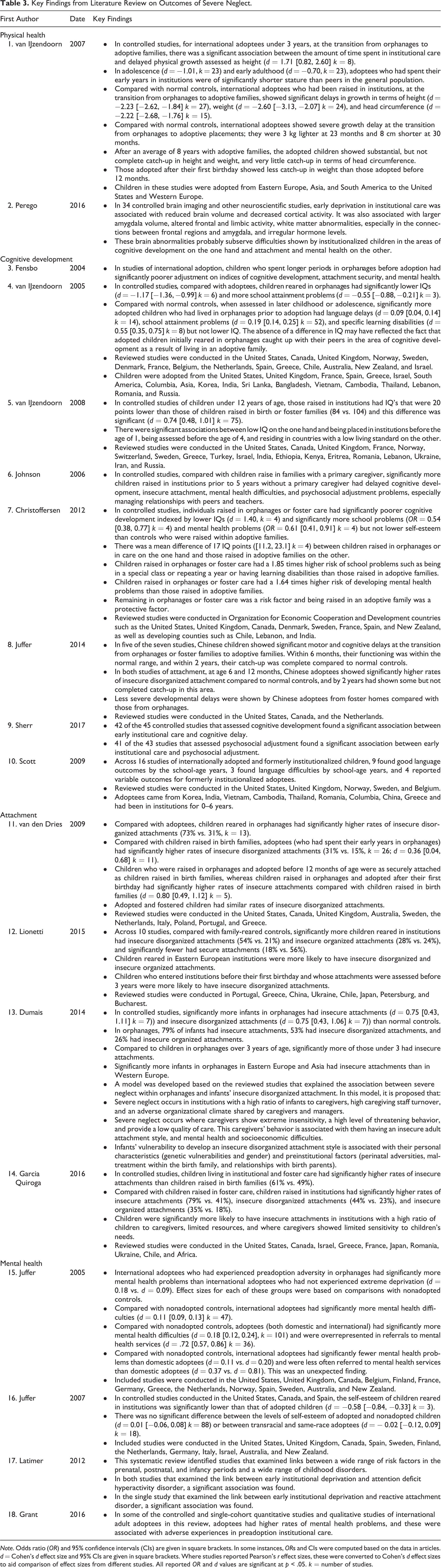
Note. Odds ratio (OR) and 95% confidence intervals (CIs) are given in square brackets. In some instances, ORs and CIs were computed based on the data in articles. d = Cohen’s d effect size and 95% CIs are given in square brackets. Where studies reported Pearson’s r effect sizes, these were converted to Cohen’s d effect sizes to aid comparison of effect sizes from different studies. All reported OR and d values are significant at p < .05. k = number of studies.
Study Quality
AMSTAR review quality scores are given in Table 1. Ten reviews and meta-analyses were of high quality, with AMSTAR scores between 7 and 11. Eight reviews had AMSTAR scores between 3 and 6 and were of moderate quality. Fewer than half included pairs of raters for record screening and data extraction, provided a list of excluded studies, provided individual quality ratings of primary studies, and assessed risk of bias. Half or more described an a priori design, used a comprehensive search strategy, searched the gray literature, tabulated study characteristics, took study quality into account when drawing conclusions, tested for study homogeneity, and took account of this in data analysis, and indicated conflicts of interests.
Study Design Features and Sample Characteristics
The 18 papers in the review were published between 2004 and 2017. Design features and sample characteristics are given in Table 2. Ten of the 18 papers focused on a single outcome. Two of these 10 focused on physical health outcomes, four on attachment, and four on mental health outcomes. The other eight were concerned with outcomes in the broad domain of cognitive development including IQ, school attainment problems, language delay, and specific learning disability. Four of these eight papers also addressed other outcomes including attachment and mental health. There were nine systematic reviews and nine meta-analyses. The number of databases searched in these studies ranged from one to nine with a mean of four. The most frequently searched databases were PsycINFO (n = 15) and PubMed/Medline (n = 15), followed by Web of Science (n = 9), Education Resources Information Centre (ERIC, n = 8), EMBASE (n = 5, PsycLIT (n = 3), Google Scholar (n = 2), and a number of databases, each of which were only searched in a single study. These included Applied Social Sciences Index and Abstracts, Academic Search Premier, British Nursing Index, Child Welfare and Adoption, ChildLink!,CINAHL, Communication and Mass Media Complete, Current Contents, Dissertation Abstracts, Evidence Based Medicine, Health Source: Nursing/Academic Edition, Online Contents, Professional Development Collection, Scientific Electronic Library Online, Science Citation Index, Science Direct, Scirus, Scopus, SocINDEX, Sociological Abstracts, and Social Science Information Gateway.
The number of studies (k) covered in papers included in this review ranged from 3 to 97 with a mean of 33. The total number of participants (N) within these review papers ranged from 466 to 1,295,767 with a mean of 97,178. Greater confidence may be placed in the validity of conclusions drawn from reviews where a larger proportion of studies involved strong research designs, especially controlled (rather than uncontrolled) studies. In the current review of 18 systematic reviews and meta-analyses, the proportion of controlled studies ranged from 40% to 100% with a mean of 88%.
Both children (under 18 years) and adults (over 18 years), and males and females were involved in studies covered in systematic reviews and meta-analyses reviewed in this article. The proportion of studies of mainly child samples ranged from 0% to 100% with a mean of 88%. The mean age of children in samples when they left care ranged from 1 to 3 years with an overall mean of 2 years. The mean age of participants when outcomes were assessed ranged from 2 to 31 with a mean of 9 years. The proportion of females in studies ranged from 42% to 75% with a mean of 53%. The proportion of studies in which participants were originally from developing countries in Easter Europe, Asia, Africa, and South America ranged from 19% to 100% with a mean of 68%.
Overlap in Primary Studies Included in Review Papers
There was overlap in the primary studies included in systematic review papers and meta-analyses selected for the current systematic review of review papers. In total, there were 451 independent studies reviewed in these 18 systematic review and meta-analyses. The percentage of review papers in which each primary study was included ranged from 6% to 28%. The percentage of all 451 independent studies included in each review paper ranged from 1% to 22%. In total, across all 451 independent studies, there were 1,749,211 participants. Of these, 169,204 had experienced severe neglect.
Outcomes for Individuals Who Experienced Severe Neglect
Key findings from 18 systematic reviews and meta-analyses on studies of the outcomes for individuals who experienced severe neglect are given in Table 3. Most participants in primary studies covered in these reviews were raised in poorly resourced orphanages and other institutions where they experienced severe neglect. In the section on Study Design Features and Sample Characteristics, it was noted that in these reviews, about two thirds (68%) of participants were originally from developing countries. Some reviews included studies of both domestic and international adoption, while others focused exclusively on the latter. In this context, domestic adoption refers to adoption from an institution to a family within a single country (e.g., the United Kingdom). International adoption, in contrast, refers to adoption from orphanages in developing countries into families in developed countries. International adoptees may have experienced greater severe neglect than domestic adoptees because orphanages in developing countries tend to be less well resourced than those in developing countries. In this context, developing countries refers to those in Eastern Europe, Asia, Africa, and South America. Developed countries refer to those in Europe and North America as well as in Australia and New Zealand.
Some participants in the primary studies in the reviews summarized in Table 3 were children exposed to severe neglect early in life and then adopted, while others were raised to adulthood in institutions. Reviews of controlled studies of adoptees provide information on the outcomes of severe neglect at the transition from institutional care to adoptive families compared with children raised in birth families. They also shed light on the degree to which these children catch-up with children raised in birth families over their time living in adoptive families. Controlled studies of individuals raised to adulthood in poorly resourced institutions indicate the outcomes of experiencing severe neglect throughout childhood and adolescence.
Physical Health
In the domain of physical health, one systematic review of physical growth delay in international adoptees who had been raised in orphanages care (van IJzendoorn, Bakermans-Kranenburg, & Juffer, 2007) and one meta-analysis of the neurobiological correlates of psychosocial deprivation in children (Perego, Caputi, & Ogliari, 2016) were identified.
van IJzendoorn, Bakermans-Kranenburg, and Juffer (2007) conducted a meta-analysis of 33 controlled studies of children adopted from poorly resourced orphanages in Eastern Europe, Asia, and South America to adoptive families in the United States and Western Europe. They concluded that compared with normal controls, international adoptees who had been raised in institutions showed significant delays in growth in terms of height, weight, and head circumference. At about 2 or 3 years of age, shortly after making the transition from orphanages to adoptive families, they were 3 kg lighter and 8 cm shorter than normal controls. In adolescence and early adulthood, adoptees who had spent their early years in institutions were of significantly shorter stature than peers in the general population. After an average of 8 years with adoptive families, adopted children showed substantial, but not complete catch-up in height and weight, and very little catch-up in terms of head circumference. Those adopted after their first birthday showed less catch-up in weight than those adopted before 12 months.
In 34 controlled brain imaging and other neuroscientific studies, Perego, Caputi, and Ogliari (2016) concluded that early deprivation in institutional care was associated with reduced brain volume and decreased cortical activity. It was also associated with larger amygdala volume, altered frontal and limbic activity, white matter abnormalities, especially in the connections between frontal regions and amygdala, and irregular hormone levels. They concluded that these brain abnormalities may subserve difficulties shown by institutionalized children in the areas of cognitive development on the one hand and attachment and mental health on the other.
Cognitive Development
Eight systematic reviews and meta-analyses of severe neglect and delayed cognitive development were identified (Christoffersen, 2012; Fensbo, 2004; Johnson, Browne, & Hamilton-Giachritsis, 2006; Juffer, Finet, Vermeer, & van den Dries, 2014; Scott, 2009; Sherr, Roberts, & Gandhi, 2017; van IJzendoorn, Juffer, & Poelhuis, 2005; van IJzendoorn, Luijk, & Juffer, 2008). In this context, delayed cognitive development was indexed by lower IQ, school attainment problems, specific learning difficulties, and language delay.
All seven reviews that investigated IQ found a significant association between this outcome and severe neglect (Christoffersen, 2012; Fensbo, 2004; Johnson et al., 2006; Juffer et al., 2014; Sherr et al., 2017; van IJzendoorn et al., 2005, 2008). For example, in meta-analyses by van IJzendoorn, Luijk, and Juffer (2008) and Christoffersen (2012), on average, the IQs of children raised in institutions were 17–20 IQ points lower than those of children raised in families. van IJzendoorn et al. (2008) found that lower IQs of children who had experienced severe neglect were associated with being placed in institutions before the age of 1 year, being assessed before the age of 4 years, and residing in developing countries with a low living standard. Adoptees who had experienced severe neglect in orphanages in their early life showed considerable catch-up during childhood following adoption, such that their IQs became similar to those of children raised in birth families and significantly higher than children who remained in orphanages (Christoffersen, 2012; Juffer et al., 2014; van IJzendoorn et al., 2005).
School attainment problems were investigated in two reviews, and in both of these, this outcome was associated with severe neglect (Christoffersen, 2012; van IJzendoorn et al., 2005). In the only review that investigated the issue, van IJzendoorn, Juffer, and Poelhuis (2005) found a significant association between severe neglect and specific learning difficulties.
Two reviews addressed developmental language delay. In a meta-analysis, van IJzendoorn et al. (2005) found a small but significant association between developmental language delay and severe neglect. However, in a systematic review, Scott (2009) reached no definitive conclusion on this issue. Across 16 primary studies of internationally adopted and formerly institutionalized children, nine found good language outcomes by school-age years, three found language difficulties by school-age years, and four reported variable outcomes for formerly institutionalized adoptees.
Attachment
Seven systematic reviews and meta-analyses of severe neglect and attachment were identified (Dumais, Cyr, & Michel, 2014; Fensbo, 2004; Garcia-Quiroga & Hamilton-Giachritsis, 2016; Johnson et al., 2006; Juffer et al., 2014; Lionetti, Pastore, & Barone, 2015; van den Dries, Juffer, van IJzendoorn, & Bakermans-Kranenburg, 2009), three of which also addressed outcomes in other areas including cognitive development and mental health (Fensbo, 2004; Johnson et al., 2006; Juffer et al., 2014). All of these reviews concluded that there was a significant association between severe neglect and insecure attachment, especially insecure disorganized attachment. Across four studies that provided sufficient aggregated data, 44–73% of survivors of institutional neglect had insecure disorganized attachments compared with 15–21% of children raised in birth families (Dumais et al., 2014; Garcia-Quiroga & Hamilton-Giachritsis, 2016; Lionetti et al., 2015; van den Dries et al., 2009). Insecure disorganized attachments were more common among young children (Dumais et al., 2014; Lionetti et al., 2015) who spent more than their first year of life experiencing severe neglect (Van den Dries et al., 2009) in institutions in developing rather than developed countries (Dumais et al., 2014; Lionetti et al., 2015), with a high ratio of children to caregivers, limited resources, and where caregivers showed limited sensitivity to children’s needs (Garcia Quiroga & Hamilton-giachritsis, 2016).
Mental Health
Six systematic reviews and meta-analyses of severe neglect and mental health were identified (Fensbo, 2004; Grant, Rushton, & Simmonds, 2016; Johnson et al., 2006; Juffer & van IJzendoorn, 2005, 2007; Latimer et al., 2012). Two of these also addressed outcomes in the areas of cognitive development and attachment (Fensbo, 2004; Johnson et al., 2006). All of these reviews concluded that there was a significant association between severe neglect in orphanages, in both developing and developed countries, and mental health problems. Juffer and van IJzendoorn (2005) found that adoptees, many of whom who had experienced severe neglect in orphanages, were overrepresented in referrals to mental health services. Latimer et al. (2012) found significant associations between severe neglect and two particular mental health problems: attention deficit hyperactivity disorder and reactive attachment disorder. Juffer and van IJzendoorn (2007) found that the self-esteem of children reared in institutions, many of which were characterized by severe neglect, was significantly lower than that of adopted children.
Conclusions
A summary of key findings from this review is given below along with implications for research policy and practice. While robust, these conclusions should be tempered by a consideration of the scientific quality of the studies on which they are based. Ten of the 18 (56%) reviews and meta-analyses in our review of reviews were of high quality, with AMSTAR scores between 7 and 11. Eight (44%) had AMSTAR scores between 3 and 6 and were of moderate quality. The primary studies included in systematic reviews and meta-analyses were predominantly controlled and relatively well designed, allowing confidence to be placed in their results.
Summary of Key Findings
The focus of this review was on outcomes of individuals who had experienced severe neglect during infancy and early childhood in poorly resourced institutions. There were significant associations between the experience of severe neglect in large congregate institutions such as orphanages and adjustment in the domains of physical health, cognitive development, attachment, and mental health. It is highly probable that severe neglect largely accounts for these adverse outcomes.
Physical health outcomes
Severe neglect was associated with short-stature, low-weight, and smaller head circumference. At about 2 or 3 years of age shortly after the transition from orphanages to adoptive families, children exposed to severe neglect were 3 kg lighter and 8 cm shorter than children raised in birth families. Severe neglect was also associated with abnormal neurobiological development affecting a range of brain structures and functions, implicated in cognitive and psychosocial difficulties. Children who had experienced severe neglect in orphanages and were placed in adoptive families showed a large degree of relatively rapid catch-up in weight and height but a lesser degree and slower rate of catch-up occurred in head circumference.
Cognitive development outcomes
Severe neglect was associated with delayed cognitive development as indexed by lower IQ, school attainment problems, specific learning disorders, and possibly by language delay. On average, the IQs of children raised in institutions were 17–20 IQ points lower than those of children raised in families. Children who had experienced severe neglect in orphanages and were placed in adoptive families showed a large degree of relatively rapid catch-up in IQ.
Attachment outcomes
Severe neglect was associated with insecure attachment, especially insecure disorganized attachment. Rates of disorganized attachment were about 3 times higher in survivors of institutional neglect compared with children raised in birth families. Disorganized attachment is a risk factor for later difficulties making and maintaining relationships across the life span. Children who had experienced severe neglect in orphanages and were placed in adoptive families showed long-term attachment insecurity, especially insecure disorganized attachment.
Mental Health outcomes
Severe neglect was associated with higher rates of mental health problems and mental health service usage.
Risk and protective factors
Significant, but incomplete, developmental catch-up occurred when children exposed to severe neglect were adopted. The degree and rate of catch-up depended on the outcome domain, the severity and duration of severe neglect, and the presence of a range of personal and contextual risk and protective factors. A large degree of relatively rapid catch-up occurred in weight, height, and IQ. A lesser degree and slower rate of catch-up occurred in head circumference and attachment security. Exposure to severe deprivation over longer time periods in understaffed, poorly resourced institutions in underdeveloped countries was a risk factor for poorer outcomes. Early adoption was a protective factor for better outcomes.
These conclusions are consistent with those of previous reviews of systematic reviews and meta-analyses (Juffer & van IJzendoorn, 2012; McCall & Groark, 2015).
Implications for Research, Policy, and Practice
Prevention policies should aim to eliminate large underresourced congregate care institutions for infants (Hamilton-Giachritsis & Browne, 2012). In taking steps toward this, policies should aim to adequately resource congregate care institutions to meet children’s developmental needs for a secure and adequately resourced living environment, nutrition, stimulation, and attachment to a stable primary caregiver with adequate parenting skills and training.
There are certain minimum standards essential for healthy child development. All children require a safe, secure, clean, and structurally robust residence that is not overcrowded. It should have adequate heat, light, sleeping, playing, feeding, washing, and sanitation facilities. All children require clean and appropriate bedding, clothing, and play equipment. They require a regular balanced diet appropriate to their developmental stage and access to regular health care. They require stable attachments to one or two skilled primary caregivers. This means that staffing in orphanages should be stable, and child/carer ratios should be low, for example, 1–4:1. This also means that institutional childcare staff require careful selection and training. On a daily basis, all children living in institutions require prolonged periods of interaction with their primary carers and with other children, and access to recreational and educational opportunities appropriate to their developmental stage.
Early placement in adoptive or foster families, with access to routine physical and mental health-care service available in developed countries, is the most viable effective intervention for child survivors of severe neglect in childcare institutions. Future studies in this area should assess the full range of outcomes considered in this article along with risk and protective factors. Study designs should include adopted and non-adopted survivors of severe neglect as well as normal controls, and cases should be followed up into adulthood.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was supported by funding from the Scottish Child Abuse Inquiry.