
Abstract
Theoretical literature suggests that trauma and (PTSD) may instigate changes in the interpretation of bodily signals. Some findings support these inquiries, revealing that exposure to traumatic events and PTSD are associated with pain catastrophizing, body vigilance, fear of pain, and other manifestations of bodily perceptions and interpretations. However, these findings are not integrated into an inclusive empirically based conceptualization, thus leading to a limited comprehension of this phenomenon. This systematic literature review was conducted to synthesize the existing literature referring to orientation to bodily signals. Using Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, the review included a final of 48 manuscripts that addressed orientation to bodily signals among participants (aged 18 and above) and its potential associations with PTSD. The review revealed that most studies assessed one orientation manifestation, which was tested for its link to PTSD. The majority of the manuscripts were cross-sectional and included participants who faced combat, vehicle accidents, or various types of traumas. Only five manuscripts focused on interpersonal trauma and abuse. Most manuscripts reported significant correlations, revealing that trauma and PTSD are associated with a negative, catastrophic and frightful interpretation of bodily signals. These findings emphasize the need to encapsulate the various manifestations of orientation to bodily signals under a unified construct, as proposed by the term post-traumatic orientation to bodily signals. Further research is needed to illuminate the circumstances and processes by which trauma is implicated in post-traumatic orientation to bodily signals.
Keywords
Trauma has been shown to yield a myriad of debilitating consequences (Pace & Heim, 2011; Pacella et al., 2013). Extensive literature has demonstrated the malevolent implications of exposure to trauma for mental health, with the most conspicuous ramification encapsulated in post-traumatic stress disorder (PTSD; Bryant, 2019; Dworkin et al., 2017; Lohr et al., 2015; Solomon et al., 2017). Other commonly documented psychosocial implications of trauma have been observed in complex post-traumatic stress disorder (CPTSD; Cloitre et al., 2018; Zerach et al., 2019) depression (Heim et al., 2008; Nichter et al., 2019), anxiety (Heim & Nemeroff, 2001; Price et al., 2019), dissociation (Bailey & Brand, 2017; Bremner & Marmar, 2002; Spiegel, 1997), substance abuse disorders (Ullman et al., 2013), eating disorders (Brewerton, 2007; Trottier & MacDonald, 2017), and various types of self-mutilating behaviors (C. M. Lang & Sharma-Patel, 2011; Turell & Armsworth, 2000). Furthermore, exposure to trauma has been shown to be implicated in physical morbidity, such as gastrointestinal health (Pacella et al., 2013), cardiovascular morbidity (Beristianos et al., 2016), chronic pain (Asmundson & Katz, 2009; Sharp & Harvey, 2001; Siqveland et al., 2017), autoimmune diseases (O’Donovan et al., 2015), and early mortality (see Lohr et al., 2015).
Between these mental and physical derivatives of exposure to trauma, it seems that another dimension has gone under the radar. This dimension is related to the way individuals interpret their bodily signals following exposure to trauma, especially in cases where they suffer from PTSD. Although less studied, theoretical explanations have been proposed for the experience of the body following exposure to traumatic events, mainly referring to the understanding that “the body keeps the score” (Van der Kolk, 2015). Specifically, PTSD may alter an individual’s interpretation of the body as a safe entity by disrupting the basic constellation of their orientation toward their body (Tsur, Defrin, et al., 2018; Van der Kolk, 2015). Potential mechanisms by which interpretation of bodily signals may be altered following trauma can be viewed through the lens of the psychophysiology of PTSD (Dunlop & Wong, 2019). Specifically, the activation of the hypothalamic–pituitary–adrenal (HPA) axis and sympathetic–adrenal–medullary system (Heim & Nemeroff, 2009) entail significant bodily sensations that instigate the sense of the traumatic event repeatedly reoccurring (Van der Kolk, 1994). This may be especially relevant for the hyperarousal PTSD cluster (Tsur, Defrin, et al., 2018). As such, stress-related somatic signals could be categorized as threatening stimuli and interpreted as catastrophic and frightful. Unique post-traumatic memory processes may intensify such negative interpretations of bodily sensations imprinted in the memory of the traumatic event. In these memory processes, traumatic experiences are coded in implicit-somatosensory memory, which is often not properly synced with the autobiographical memory (Brewin, 2011). As a result, the sense of ease and trust in the functioning of the body are often replaced with bodily sensations that reflect the implicit memory of the traumatic experience (Brewin, 2011).
These theoretical explanations suggest that, for individuals exposed to trauma and especially those who suffer from PTSD, the body may become the stage for reexperiencing pain and suffering (Tsur et al., 2020; Tsur, Shahar, et al., 2017), referred to as the “somatic memory” of trauma (Levine, 1997; Van der Kolk, 2015). As a result, bodily sensations, such as heart palpitations or headaches, whether related to illness or not, might be construed as a potential danger to the self, interpreted as catastrophic and frightful sensations (Tsur, Defrin, et al., 2018).
Unfortunately, empirical investigations of these theoretical ideas are limited and lack a well-articulated integration of empirical findings with theoretical explanations. That is, some findings have revealed that PTSD is correlated with the tendency to interpret pain sensations as catastrophic, as seen in the association between PTSD and pain catastrophizing (e.g., Gaffey et al., 2019; Ravn et al., 2019) and PTSD and fear of pain (Andersen et al., 2016; Martin et al., 2010). Katz and colleagues (2017) proposed the term sensitivity to pain traumatization. This term reflects the tendency to develop anxiety-related behavioral responses to pain that resemble traumatic stress reactions, thus potentially underlying existing pain-related anxiety. Other findings have implied a significant link between PTSD and the tendency to fear somatic-related manifestations of anxiety. Such findings denote an association between PTSD and the physical dimension of the anxiety sensitivity construct (Short et al., 2017; Zvolensky et al., 2018). From another related point of view, findings have also demonstrated a link between body vigilance and PTSD, particularly as part of the panic disorder cycle (Vujanovic et al., 2008).
Most of the above studies were not originally conducted to attest to the interpretation of bodily signals following trauma. However, these findings indirectly indicate that PTSD may be implicated in negative, presumably catastrophic and frightful interpretations of bodily signals. Nevertheless, a synthesized and comprehensive conceptualization is still lacking, as well as a firm integration of theoretical ideas with empirical findings.
Considering the enormous costs of chronic morbidity, often comorbid with PTSD (Ferry et al., 2015), a synthesis of previous literature regarding how individuals interpret bodily signals (i.e., orientation to bodily signals) holds substantial implications for research, practice, and policy. This study aims to systematically analyze the literature referring to indications of the ways individuals interpret bodily sensations following exposure to potentially traumatic events, inferring to orientation to bodily signals. The current review will assess manuscripts detailing findings regarding various manifestations of orientation to bodily signals that have included an examination of its association with PTSD following potentially traumatic experiences.
Method
This review was prepared in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Moher et al., 2009). The studies included in the current analysis were identified by searching the following primary databases: PsycNet, PubMed, and Science Direct. The PRISMA guidelines were implemented to filter the studies, in accordance with the PRISMA stages. First, all databases were searched with the following key words: (1) posttraumatic stress 1 and (2) PTSD, which were combined with (using “plus” +) the following key words: (1) pain catastrophizing, (2) anxiety sensitivity, (3) body vigilance, (4) fear of pain, and (5) pain acceptance. The review included orientation manifestations that reflected the interpretation of bodily signals. Other related concepts such as sensitivity to pain traumatization, pain anxiety, illness perception, and fear of movement were not included, as they refer to multifaceted constructs (Carleton & Asmundson, 2009) and include additional factors such as physiological arousal, behavioral responses (Katz et al., 2017; McCracken & Dhingra, 2002; McCracken et al., 1992), or perceptions regarding behavior rather than bodily signals (Korri et al., 1990; Shelby et al., 2012). These factors also include manifestations presumably related to the interpretation of bodily signals, however, they extend beyond it and, therefore, were not included in the current analysis. Figure 1 depicts the PRISMA stages that were followed to create the systematic review. 2
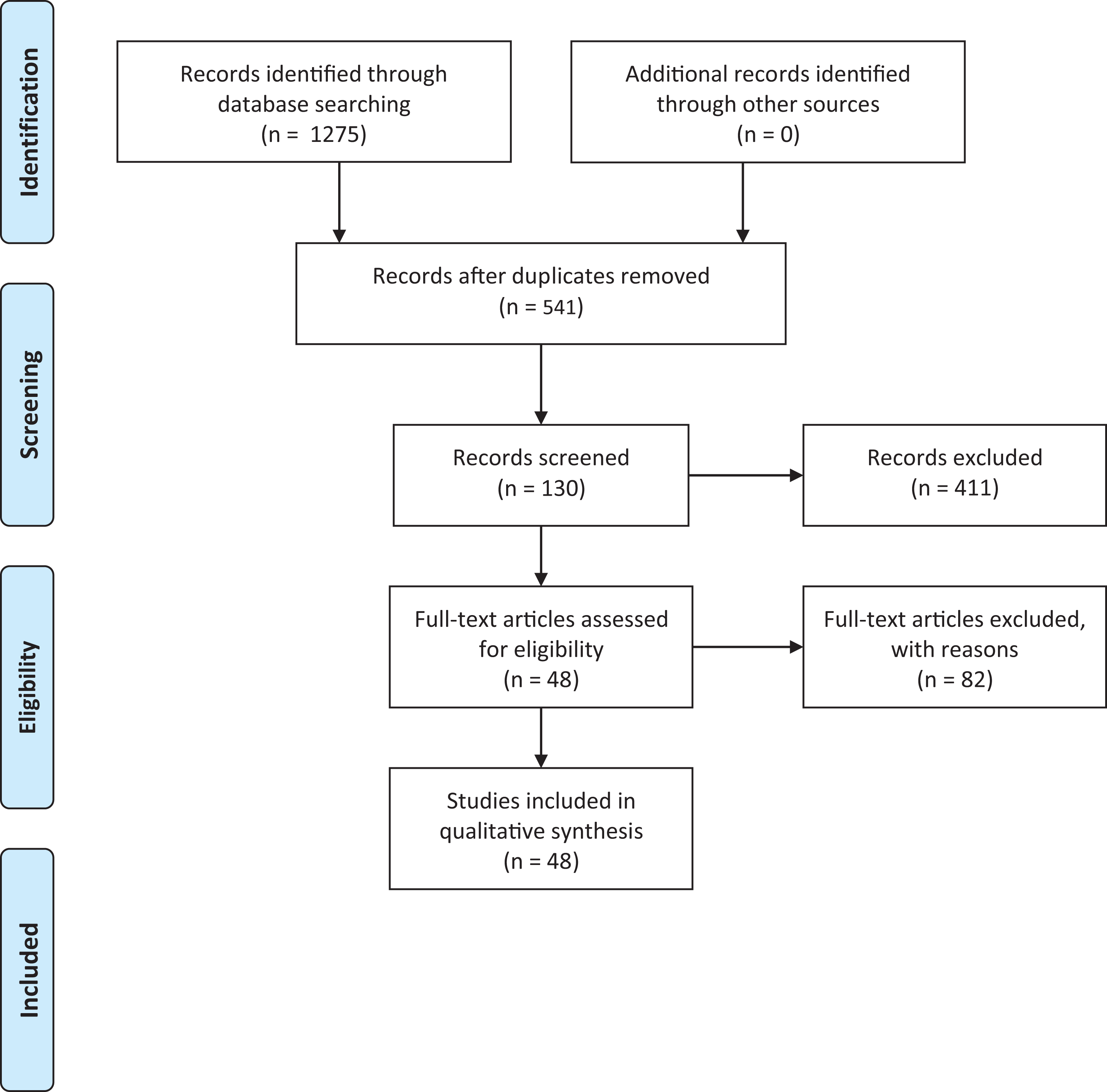
Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2009 flow diagram.
A database was generated compiling the above search criteria. Then, all abstracts were screened to determine eligibility based on the following predefined criteria: (1) English language, (2) published in peer-reviewed journals, (3) addressing orientation to bodily signals among participants above the age of 18, (4) reporting findings inferring associations between orientation to bodily signals and PTSD or exposure to trauma, and (5) for the anxiety sensitivity literature, the results sections of papers that used the Anxiety Sensitivity Index (ASI) were reviewed to check whether they reported findings concerning the association between the ASI-Physical subscale and post-traumatic stress/PTSD. Papers were included if they tested the anxiety sensitivity-physical (AS-physical) dimension separately rather than the total ASI (Peterson & Heilbronner, 1987; Taylor et al., 2007).
Although the results included hundreds of manuscripts, only 48 manuscripts fit the study’s inclusion criteria. In cases of uncertainty or discrepancy regarding suitability, both authors thoroughly reviewed the papers and determined their relevancy. Exhaustive relevant information regarding the study’s goals and each paper from the search results were summarized in Table 1, leading to the final included manuscripts.
Preliminary Analysis
Summary of Main Findings.
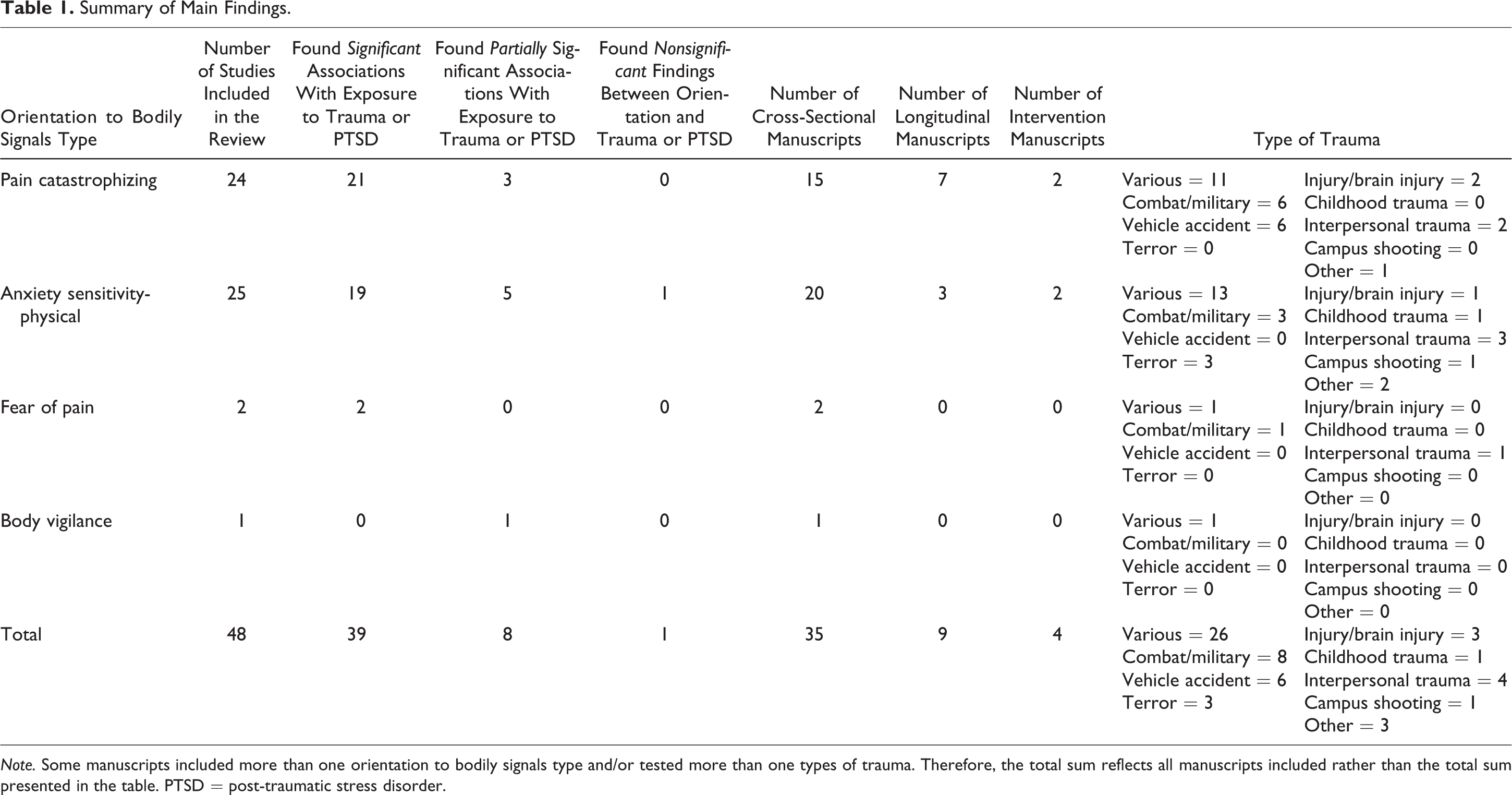
Note. Some manuscripts included more than one orientation to bodily signals type and/or tested more than one types of trauma. Therefore, the total sum reflects all manuscripts included rather than the total sum presented in the table. PTSD = post-traumatic stress disorder.
As can be seen in Table 1, 24 manuscripts (50% of all manuscripts) reported findings referring to an association between PTSD and pain catastrophizing, 25 manuscripts (52.08%) reported findings referring to the association between PTSD and AS-physical, two manuscripts (4.17%) reported findings referring to the association between PTSD and fear of pain, and one manuscript (2.08%) reported findings regarding the association between PTSD and body vigilance. Although one manuscript was originally thought to be relevant as it inferred an association between PTSD and/or pain acceptance, it was later excluded in the advanced review stages as it was not in line with the inclusion criteria. Sample sizes varied from 45 to 1,377, with a mean sample size of 268.64 (SD = 255.26).
The majority of the manuscripts reported findings inferring significant associations between orientation to bodily signals and PTSD (n = 39; 81.25%), eight manuscripts reported partially significant associations between orientation to bodily signals and PTSD (16.67%), and only one manuscript reported nonsignificant associations between orientation to bodily signals and PTSD (2.08%).
Primary Analysis
Table 1 depicts the main findings of the current review. Full information regarding the reviewed manuscripts can be found in Online Appendix A.
Types of trauma and the link to orientation to bodily signals
The samples in the reviewed manuscripts were heterogeneous in the types of trauma tested. Specifically, approximately half of the manuscripts (n = 26; 54.17%) assessed adults with various trauma types. Among these manuscripts, 11 included pain catastrophizing orientation (Andersen et al., 2017; Defrin et al., 2015; Gaffey et al., 2019; Grossi et al., 2000; Horsham & Chung, 2013; Kleiman et al., 2011; López-Martínez et al., 2014; Martin et al., 2010; M. L. Roth et al., 2013; R. S. Roth et al., 2005; Ruiz-Párraga & López-Martínez, 2014), 13 included AS-physical orientation (Albanese et al., 2018; Asmundson & Carleton, 2007; Asmundson & Stapleton, 2008; Bakhshaie et al., 2015; Feldner et al., 2008; Kraemer et al., 2013; McDermott et al., 2009; Post et al., 2016; Short et al., 2017; Stanley et al., 2017; Vujanovic et al., 2008; Zvielli et al., 2012; Zvolensky et al., 2018), one included fear of pain orientation (Asmundson & Carleton, 2007), and one included body vigilance orientation (Vujanovic et al., 2008).
Eight manuscripts (16.67%) assessed combat or military types of trauma. Among these manuscripts, six included pain catastrophizing orientation (Aase et al., 2018; Alschuler & Otis, 2012; Ciccone & Kline, 2012; Outcalt et al., 2014; Tsur, Defrin, & Ginzburg, 2017; Tsur, Defrin, et al., 2018), three included AS-physical orientation (Raines, Capron, et al., 2017; Raines, Walton, et al., 2017; Tsur, Defrin, et al., 2018), one included fear of pain orientation (Tsur, Defrin, & Ginzburg, 2017), and no manuscripts included body vigilance orientation.
Six manuscripts (12.5%) assessed vehicle accident types of trauma. Among these manuscripts, six included pain catastrophizing (Andersen et al., 2016; Pedler et al., 2016; Ravn et al., 2019; Smith et al., 2016; Sullivan et al., 2009; Vaegter et al., 2018). None included AS-physical, fear of pain, or body vigilance. Three manuscripts (6.25%) assessed exposure to terror types of trauma. These manuscripts included AS-physical (Collimore et al., 2008; Farris et al., 2016; Mahaffey et al., 2017) and none included other orientation types. Three manuscripts (6.25% of manuscripts) assessed injury or brain injury type of trauma type. Two manuscripts included pain catastrophizing (Aase et al., 2018; Giummarra et al., 2017), and another manuscript included AS-physical (Zahradnik et al., 2009). None of these manuscripts included either fear of pain or body vigilance.
Only one manuscript (2.08%) assessed childhood trauma and included anxiety sensitivity orientation (Wilson & Newins, 2018). Four manuscripts (7.55%) assessed exposure to interpersonal trauma in adulthood types of trauma. Two included pain catastrophizing orientation (Tsur, Defrin, & Ginzburg, 2017; Tsur, Defrin, et al., 2018), three included AS-physical orientation type (Christiansen & Hansen, 2015; A. J. Lang et al., 2002; Tsur, Defrin, et al., 2018), one included fear of pain orientation type (Tsur, Defrin, & Ginzburg, 2017), and none included body vigilance orientation. Finally, one manuscript (2.08%) assessed campus shooting type of trauma (Boffa et al., 2016) and referred to anxiety sensitivity orientation.
Taken together, it is apparent that the literature is nonspecific with regard to the question of which trauma types may instigate an association between PTSD and orientation to bodily signals. Additionally, except for the interpersonal traumas during childhood or adulthood and the “various” traumas that may include interpersonal traumas, most of the research refers to exposure to type 1 traumatic events (i.e., a single traumatic incident), as opposed to type 2 (i.e., repeated traumatic incidents).
Research designs and reported findings
The review indicated that the majority of the manuscripts utilized a cross-sectional research design (n = 35; 72.92%). Among these cross-sectional designs, 15 manuscripts (31.25%) assessed the association between pain catastrophizing and trauma and/or PTSD, 20 (41.67%) assessed the association between AS-physical and trauma and/or PTSD, two assessed the association between fear of pain and trauma and/or PTSD (4.17%), and one (2.08%) assessed the association between body vigilance and trauma and/or PTSD.
Among cross-sectional design manuscripts, 28 (58.33%) reported findings inferring significant associations between orientation to bodily signals and PTSD. Six (12.5%) reported partially significant associations between orientation and PTSD; four of these manuscripts found an association between AS-physical and PTSD in simple correlations that were partially or fully nonsignificant when the other ASI dimensions were controlled for (A. J. Lang et al., 2002; Raines, Walton, et al., 2017; Vujanovic et al., 2007; Wilson & Newins, 2018). The ASI dimensions included social, cognitive, and physical concerns (Taylor et al., 2007). Considering that the social and cognitive dimensions do not refer to bodily manifestations, the inclusion of these dimensions is not relevant in assessing the link between orientation to bodily signals and trauma/PTSD. Another two cross-sectional manuscripts reported partially insignificant associations between orientation and PTSD; one reported findings whereby AS-physical was significantly correlated with PTSD. However, this correlation was no longer significant when depression was controlled for (Stanley et al., 2017). Another manuscript reported an association between PTSD and pain catastrophizing to be significant among women but not men (Grossi et al., 2000). Finally, one cross-sectional manuscript (2.08%) found insignificant findings, reporting that participants with PTSD did not exhibit higher AS-physical compared to participants without PTSD (McDermott et al., 2009).
Nine manuscripts (18.75%) used a longitudinal research design. Among the longitudinal manuscripts, five tested whether orientation to bodily signals predicted PTSD. Among these, three found that orientation did not significantly predict PTSD (Ciccone & Kline, 2012; Ravn et al., 2019; Sullivan et al., 2009), one reported that pain catastrophizing significantly predicted later PTSD (Andersen et al., 2016), and another reported that preshooting AS-physical significantly predicted postshooting PTSD (Boffa et al., 2016). Another four longitudinal manuscripts had various findings. One tested whether AS-physical mediated the link between sex and PTSD and found that AS-physical did not significantly mediate this association (Christiansen & Hansen, 2015). Another two studies, although longitudinal, did not examine the potential bidirectional prediction of orientation to bodily signals or PTSD (Pedler et al., 2016; Smith et al., 2016). Only one manuscript examined whether PTSD predicted later orientation to bodily signals and found that PTSD trajectories significantly predicted pain catastrophizing, AS-physical, and fear of pain (Tsur, Defrin, et al., 2018). Nevertheless, since orientation was only measured in the final time point, these results cannot imply causation.
Four studies utilized an experimental or intervention research design (8.33%). Among these manuscripts, one conducted a quantitative somatosensory assessment of pain perception and modulation (Defrin et al., 2015). This study found significant correlations between pain catastrophizing and PTSD symptoms. However, the experimental assessments did not examine these associations (Defrin et al., 2015). Another study assessed and found that AS-physical did not mediate the association between the intervention group and PTSD (Short et al., 2017). One study conducted a randomized controlled clinical trial of a brief somatic experiencing intervention. The analyses included an examination of the link between pain catastrophizing and PTSD at baseline and found a significant correlation (Andersen et al., 2017). Finally, in another study, the trauma film paradigm was conducted, indicating that AS-physical predicted greater post-traumatic reactions to the film over 1 week (Olatunji & Fan, 2015).
The findings imply that orientation to bodily signals is commonly referred to as a risk factor for PTSD and not a PTSD derivative. Considering that the predictability of orientation to bodily signals and PTSD received mixed findings, support for this perspective is limited. Additionally, it seems that only one longitudinal examination tested the potential process by which PTSD contributed to the development of a catastrophic and frightful orientation to bodily signals (Tsur, Defrin, et al., 2018). As such, although cross-sectional indications of a link between orientation to bodily signals were quite extensive, examinations addressing potential causality are limited. Therefore, the temporal associations between PTSD and the orientation to bodily signals cannot be drawn.
As can be seen in the Online Appendix, most manuscripts reported weak to moderate effect sizes to associations found between PTSD and orientation to bodily signals. Specifically, 24 manuscripts reported weak effect sizes, while 19 manuscripts reported moderate effect sizes.
Associations between orientation to bodily signals and different PTSD clusters
According to the Diagnostic and Statistical Manual of Mental Disorders-V (American Psychiatric Association, 2013), PTSD is included in “trauma and stressor-related disorders.” The criteria of PTSD can be seen in several clusters: intrusion, avoidance, arousal, and negative alterations in cognitions and mood.
The majority of the manuscripts included in this review assessed PTSD as a unified construct (n = 40; 83.33%), thus not including examinations of associations between orientation to bodily signals and divergent PTSD clusters. However, eight manuscripts (16.67%) did include such examinations, and two reported findings showing that pain catastrophizing was significantly associated with all PTSD clusters (López-Martínez et al., 2014; Martin et al., 2010). Five manuscripts reported that anxiety sensitivity was significantly associated with all PTSD clusters (Asmundson & Stapleton, 2008; Bakhshaie et al., 2015; Mahaffey et al., 2017; Martin et al., 2010; Stanley et al., 2017). Another two manuscripts found that orientation was associated with some PTSD clusters; one tested long-term PTSD over more than 30 years and found that hyperarousal symptoms were significantly associated with pain catastrophizing and AS-physical and that intrusion symptoms were associated with pain catastrophizing (Tsur, Defrin, et al., 2018). Another manuscript reported that AS-physical was correlated with intrusion, hyperarousal, and dysphoria PTSD symptoms but not with avoidance symptoms (Raines, Walton, et al., 2017). Thus, the review indicates that research on differential associations between orientation to bodily signals and PTSD clusters is limited, making it difficult to comprehend whether orientation to bodily signals is symptom-cluster specific. Nevertheless, although limited, it is apparent that preliminary investigations were mostly consistent regarding the associations between orientation to bodily signals and hyperarousal symptoms, as well as intrusion symptoms to a lesser extent.
Associations between two or more orientation types
Most manuscripts utilized only one manifestation of orientation to bodily signals. Only three (6.25%) included more than one type of orientation to bodily signals; in two manuscripts, the associations between the studies’ two orientation types were not reported (Tsur, Defrin, & Ginzburg, 2017; Tsur, Defrin, et al., 2018). Only one manuscript reported an assessment of the association between two types of orientation to bodily signals, indicating that AS-physical correlated significantly with pain catastrophizing (Martin et al., 2010). Although other studies did test associations between two or more orientation types, it was determined that they did not meet the inclusion criteria for this review as the contexts of trauma and PTSD were not included. Consequently, it is not possible to assess the extent to which types of orientation to bodily signals overlap with each other or are linked in the context of trauma.
Diversity as it applies to the manuscripts included in the review
The number of women and men participants varied in the reviewed manuscripts, with a mean percentage of women of 54.16% (SD = 29.02). The majority of the samples were recruited in the United States (n = 27; 56.25%) and Europe (n = 10; 20.83%). Other places included Canada (n = 5; 10.42%), Australia (n = 3; 6.25%), and Israel (n = 3; 6.25%). These findings indicated that research on the association between orientation to bodily signals and trauma/PTSD has been conducted mainly in Western cultures. As such, this research realm fails to address the issues of cultural diversity.
Discussion
The current study aimed to review previous findings that inferred a potential link between PTSD and the interpretation of bodily signals as seen through several orientation manifestations. The results indicated that the majority of the manuscripts provided consistent support for the link between PTSD and the tendency to interpret physical symptoms and other bodily signals as catastrophic and frightful. Furthermore, the findings showed that various orientation manifestations included in the review were most often tested alone. Thus, an inclusive indication of the fundamental ways individuals may interpret their bodily signals following exposure to traumatic events was lacking. These findings call for the need to conceptually synthesize the different orientation manifestations into a comprehensive theoretical construct. As such, the concept of post-traumatic orientation to bodily signals is hereby proposed as an umbrella term, reflecting the tendency to interpret bodily signals as catastrophic and frightening following exposure to trauma.
The findings of this review provided significant evidence for a link between PTSD and several orientation manifestations following various types of trauma and within various populations. The majority of the manuscripts did not specify an intent to test the association between orientation to bodily signals and PTSD and did not conceptualize it as orientation to bodily signals. Rather, they implemented a construct related to perception and/or coping with a chronic health-related condition (Sullivan, 2012) or a risk factor for PTSD (Olatunji & Fan, 2015; Short et al., 2017). Nevertheless, the findings highlighted the potential relevancy of post-traumatic orientation in understanding the experience of the body following exposure to trauma.
According to the dual representation model (Brewin, 2011; Brewin et al., 1996), traumatic memories are often stored in implicit memory, lacking a coherent connection with the rest of the autobiographical explicit memory. As such, somatosensory memories of the traumatic experience are often fragmented and involve intrusive reexperiencing of the traumatic event. Van der Kolk (1994, 2014) encapsulated these somatic manifestations as the “somatic memory.” He further postulated that they might result in distrust and estrangement from the body, destroying the adaptive experience in the body as a safe entity. From another standpoint, it has been suggested that trauma has the potential to shatter basic world assumptions regarding benevolence, meaningfulness of the world, and self and others as worthy (Janoff-Bulman, 2010). Integrating this idea with the current understandings regarding the experience of the body following trauma, trauma may also shatter the basic assumptions regarding the body as a well-functioning, comforting, and safe entity for the self to be embodied/placed/situated in. Danger, in this perspective, is not limited to external factors but also embodied in the basic experience of the body (Tsur, Defrin, et al., 2018). Simply put, it is postulated that post-traumatic orientation to bodily signals may presumably reflect the shattering of assumptions regarding one’s own body.
The current study provides a conceptual bridge between the above theoretical understandings and the reviewed empirical findings. Specifically, the present review denotes the extensive indications of a negative orientation to the body following trauma, as seen through pain catastrophizing, AS-physical, fear of pain, and body vigilance. Therefore, the consistent associations across various orientation manifestations suggest a fundamental tendency to orient to bodily signals as catastrophic and frightful, framed through the construct of post-traumatic orientation to bodily signals. Presumably, post-traumatic orientation to bodily signals is generated by the processes described in theory and presented above as well as reflected in the findings arising from this review.
Nevertheless, although the current review provides initial evidence for the construct of post-traumatic orientation to bodily signals, it also illuminates several methodical and conceptual caveats in literature. First, most manuscripts were conducted using cross-sectional examinations. Thus, initial evidence of an association between PTSD and orientation to bodily signals was provided; however, causality cannot be inferred. The paucity of longitudinal research designs impedes the ability to draw the temporal links between PTSD and orientation to bodily signals and, therefore, indicates a lack of knowledge in this field. Of the few manuscripts that tested longitudinal directions of associations or utilized experimental research designs, the majority referred to AS-physical as a risk factor for PTSD (Andersen et al., 2016; Boffa et al., 2016; Olatunji & Fan, 2015; Short et al., 2017). Only one manuscript assessed whether long-term PTSD was correlated with pain catastrophizing and AS-physical and found significant results, although orientation measures were only tested in the final time point (Tsur, Defrin, et al., 2018). This pattern of findings may reflect a theoretical stance in which orientation to bodily signals is not hypothesized to reflect potential derivatives of trauma and PTSD but rather is suspected to be a risk factor for its development. Thus, more emphasis should be dedicated to assessing the causality of PTSD as implicated in post-traumatic orientation to bodily signals.
Relatedly, the findings of this review demonstrated that the existing literature is generally unspecific with regard to the type of trauma that may be linked with orientation to bodily signals. Particularly, more than half of the studies assessed exposure to various trauma types, thus obstructing the ability to indicate whether certain types of traumatic events are more prone to be implicated in a post-traumatic orientation to the body. Among the other half of manuscripts, which assessed specific types of traumatic events, the majority referred to type 1 traumatic events, such as car accidents (Pedler et al., 2016; Ravn et al., 2019; Smith et al., 2016; Vaegter et al., 2018), combat (Outcalt et al., 2014; Raines, Capron, et al., 2017; Raines, Walton, et al., 2017), and injury or brain injury (Giummarra et al., 2017; Zahradnik et al., 2009). Only five referred to interpersonal trauma during adulthood, including bank robbery and potentially type 2 traumatic events of previous sexual trauma (Christiansen & Hansen, 2015), intimate partner violence (A. J. Lang et al., 2002), torture (Tsur, Defrin, & Ginzburg, 2017; Tsur, Defrin, et al., 2018), or childhood trauma (Wilson & Newins, 2018). From a developmental standpoint, abusive relationships are characterized by parallel dynamics of nurturing and injuring (physically or mentally), with the threat transpiring from a supposedly safe environment (Schuder & Lyons-Ruth, 2004; Van der Kolk, 2017). This discrepancy reflects a severely pathological bond, often incorporating a sense of betrayal. This has been shown to be deeply engraved in the fundamental experience of the self and body (Freyd et al., 2005; Herman, 1997), as encapsulated in developmental trauma (Ford et al., 2018) and complex PTSD (Cloitre et al., 2018; Van der Kolk, 2017). Further investigations are needed to underscore the divergent effects of various traumas for the orientation toward the body. Particularly, more research is needed to better understand the magnitude of the associations between exposure to type 1 and type 2 traumatic experiences and orientation to bodily signals. Additionally, further research should clarify the underlying mechanisms of the path from exposure to a traumatic event to PTSD/CPTSD to orientation to bodily signals.
Additionally, this review’s findings showed that most studies assessed PTSD as a unidimensional phenomenon, thus lacking diverse associations between orientation to bodily signals and the different PTSD clusters. It has been suggested that hyperarousal symptoms inherently involve bodily sensations. This presumably reflects the “somatic channel” by which PTSD is implicated in orientation to the body (Tsur, Defrin, et al., 2018). This somatic channel may be linked to the psychophysiology of PTSD, as seen in the activation of the HPA axis expressed through hyperarousal symptoms (Wessa et al., 2006). Indeed, it seems that the manuscripts reviewed in this study showed that hyperarousal was significantly associated with orientation to bodily signals and, to a lesser extent, also intrusion (Raines, Capron, et al., 2017; Tsur, Defrin, et al., 2018). Nevertheless, further research is needed to assess whether and which PTSD symptoms hinder the experience of the body as manifested in the orientation toward the body. Furthermore, considering the essential role of the experience of the body within interpersonal relationships (Lyons-Ruth et al., 1998; Ogden, 2018), research should also explore the links between orientation to bodily signals and CPTSD.
Only one manuscript tested and reported the associations between two types of orientation to bodily signals (Martin et al., 2010). The current review demonstrated that orientation variables were often tested separately, reflecting a specific and rather narrow dimension of orientation to bodily signals. However, extensive literature not in the field of trauma has provided abundant evidence for the associations between different types of orientation to bodily signals (Esteve & Camacho, 2008; McWilliams & Asmundson, 2007; Somers et al., 2009; Vancleef et al., 2006). This understanding signifies the need to combine several indications of orientation to bodily signals in research to attest to the implications of trauma for the interpretation of body signals from a more inclusive stance. Moreover, these findings point to the need to develop a comprehensive measure for post-traumatic orientation to the body. Such a scale would pave the way for future empirical endeavors and potentially enhance the applicability of these understandings to clinical practice and policy.
The complex correspondence between biopsychosocial processes as seen in the perception of the body following exposure to potentially traumatic events and PTSD has been exhaustively explored. However, this has yet to be fully established. Afari et al. (2014) demonstrated that exposure to potentially traumatic events and PTSD could be associated with somatic complaints that lack a medical explanation or what is considered functional somatic syndromes. As previously suggested by Sharp and Harvey (2001), the ways in which individuals interpret bodily signals may play a significant role in uncovering the complex intercorrelations of mental and physical manifestations of post-traumatic proclivities, which serve as an exacerbating factor. Recently, a new mind–body four-cluster model has been proposed highlighting the significant role of the interpretation of bodily signals in stress-exacerbated diseases and functional somatic syndromes (Ezra et al., 2019). Despite needing further examination, the currently established understandings stress the potential role of the interpretation of bodily signals in uncovering biopsychosocial morbidities following exposure to potentially traumatic events.
The findings further showed that cultural contexts and circumstances have rarely been included in the examination of the orientation to the body following trauma. It has been proposed that the binary Cartesian differentiation between body and mind, embraced by Western cultures, may impede the perception of the body as an integral part of the self. Instead, it is implicated in the experience of the body as a “vehicle” in service of the “self” (Mehling et al., 2009; Mehling et al., 2012). Hence, somatic sensations are not viewed as integral to the mental state or experience but rather as “medical” symptoms to be medically tested and treated. Presumably, a less dichotomized perception of the mind–-body association, often held by non-Western cultures, may affect the orientation, in general, and following potentially traumatic events, in particular. Therefore, further research should be dedicated to investigating the cultural context of post-traumatic orientation to bodily signals.
Regarding diversity in gender, the findings pointed to gender differences in post-traumatic orientation to bodily signals. However, it is possible that objectification processes, imposed on women as well as men, although differently, may intervene in the ways individuals orient to their body (Calogero et al., 2011; Noll & Fredrickson, 1998). Menstrual cycles, childbearing, and breastfeeding may also affect these processes. Indeed, one of the reviewed manuscripts found that PTSD was associated with pain catastrophizing among women but not men (Grossi et al., 2000). However, another study found that AS-physical did not mediate the link between gender and PTSD (Christiansen & Hansen, 2015). Considering the limited examinations of gender differences, future investigations should include the cultural and biological factors that play a role in the expressions of orientation toward the body as they are associated with PTSD.
Limitations
To the best of our knowledge, the current literature review is the first to systematically synthesize research findings inferring the ways PTSD is linked with post-traumatic orientation to bodily signals. Most manuscripts reported weak or moderate effect sizes between PTSD and the orientation to bodily signals. Nevertheless, one while these effect sizes support the concluded association between PTSD and orientation, it is recommended that a meta-analysis be conducted as a next step. Nevertheless, several limitations should be considered when interpreting the results. First, the selection of included orientation types aimed to be exhaustive and inclusive. However, in light of the lack of previous conceptualizations of this phenomenon, other variables should be considered as possibly reflecting orientation to bodily signals. Second, this review discusses orientation to bodily signals resulting from PTSD. Nevertheless, particularly when considering the paucity of longitudinal research designs, orientation to bodily signals may also precede PTSD and play a role in increasing the risk of PTSD following exposure to potentially traumatic events. Third, the current analysis was based on three large databases (PsycNet, PubMed, and ScienceDirect), which include published research from all disciplines. Nevertheless, one should consider that other relevant manuscripts may not have been found using this approach. Other limitations are embedded in methodological aspects of the reviewed manuscripts. Particularly, as the majority of the manuscripts were based on self-reports, some bias may have affected their results and our conclusions. Additionally, as previously noted, most manuscripts utilized cross-sectional research design. Therefore, this limits the ability to ground causal relationships between PTSD and orientation to bodily signals. Furthermore, more emphasis should be given to contextual factors that may intervene in the trauma-PTSD-orientation to body signals links.
Finally, some limitations may arise from the use of an umbrella term to conceptualize interpretations of bodily signals, as proposed in this study. On the one hand, using such a term may impede the ability to differentiate between divergent mechanisms involved in the interpretation of bodily signals. On the other hand, using particular and specific constructs may interfere with the ability to draw broader understandings, such as when using an umbrella term. Therefore, it is recommended that future investigations utilize both broad and specific conceptualizations of orientation to bodily signals manifestations.
Implications for Practice and Policy
A summary of practice, policy, and research implications is presented in Table 2. Findings revealed that various forms of orientation to bodily signals are associated with decreased self-rated health (Weston & Jackson, 2018), poorer health-related quality of life (McPeak et al., 2018), and increased utilization of health services (Olatunji et al., 2007). Some of the orientation manifestations have also been found to be linked with the etiology and coping regarding various debilitating physical morbidities, such as chronic pain (Burns et al., 2015), irritable bowel syndrome (Sherwin et al., 2017), asthma (Avallone et al., 2012), cancer (Jones et al., 2014), and premature aging (Tsur, Levin, et al., 2018). Enormous endeavors are dedicated to diagnose, prevent, and treat chronic morbidity following trauma (Ferry et al., 2015) and, therefore, there is a need to uncover its psychosocial connections as seen in post-traumatic orientation to bodily signals.
Summary of Study Implications.
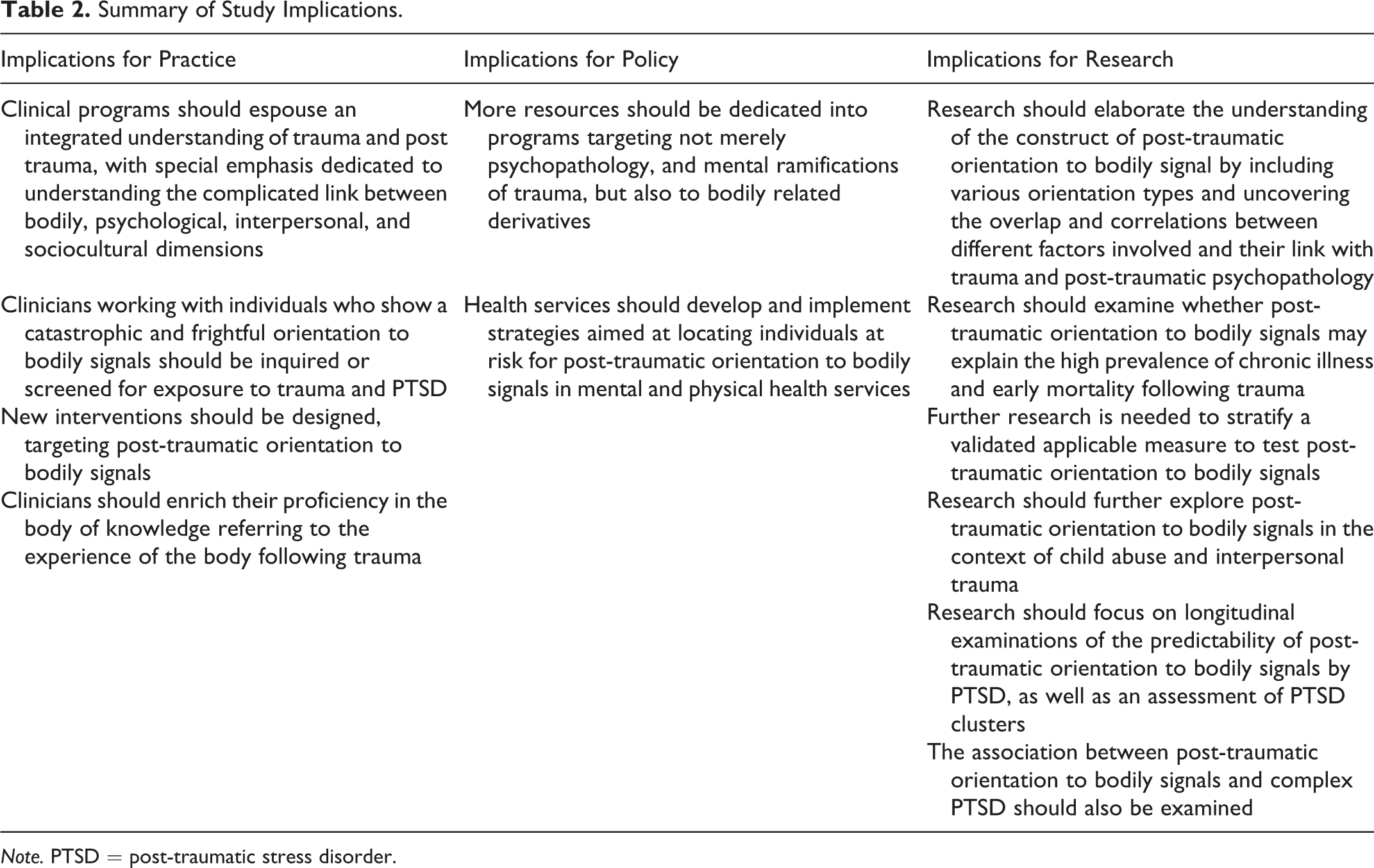
Note. PTSD = post-traumatic stress disorder.
Additionally, psychosocial and medical settings are constantly busy providing treatment and care to individuals who report increased somatic symptoms, poor health, and extensively utilize healthcare services. Although medical services continue to progress, the understanding of psychosocial factors involved in poor health-related well-being is still lacking. This review provides a framework for practitioners and policymakers to observe, understand, and treat individuals who have faced trauma by conceptualizing the post-traumatic orientation to bodily signals. Furthermore, a growing body of knowledge has emphasized the bodily experience as representing a core repercussion of trauma and PTSD (Brewin, 2011; Tsur, Defrin, et al., 2018; Van Der Kolk, 2014). Therefore, the proposed conceptualization of post-traumatic orientation to bodily signals may assist practitioners in better understanding and targeting the experience of the body following trauma and its implications for recovery.
Supplemental Material
Supplemental Material, sj-pdf-1-tva-10.1177_15248380211025237 - Post-Traumatic Orientation to Bodily Signals: A Systematic Literature Review
Supplemental Material, sj-pdf-1-tva-10.1177_15248380211025237 for Post-Traumatic Orientation to Bodily Signals: A Systematic Literature Review by Noga Tsur and Ada Talmon in Trauma, Violence, & Abuse
Footnotes
Acknowledgment
Sincere thank-you to Ms. Laura Crompton MSW for the language editing of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.