
Abstract
Studies investigating rates of acute stress disorder following exposure to a traumatic event report widely varying results, even when examining the same types of traumatic events. The first purpose of this systematic review and meta-analysis was to describe rates of acute stress disorder following five different types of traumatic events. The second goal was to assess the methodological and trauma-related factors influencing these rates. Between May 2017 and October 2019, studies were identified by searching through the PsychINFO, PubMed/Medline, OVID, CINAHL, Scopus, and PILOTS databases. Records were included if (1) participants were 16 years old and over, (2) the assessment was completed within 30 days of the event, (3) a standardized assessment instrument was utilized, (4) the type of traumatic event was specified, and (5) the acute stress disorder rate was reported. The list of traumatic events used for the search strategy was based on the Diagnostic and Statistical Manual of Mental Disorders and was complemented by those listed in the Life Events Checklist and the National Comorbidity Survey Replication. Seventy-three samples from 70 studies totaling 20,065 participants met inclusion criteria. Results revealed that rates of acute stress disorder ranged from 14.1% for war-related trauma to 36.0% for interpersonal trauma. Interpersonal trauma was significantly more likely to lead to acute stress disorder than other types of events, except for disaster-related trauma. Differing assessment instruments, types of exposure and geographical locations, and the intentional nature of certain events contributed to heterogeneity in rates within each type of traumatic event.
Experiencing a traumatic event is very common, with lifetime self-reported exposure rates estimated at 70.4% worldwide and up to 89.7% in the United States (Benjet et al., 2016; Liu et al., 2017; Neria et al., 2008). Multiple incidents across the lifespan appear to be the norm rather than the exception (Kilpatrick et al., 2013). These elevated rates of exposure are problematic, as affected individuals may develop traumatic stress reactions such as acute stress disorder (ASD) and post-traumatic stress disorder (PTSD). Traumatic events that can lead to ASD and PTSD are defined in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5, 5th ed.) as exposure to actual or threatened serious injury, sexual violence, or death (American Psychiatric Association [APA], 2013). Exposure may occur through direct victimization, witnessing the event, learning that a relative or a close friend experienced the event, or indirect exposure to aversive details of the event in the course of professional duties (APA, 2013). These traumatic events include, but are not limited to, natural or man-made disasters, war, interpersonal violence, life-threatening illnesses, and severe accidents (APA, 2013; McCall-Hosenfeld et al., 2014; Weathers et al., 2013). Although ASD and PTSD list similar symptoms, important differences distinguish the two. ASD is often used to facilitate access to treatment in the immediate aftermath of a traumatic event since its diagnosis is limited to the acute phase (3–30 days; APA, 2013; Bryant, 2016). In contrast, PTSD can only be diagnosed if symptoms persist past the initial 30 days. PTSD and ASD symptoms include reexperiencing the traumatic event (e.g., flashbacks), avoidance (e.g., repressing thoughts, avoiding places), and increased arousal (e.g., being startled; APA, 2013; Bryant, 2016). Dissociative symptoms, such as personalization and derealization, are also typical of ASD but not PTSD (i.e., except for the dissociative subtype of PTSD—APA, 2013; Bryant, 2016). PTSD symptoms can also include non-fear-related symptoms such as distorted negative thoughts that worsen after trauma (e.g., seeing isolated) or destructive behaviors (APA, 2013). Unlike PTSD, ASD symptoms are not classified within clusters, patients must simply fulfill at least 9 of the 14 criteria to receive a diagnosis (APA, 2013; Bryant, 2016). In contrast, a PTSD diagnosis is contingent on the presence of a minimum of symptoms across all four clusters: meaning one or more reexperiencing symptoms, one or more avoidance symptoms, two or more arousal or reactivity symptoms, and two or more cognition or mood symptoms (APA, 2013).
Issues in Assessing the Rates of ASD
According to the DSM-5 (APA, 2013), traumatic events that do not involve interpersonal assault lead to ASD in fewer than 20% of cases. Events with interpersonal assault, on the other hand, are reported to lead to higher rates of ASD (i.e., 20%–50%) due to the intentional nature of the incident. Meanwhile, the empirical literature on ASD yields widely varying rates, even within the same categories of traumatic events. For example, some studies report significantly elevated rates of ASD following motor vehicle accidents (41%–46%; King, 2007; Suliman et al., 2013), whereas others describe relatively low percentages (5%; Winston et al., 2005). Although it is expected for ASD rates to vary from one type of traumatic event to another, it is unusual that rates reported within the same category of trauma are so conflicting. Methodological differences between studies may account for these variations. First, some studies combine multiple types of events when reporting ASD rates, making it difficult to accurately examine the rates for each distinct category of trauma (Marchand et al., 2015; Mokrue et al., 2011; Ouanes et al., 2014). Second, various measures of ASD symptomatology are used across the literature and possibly yield differing rates. Third, the time frame during which ASD is assessed varies considerably, with a few studies even reporting ASD rates while the traumatic event is still ongoing (Cohen, 2008; Cohen & Yahav, 2008; Yahav & Cohen, 2007). Indeed, measuring ASD in the midst of an ongoing traumatic event poses methodological challenges. For example, if researchers can assess ASD in parents less than 30 days after learning of their child’s life-threatening diagnosis, the same cannot be said for measuring ASD during military conflicts. In such a context, for example, survivors may have been living in fear and suspecting the death of their loved ones months before they actually witness the impact of war first hand. Fourth, the countries in which the studies are conducted may influence ASD rates, as different cultural significance may be attributed to symptoms (Bryant et al., 2011). This heterogeneity in rates makes it difficult to obtain an accurate portrait of the types of traumatic events that most frequently lead to ASD, thus undermining the identification of at-risk individuals, the allocation of resources, and the provision of prompt and adequate treatment (Bryant, 2016). Consolidating knowledge regarding the methodological factors that lead to heterogeneity in ASD rates may also prove useful for the interpretation of future research results.
On this note, other systematic studies on ASD exist (see Bryant et al., 2011; Sijbrandij et al., 2015), but none have specifically looked at the prevalence of ASD. Indeed, previous systematic reviews were concerned with evaluating treatment options for ASD (Sijbrandij et al., 2015; Wright et al., 2019) or assessing the capacity of ASD to predict PTSD (Bryant et al., 2011), not its prevalence as a function of trauma type. For this reason, this study adds important information to contextualize not only these previous systematic reviews but other studies in the field of trauma as well.
Objectives
The aims of the present systematic review and meta-analysis are (1) to consolidate and describe ASD rates associated with different types of traumatic events and (2) to explore the influence of selected methodological and trauma-related factors on these rates. This study represents the first systematic review and meta-analysis on the subject since the introduction of the ASD diagnosis in 1994.
Method
The current article is in line with the guidelines provided by the preferred reporting items for systematic reviews and meta-analyses (PRISMA; Liberati et al., 2009; see checklist in Appendix A). The protocol for this study was registered in PROSPERO (registration number: CRD42017062586).
Inclusion Criteria
Records were included if (1) participants were 16 years old and over; (2) the assessment was completed within 30 days of the event; (3) a standardized assessment instrument for ASD, as listed in Bryant (2016), was utilized; (4) the type of traumatic event was specified; and (5) the ASD rate was reported or the study contained enough information to calculate it. Cohort studies, baseline data from clinical trials, and cross-sectional studies were included in this review. Scientific and lay articles, dissertations, posters, book chapters, and gray literature were also considered. Systematic reviews were excluded but their references were screened. Studies examining the physical consequences of trauma (e.g., burns or traumatic brain injuries) were excluded unless the nature of the event itself was specified.
Sources of Information
Between April and May 2017, we identified ASD-related studies by searching through the PsychINFO, PubMed/Medline, OVID, CINAHL, Scopus, and PILOTS databases. The search was updated in August 2018 and October 2019 to include newly published relevant studies. Additional articles were found through the reference lists of the included studies and systematic reviews. The PROSPERO and ISRCTN databases were also scanned for potentially relevant records. Governmental websites from the United States, Canada, Australia, France, and the UK as well as the International Society for Trauma Stress Studies website were searched (see full list in Appendix B). Finally, a list of 12 select authors and known experts on ASD were contacted in August 2017 to identify additional records, published or unpublished. The list of traumatic events used for the search strategy was based on the DSM-IV and DSM-5 and was complemented by those listed in the Life Events Checklist for DSM-5 (LEC-5; Weathers et al., 2013) as well as those in the National Comorbidity Survey–Replication (NCS-R; see details in Appendix C). The search was limited to studies that were published as of 1994, the year that ASD was introduced in the DSM IV. Articles in both English and French were included. The complete list of strategies used for each database is available in Appendix D.
Study Selection and Data Collection
Identified records were distributed among four pairs of independent trained reviewers (S.Ge., J.G., I.R., J.S., S.L., M.F., and J.L.) and were subjected to a title and abstract screening to identify potential inclusions. A third reviewer (S.Ge., J.G., J.S., and S.L.) resolved disagreements between dyads. Next, each reviewer independently extracted data from their relevant articles. One reviewer (J.S.) combined the data into a spreadsheet and two reviewers (J.G. and J.S.) revised all data extraction. Extracted data pertained to methodology (e.g., participation rate, assessment instrument, assessment timeframe, DSM version), sociodemographics (e.g., country, age, sex), trauma-related information (e.g., description of event, trauma category, type of exposure), and outcomes (e.g., mean ASD scores, percentage of participants with ASD). In addition, the methodological quality of the included studies was evaluated with an instrument based on the Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies criteria (National Institutes of Health, 2014; see Appendix E for details). As such, two reviewers (S.Ge., J.G., I.R., J.S., S.L., M.F., and J.L.) independently answered 10 questions for each study, involving a third reviewer (S.Ge., J.G., I.R., J.S., and S.L.) in case of disagreement.
The following methodological and trauma-related covariates that may potentially affect ASD rates were included in the analysis: time elapsed since the event, methodological quality of the study, assessment instrument, DSM version, type of exposure (i.e., direct victims, witnesses, combined sample), geographical location, and the intentional (i.e., war-related and interpersonal) or unintentional (i.e., accident-related, disaster-related, life-threatening illness) nature of the event.
Consistent with the DSM-IV, DSM-5, LEC-5, and NCS-R, traumatic events were divided into five categories: (1) interpersonal trauma (e.g., physical, assault with a weapon, sexual assault or attempted sexual assault, captivity), (2) accident-related trauma (e.g., transportation accident, serious accident at work), (3) disaster-related trauma (e.g., natural disaster, fire, or explosion), (4) life-threatening illness (e.g., being diagnosed with or having a child diagnosed with a cancer), and (5) war-related trauma (e.g., combat or exposure to a war zone in the military or as a civilian). Studies examining ASD among individuals who were exposed to traumatic events through media coverage were excluded. According to the DSM-5, “events experienced indirectly through hearing about it are limited to close relatives and friends” and do not apply to exposure through media coverage (APA, 2013, p. 282).
Statistical Analyses
Comprehensive Meta-Analysis software (Version 3.0) was used for all statistical analyses. Data regarding ASD rates from all included studies were pooled using random-effects statistics due to the substantial methodological heterogeneity generally identified in systematic reviews. A series of univariate meta-regressions were conducted to examine the effect of potential methodological and trauma-related moderators, using continuous and categorical analyses where appropriate. Multiple meta-regressions could not be calculated due to an insufficient number of studies. The extent of heterogeneity was measured with Q value (Higgins & Thompson, 2002), while the percentage of variation across studies due to heterogeneity rather than chance (Higgins & Thompson, 2002) was assessed with I2. Finally, the potential for publication bias was assessed using funnel plots (Song et al., 2002), and Duval and Tweedie’s trim and fill was performed in cases of possible publication bias.
Results
Characteristics of the Included Studies
A total of 5,187 records were identified and 70 studies were ultimately included in the present review. Figure 1 presents the PRISMA flow diagram describing the study selection process. The 70 records included in this review, comprised of 73 samples, assessed the associations between five categories of traumatic events and subsequent ASD rates: interpersonal trauma (k = 14), accident-related trauma (k = 22), disaster-related trauma (k = 4), life-threatening illness (k = 28), and war-related trauma (k = 5). Studies that assessed both adults and youth under 16 were included if they reported data separately, making it possible to exclude youth from the present meta-analysis. Of the 73 samples, 62 relied on the DSM-IV, 5 on the DSM-IV-TR, and 6 did not mention the DSM version on which they relied. No studies utilizing the DSM-5 met inclusion criteria. The full reference list as well as the characteristics of each included study are presented in Appendix F.
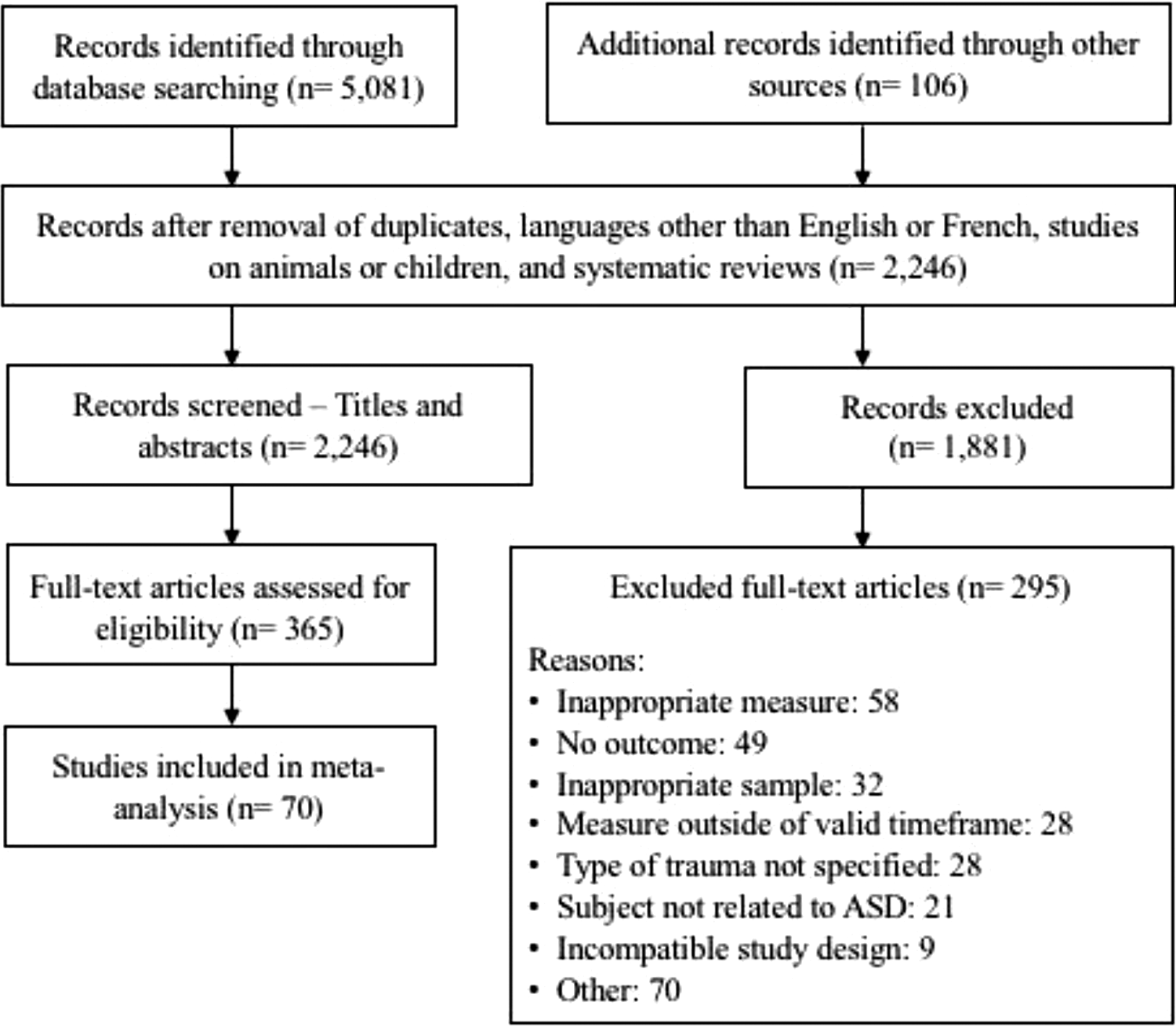
Preferred reporting items for systematic reviews and meta-analyses flow diagram.
Rates per Type of Traumatic Event and Differences Between Instruments
The overall rate for ASD was 20.4% (95% CI [16.6, 24.9], k = 73). Rates ranged from 14.1% (95% CI [6.3, 28.4], k = 5) for war-related trauma to 36.0% (95% CI [23.9, 50.1], k = 14) for interpersonal trauma. The overall Q value was 2,762.962, p < .001, which indicates that the true effect size probably varies across studies, and so the assumptions of the fixed-effect model have been violated. The I2 = 97.39% indicates that almost all of the observed variance reflects real differences in study effects. In the mixed-effect analysis, the effect size differed by assessment measure (Q value = 30.70, df = 4, p < .001) and by type of traumatic event (Q value = 13.56, df = 4, p = .009). The highest rate, that of interpersonal trauma, was significantly different from all other types, except for disaster-related trauma. No other statistical differences were found. Table 1 presents the results of the meta-regression of ASD rates according to the type of traumatic event.
Meta-Regression of ASD Rates According to the Type of Traumatic Event.
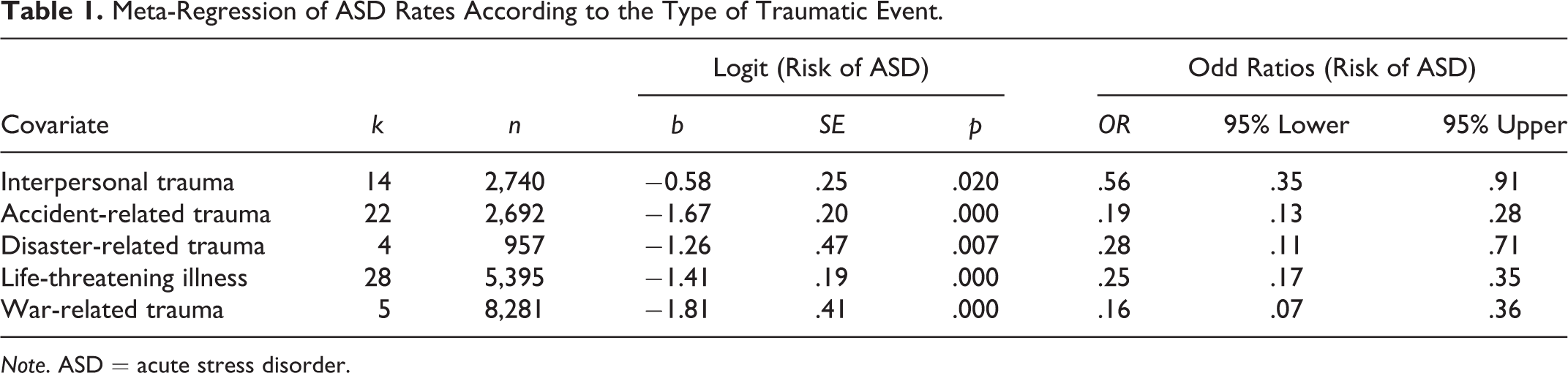
Note. ASD = acute stress disorder.
The following section presents the differences in ASD rates across measurement instruments for each type of traumatic event. Since different instruments have different psychometric properties, use different cutoff scores and item formulation, prevalence rates were regrouped by instrument type. Certain comparisons included a small number of studies per category (<5) and should thus be interpreted with caution. See Appendix G for plots according to the different types of trauma.
Interpersonal trauma
The ASD rate for interpersonal trauma is 36.0% (95% CI [23.9, 50.1], k = 14). Significant heterogeneity across studies was found for the Acute Stress Disorder Interview (ASDI; Bryant et al., 1998; I2 = 93.97%, p < .001, k = 3), the Acute Stress Disorder Scale (ASDS; Bryant et al., 2000; I2 = 97.89%, p < .001, k = 9), and the Stanford Acute Stress Reaction Questionnaire (SASRQ; Cardena et al., 2000; I2 = 90.76%, p = .001, k = 2). The use of the ASDS and the ASDI led to a rate of 27.9% (95% CI [16.1, 43.8], k = 9) and 39.2% (95% CI [15.8, 68.9], k = 3), respectively. Finally, the studies that used the SASRQ yielded a rate of 71.6% (95% CI [35.9, 91.9], k = 2).
Accident-related trauma
The ASD rate for accident-related trauma was 15.9% (95% CI [11.5, 21.7], k = 22). Significant heterogeneity across studies was observed for the ASDI (I2 = 54.51%, p = .009, k = 13), the ASDS (I2 = 88.64, p < .001, k = 4), and the Structured Clinical Interview for DSM-IV (SCID; First & Gibbon, 2004; I2 = 93.79%, p < .001, k = 2). Studies combining the Clinically Administered PTSD Scale (Blake et al., 1995) and the Peritraumatic Dissociative Experiences Questionnaire (Marmar et al., 1997), and those using the SASRQ yielded a rate of 3.9% (95% CI [1.8, 8.4], k = 2) and 12.3% (95% CI [4.7, 28.3], k = 1), respectively. Studies using the ASDI yielded a rate of 15.5% (95% CI [11.7, 20.3], k = 13). Papers that used the SCID and the ASDS reported the highest rate, with 23.6% (95% CI [11.7, 42.0], k = 2) and 29.4% (95% CI [19.5, 41.8], k = 4), respectively.
Disaster-related trauma
The ASD rate for disaster-related trauma was 21.9% (95% CI [9.2, 43.6], k = 4). Between-study heterogeneity was observed for ASDS (I2 = 97.56%, p < .001, k = 3). The study that used the SASRQ yielded a rate of 4.9% (95% CI [0.1, 27.5], k = 1), while studies using the ASDS found higher rates with 31.4% (95% CI [13.7, 57.0], k = 3).
Life-threatening illness
The ASD rate for life-threatening illness is 20.7% (95% CI [16.2, 26.1], k = 28). Significant between-study heterogeneity was found for the ASDS (I2 = 93.97%, p < .001, k = 12), SASRQ (I2 = 80.40%, p < .001, k = 7), and SCID (I2 = 64.52%, p = .015, k = 6). Studies that used the SCID yielded a rate of 4.1% (95% CI [2.1, 7.7], k = 6). Studies using the SASRQ and the ASDI found higher rates at 19.8% (95% CI [13.6, 28.0], k = 7) and 19.7% (95% CI [10.2, 34.7], k = 3), respectively. Studies that used the ASDS yielded the highest rate, with 33.8% (95% CI [26.7, 41.7], k = 12).
War-related trauma
The ASD rate for war-related trauma was 14.1% (95% CI [6.3, 28.4], k = 5). Significant heterogeneity across studies was observed for the SASRQ (I2 = 97.51%, p < .001, k = 4). Studies that used the SASRQ reported a rate of 10.1% (95% CI [5.6, 17.5], k = 4). The study that used the ASDI yielded a rate of 39.0% (95% CI [15.6, 68.8], k = 1).
Other Covariates Contributing to the Variance of ASD Rates
The type of exposure to the traumatic event (i.e., direct victim, witness, combined sample), the geographical region in which the studies were conducted (i.e., North America, Europe, Asia, Africa, Oceania), the mean number of days between the event and the diagnosis, the quality of the study design, and the intentional nature (vs. unintentional) of the event were entered into univariate meta-regressions to assess for their contribution to the variance of ASD rates. The type of exposure, the intentional nature of the event, and the geographical location were found to contribute to heterogeneity in ASD.
Type of exposure
The type of exposure to the traumatic event did not explain a significant proportion of variability across studies for accident-related trauma, Qmodel(1) = 0.73, p = .3944, R2 < .01, or for disaster-related trauma, for which there was only one type of exposure. However, studies assessing combined types of exposure to war-related trauma, Qmodel(2) = 9.31, p = .002, R2 = .66, reported significantly lower rates of ASD than those evaluating direct victims exclusively. The type of exposure also explained significant variability across studies for life-threatening illness, Qmodel(2) = 21.69, p < .001, R2 = .13. Generally, studies focusing on witnesses only and those combining both types of exposure reported higher rates than those focusing solely on direct victims. See Table 2 for complete meta-regression results by type of exposure to the traumatic event.
Meta-Regression According to the Type of Exposure to the Traumatic Event.
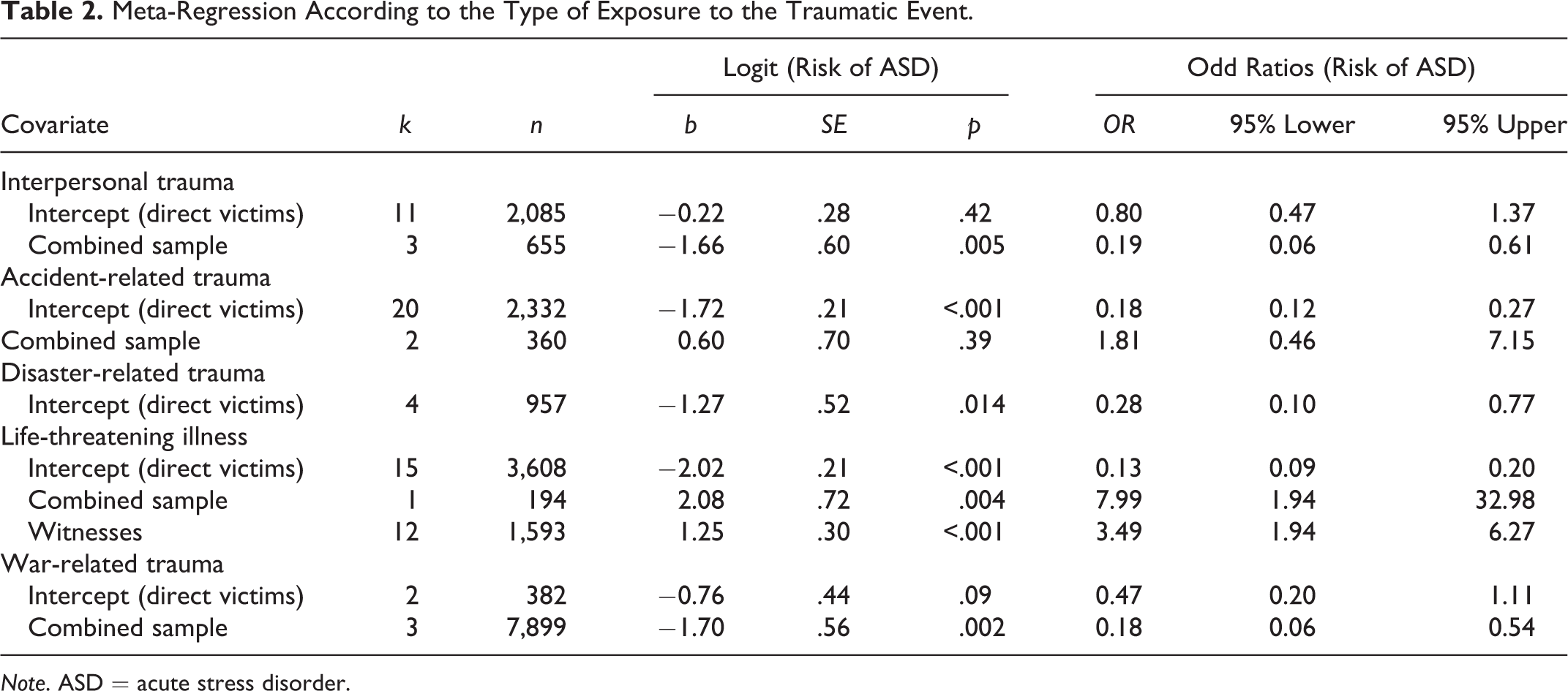
Note. ASD = acute stress disorder.
Intentional versus unintentional nature of the event
The five categories of traumatic events were dichotomized into intentional acts (i.e., war-related and interpersonal trauma; k = 19) and unintentional events (i.e., life-threatening illness, accident-related trauma, disaster-related trauma; k = 54). The nature of the event accounted for significant variability across studies, Qmodel(1) = 4.51, p = .034, R2 < .0, with intentional acts yielding higher rates of ASD (OR = 1.87, 95% CI [1.05, 3.35]) than unintentional traumas.
Geographical location
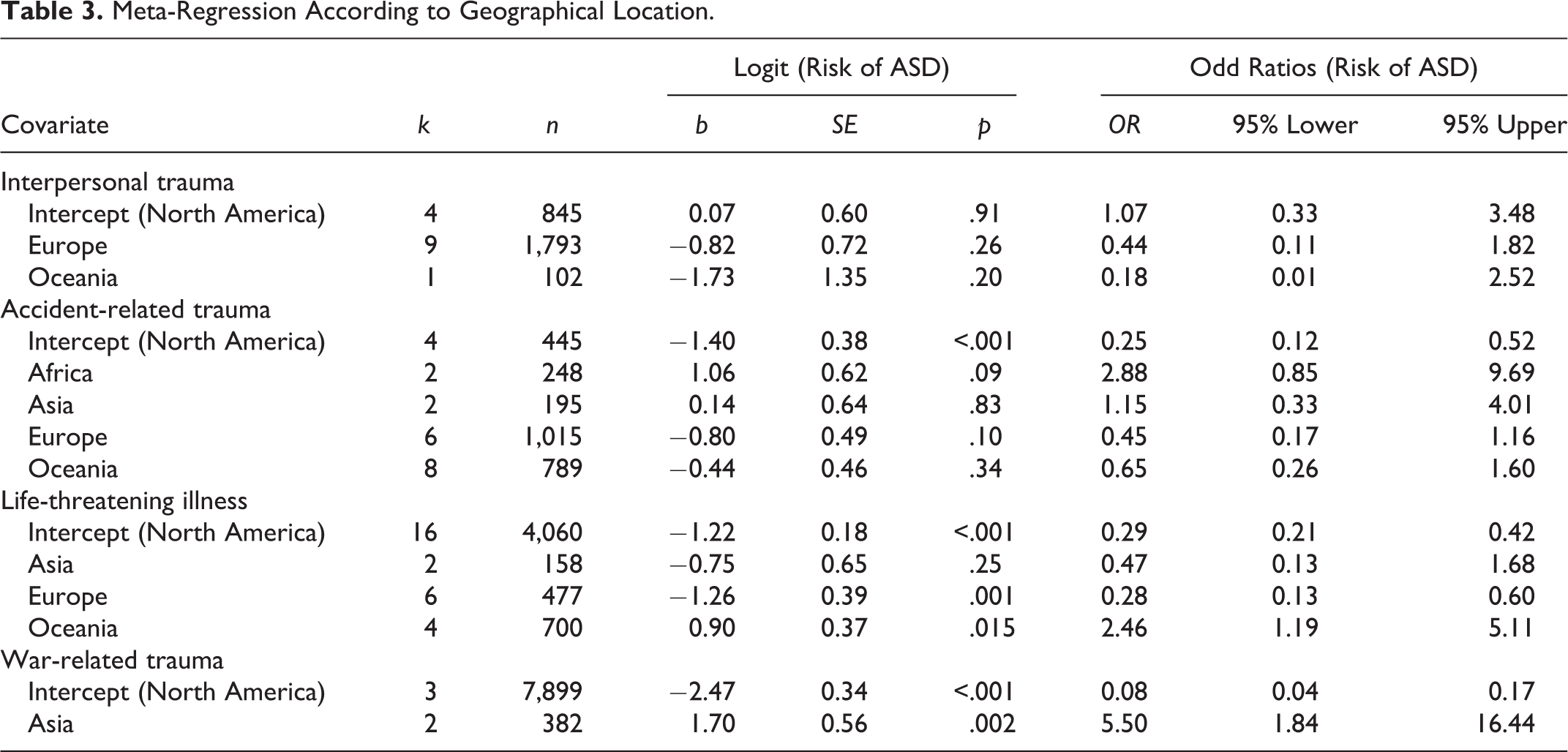
The geographical regions in which studies were conducted explained significant variability across studies for war-related trauma, Qmodel(1) = 9.31, p < .001, R2 = .66. Generally, war-related studies conducted in Asia reported higher rates than those from North America. For life-threatening illness, Qmodel(3) = 22.22, p < .001, R2 = .24, studies conducted in North America reported higher rates than those from Europe but lower rates than those from Oceania. For accident-related trauma, Qmodel(4) = 11.99, p = .017, R2 = .39], studies conducted in Europe and Oceania reported lower ASD rates than other regions. There were no significant differences in ASD rates across geographical regions for interpersonal trauma, Qmodel(2) = 2.13, p = .3442, R2 < .01. Finally, studies investigating disaster-related trauma were insufficient to conduct analyses. See Table 3 for complete meta-regression results.
Meta-Regression According to Geographical Location.
Funnel Plot Analysis
The only probable publication bias concerned life-threatening illness (see Appendix H). For this trauma category, the funnel plot was asymmetrical, with a relatively high number of small samples (representing a large effect size) falling toward the left of the mean effect and relatively few falling toward the right. A Duval and Tweedie’s trim and fill showed that five studies would be missing to the right of mean. The random effects of the OR would shift from 29.6% (95% CI [28.3, 31.0]) to 30.0% (95% CI [28.7, 31.4]). For the other types of traumatic events, analyses indicated that the studies were distributed symmetrically around the mean effect size (see tables and figures in Appendices G and H).
Discussion
The main purpose of this study was to describe ASD rates following different types of traumatic events. Given the disparity of these rates in the literature, a systematic review and meta-analysis were conducted to assess the influence of different methodological and trauma-related factors on these rates. Results revealed that ASD rates ranged from 14.1% for war-related trauma to 36.0% following interpersonal trauma, with accident-related trauma (15.9%), life-threatening illness (20.7%), and disaster-related trauma (21.9%) falling in between. Interpersonal trauma was significantly more likely to lead to ASD than other types of events, except for disaster-related trauma. The lack of statistical difference between these two types of events appears to be related to the limited number of studies assessing disaster-related trauma and the resulting coefficient and standard error. Taking this into account, the present results are consistent with previous studies that have shown that persons exposed to interpersonal trauma are at higher risk of developing post-traumatic sequelae such as PTSD (Creamer et al., 2001; Kessler et al., 1995). The current review extends these findings to the development of ASD. As such, exposure to interpersonal violence should be considered a risk factor for the development of ASD and should be included in clinical screening practices. In the same vein, governmental and private aid agencies should dedicate financial and human resources to the provision of interventions aiming to prevent enduring post-traumatic symptoms among victims of interpersonal violence.
The influence of certain covariates on the heterogeneity of rates within categories of traumatic events was also analyzed. The utilized assessment instruments, the types of exposure, the intentional nature of certain events, and the geographical locations in which the studies were conducted significantly contributed to disparities in ASD rates. On the other hand, the quality of the research design and the time elapsed since the event did not contribute to heterogeneity.
Assessment Instruments
The assessment instruments used to evaluate ASD contributed to heterogeneity within the categories of traumatic events. For example, the use of the ASDS for accident-related trauma, disaster-related trauma, and life-threatening illnesses, as well as the SASRQ for interpersonal trauma, yielded higher ASD rates in these respective categories than any other measures. The ASDI yielded a higher rate for war-related trauma, although this result is to be interpreted with caution as it relies solely on one study. Altogether, these findings illustrate how different assessment strategies contribute to disparity in ASD rates within the same types of traumatic events.
Types of Exposure to the Traumatic Event
War-related trauma studies exclusively assessing direct victims reported higher ASD rates than those combining direct victims and witnesses. This result is reminiscent of the “magnitude of exposure” to traumatic events, a concept documented in the PTSD literature and based on the finding that the severity of physical injuries and the presence of an immediate risk to one’s life are predictive of high rates of PTSD (Neria et al., 2008). This implies that direct victimization may lead to higher post-traumatic reactions than more distal exposure. However, studies that relate to life-threatening illnesses yielded opposite results. In this case, studies assessing witnesses and those combining both types of exposure uncovered higher ASD rates than studies exclusively focusing on direct victims. A possible explanation for this may lie in the fact that, in all the included studies, the witnesses were parents of children who were facing death. These parents may perceive a low sense of control regarding the health outcomes of their child or may have to act as a source of support for their child in addition to coping with the diagnosis themselves. This lack of perceived control (Benight & Bandura, 2004) and the presence of ongoing stressors (Bryant, 2016) may exacerbate post-traumatic reactions. Overall, additional research examining witnesses of traumatic events is warranted in order to comprehensively evaluate the psychological impact of such events as a function of type of exposure.
The Intentional Nature of Certain Events
Intentionally inflicted acts of violence were associated with higher rates of ASD than unintentional traumas such as accidents, natural or man-made disasters, and life-threatening illnesses. These findings corroborate the research that has been conducted among victims of violent crime, which demonstrates the multitude of exacerbating factors related to such intentional victimization. Indeed, certain psychosocial aspects such as negative social reactions (e.g., victim blaming, stigma, control) and loss of interpersonal trust may increase the risk of post-traumatic stress reactions and maladaptive coping strategies while hindering help-seeking (O’Hara, 2012; Ullman & Peter-Hagene, 2014). Furthermore, previous authors have found that intentional trauma, especially when it involves betrayal, is associated with increased symptomatology (Platt et al., 2017). For example, survivors of intentional trauma are more likely to report suicidal ideation than survivors of unintentional trauma (Yoo et al., 2018). There are also different factors to consider during treatment. For example, Yoo and colleagues (2018) have found that high agreeableness and conscientiousness predicted less suicidality in those exposed to unintentional trauma, while predicting more suicidality in those exposed to intentional trauma. Also, patterns associated with revictimization risk differ between intentional trauma and unintentional trauma (Jaffe et al., 2019). Another exacerbating aspect of intentional victimization is the possibility of involvement in judicial processes. In addition to the psychosocial consequences of the event itself, victims may experience secondary victimization and increased distress due to negatively perceived interactions with law enforcement and the criminal justice system, as well as involvement in or even anticipation of legal investigations, hearings, trials, and the uncertain nature of the outcome (Green & Roberts, 2008). Put together, these psychosocial and judicial factors may account for increased rates of ASD following intentional traumatic events and interpersonal trauma more specifically.
Geographical Location
The region of the world in which the studies were conducted was a contributor to the heterogeneity of ASD rates for war-related trauma, accident-related trauma, and life-threatening illnesses. These findings should however be considered with caution given that different types of traumatic events were regrouped into larger categories (e.g., physical and sexual assaults studied together). Also, findings are based on a limited number of studies that do not presume to represent the population of the continent from which they stem. Most importantly, findings illustrate the pervasive underrepresentation of patients, especially women, in developing countries in research studies. This lack of specific information regarding the acute phase of trauma impedes the development of culturally appropriate treatment options for minorities and the global community (Wilson, 2008). Nonetheless, when considering differences and similarities in reported ASD rates within the same type of traumatic event, it may be useful to consider the culture-related diagnostic issues discussed in the DSM-5. The profile of symptoms of ASD may vary cross-culturally, particularly with respect to dissociative symptoms, nightmares, avoidance, and somatic symptoms (e.g., dizziness, shortness of breath, heat sensations). Cultural syndromes and idioms of distress shape the local symptom profiles of ASD. (APA, 2013, p. 285)
Comments Regarding the DSM and Life-Threatening Illnesses
The results of this meta-analysis should be interpreted in light of the changes made to the ASD diagnosis in the DSM-5 as compared to the DSM-IV. “Being diagnosed with a life-threatening illness” was considered a potentially traumatic event in the DSM-IV (APA, 1994, p. 424). Diagnostic Criterion A (i.e., exposure to an extreme traumatic stressor involving direct personal experience of an event that involves actual or threatened death) allowed for the inclusion of such medical diagnoses. In addition, this same criterion (i.e., the threat of death or injury experienced by a family member or other close associate) allowed for the inclusion of relatives, suggesting that they too could suffer from ASD as a result of their loved one’s illness. The DSM-5, however, no longer characterizes life-threatening illnesses in-and-of-themselves as potentially traumatic events. According to this version of the DSM, “medical incidents that qualify as traumatic events involve sudden, catastrophic events (e.g., waking during surgery, anaphylactic shock),” thus excluding more gradual illnesses such as cancer (APA, 2013, p. 282). By focusing on the medium and duration of the event while neglecting its subjective experience (Swartzman et al., 2017), the DSM-5 may be neglecting patients and loved ones that are at risk of developing post-traumatic sequelae such as ASD. In fact, the results of the present systematic review revealed that up to 30.4% (Zhu et al., 2018) of patients diagnosed with cancer and up to 61.4% of relatives of patients with cancer (McCarthy et al., 2012) are at risk of developing ASD. These findings are similar to those of a recent meta-analysis regarding PTSD following cancer, in which survivors were 1.66 times more likely to develop PTSD compared to controls, and the relatives and caregivers of cancer survivors had PTSD in similar proportions to the survivors themselves (Swartzman et al., 2017). Taken together, these findings suggest that further discussion is warranted regarding the potentially traumatic impact of life-threatening illnesses on patients and their loved ones. The inclusion or exclusion of life-threatening illnesses in future DSM diagnostic criteria for ASD and even PTSD may need to be revisited.
Limitations
The current findings should be interpreted considering certain limitations. First, as war-related studies are numerous within PTSD research but are scarce in the field of ASD, the results related to this type of trauma should be interpreted with caution. The difficulties related to assessing individuals within a 1-month period of war-related trauma exposure may explain this scarcity of studies. An additional consideration would be for future studies to evaluate differences in ASD rates in patients who sought help and those who were recruited through other means. Second, no studies utilizing the DSM-5 met inclusion criteria. It was therefore not possible to compare rates based on the DSM-5 and the DSM-IV and to assess possible disparities. This comparison should be conducted in a few years when a larger number of studies utilizing the DSM-5 become available. As noted by Bryant (2016), substantial changes were made to the diagnostic formulation of ASD in the DSM-5, namely the elimination of dissociative reactions as a requisite, an increase in the number of symptoms necessary for diagnosis, and modifications to Criterion A. In light of these changes, it remains to be seen whether the present ASD rates will generalize to rates of probable diagnosis in future research. A third limitation stems from the categorization of traumatic events. Although our classification was conceptually based, specific subtypes of events (e.g., physical assault, rape) may differ in their impact on ASD rates, and this effect may have been suppressed by the overarching categories of trauma (e.g., interpersonal trauma). Fourth, the majority of included studies omitted analyses regarding sex and gender differences in rates, even though there is strong evidence that suggests that women are more likely than men to manifest post-traumatic reactions after a traumatic event (Bryant, 2016; Tolin & Foa, 2006). This same limitation applies to racial and ethnic disparities. Although many authors have concluded that Black people are more likely to suffer from PTSD than Whites (Roberts et al., 2011), studies on ASD have so far not verified these findings. Therefore, the current study could not test the moderating effect of sex, gender, race, or ethnicity on ASD rates. This underrepresentation limits the generality of findings as well as the development of culturally appropriate treatment options (Wilson, 2008). Nevertheless, this article has several strengths, as steps were taken to minimize biases related to language (Egger et al., 1997), availability, cost, familiarity, and duplication. In addition, except for studies on life-threatening illnesses, no evidence of publication bias was uncovered, which suggests that the present results represent the overall literature on ASD rates.
Conclusion
The first of its kind, this systematic review and meta-analysis aimed to assess ASD rates following different types of traumatic events. Results suggested that the type of traumatic event, differing assessment instruments, types of exposure, geographical locations, and the intentional nature of certain events contribute to disparities in ASD rates. Future systematic reviews attempting to draw a portrait of risk would benefit from more thorough reporting of sociodemographic characteristics (i.e., age, sex, gender) and antecedents of trauma among studies examining ASD. Moreover, additional research examining the impact of proximity to the traumatic event on ASD rates is warranted. This would benefit the debate regarding direct exposure to trauma as a necessary condition for ASD (APA, 2013), as some researchers question the notion of an interaction between a “sufficient” level of exposure (e.g., through TV broadcasts) and certain risk factors (e.g., genetic susceptibility; Neria et al., 2008). In line with the cultural issues discussed in the DSM-5, future studies should also investigate the factors underlying differential experiences of trauma according to the region or culture of the affected individual. Finally, when more studies using DSM-5 diagnostic criteria become available, future research should investigate the moderating effects of different DSM versions on reported ASD rates.
Summary of Implications for Practice, Policy and Research
Supplemental Material
Supplemental Material, Appendix_JS_11122019 - Systematic Review and Meta-Analysis on Acute Stress Disorder: Rates Following Different Types of Traumatic Events
Supplemental Material, Appendix_JS_11122019 for Systematic Review and Meta-Analysis on Acute Stress Disorder: Rates Following Different Types of Traumatic Events by Steve Geoffrion, Jane Goncalves, Isabelle Robichaud, Josette Sader, Charles-Édouard Giguère, Maxime Fortin, Josianne Lamothe, Paquito Bernard and Stéphane Guay in Trauma, Violence, & Abuse
Footnotes
Acknowledgments
The authors would like to thank Sophie Lacerte, psychologist, for her precious help in the study selection process. The authors would also like to thank the experts who gave them their feedback on the potential inclusion of other studies.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a research grant awarded to the VISAGE research team by the Canadian Institutes of Health Research (CIHR—TVG251591) and the Foundation of Institut universitaire en santé mentale de Montréal.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.