
Abstract
Enthusiasm for trauma-informed practice has increased dramatically. Organizational interventions that train staff about trauma-informed practice are frequently used to promote trauma-informed systems change, but evidence about these interventions’ effects has not been integrated. A systematic review was conducted of studies that evaluated the effects of organizational interventions that included a “trauma-informed” staff training component. A search was conducted in July 2017 and studies were identified in PubMed, PsycINFO, and the Published International Literature on Traumatic Stress database, limited to articles published in English after 2000. Six hundred and thirty-two articles were screened and 23 met inclusion criteria. Seventeen studies used a single group pretest/posttest design, five used a randomized controlled design, and one used a quasi-experimental design with a nonrandomized control group. The duration of trauma-informed trainings ranged from 1 hr to multiple days. Staff knowledge, attitudes, and behaviors related to trauma-informed practice improved significantly pre-/posttraining in 12 studies and 7 studies found that these improvements were retained at ≥1month follow-up. Eight studies assessed the effects of a trauma-informed organizational intervention on client outcomes, five of which found statistically significantly improvements. The strength of evidence about trauma-informed organization intervention effects is limited by an abundance of single group, pretest/posttest designs with short follow-up periods, unsophisticated analytic approaches, and inconsistent use of assessment instruments. In addition to addressing these methodological limitations, priorities for future research include understanding intervention effects on clients’ perceptions of care and the mechanisms through which changes in staff knowledge and attitudes about trauma-informed practice influence client outcomes.
Traumatic experiences have significant impacts on well-being and increase risk of many adverse outcomes—including physical and mental health problems (Felitti et al., 1998; Shonkoff et al., 2011), arrest and incarceration (Abram et al., 2004; Messina & Grella, 2006), academic difficulties (Stein et al., 2003), and homelessness (Hopper, Bassuk, & Olivet, 2010; Kim, Ford, Howard, & Bradford, 2010). In recognition of the high prevalence of trauma exposure among people served by public systems, the concept of trauma-informed practice emerged in the 1990s (Becker-Blease, 2017; Bloom, 2013; Harris & Fallot, 2001; Ko et al., 2008). Although there is no universal definition of trauma-informed practice (Branson, Baetz, Horwitz, & Hoagwood, 2017; Hanson & Lang, 2014; Marsac et al., 2016), the core tenets are reflected in the Substance Abuse and Mental Health Services Administration’s (SAMHSA) Four “Rs” of realizing the widespread impact of trauma, recognizing the signs and symptoms of trauma among clients and staff, responding by integrating knowledge about trauma into practice and policy, and proactively resisting retraumatization (SAMHSA, 2014).
Enthusiasm for trauma-informed practice has grown dramatically in recent years (Becker-Blease, 2017). While trauma-informed practice initially gained traction in mental health, substance abuse, and child welfare service sectors, calls for trauma-informed practice have been made across increasingly diverse fields—such as social policy (Bowen & Murshid, 2016), intellectual disabilities (Keesler, 2014), dentistry (Raja et al., 2015), obesity prevention (Mason et al., 2016), and children’s sports (D’Andrea, Bergholz, Fortunato, & Spinazzola, 2013). U.S. cities (e.g., San Francisco, CA [SAMHSA, 2017], Philadelphia, PA [Beidas et al., 2016]) and states (e.g., Washington [Kagi & Regala, 2012]) have made commitments to integrating trauma-informed practice into their public service systems. Trauma-informed practice is also gaining traction in U.S. Congress. In 2015, 28 bills were introduced with an explicit purpose to promote trauma-informed practice (Purtle & Lewis, 2017) and similar bills are currently being considered in the 115th Congress (e.g., the Trauma-Informed Care for Children and Families Act of 2017, H.R.1757, S.774; A Resolution Recognizing the Importance and Effectiveness of Trauma-Informed Care, S.Res.346, H.Res.443). Trauma-informed practice is also receiving increasing attention in the peer-reviewed literature. The number of journal articles published annually that mentioned “trauma-informed” in the title, abstract, or key words has increased from 7 in 2010, to 127 in 2016 (Figure 1).
New articles in PubMed, PsycINFO, and PILOTS mentioning “trauma-informed” or “trauma-informed” in the title, abstract, or key words by publication year (N = 528).
The Importance of Trauma-Informed Trainings
Enthusiasm for trauma-informed practice reflects growing consensus about the reasons why trauma-informed approaches should be embraced, but less is known about how to create trauma-informed organizational and systems change (Hanson & Lang, 2014). Staff training about trauma-informed practice is often the first step an organization takes when it commits to becoming trauma
Study Aims
Staff trainings about trauma-informed practice are potentially instrumental to fostering trauma-informed organizational and systems change, but evidence about the effects of these trainings has not been assessed or integrated. The purpose of this review was to begin to address this knowledge gap. A systematic review was conducted of peer-reviewed studies that evaluated the effects of trauma-informed organizational interventions that included a staff training component. The study aims were to: describe the characteristics of studies that have evaluated the effects of trauma-informed organizational interventions that include staff trainings; synthesize evidence about the effects of trauma-informed organizational interventions that include staff trainings on staff and client outcomes; and identify areas for future research about the effects of trauma-informed organizational interventions that include staff trainings.
Scope and Limitations
This review was narrow in scope and its results should be interpreted within the context of its parameters. First, the review was limited to trauma-informed interventions at the organizational level-that included a staff training component. The review did not include evaluations of interventions focused on programing (e.g., trauma-informed yoga), direct services (e.g., trauma-informed case management), or clinical care (e.g., trauma-specific treatments). Second, the review was limited to the peer-reviewed outcome evaluations and did not capture practice-based evidence that is unpublished or published in nonpeer-reviewed venues (e.g., online reports).
Third, perhaps most importantly, the review was limited to organizational interventions that were explicitly trauma-informed. The rationale for limiting the review to organizational interventions that are explicitly trauma-informed reflects the fact that a single definition of trauma-informed, or the elements that it encompasses, does not exist (Branson et al., 2017; Hanson & Lang, 2014; Marsac et al., 2016). As Hanson and Lang (2014) describe trauma-informed practice “is an amorphous concept that has been defined in a number of ways, making it difficult to evaluate [trauma-informed] initiatives” (p. 96). The use of specific language to classify interventions as trauma-informed allows for systematic and replicable methods to be applied to evaluate the body of evidence, but with the limitation of excluding interventions that embrace principles of trauma-informed practice without using language of trauma-informed.
Method
Article Identification
On July 28, 2017, PubMed, PsycINFO, and the Published International Literature on Traumatic Stress database were searched for all articles that mentioned trauma-informed or “trauma-informed” in title, abstract, or key words. After removing duplicates, this resulted in 632 articles.
Article Screening
The abstracts of all articles were screened for inclusion and classified into one of the three mutually exclusive categories: (1) empiric study, outcome evaluation (e.g., a randomized controlled trial of an intervention that claimed to be trauma-informed); (2) empiric study, not outcome evaluation (e.g., epidemiologic studies that recommend trauma-informed practice based on findings); and (3) nonempiric (e.g., commentaries about the need for trauma-informed practice).
Article Full-Text Review and Data Extraction
Ninety-six articles were classified as empiric outcome evaluations. The full texts of these articles were obtained and reviewed to identify evaluations of organizational-level interventions that included a trauma-informed training. Articles were excluded if they met any of the following criteria: evaluations of trauma-informed program/clinical interventions (e.g., trauma-informed parenting interventions, interventions aimed at integrating trauma-specific treatments into primary care); exclusively qualitative evaluations; single-group, posttest only evaluations; and nonempiric descriptions of implementation processes.
Twenty-three articles met inclusion criteria. Figure 2 shows the screening and review process. Information on the following characteristics of each study was extracted from the articles: study design, sample size, population and organizational setting, follow-up period, intervention components, outcomes and measures, main findings, and limitations.
Flow diagram to identify studies evaluating of trauma-informed organizational interventions that include staff training.
Results
Characteristics of Trauma-Informed Organizational Interventions and Evaluation Designs
Table 1 presents information extracted from the 23 studies. The majority of evaluations (17 studies) used a single group, pretest/posttest design, five used a randomized controlled design, and one used a quasi-experimental design that had an intervention group and a nonrandomized control group. The interventions targeted a range of sectors, with six being implemented in child welfare agencies, six in psychiatric hospitals, four in general medical settings (e.g., emergency departments, primary care clinics), one in a juvenile justice facility, and one in a school.
Outcome Evaluations of Trauma-Informed Organizational Interventions That Include Staff Training.
Note. N = 23 studies. SAMHSA = Substance Abuse and Mental Health Services Administration.
The trauma-informed training curricula most frequently used were Risking Connection (four studies) and the National Child Traumatic Stress Network’s trauma-informed training (three studies). In most studies, no specific training curriculum was identified and the training was developed in-house by the evaluators. There was substantial variation in the amount of information provided about the content of the trainings and their didactic approach. Some articles provided meticulous detail about the theory behind the training approach and the process used to develop the content, while other articles provided limited information. Common elements of the trainings included information about the psychological and physiological effects of trauma, strategies to avoid retraumatizing clients and cultivate feelings of safety, tools to develop of a “common language” about trauma, and strategies to prevent vicarious trauma and improve self-care among staff. The duration of the trauma-informed trainings varied dramatically, ranging from only 1 or 2 hr (three studies) to multiple days (five studies).
Six interventions had at least one additional, nontraining component aimed at fostering trauma-informed organizational change. Examples of these intervention components include internal steering committees to guide trauma-informed change, policies that require an administrative review to be conducted each time a potentially retraumatizing incident occurs (e.g., seclusion and restraint, violence against staff), checklists to encourage trauma-informed practice, changes to features of the physical environment, ongoing consultation and technical assistance about trauma-informed practice, and wellness programs to improve staff self-care.
Staff knowledge, attitudes, and behaviors related to trauma-informed practice were assessed as outcomes in the majority of evaluations (14 studies). These outcomes were measured using a variety of self-report instruments, ranging from single-item instruments to the 90-Item Trauma System Readiness Tool (Hendricks, Conradi, & Wilson, 2011). The same instrument was not used in any two studies to assess the effect of a trauma-informed training on staff knowledge, attitudes, or behaviors. Seven studies used administrative data (e.g., hospital discharge data, disciplinary action records, and routine quality improve surveys) to assess the organizational intervention’s effects on client outcomes. Only two studies collected data from clients to assess intervention effects on their perceptions of the organization’s staff and the extent to which the organization was trauma-informed (Borckardt et al., 2011; Green et al., 2016).
Effects of Trauma-Informed Organizational Interventions on Staff Outcomes
Of the 14 studies that assessed the effects of a trauma-informed organizational intervention on staff knowledge, attitudes, or behaviors, 12 found a statistically significant improvement in one or more of these outcomes pre-/posttraining. The effect sizes were typically about one standard deviation (SD) in magnitude. Trainings with shorter durations generally had smaller effect sizes than trainings with longer durations. For example, Choi and colleagues’ (2015) evaluation of a 1-hr trauma-informed training on perinatal health-care providers’ knowledge and attitudes about trauma-informed practice found pre-/postchanges that were statistically significant but only about half of a SD in magnitude.
Only one study was designed to determine the effect of a trauma-informed training on staff attitudes independent of other, nontraining intervention components. Borckardt and colleagues (2011) used a cluster-randomized design in which each unit of a pediatric psychiatric hospital received trauma-informed organization intervention components in a different order, allowing for the effect of each component to be assessed independently. The study found that the trauma-informed training, in isolation, did not significantly change staff attitudes about their own “trauma sensitivity” and that the training was not significantly associated with a reduction in seclusion and restraint events that was observed.
Administrative data were used to assess intervention effects on staff outcomes in two evaluations, both of which used these data to assess staff safety. For example, an evaluation of a 5-day training in the sanctuary model and ongoing technical assistance in trauma-informed practice at a juvenile justice facility found that assaults on staff reduced by 1.13 per 100 staff days (p < .01) between the preintervention period and 2 years postintervention (Elwyn, Esaki, & Smith, 2015). During this same time period, the national rate of assaults on staff at juvenile justice facilities increased significantly. No studies assessed the effects of trauma-informed organizational interventions on staff turnover.
Persistence of the Effects of Trauma-Informed Organizational Interventions on Staff Outcomes Over Time
Of the 14 studies that evaluated the effect of trauma-informed trainings on staff knowledge, attitudes, or behaviors, nine assessed these outcomes at ≥1 month after the training occurred. Seven of these studies found that significant improvements were retained. For example, knowledge about trauma-informed practice among child welfare agency staff increased from a mean score of 10.8 (SD = 2.17) prior to a half day trauma-informed training to 12.7 (SD = 2.02) immediately after the training and 12.4 (SD = 2.02, p < .05) at 12-month follow-up (Kenny, Vazquez, Long, & Thompson, 2017).
Three studies found that changes in trauma-informed behaviors were retained at ≥1-month follow-up. For example, among child welfare agency directors who participated in a 2-day trauma-informed training, self-reported use of trauma-informed practices increased significantly immediately after the training and these increases were retained at 3 months follow-up (p < .001; Kramer, Sigel, Conners-Burrow, Savary, & Tempel, 2013). A randomized controlled trial of a 1-day trauma training for substance abuse treatment providers found that self-reported frequency of trauma screening increased significantly between pretraining and 3 and 6 months follow-up (p < .001; Lotzin et al., 2017).
Effects of Trauma-Informed Organizational Interventions on Client Outcomes
Eight studies assessed the effects of a trauma-informed organizational intervention on client outcomes, five of which found a statistically significant improvement for one or more outcomes (significance testing was not conducted in two of these studies). Six of the eight studies used administrative data to assess these outcomes. For example, an evaluation of the Healthy Environments and Response to Trauma in Schools intervention—which included a school-wide trauma training, ongoing consultation about trauma-informed practice, and the provision of trauma-specific treatment in schools—found that disciplinary office referrals decreased by 32% between pre- and 1-year postintervention and deceased by 87% 5 years postintervention (Dorado, Martinez, McArthur, & Leibovitz, 2016). Blair and colleagues (2017) found that the incidence of seclusions at a psychiatric hospital was cut in half (9.2 per 100 admissions vs. 4.4 per 100 admissions, p < .01) 2 years after an intervention that included a 2-day Risking Connection trauma training, administrative reviews for all seclusion and restraints events, and routine use of checklists to minimize seclusion and restraint.
Two studies assessed the effect of staff trauma-informed trainings on patients’ perceptions of care. In one randomized controlled trial, Green and colleagues (2016) assessed the impact of a 6-hr trauma-informed training for primary care physicians on their patients’ perceptions of patient–provider rapport, communication, and shared decision-making. The evaluation found that the training significantly improved patient perceptions of shared decision-making (p < .01), but not patient–provider rapport or communication. Borckardt and colleagues’ (2011) cluster-randomized controlled trial of a trauma-informed organizational intervention at a psychiatric hospital did not find that the intervention significantly improved patients’ perceptions of the staff’s trauma sensitivity.
Limitations of Evaluations of Trauma-Informed Organizational Interventions
There were serious limitations related to study design, measurement, and analysis in many of the evaluations. In 12 of the studies, staff knowledge, attitudes, and/or behaviors were assessed using questionnaires that were developed by the intervention developers for the purpose of the evaluation. This introduces the risk of a “teaching to the test” effect in which the training heavily emphasizes specific content that is assessed by survey items. In seven studies, posttests were only administered immediately after the training—providing no indication of whether changes in knowledge or attitudes were retained for an amount of time meaningfully enough to impact staff or client outcomes. Although nine studies assessed changes in staff knowledge, attitudes, or behaviors at ≥1-month follow-up, pretest/posttest retention rates varied dramatically. For example, Bartlett and colleagues (2016) achieved 80.5% retention at 1-year follow-up, while Kenny and colleagues (2017) only achieved 12% retention at 1-year follow-up. High loss-to-follow-up rates increase the risk of attrition bias because it is plausible that participants who completed posttests had more favorable perceptions of, and gained more from, the training than participants who did not complete posttests. Studies that assessed outcomes at ≥1-month follow-up were limited by the absence of a control group that did not participate in the training. Without a control group, it is unclear whether changes in outcomes ≥1 month after the training are the result of exposure to the training or exposure to information about trauma-informed practice from obtained from other different sources.
In nine studies, multiple trauma-informed organizational intervention components were implemented at the same time as the trauma-informed training. This limits the ability of studies to determine the extent to which outcomes are attributable to the training as opposed to other intervention components. Of the six studies that used administrative data to assess the effects of interventions on client outcomes, four presented outcome data in the form of counts, not rates (e.g., number of incidents per 100 patient days). Thus, it is unclear whether changes in outcomes are attributable to the training or temporal changes in facility census. Finally, unsophisticated analytic techniques were used to evaluate intervention effects in many of the studies. Three of the studies did not conduct statistical significance testing and only 6 of the 23 studies conducted statistical adjustment (e.g., used multivariate regression) to assess intervention effects while controlling for potentially confounding variables. In four studies, differences in pre-/posttraining means were only reported for individual survey items and aggregate differences in pre-/postmeans were not presented.
Discussion
Trauma-informed organizational interventions that include staff trainings have been the focus of at least 23 empirical outcome evaluations published in the peer-reviewed literature. The strength of this body of evidence is limited by an abundance of single group, pretest/posttest designs with short follow-up periods, inconsistent use of assessment instruments to ascertain outcomes, and unsophisticated analytic approaches. Nevertheless, some well-designed and analytically rigorous evaluations of trauma-informed organizational interventions that include staff trainings have been conducted and demonstrate positive effects. Overall, the review indicates that staff knowledge, attitudes, and behaviors related to trauma-informed practice improve after participating in a trauma-informed training. It is less clear, however, the extent to which staff changes in knowledge, attitudes, and behaviors related to trauma-informed practice are retained over time and translate into client outcomes. Trauma-informed organizational interventions appear to have the most meaningful impacts on client outcomes when the intervention includes other components (e.g., policy changes) in addition to trauma-informed trainings for staff (Table 2).
Summary of Key Findings.
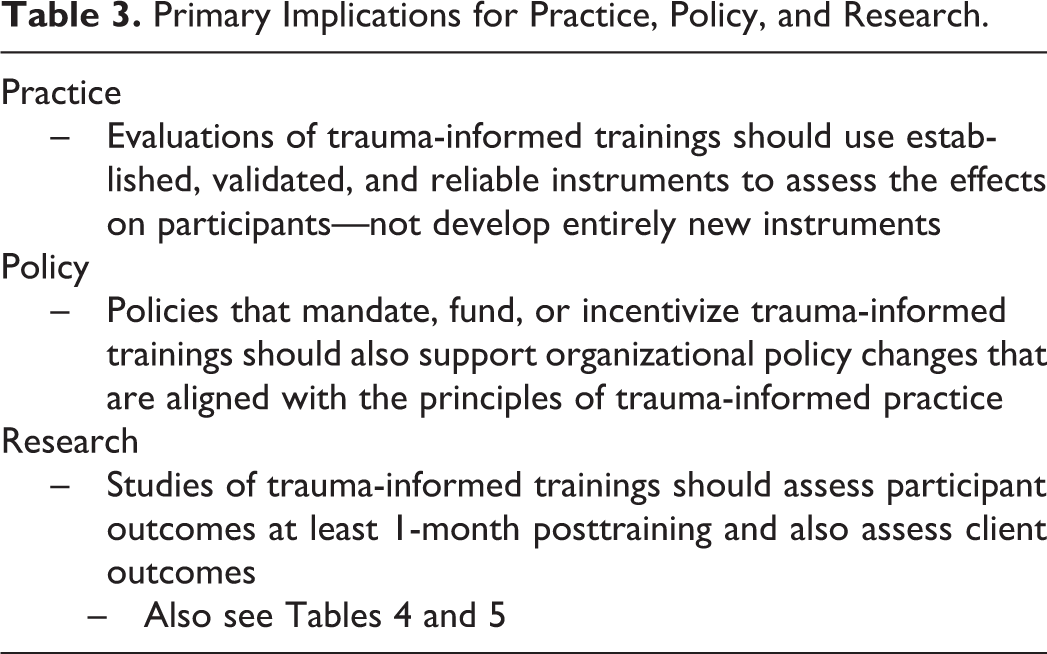
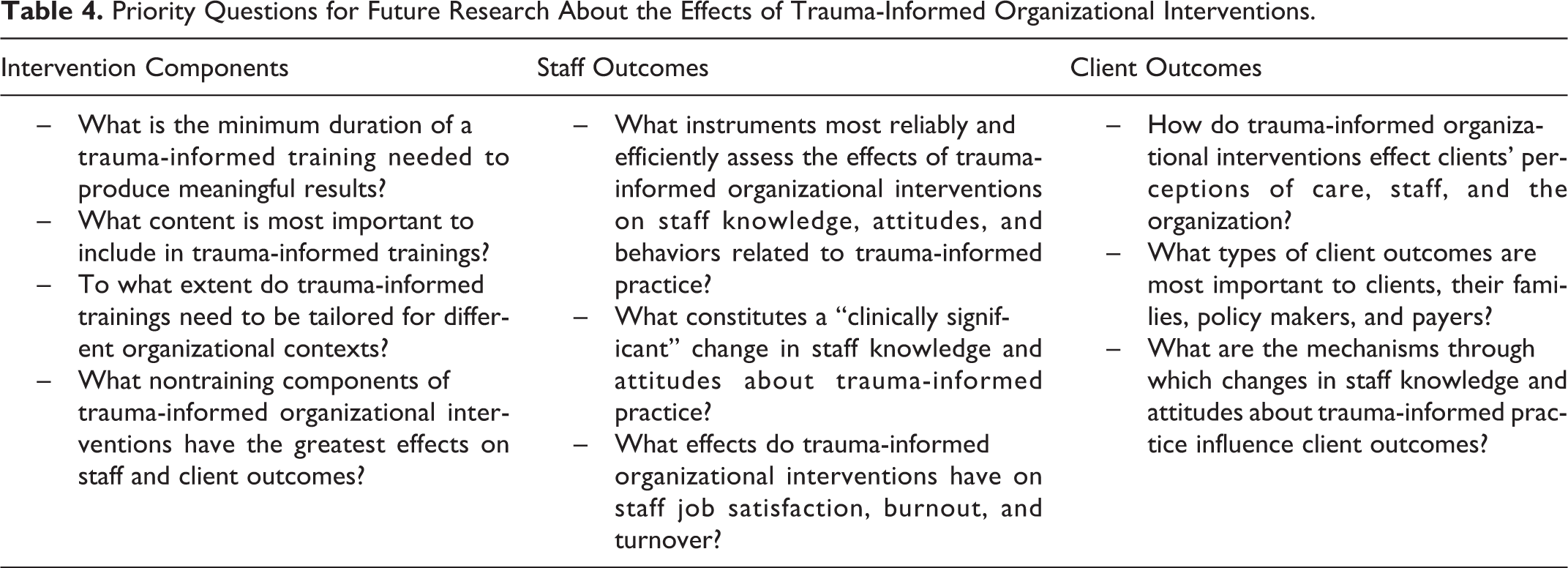
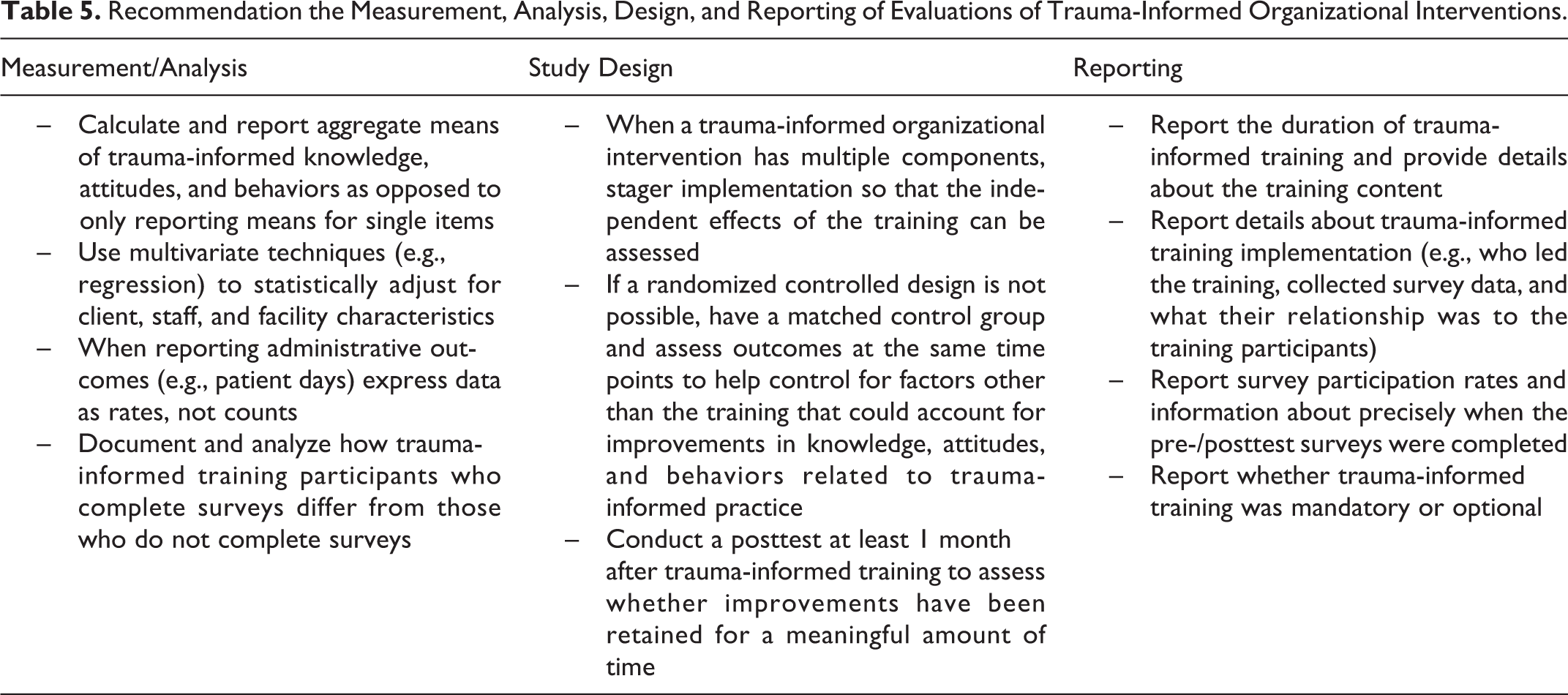
Informed by the results of the review, Table 3 summarizes primary implications for practice, policy, and research. Table 4 specifies priority questions for future research about the effects trauma-informed organizational interventions and trainings. Table 5 summarizes recommendations for measurement, analysis, study design, and reporting in the evaluation of trauma-informed organizational interventions that include staff trainings.
Primary Implications for Practice, Policy, and Research.
Priority Questions for Future Research About the Effects of Trauma-Informed Organizational Interventions.
Recommendation the Measurement, Analysis, Design, and Reporting of Evaluations of Trauma-Informed Organizational Interventions.
Future Research Related to Intervention Components
The duration of the trauma-informed trainings varied dramatically, ranging for 1 hr to 5 days. A question for future research relates to the minimum “dose” of trauma-informed training needed to produce meaningful changes in staff and client outcomes. There was also substantial variation in the content of the trauma-informed trainings. This raises questions about what types of content (e.g., information about the biology of trauma, information about specific trauma-informed practices) are most important and the extent to which the content from existing trauma-informed trainings (e.g., Risking Connection) should be tailored for different organizational contexts. Lastly, only one study was designed to assess the effects of a trauma-informed training independent of other components of the organizational intervention (Borckardt et al., 2011). SAMHSA’s (2014) Treatment Improvement Protocol for Trauma-Informed Care enumerates 16 nontraining components that could be integrated into trauma-informed organizational interventions (e.g., create a trauma-informed oversight committee, change the physical environment) and future research should assess the effects of such components independent of, and in combination with, trauma-informed trainings.
Future Research Related to Staff Outcomes
Staff outcomes were measured in a variety of ways. A different instrument was used in each evaluation to assess the effect of trauma-informed trainings on staff knowledge, attitudes, or behaviors. In most instances, the instrument was developed by the same people who developed the intervention and the instrument’s validity and reliability was not assessed. Many valid and reliable instruments for measuring trauma-informed organizational interventions have recently been developed (e.g., the Trauma-Informed Medical Care Questionnaire, Weiss et al., 2017; Trauma System Readiness Tool, Hendricks et al., 2011; Trauma-Informed System Change Instrument, Richardson, Coryn, Henry, Black-Pond, & Unrau, 2012; Attitudes Related to Trauma-Informed Care Scale, Baker, Brown, Wilcox, Overstreet, & Arora, 2016; Trauma-Informed Practices Scale, Goodman et al., 2016; and the “TICOMETER,” Bassuk, Unick, Paquette, & Richard, 2017), and future research should examine which instruments most efficiently assess the effects of trauma-informed organizational interventions. More standardized use of instruments would also allow for the results of different trauma-informed organizational interventions to be compared. This would also enable the results of multiple evaluations to be pooled together and help establish what constitutes a “clinically significant” change in staff knowledge, attitudes, and behaviors related to trauma-informed practice. Beyond assessment staff knowledge, attitudes, and behaviors, future research should examine the effects of trauma-informed organizational interventions on staff outcomes such as job satisfaction, burnout, and turnover. None of the evaluations included in the review assessed these outcomes.
Future Research Related to Client Outcomes
Evidence about the impacts of trauma-informed organizational interventions on client outcomes is less developed than it is for staff outcomes. Although six studies used administrative data to assess client outcomes, only two examined the effect of a trauma-informed organizational intervention on clients’ perceptions of care. This represents an important area for future research given the person-centered orientation of trauma-informed practice. Formative research is also needed to identify the types of client outcomes that are most important to clients, their families, policy makers, and payers, and other system leaders. The scale-up and sustainability of trauma-informed organizational interventions will likely be influenced by the extent to which they achieve outcomes that are important to policy makers and payers. Lastly, research is needed about the mechanisms through which staff knowledge, attitudes, and behaviors related to trauma-informed practice impact client outcomes. This information can inform the design and enhance the effectiveness of trauma-informed staff trainings.
Conclusions
Organizational interventions that train staff about trauma-informed practice appear to improve staff knowledge, attitudes, and behaviors for some period of time. It is less clear, however, extent to which staff trainings, independent of other components of trauma-informed organizational interventions, translate into meaningful outcomes for the clients the organizations serve. Use of more rigorous evaluation designs, sophisticated analytic techniques, and valid and reliable assessment instruments would substantially improve the evidence base for trauma-informed organizational interventions and help ensure that their effects on staff and client well-being are maximized.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Robert Wood Johnson Foundation (74672) and National Institute of Mental Health (R25MH080916).