
Abstract
Objective:
Sexual assault is associated with higher rates of posttraumatic stress disorder (PTSD) than other traumas, and the course of PTSD may differ by trauma type. However, the course of PTSD after sexual assault has not been summarized. The aim of this meta-analysis was to identify the prevalence and severity of PTSD and changes to the average rate of recovery in the 12 months following sexual assault.
Method:
Authors searched four databases for prospective studies published before April 2020 and sought relevant unpublished data. Eligible studies assessed PTSD in at least 10 survivors of sexual assault in at least two time points, starting within 3 months postassault. Random effects linear-linear piecewise models were used to identify changes in average recovery rate and produce model-implied estimates of monthly point prevalence and mean symptom severity.
Results:
Meta-analysis of 22 unique samples (N = 2,106) indicated that 74.58% (95% confidence interval [CI]: [67.21, 81.29]) and 41.49% (95% CI: [32.36, 50.92]) of individuals met diagnostic criteria for PTSD at the first and 12th month following sexual assault, respectively. PTSD symptom severity was 47.94% (95% CI: [41.27, 54.61]) and 29.91% (95% CI: [23.10, 36.73]) of scales’ maximum severity at the first and 12th month following sexual assault, respectively. Most symptom recovery occurred within the first 3 months following sexual assault, after which point the average rate of recovery slowed.
Conclusions:
Findings indicate that PTSD is common and severe following sexual assault, and the first 3 months postassault may be a critical period for natural recovery.
Sexual assault—defined as unwanted, nonconsensual sexual contact achieved via force, incapacitation, and/or coercion—is a common form of trauma. Epidemiological data indicate that, in their lifetime, 12.3%–13.5% of women and 0.9%–1.6% of men in the United States experience forced penetration, and 8.0%–11.0% of women and 0.6%–5.5% of men experience alcohol/drug-facilitated penetration (Black et al., 2011; Smith et al., 2018). In addition, 12.5%–16.0% of women and 2.0%–2.4% of men experience lifetime sexual coercion (Black et al., 2011; Breiding et al., 2014; Smith et al., 2018).
Sexual assault is associated with heightened risk of posttraumatic stress disorder (PTSD; Dworkin et al., 2017), which is characterized by reexperiencing (i.e., reliving the event), avoidance behavior, negative changes to thoughts and emotions, and hyperarousal (American Psychiatric Association [APA], 2013). Studies assessing PTSD in relation to any trauma exposure (not necessarily due to sexual assault) indicate that 36% of sexual assault survivors meet criteria for lifetime PTSD (Dworkin, 2020) and 12%–25% meet criteria for current PTSD (Kilpatrick et al., 2007; Resnick et al., 1993; Zinzow et al., 2012).
Immediately following sexual assault, the majority of survivors experience PTSD symptoms (Rothbaum et al., 1992; Steenkamp et al., 2012). Prospective studies demonstrate that, over the months following sexual assault, many survivors experience at least some natural remission of their initial symptoms (e.g., Gutner et al., 2006; Riggs et al., 1995; Rothbaum et al., 1992), and PTSD is only diagnosed when sufficient symptoms are present for at least 1 continuous month (APA, 2013). Accordingly, PTSD is considered to be a disorder of nonrecovery from initial symptoms (Monson & Friedman, 2006).
Compared to other potentially traumatic events (e.g., physical assault, accidents, natural disasters), for which only a minority of survivors experience significant levels of PTSD (Galatzer-Levy et al., 2018; Lowe et al., 2020), sexual assault appears to carry relatively greater risk for PTSD (Brewin et al., 2000; Dworkin, 2020; Kessler et al., 2014; Kilpatrick et al., 2003) and may be associated with unique trajectories of recovery. According to cognitive-behavioral theories of PTSD, negative attributions regarding the cause and meaning of trauma (e.g., self-blame, believing that the world is extremely dangerous) and avoidance of trauma reminders (e.g., thoughts/feelings associated with the assault, situations that remind the individuals of the assault) prevent natural recovery from PTSD symptoms (Ehlers & Clark, 2000; Foa & Kozak, 1986; Foa et al., 2006; Resick et al., 2017). Stigma associated with sexual assault (e.g., victim blame; Kennedy & Prock, 2018; Lebowitz & Roth, 1994) may contribute to inaccurate or unhelpful negative attributions or encourage avoidance of discussing the assault with others (Kelley et al., 2009; see for exception Smith et al., 2016), ultimately obstructing PTSD recovery.
Two prior meta-analyses of prospective studies have summarized the prevalence of PTSD within the first year after exposure to a range of potentially traumatic events, although neither focused specifically on sexual assault. First, Hiller et al. (2016) conducted a meta-analysis of recovery from childhood trauma involving 27 peer-reviewed studies and one unpublished data set (including three studies that sampled at least some children exposed to interpersonal violence). The aggregate prevalence of PTSD was 21% at 1 month, 15% at 3 months, 12% at 6 months, and 11% at 1 year (Hiller et al., 2016). Analyses of the subset of studies that examined reductions in symptomatology identified that the greatest reductions in symptom severity occurred between 1 and 3 months, although there was a greater reduction in prevalence of PTSD diagnosis from 3 to 6 months (32%) than 1 to 3 months (17%). Second, by pooling item-level data from 13 studies of acutely hospitalized trauma survivors (7.7% of whom were hospitalized following interpersonal violence), Qi et al. (2018) found that PTSD prevalence ranged from 3% to 62% at studies’ baseline assessment; 4%–38% at studies’ first follow-up assessment, and 4%–27% at studies’ third follow-up assessment. These wide prevalence ranges reflected the inclusion of studies that explicitly selected participants on the basis of elevated symptom severity as well as studies that enrolled participants regardless of symptom severity. Results were not presented as a function of time since trauma.
Similar results have been identified in systematic reviews of published prospective studies. Santiago et al. (2013) conducted a systematic review of 58 published studies of various trauma types. Although this review included mixed physical and sexual assault samples, no studies specific to sexual assault were included. Consistent with the notion of natural recovery, they reported decreases in the median prevalence of PTSD between 1 month (28.8%) and 3 months (17.8%) posttrauma, followed by a stabilization in prevalence through 12 months (17.0%; Santiago et al., 2013). Differences in trajectories were observed for different types of trauma: whereas PTSD prevalence decreased over time for nonviolent traumas (20.1% at month 1 and 14.0% at month 12), the median prevalence increased from 11.8% at Month 1 to 23.3% at Month 12 for violent traumas. More recently, MacGregor and colleagues (2019) conducted a systematic review of 10 published studies of sexual assault recovery in young people (aged 10–24). PTSD prevalence was 65%–88% at Month 1 (based on two studies), 35%–71% at 3 months (based on three studies), and 58%–60% at Month 12 (based on two studies).
These meta-analyses and systematic reviews generally provide evidence for the presence of high levels of initial posttrauma symptoms that tend to stabilize by the end of the first year posttrauma. However, they have two major limitations. First, although the Santiago and Hiller reviews found that large reductions in PTSD symptomatology occurred between 1 and 3 months posttrauma, neither statistically determined if there was a time point at which the average rate of recovery slowed (Hiller et al., 2016; Santiago et al., 2013). This information would be critical to inform the timing of early assessment and intervention efforts. Second, despite evidence that sexual assault is more strongly associated with PTSD than other forms of trauma (Brewin et al., 2000; Dworkin, 2020; Kessler et al., 2014; Kilpatrick et al., 2003), no prior work has quantitatively summarized the natural course of PTSD recovery specifically for adolescent and adult sexual assault survivors (i.e., via meta-analysis). Meta-analytically aggregating across samples would clarify average rates of recovery in the acute aftermath of sexual assault, which would in turn inform clinical practice and help to contextualize individual responses.
Thus, the goal of this study was to characterize the average month-to-month rates of PTSD in adolescents and adults in the year following sexual assault. We aimed to use random effects meta-analysis to (1) statistically summarize the point prevalence and average symptom severity of PTSD in the 12 months following sexual assault and (2) empirically test whether there is a point at which the average rate of recovery changes. Building on prior reviews of PTSD following other types of trauma, we focused specifically on samples exposed to adolescent and/or adult sexual assault. We also sought to address the reliance of prior reviews on published literature by seeking unpublished data to supplement published reports.
Method
Procedures
We undertook an extensive search strategy to identify published and unpublished literature on this topic. First, we searched PsycINFO, PsycArticles, Academic Search Complete, and PubMed on November 20, 2018, and April 6, 2020, using the following search terms and Boolean operators: (“posttraumatic stress” OR “post-traumatic stress” OR ptsd) AND (“sexual assault” OR rape OR “sexual violence” OR “sexual victimization”) AND (prospective OR recent OR month* OR year* OR week* OR trajector*). This search yielded 929 unique results, which were each independently subject to abstract and/or full-text review by two authors using the eligibility criteria (discussed next). Kappa values for eligibility decisions of “yes” versus “maybe” or “no” ranged from .82 to .87 across coders. Disagreements were discussed collaboratively, and 58 articles were ultimately retained for coding from this step. Second, the first author reviewed the citations of the articles retained for coding and the citations of prior reviews on related topics (i.e., Bryant, 2011; Dworkin et al., 2017; Guay et al., 2019; Forneris et al., 2013; MacGregor et al., 2019), and the third author reviewed a database of articles collected for a prior review, which yielded an additional 12 -articles. Third, requests for unpublished data were posted to relevant listservs, which did not yield any additional studies. Finally, when full information was not included in a published report, we emailed authors to request supplemental PTSD data, and alerted these authors that we sought any other unpublished data sets available to them. We ultimately sent 29 emails requesting data, 13 of which yielded supplemental data, but no previously unidentified data sets were obtained through this step.
Eligible studies were those where (1) results were reported in English; (2) at least 10 survivors of sexual assault were included (we contacted authors to request sexual-assault–specific data for mixed-trauma samples and did not include studies when we could not obtain these data); (3) the sample included at least some survivors who were not receiving an active treatment meant to reduce PTSD as a part of study participation (we contacted authors to request data for control conditions in clinical trials and did not include studies when we could not obtain these data); (4) survivors were recruited because they experienced a past-year trauma; (5) PTSD symptoms were first assessed within 3 months of sexual assault; (6) PTSD was assessed prospectively; (7) the sample was not primarily comprised of children (defined as a sample mean age of 13 years old or younger); and (8) the study did not exclude participants on the basis of symptom-level cutoffs (i.e., the study did not have a PTSD symptom maximum or minimum as an inclusion criterion). From the 70 studies that met these criteria, we selected the 22 unique samples in which relevant outcome data could be obtained (i.e., the percent of sexual assault survivors with PTSD or means and standard deviations on a measure of PTSD at multiple time points were published or provided by authors).
Data Extraction
All articles were coded independently by at least two coders. Discrepancies were resolved by group discussion.
Effect sizes
For studies that reported proportions, we coded the n with PTSD, the proportion with PTSD, and the sample size (N) on which this proportion was based. When N was not reported for a time point, we carried forward the last available N from a prior time point and calculated n based on the reported proportion with PTSD at that time point. 1 Consistent with recommendations for meta-analyses of single proportions (Schwarzer et al., 2019), arcsine square root transformations were used for analyses to normalize and stabilize sampling distributions. Transformed proportions were back-transformed to percentages (range: 0–100) for presentation of model-predicted values using the formula (sin(transformed proportion))2 × 100.
For studies that reported means, we recorded the mean and its associated standard deviation, the scale minimum and scale maximum, and the sample size on which the mean was based (or the last available N from a prior time point). We rescaled all means to a 0–1 scale using the formula: M rescaled = (M raw − scale minimum)/(scale maximum − scale minimum). Rescaled variance was calculated as v rescaled = SD 2 raw/(n(scale maximum − scale minimum)2). We multiplied model-predicted mean scores by 100% when presenting month-by-month point estimates to represent a percent of maximum severity.
Time since assault
Each assessment time point was coded in units of months since assault. When assessment time points were reported in the source in a unit smaller than months (i.e., hours, days, or weeks), we transformed this information into a ratio variable representing months since assault. For assessments that were stated to be performed within a certain time frame, we took the midpoint of that time frame (e.g., assessments that were performed within 1 month post-assault were coded as 0.5 months post-assault).
Descriptive variables
With regard to study methods, we coded the type of source (e.g., peer-reviewed journal article, dissertation) in which the study was made publicly available, even when unpublished data were obtained; the country of data collection; the site from which the majority (at least 67%) of participants were recruited; the name of the PTSD measure; whether PTSD point prevalence was determined by a cut score or meeting Diagnostic and Statistical Manual of Mental Disorders (DSM) diagnostic criteria (e.g., based on the number of symptoms in clusters B, C, and D in the DSM, Fourth Edition [DSM-IV]; APA, 2000); the DSM version on which the PTSD measure was based; and whether an interview or self-report measure was used to assess PTSD. The following sample characteristics were coded: the percent of participants who were women, participant mean age, the majority (>67%) racial composition of samples in the United States, and the percent of participants with a prior history of sexual assault. With regard to characteristics of the index assault, we coded the percent of participants presenting with assaults involving alcohol/drug use by the survivor, weapon use by the perpetrator, physical injury, a stranger perpetrator (i.e., unknown to the survivor), and a police report. Finally, attrition was calculated as the percent reduction in sample size at each follow-up time point relative to the N at baseline. Attrition was not coded for two samples that presented outcomes only for the subsample of individuals who completed all study visits and one sample that enrolled participants in an ongoing manner after baseline.
Study quality
Methodological quality of studies was rated using a nine-item adapted version of the Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies (National Heart, Lung, and Blood Institute, 2014; see Online Appendix A).
Analyses
Analyses were conducted in R Version 3.6.3 (R Core Team, 2020). We employed a multilevel modeling approach to the meta-analysis using the package metafor (Viechtbauer, 2010). All models used inverse-variance weights, which is a strategy to give more weight to more precise effect sizes (e.g., those obtained from larger studies). We first undertook a process of comparing models to select the most appropriate models. The method used to compute the values for the parameters in these models (e.g., summary estimates and variances) was maximum likelihood estimation, which maximizes the likelihood that the model parameters could have generated the observed data (i.e., the effect sizes obtained from studies included in the analysis). We selected models by comparing their fit statistics (e.g., −2 log likelihood, information criteria) against each other and selecting the best fitting model. The method used to compute the values for the parameters in our final models was restricted maximum likelihood estimation, which is a variant of maximum likelihood estimation that reduces the risk of bias that can arise with small sample sizes.
Results
Descriptive Statistics
A total of 22 unique samples representing 2,106 participants met eligibility criteria and were included in analyses (see Table 1 for full sample characteristics; the full data set and corresponding syntax and output are available in Online Appendices B & C, respectively). The majority (19 samples) was published in peer-reviewed journal articles, two samples were only represented in dissertations, and one sample was only reported in a government-funded report. Across these samples, 75 effects were computed for PTSD diagnostic point prevalence (including 26 unpublished effects) from 20 samples, and 57 effects were computed for average symptom severity (including 42 unpublished effects) from 17 samples.
Characteristics of Samples Included in Meta-Analysis.
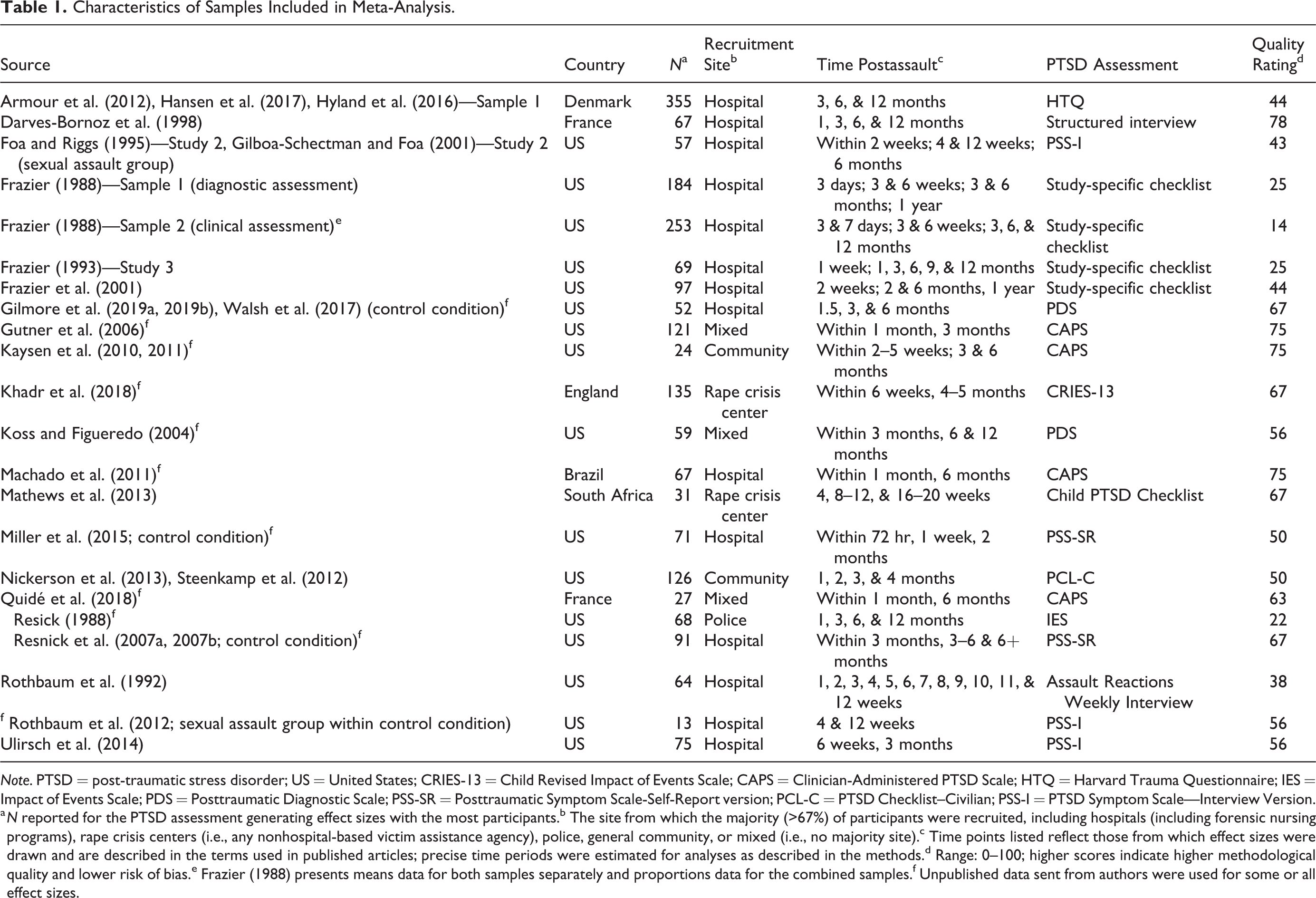
Note. PTSD = post-traumatic stress disorder; US = United States; CRIES-13 = Child Revised Impact of Events Scale; CAPS = Clinician-Administered PTSD Scale; HTQ = Harvard Trauma Questionnaire; IES = Impact of Events Scale; PDS = Posttraumatic Diagnostic Scale; PSS-SR = Posttraumatic Symptom Scale-Self-Report version; PCL-C = PTSD Checklist–Civilian; PSS-I = PTSD Symptom Scale—Interview Version.
a N reported for the PTSD assessment generating effect sizes with the most participants.b The site from which the majority (>67%) of participants were recruited, including hospitals (including forensic nursing programs), rape crisis centers (i.e., any nonhospital-based victim assistance agency), police, general community, or mixed (i.e., no majority site).c Time points listed reflect those from which effect sizes were drawn and are described in the terms used in published articles; precise time periods were estimated for analyses as described in the methods.d Range: 0–100; higher scores indicate higher methodological quality and lower risk of bias.e Frazier (1988) presents means data for both samples separately and proportions data for the combined samples.f Unpublished data sent from authors were used for some or all effect sizes.
Study quality
As indicated in Table 1, study quality ratings ranged from 14 to 78 on a 0–100 scale (M = 52.59, SD = 18.95; higher ratings indicate superior quality). Common issues with study quality (Online Appendix A) were participation-related issues (low participation rates, attrition, lack of sample size justification or power description) and lack of standardized measures.
Study methods
Most samples (72.7%; n = 16) were recruited in the United States. The most common recruitment site (for 63.6% of samples; n = 14) was a hospital, including hospital-based sexual assault services (e.g., during a sexual assault medical forensic exam); other recruitment sites were the general community (n = 2), rape crisis centers and other nonhospital-based victim assistance agencies (n = 2), the police (n = 1), or multiple sites (n = 3). PTSD was assessed by interview in 14 samples and self-report in eight samples. All PTSD assessments were based on the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) or earlier (Diagnostic and Statistical Manual of Mental Disorders, Third Edition [DSM-III] 2 : n = 4; DSM-III-R: n = 4; DSM-IV or DSM-IV-TR: n = 14). Of the 20 samples with PTSD diagnostic point prevalence reported, this was based only on cut scores in two samples and only on diagnostic criteria in 17 samples; one additional sample provided separate frequencies for PTSD point prevalence according to both scoring approaches.
Sample and assault characteristics
Race/ethnic composition was coded for U.S. samples only. Among the 15 U.S. samples with information about racial/ethnic composition, 40.0% (n = 6) were at least two-thirds majority White, 20.0% (n = 3) were at least two-thirds majority Black/African American, and the remaining 40.0% (n = 6) had no majority race or ethnic group. Sample average age ranged from 13.5 to 35.6 (M = 26.6; SD = 5.4). Additionally, 81.0% (n = 17) of samples consisted exclusively of participants who identified as women. Information about proportion of the sample who had a history of sexual assault prior to the recent sexual assault was available for nine samples and ranged from 10.3% to 76.9% (M = 43.7%, SD = 19.2%).
Sample-level characteristics of the index sexual assault were coded when available. On average, across samples with relevant information reported, the sexual assault occurred while the survivor was under the influence of drugs or alcohol in 39.7% of cases (SD = 14.7%; based on n = 7 samples). The sexual assault was perpetrated by a stranger in 41.2% of cases (SD = 17.2%; based on n = 13 samples). Additionally, the sexual assault involved a weapon in 25.7% of cases (SD = 13.9%; based on n = 5 samples), and the sexual assault resulted in physical injury for 63.6% of survivors (SD = 18.2%; based on n = 7 samples). Finally, 76.1% of participants made a police report for the sexual assault (SD = 31.8%; based on n = 6 samples).
Publication Bias
We examined publication bias in two ways. First, we compared published to unpublished effects at 1, 3, and 6 months postassault (due to low numbers of effects at other months) using t tests and identified no significant differences in point prevalence or average symptom severity. Second, we removed unpublished effects from the data set and examined funnel plots for each month at which there were at least 10 published effects. Funnel plots are scatter plots in which the x-axis represents effect size magnitude and the y-axis represents an indicator of effect size precision (e.g., standard error), with the assumption that the most precise effect sizes (i.e., the peak of the funnel) will be closest to the “true” effect size. If the funnel is symmetrical, that means that effect sizes that are larger than the true effect size (i.e., to the right of the peak) are as likely to be published as effect sizes that are smaller than the true effect size (i.e., to the left of the peak). If publication bias is present, one would expect to see an asymmetrical plot, with fewer effect sizes present that are smaller than the true effect size. Using Egger’s regression test in a model with standard error as a predictor (Egger et al., 1997), we found no evidence for publication bias indicated by asymmetry in the funnel plots for PTSD point prevalence at 1 month, z = −0.48, p = .63, or 3 months, z = 1.06, p = .29 (Online Appendices D and E). Funnel plot asymmetry was not examined for PTSD symptom severity because the majority of means were unpublished.
Modeling Change Over Time
A multilevel modeling approach was used to evaluate separate models for the two outcomes: point prevalence (i.e., proportion of the sample with a PTSD diagnosis) and average PTSD symptom severity. This was necessary because all studies contributed multiple effect sizes across time. Thus, effect sizes were nested in samples. Failing to use a multilevel model (i.e., using a “fixed effects” approach) would mean that every effect size would be treated independently, as if it came from a different sample, even though effect sizes obtained from the same sample should be more similar to each other than effect sizes obtained from different sample. In contrast, a multilevel model can include “random effects” to model variability within and between samples. For both point prevalence and symptom severity, likelihood ratio tests revealed that a multilevel (random effects) model was superior to a fixed effects model.
Further, we recognized that several studies assessed PTSD prevalence or severity in multiple ways, which meant that some studies reported multiple effect sizes even within a given time point. This could indicate the need to model a third level of nesting (i.e., effect sizes nested in time points nested in studies). However, likelihood ratio tests revealed that a third level did not improve model fit, likely because there were few samples with multiple assessment types. Thus, the two-level random effects model with effect sizes nested within samples was retained for both PTSD prevalence and severity models. All available data were retained in these models, including multiple effect sizes at a given time point when available.
We then examined the amount of heterogeneity present in the data. If there is substantial heterogeneity, this can indicate the need for moderator analyses to identify potential sources of the heterogeneity. As indicated by I 2 (Higgins & Thompson, 2002) for the intercept-only multilevel model, 90.1% of the variance in PTSD point prevalence and 98.2% of the variance in PTSD symptom severity was due to differences across studies and across effect sizes within the same study (i.e., combined between- and within-group heterogeneity) rather than chance. This suggested that there was heterogeneity in the data that could potentially be accounted for by moderator analyses.
Next, we considered various approaches to model the course of symptom changes over time. First, we considered modeling linear change, which would indicate that average symptoms changed at a constant rate over time, and quadratic change, which would indicate that the average rate of symptom change itself changed over time. We did this by testing both linear and quadratic fixed effects for time (operationalized as the number of months since assault). For both point prevalence and symptom severity, likelihood ratio tests revealed that a model containing a quadratic term was a superior fit to a model containing only a linear term. This suggested that the rate of change in average symptoms over time was not linear; instead, the rate of change itself changed over time.
Given this evidence for a change over time in the rate of average symptom change, we investigated whether there was a particular point in time at which the trajectory of symptoms changed. To do this, we evaluated linear-linear piecewise models, where symptom change over time was modeled as two lines connected by an elbow, or “knot,” which could be placed at various points in time. Drawing on algorithmic approaches to detect unknown knots (e.g., Marcoulides, 2018), we specified model parameters to test in advance. First, based on theoretical conceptualizations of PTSD suggesting symptoms decrease substantially in the months following assault and stabilize thereafter (Monson & Friedman, 2006), we decided to consider at most one knot. Second, for ease of conceptual interpretation, we only considered knots at the monthly level (i.e., integer time values). Third, because there were few samples with multiple assessments after 6 months, and because prior studies suggested that decreases happen prior to 6 months posttrauma (Hiller et al., 2016; Santiago et al., 2013), we only considered knots up to 6 months. Thus, there were seven potential models to consider, including a model with no knots, as well as models with knots at 1, 2, 3, 4, 5, and 6 months. We compared the fit of these models to the data using fit indices appropriate for nonnested models, Akaike Information Criteria (Akaike, 1974) and Bayesian Information Criteria (Raftery, 1995), where lower values represented better fit.
As seen in Online Appendix F, model fit statistics indicated that a knot at 3-months postsexual assault fit the data best for both PTSD point prevalence and symptom severity. These models suggested that, on average, both PTSD point prevalence and symptom severity declined most rapidly within the first 3 months after a sexual assault and continued to decline, but at a slower average rate, in months 3 through 12. All subsequent analyses used models with knots at 3-months post sexual assault.
Month-by-Month Estimates of Point Prevalence and Symptom Severity
Based on the model with a knot at 3 months, model-predicted estimates of PTSD point prevalence and average symptom severity were computed at each time point 3 (Table 2). With regard to the percent meeting PTSD diagnostic criteria, point prevalence decreased from 74.58% at 1 month postassault to 41.49% at 12 months postassault. Mean symptom severity reduced from 47.94% of maximum severity on average at 1 month postassault to 29.91% at 12 months postassault. Model-predicted estimates for PTSD point prevalence and mean symptom severity can be viewed alongside sample-level data in Figures 1 and 2, respectively.
Model-Implied Estimates at Each Month Postassault.
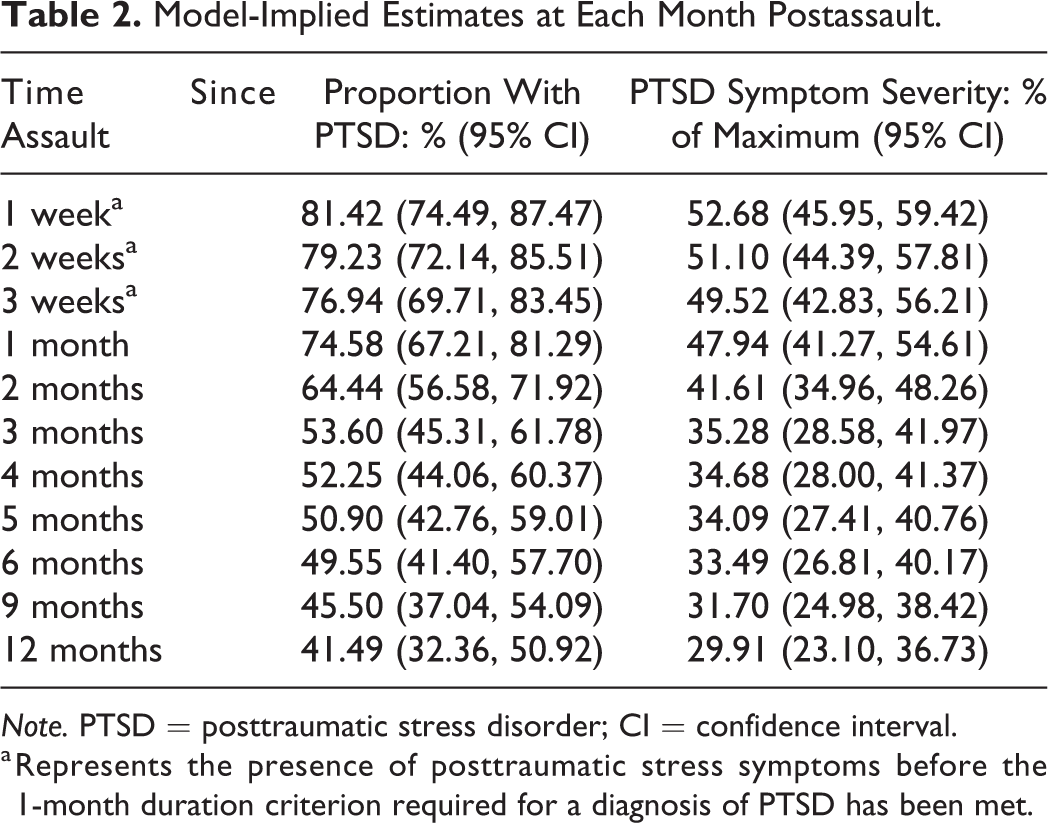
Note. PTSD = posttraumatic stress disorder; CI = confidence interval.
a Represents the presence of posttraumatic stress symptoms before the 1-month duration criterion required for a diagnosis of PTSD has been met.
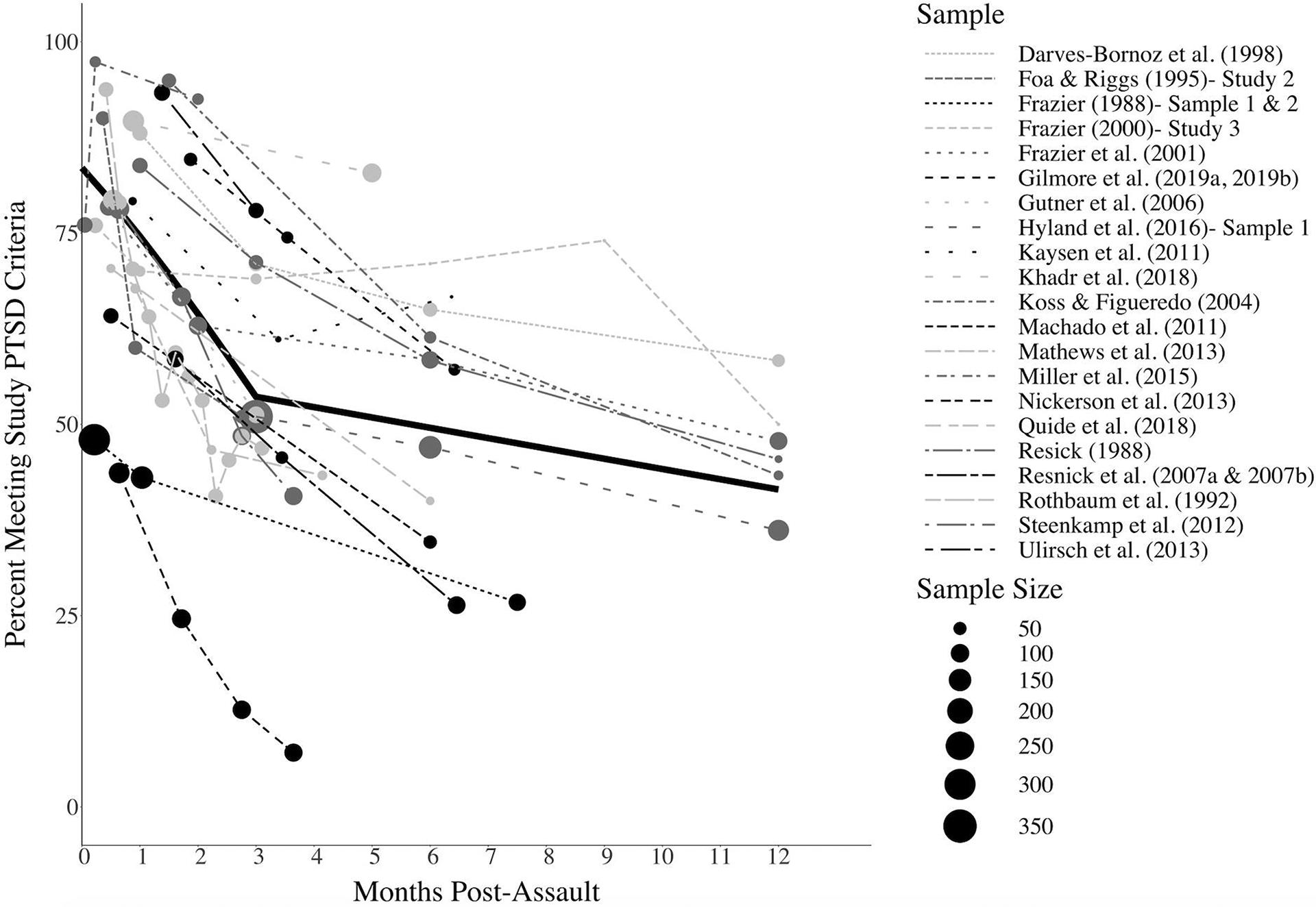
Post-traumatic stress disorder (PTSD) point prevalence by sample and overall (color version available in Online Appendix I). Note. The solid black line represents the overall (i.e., model-predicted) estimates of PTSD point prevalence. A 95% confidence interval for these estimates is additionally presented in the color version of this figure (Online Appendix I).
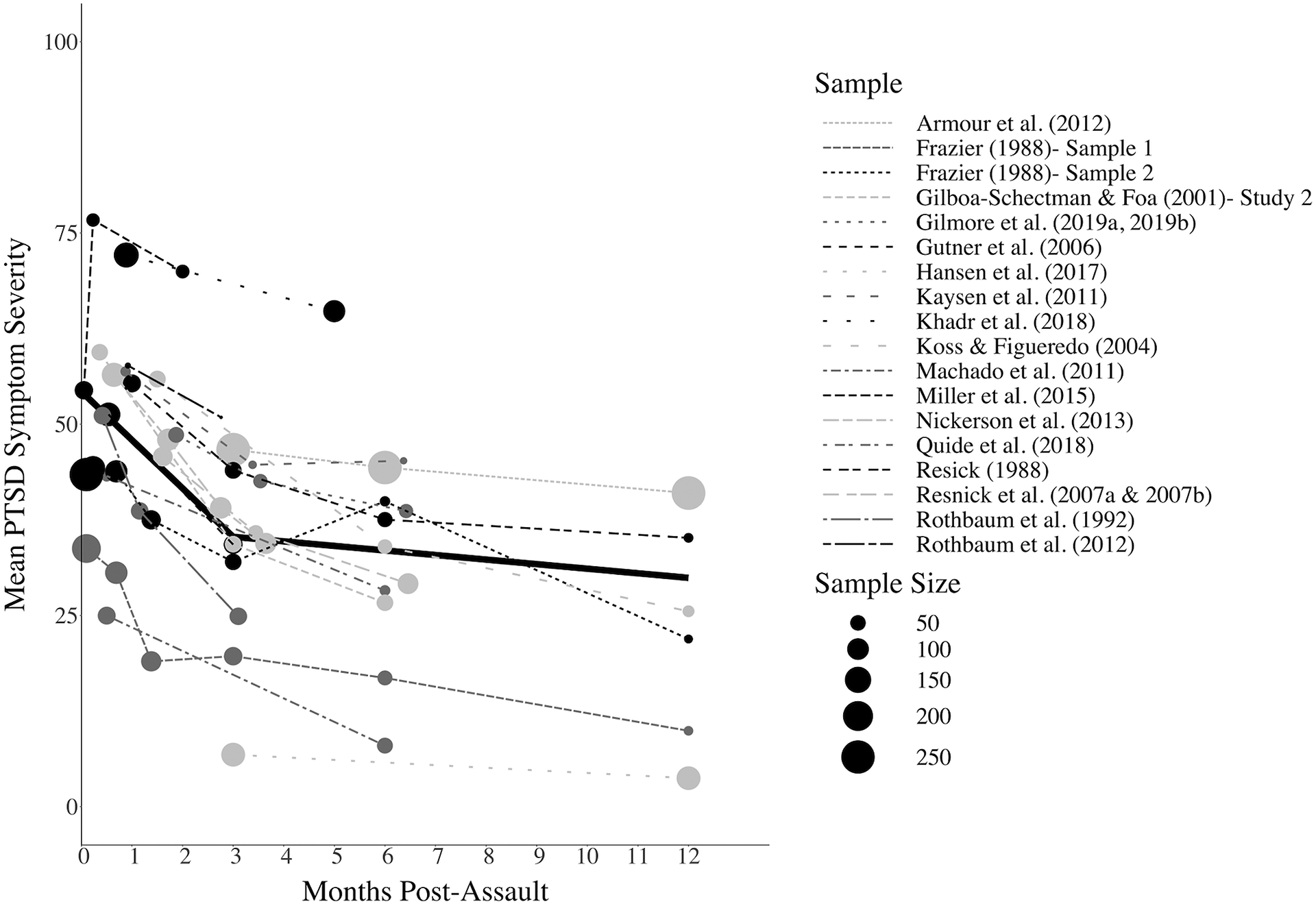
Post-traumatic stress disorder (PTSD) mean severity by sample and overall (color version available in Online Appendix J). Note. The solid black line represents the overall (i.e., model-predicted) estimates of average PTSD symptom severity. A 95% confidence interval for these estimates is additionally presented in the color version of this figure (Online Appendix J).
The Effects of Attrition on Point Prevalence
As described above, the percent of the sample that dropped out at follow-up assessments relative to the study’s baseline was computed for each effect size. Attrition varied over time within a given sample. Across the 19 samples (for effects which were not limited to completers and did not allow for ongoing enrollment) and all post-baseline time points, maximum attrition ranged from 3.23% to 92.49% (M = 45.50%, SD = 26.54%), with greater maximum attrition at later follow-ups, r = .44, p < .001. The average attrition was 33.73% for follow-ups that occurred within the first 6 months postassault and 54.58% for follow-ups that occurred in Months 6–12.
The month-by-month estimates of PTSD point prevalence presented in the prior section were based on calculations assuming that people with PTSD were no more or less likely to drop out of a given study between observations (henceforth, the standard assumption). Correlations were not statistically significant between baseline point prevalence and attrition rates at 3 months, r = −0.33, p = .35, and 6 months, r = −0.18, p = .62, and between baseline symptom severity and attrition rates at 3 months, r = −0.25, p = .48, and 6 months, r = −0.29, p = .38. However, given that these analyses likely had low power to detect statistical significance and correlation magnitude was in the medium range, we next tested the degree to which these findings are robust to violations of the standard assumption.
We recalculated model-implied effects in the models with knots at 3 months postassault under two alternative assumptions, similar by to the approach used Hiller and colleagues (2016). First, we tested the assumption that survivors with PTSD would be less likely to be lost to follow-up (Alternative Assumption 1). To calculate point prevalence under this assumption, we divided the n with PTSD at a given observation by the total sample size (N) at the first observation, which treats all dropouts as if they did not have PTSD. Second, we tested the assumption that survivors with PTSD would be more likely to be lost to follow-up (Alternative Assumption 2). To calculate point prevalence under this assumption, we added the number of people who dropped out by a given observation to the n with PTSD at that observation, up to n with PTSD at the baseline observation, and divided this figure by the total sample size (N) at the first observation. This treats all dropouts as if they had PTSD. We did not allow the numerator to surpass the n with PTSD at the baseline observation given evidence that it is unlikely for the prevalence of PTSD to increase over time (Galatzer-Levy et al., 2018; Smid et al., 2009). Data from three studies involving completer analyses and two studies that enrolled new participants post-baseline were included uncorrected in these analyses to maximize comparability to the original analysis. Online Appendix G includes results under each of the three assumptions. CIs overlapped for the standard assumption and each of the two alternative assumptions through Month 5, but CIs were nonoverlapping for Alternative Assumption 1 at Month 6, and both alternative assumptions at months 9 and 12. This indicates that point prevalence estimates for Months 0–5 are robust to violations of the assumption that attrition is unbiased by PTSD but later estimates should be interpreted with caution.
Moderator Analyses
In unconditional models with knots at 3 months tested using the standard attrition assumption, significant residual heterogeneity was observed in both the point prevalence model, QE(72) = 892.03, p < .0001, and the mean severity model, QE(54) = 3156.43, p < .0001, suggesting the presence of heterogeneity that could potentially be explained by moderators. Because moderation models would test differences in pre- and post-3-month slopes at each level of the moderator, we only considered moderators for which we had data at each level of the moderator from at least three samples both before and after 3 months postassault in both mean and point prevalence models. Results are presented in Table 3. We used a Bonferroni-corrected p value of .004 to interpret the significance of effects in these models. In all, no moderator reduced heterogeneity to nonsignificance.
Moderator Analysis.
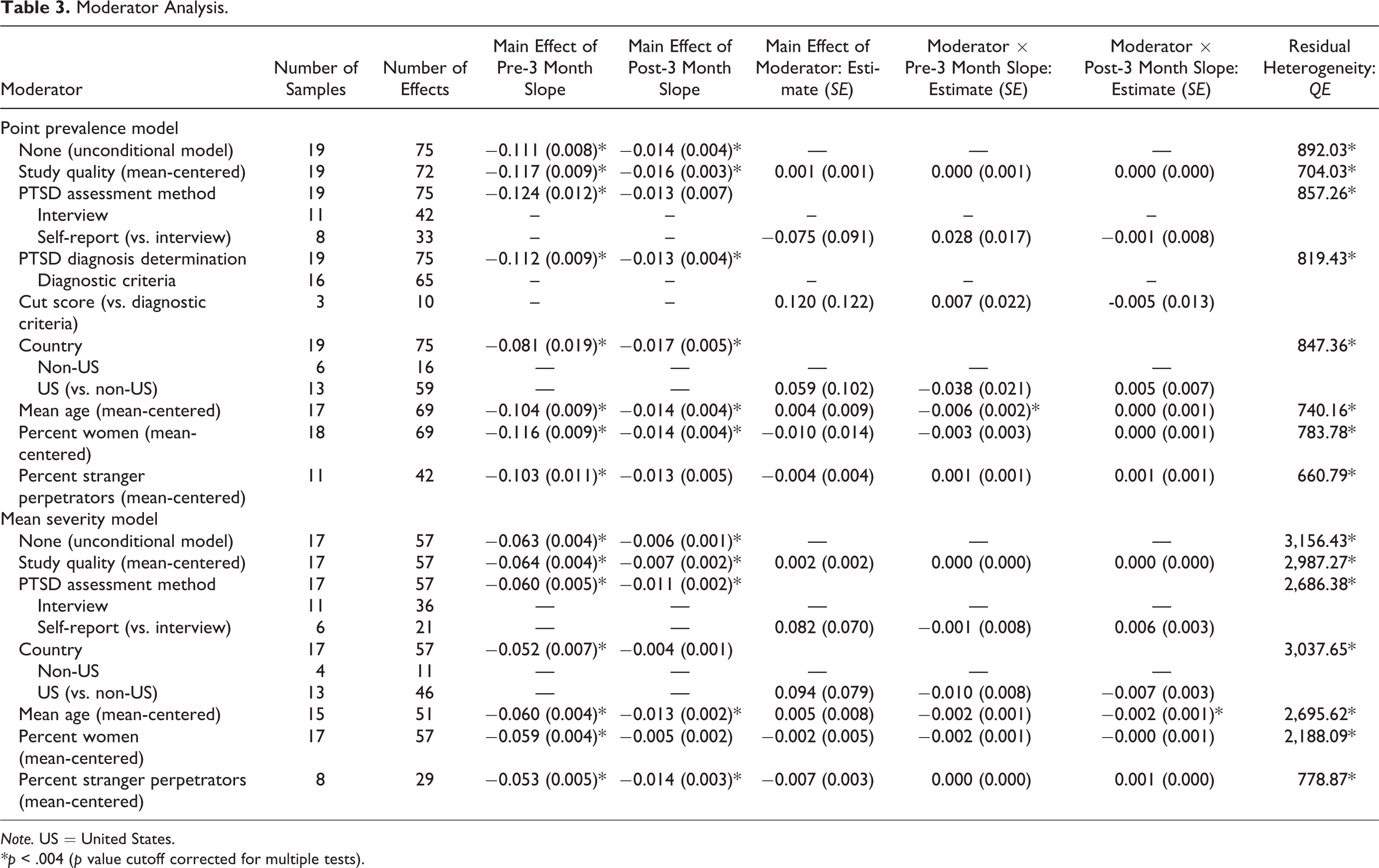
Note. US = United States.
*p < .004 (p value cutoff corrected for multiple tests).
Study quality
There were no statistically significant main or interaction effects for study quality in either model.
Study methods
There were no statistically significant main or interaction effects for PTSD assessment method (interview vs. self-report) or study country in either model. The method used to determine whether participants met study criteria for PTSD was tested in the point prevalence model only (given that study criteria for determining PTSD diagnosis are irrelevant in estimates of severity), and no significant main or interaction effects were identified.
Sample and assault characteristics
Mean age significantly moderated the pre-3-month trajectory in the point prevalence model, such that point prevalence decreased more quickly from 0 to 3 months among older samples. Age also moderated the post-3-month trajectory in the mean severity model, such that mean severity decreased more quickly from 3 to 12 months among older samples. See Online Appendix H for interaction plots. There were no main or interaction effects for gender or the percent of participants assaulted by a stranger in either model.
Discussion
Sexual assault is prevalent (Black et al., 2011; Breiding et al., 2014; Smith et al., 2018) and debilitating (Dworkin et al., 2017). Sexual assault is associated with higher rates of PTSD than other traumas (Brewin et al., 2000; Dworkin, 2020; Kessler et al., 2014; Kilpatrick et al., 2003), and there is evidence that the course of PTSD differs by trauma type (Santiago et al., 2013). However, the unique course of PTSD onset and recovery after sexual assault specifically had not been summarized prior to this study. This was the first known meta-analysis to summarize the month-by-month point prevalence and symptom severity of PTSD and test the timing of changes in average recovery rates, during the year after sexual assault. The current meta-analysis aggregated studies not previously reviewed, as past meta-analyses of posttrauma trajectories (Hiller et al., 2016; Qi et al., 2018) did not include any of the sexual assault-specific samples included in the current analysis. These findings on the unique course of PTSD onset and recovery after sexual assault specifically provide novel information that can be applied to improve prevention and intervention efforts for an especially vulnerable group of trauma survivors.
Point Prevalence and Severity of PTSD Following Sexual Assault
This meta-analysis underscores prior findings that PTSD is common and severe in the immediate aftermath of sexual assault, but strengthen this assertion by representing prospective studies. Specifically, at 1 month after a sexual assault, a majority (74.58%) met criteria for PTSD, and at the 12th month, two of five individuals (41.49%) met criteria. Mean symptom severity was 47.94 out of 100 at 1-month postassault and 29.91 of 100 at 12 months postassault. Although assessments of PTSD included in this analysis reflect DSM-IV-TR and earlier, to assist with interpretation of these findings, we calculated comparable scores on the Clinician-Administered Posttraumatic Stress Disorder Scale (CAPS-5; Weathers et al., 2018) and the PTSD Checklist (PCL-5; Blevins et al., 2015). The PCL-5 has a recommended clinical cutoff of 31–33 (Bovin et al., 2016), and both scales range from 0 to 80. With acknowledgment that this comparison is not exact given changes to DSM diagnostic criteria, average symptom severity scores identified in this analysis were comparable to a CAPS-5 or PCL-5 score of 38.35 at 1 month, 28.22 at 3 months, and 23.93 at 12 months.
PTSD prevalence was high. For example, the 12-month prevalence of 41.49% identified in this prospective meta-analysis—which is the lowest rate observed in the year postassault—is still higher than the lifetime prevalence of PTSD (36.2%, 95% CI: [31.4%–41.1%]) identified in a prior retrospective meta-analysis on this topic (Dworkin, 2020). One would expect the true lifetime prevalence of PTSD in sexual assault survivors to be higher than the prevalence at 12 months postassault, given that the 12-month prevalence rate focuses on a shorter time frame, does not capture PTSD with onset more than 1 year after the assault (though rare; Galatzer-Levy et al., 2018; Smid et al., 2009), and is linked to a specific sexual assault (whereas lifetime prevalence can be linked to any sexual assault or other past traumatic event). Yet, PTSD prevalence rates were higher in the current prospective meta-analysis compared to the Dworkin (2020) retrospective meta-analysis. One potential explanation for this unexpected finding is that the prevalence of PTSD obtained in the prior meta-analysis may be an underestimate due to retrospective reporting biases (e.g., recall failure). Indeed, lifetime prevalence estimates have been critiqued (Streiner et al., 2009), and one study found that the prevalence of common mental disorders obtained from prospective studies was double the prevalence obtained from retrospective studies (Moffitt et al., 2010). Therefore, although prevalence estimates in the current prospective meta-analysis are high, they may be more accurate than retrospectively assessed lifetime prevalence rates. An alternate explanation is differences in sample selection. Specifically, the prospective studies included in the current analysis largely consisted of help-seeking samples, whereas the retrospective studies included in the prior meta-analysis included more college and community-recruited samples. Survivors seeking help might be in more distress, might have more risk factors for the development of PTSD (e.g., greater life threat associated with the assault, fewer social resources; Ozer et al., 2003), or may be subject to additional stressors related to engagement with the criminal justice system.
The rates of PTSD identified in the current study are also much higher than in prior meta-analyses that reflected multiple types of trauma (none of which included any studies reviewed here). For example, in the first month posttrauma, PTSD prevalence was 74.58% following sexual assault in the current analysis. In prior meta-analyses, 1-month PTSD prevalence was 28.8% following mixed trauma exposure (Santiago et al., 2013) and 21.3% following childhood trauma (Hiller et al., 2016). PTSD prevalence at the 12th month posttrauma was 41.5% following sexual assault in this study, as compared to prior meta-analyses, which found 17.0% following mixed trauma exposure (Santiago et al., 2013) and 10.9% following childhood trauma (Hiller et al., 2016). Thus, although the present work did not directly compare the rates and severity of PTSD following sexual assault to that of other trauma types, these comparisons of our findings to prior meta-analyses indirectly corroborate extant literature suggesting sexual assault may be associated with greater prevalence and symptom severity of PTSD relative to other forms of trauma (Brewin et al., 2000; Dworkin, 2020; Kessler et al., 2014; Kilpatrick et al., 2003).
There are several reasons why high rates of PTSD might be observed following sexual assault. First, it is possible that societal stigma and myths related to sexual assault contribute to the development of cognitive changes in survivors that are more substantial or inflexible than those following other forms of trauma. Specifically, cognitive theories of PTSD posit that, following any form of trauma, survivors often develop negative and unhelpful beliefs regarding the trauma itself (e.g., self-blame), oneself (e.g., “I am permanently damaged”), others (e.g., “others cannot be trusted”), and the world (e.g., “the world is totally unsafe”) that prevent natural resolution of PTSD symptoms (Ehlers & Clark, 2000; Janoff-Bulman, 1992; Resick et al., 2017). Commonly-held societal myths about sexual assault (e.g., victim blame; Kennedy & Prock, 2018; Lebowitz & Roth, 1994) may contribute to the development of these negative beliefs following sexual assault (Dworkin & Weaver, 2020), which may create greater obstructions to PTSD recovery for sexual assault relative to other forms of trauma. Second, when survivors disclose sexual assault to others, they may be more likely to receive negative social reactions than survivors of nonstigmatized traumas (Kennedy & Prock, 2018). Meta-analytic findings indicate that these negative social reactions are cross-sectionally and prospectively associated with PTSD symptom severity (Dworkin et al., 2019). Third, sexual assault is more likely than other traumas to produce specific emotional reactions such as anger, guilt, and shame (Amstadter & Vernon, 2008), which may theoretically obstruct PTSD recovery by inhibiting processing of other emotions that naturally occur in response to trauma (e.g., fear, sadness; Resick et al., 2017). Fourth, sexual assault—unlike many other forms of trauma—occurs primarily to women, and women are more likely than men to develop PTSD following trauma (Tolin & Foa, 2006). Some research suggests that the higher population-level prevalence of PTSD in women is not accounted for by the higher likelihood of sexual assault (in which case PTSD prevalence would be expected to be equivalent for men and women following sexual assault) but rather by the presence of psychological risk factors for the development of PTSD in the wake of trauma that are more common among women (e.g., preexisting depression or anxiety; Breslau, 2009; Tolin & Foa, 2006). In addition, risk factors in women’s sociocultural contexts (e.g., sexism) may increase their risk for the development of posttrauma psychopathology (Dworkin & Weaver, 2020). Given that most of the samples (81%) in this study exclusively consisted of women, it is possible that risk factors that differ by gender, rather than sexual assault specifically, contributed to the high rates of PTSD observed in this meta-analysis. Additional literature reviews with greater representation of men and gender minorities are required to fully understand differential symptom trajectories by trauma type and gender.
Trajectory of PTSD Recovery Following Sexual Assault
Our findings also corroborate the extant theoretical and empirical literature by suggesting the majority of PTSD recovery occurs within the first few months following sexual assault, after which point the average rate of recovery slows. These findings are consistent with a past review of multiple types of trauma which indicated that the prevalence of PTSD stabilizes after 3 months following trauma exposure (Santiago et al., 2013). Similarly, Hiller and colleagues’ (2016) meta-analysis of mixed trauma in youth suggested that PTSD symptom severity plateaued after 3 months, although the prevalence of PTSD stabilized at approximately 6 months. Thus, although sexual assault is associated with a particularly high point prevalence and severity of PTSD, the timing of recovery for adolescents and adults appears to be comparable to that of other traumas.
Of note, observed trajectories of symptom recovery may be affected by attrition, given that PTSD could only be assessed for participants who completed longitudinal assessments. Samples varied widely in their maximum attrition, with an average of 45.5% of sexual assault survivors not returning for a follow-up assessment across time points, highlighting the difficulties of retaining participants in the early aftermath of sexual assault. This rate is higher than Qi and colleagues’ (2018) meta-analysis of PTSD in the 4–36 months after acute hospitalization (average attrition of 13%), where the most frequently represented traumatic event was a motor vehicle collision. It is possible that the stigmatized nature of sexual assault relative to other forms of trauma (Kennedy & Prock, 2018) may make it more difficult to retain survivors in assault-related research.
We found no evidence that attrition rates were significantly associated with baseline PTSD in a given sample. Additionally, sensitivity analyses indicated that, even if individual-level attrition differed as a function of PTSD status, estimates for the first 6 months posttrauma were unlikely to be substantially changed, but later estimates may be affected. We considered possibilities at both extremes—that either all or no participants with missing follow-up data had PTSD. Although neither extreme assumption is likely to be true, and the subset of individuals who dropout is likely to be comprised of people both with and without PTSD, our sensitivity analyses focused on these extremes to characterize the range of possibilities. We can further narrow in on the possibilities that appear most likely by interpreting our results in the context of prior work. For example, assuming that all dropouts had PTSD led to very high point prevalence estimates (64.07% and 65.41% at 9 and 12 months, respectively) that are unlikely to be accurate, especially in light of cross-sectional studies that show 12%–25% of survivors meet criteria for current PTSD at any given time (Kilpatrick et al., 2007; Resnick et al., 1993; Zinzow et al., 2012). Instead, true point prevalence estimates may be closer to those estimates obtained under the assumption that no dropouts had PTSD (23.04% and 14.75% at 9 and 12 months, respectively), which would be consistent with prior meta-analytic results revealing that individuals with lower baseline PTSD scores were more likely to drop out of prospective posttrauma studies (Shalev et al., 2019). It is also notable that all correlations obtained for the association between baseline PTSD and attrition were negative. Although these bivariate tests were based on a small number of samples and thus were likely underpowered to detect statistical significance, this implies that it is possible that samples with higher baseline PTSD might have lower dropout. Thus, 9 months after a sexual assault, the point prevalence of PTSD is likely between 23.04% and 45.50%, and by 12 months, the point prevalence is likely between 14.75% and 41.49%.
Moderators of Trajectory of Recovery
In general, we found little evidence that characteristics of studies or samples variables moderated the average rate of recovery. Only age was a significant moderator, such that samples that were older on average tended to evidence quicker recovery. Although prior research on risk of PTSD in relation to age has been somewhat mixed, there is some evidence from cross-sectional studies that younger individuals have higher risk of PTSD (Brewin et al., 2000; Kessler et al., 2017), as one would expect to see for a group that recovers more slowly. In addition, in the only prospective study to our knowledge that examined age in relation to PTSD outcomes, a study of hospitalized trauma survivors found that younger patients were more likely to have PTSD at 3 months posttrauma (Powers et al., 2014), suggesting that—consistent with the current study—younger individuals may have a slower average rate of recovery. When understanding this finding, it is important to note that, in general, samples included in this meta-analysis consisted mostly of adolescents and young adults; indeed, the maximum average age was 35.6 years. Younger sexual assault survivors may have fewer coping skills that could promote their resilience, or may be more likely to disclose to parents, who tend to offer more negative reactions to disclosure than other types of confidants (Reitsema & Grietens, 2016). It is possible that differences in the types of assaults experienced by younger samples (e.g., ongoing child sexual abuse) could account for differences in average rates of recovery, but this possibility has not been tested empirically. Future prospective research should test these possibilities and also explore average rates of recovery among older adults, who also evidence high risk of PTSD following trauma exposure (Kessler et al., 2017) but are minimally reflected in the studies included in this analysis.
Strengths and Limitations
This was the first prospective meta-analysis to examine and clarify the course of recovery from sexual assault. Our inclusion of a substantial amount of unpublished data—representing 52% of the effects analyzed—addresses limitations of past meta-analyses in this area, helps to overcome publication biases that obstruct the dissemination of anomalous findings, and increases the representation of studies, sexual assaults, and survivors with varied characteristics. Additionally, our statistical evaluation of linear-linear piecewise models allowed us to empirically corroborate past work and common perceptions that PTSD recovery slows 3 months after a sexual assault. Finally, our examination of potential bias due to attrition increases confidence in study findings, and our tests of moderators help to contextualize results.
However, this study also had limitations. First, this meta-analysis used aggregate (rather than individual-level) data, which prohibits examination of distinct trajectories in recovery. Indeed, the point prevalence of PTSD at follow-up time points may comprise individuals who have not yet recovered from PTSD, individuals who experienced a new emergence of delayed-onset PTSD, or some combination of the two. Second, we were unable to test some relevant moderators that were unreported for many studies (e.g., percent seeking treatment, frequency of police reporting, weapon use in the assault, physical injury due to the assault, prior history of sexual assault). This is consistent with prior meta-analyses on related topics (e.g., Hiller et al., 2016) and reflects the relatively small number of studies and inconsistent reporting of key characteristics. As a result, it is unclear to what extent these characteristics of studies and samples affected observed results. Future studies should consistently report characteristics of their methods and samples and use novel methodological approaches (e.g., recruitment at nonhospital sites) against which the current results can be compared. We also encourage future researchers to study whether comorbidities moderate average rates of PTSD recovery after sexual assault.
We identified several strengths of the body of research on which this analysis was based. In terms of strengths, the U.S.-based studies were relatively diverse in terms of race and ethnicity: most studies were not comprised primarily of White participants. In addition, although most studies were comprised exclusively of women, approximately a fifth of studies included survivors regardless of gender. This representation is especially important given that the intersection of racism, sexism, and other sociocultural systems of oppression may affect recovery from sexual assault (Bryant-Davis et al., 2009; Dworkin & Weaver, 2020). Although we did not have sufficient data to test gender or race/ethnicity as moderators of PTSD symptom trajectories, future studies should explore this these factors as well as other aspects of diversity. It is possible that rates of recovery may differ as a function of survivors’ intersecting identities, and an individual patient meta-analysis could more effectively disentangle such patterns.
We also identified weaknesses of the primary studies used in this analysis. First, the majority of studies recruited individuals who were seeking some medical or rape crisis services following sexual assault, which may not be representative of survivors who specifically do not disclose their assaults to, or seek help from, health care providers, or who choose not to seek help at all. Non-help-seeking individuals may (a) recover at a more rapid rate than others and therefore may not perceive a need to seek health care, or (b) experience much more severe forms of PTSD that prohibit adaptive help-seeking behavior. Future researchers are advised to study sexual assault recovery using recruitment methods that do not rely on individuals seeking some form of services in order to disentangle these effects. Second, there was substantial variation in the methods used to assess PTSD. In particular, studies varied in terms of whether they used DSM diagnostic criteria or cut scores to establish PTSD diagnoses, so the point prevalence at each month postassault reflects a combination of these methods. The measures used to assess average PTSD symptom severity also varied between studies. We addressed this by transforming all measures to a common scale, but a rescaled score on different measures could have different meanings. We encourage the use of standardized PTSD measures, such as the CAPS-5 or PCL-5, in future work. Third, although not an inclusion criterion, all included samples assessed PTSD with criteria from DSM-IV-TR or earlier. Given that there is evidence that the prevalence of PTSD may change somewhat with DSM-5 criteria (Kilpatrick et al., 2013), this analysis is limited in the conclusions that can be drawn about the prevalence of PTSD using current DSM-5 criteria. Prospective studies using updated criteria are needed to address this gap.
Clinical Implications
Current findings offer important clinical implications. First, our findings suggest that PTSD is common and severe following sexual assault, which may help to normalize survivors’ distress following sexual assault. Second, our results suggest that on average, PTSD symptom severity continues to decline up to a year after a sexual assault. This suggests natural recovery is an ongoing process that may continue, however slowly, beyond the immediate aftermath of a trauma and could be used by clinicians to combat negative attributions regarding symptoms (e.g., reduce beliefs such as “I will never feel better”; Ehlers & Clark, 2000).
Efforts to prevent PTSD in the aftermath of trauma exposure have long focused on the first 3 months posttrauma as a critical period for delivering interventions (Roberts et al., 2019). A recent meta-analysis indicates that certain such interventions (especially trauma-focused cognitive behavioral therapy) are effective at preventing PTSD (Roberts et al., 2019), and there is some evidence that these interventions are more effective at preventing PTSD after sexual assault as compared to other types of traumas (Rothbaum et al., 2012). Although the current results cannot not speak to the efficacy of early versus later intervention, they suggest that the first 3 months following sexual assault appear to be a period in which substantial symptom change is occurring, which could potentially increase malleability to intervention. Intervening in this period of time could change trauma-related thoughts and behaviors before they become habitual. Given prior research suggesting that societal stigma and negative social reactions may explain higher PTSD prevalence and severity after sexual assault versus other traumas (Dworkin et al., 2019; Kennedy & Prock, 2018), such interventions could potentially be more effective by explicitly attending to the societal context of sexual assault recovery.
In light of the finding that recovery may slow after 3 months following trauma exposure, providers of intensive treatments may consider adopting an approach of “watchful waiting” in the months following sexual assault in order to identify who may not quickly recover without subsequent clinical intervention and thus may be in need of more intensive services. Our provision of average scores on commonly used PTSD measures may help clinicians determine if their clients are experiencing more severe symptoms than typical at each month postassault.
Conclusions and Directions for Future Research
In conclusion, this meta-analysis examined the point prevalence, severity, and trajectory of recovery from PTSD following sexual assault. Findings suggested that PTSD is common and severe following sexual assault, and the average rate of recovery slows (but continues) after 3 months. Building on the present work, future researchers are advised to prospectively study sexual assault recovery in survivors who are not actively seeking help in order to identify whether their PTSD prevalence, severity, and average recovery rates differ between survivors who do and do not seek services. To further disentangle unique trajectories following sexual assault, an individual patient meta-analysis drawing on archived data is recommended.
Critical Findings
One month after sexual assault, 75% of survivors met criteria for PTSD. Twelve months after sexual assault, 41% of survivors met criteria for PTSD.
The majority of PTSD recovery occurs within the first 3 months following sexual assault, after which point the average rate of recovery slows.
Supplemental Material
Supplemental Material, sj-csv-1-tva-10.1177_15248380211032213 - PTSD in the Year Following Sexual Assault: A Meta-Analysis of Prospective Studies
Supplemental Material, sj-csv-1-tva-10.1177_15248380211032213 for PTSD in the Year Following Sexual Assault: A Meta-Analysis of Prospective Studies by Emily R. Dworkin, Anna E. Jaffe, Michele Bedard-Gilligan and Skye Fitzpatrick in Trauma, Violence, & Abuse
Supplemental Material
Supplemental Material, sj-docx-1-tva-10.1177_15248380211032213 - PTSD in the Year Following Sexual Assault: A Meta-Analysis of Prospective Studies
Supplemental Material, sj-docx-1-tva-10.1177_15248380211032213 for PTSD in the Year Following Sexual Assault: A Meta-Analysis of Prospective Studies by Emily R. Dworkin, Anna E. Jaffe, Michele Bedard-Gilligan and Skye Fitzpatrick in Trauma, Violence, & Abuse
Supplemental Material
Supplemental Material, sj-pdf-1-tva-10.1177_15248380211032213 - PTSD in the Year Following Sexual Assault: A Meta-Analysis of Prospective Studies
Supplemental Material, sj-pdf-1-tva-10.1177_15248380211032213 for PTSD in the Year Following Sexual Assault: A Meta-Analysis of Prospective Studies by Emily R. Dworkin, Anna E. Jaffe, Michele Bedard-Gilligan and Skye Fitzpatrick in Trauma, Violence, & Abuse
Supplemental Material
Supplemental Material, sj-pdf-2-tva-10.1177_15248380211032213 - PTSD in the Year Following Sexual Assault: A Meta-Analysis of Prospective Studies
Supplemental Material, sj-pdf-2-tva-10.1177_15248380211032213 for PTSD in the Year Following Sexual Assault: A Meta-Analysis of Prospective Studies by Emily R. Dworkin, Anna E. Jaffe, Michele Bedard-Gilligan and Skye Fitzpatrick in Trauma, Violence, & Abuse
Supplemental Material
Supplemental Material, sj-pdf-3-tva-10.1177_15248380211032213 - PTSD in the Year Following Sexual Assault: A Meta-Analysis of Prospective Studies
Supplemental Material, sj-pdf-3-tva-10.1177_15248380211032213 for PTSD in the Year Following Sexual Assault: A Meta-Analysis of Prospective Studies by Emily R. Dworkin, Anna E. Jaffe, Michele Bedard-Gilligan and Skye Fitzpatrick in Trauma, Violence, & Abuse
Supplemental Material
Supplemental Material, sj-pdf-4-tva-10.1177_15248380211032213 - PTSD in the Year Following Sexual Assault: A Meta-Analysis of Prospective Studies
Supplemental Material, sj-pdf-4-tva-10.1177_15248380211032213 for PTSD in the Year Following Sexual Assault: A Meta-Analysis of Prospective Studies by Emily R. Dworkin, Anna E. Jaffe, Michele Bedard-Gilligan and Skye Fitzpatrick in Trauma, Violence, & Abuse
Supplemental Material
Supplemental Material, sj-pdf-5-tva-10.1177_15248380211032213 - PTSD in the Year Following Sexual Assault: A Meta-Analysis of Prospective Studies
Supplemental Material, sj-pdf-5-tva-10.1177_15248380211032213 for PTSD in the Year Following Sexual Assault: A Meta-Analysis of Prospective Studies by Emily R. Dworkin, Anna E. Jaffe, Michele Bedard-Gilligan and Skye Fitzpatrick in Trauma, Violence, & Abuse
Supplemental Material
Supplemental Material, sj-pdf-6-tva-10.1177_15248380211032213 - PTSD in the Year Following Sexual Assault: A Meta-Analysis of Prospective Studies
Supplemental Material, sj-pdf-6-tva-10.1177_15248380211032213 for PTSD in the Year Following Sexual Assault: A Meta-Analysis of Prospective Studies by Emily R. Dworkin, Anna E. Jaffe, Michele Bedard-Gilligan and Skye Fitzpatrick in Trauma, Violence, & Abuse
Supplemental Material
Supplemental Material, sj-png-1-tva-10.1177_15248380211032213 - PTSD in the Year Following Sexual Assault: A Meta-Analysis of Prospective Studies
Supplemental Material, sj-png-1-tva-10.1177_15248380211032213 for PTSD in the Year Following Sexual Assault: A Meta-Analysis of Prospective Studies by Emily R. Dworkin, Anna E. Jaffe, Michele Bedard-Gilligan and Skye Fitzpatrick in Trauma, Violence, & Abuse
Supplemental Material
Supplemental Material, sj-png-2-tva-10.1177_15248380211032213 - PTSD in the Year Following Sexual Assault: A Meta-Analysis of Prospective Studies
Supplemental Material, sj-png-2-tva-10.1177_15248380211032213 for PTSD in the Year Following Sexual Assault: A Meta-Analysis of Prospective Studies by Emily R. Dworkin, Anna E. Jaffe, Michele Bedard-Gilligan and Skye Fitzpatrick in Trauma, Violence, & Abuse
Footnotes
Acknowledgments
The authors would like to thank the researchers who submitted unpublished data or facilitated these requests: John B. Barnes, Venetia Clarke, Patricia Frazier, Amanda Gilmore, Debra Kaysen, Sophie Khadr, Mary Koss, Katherine Miller, Jani Nöthling, Matthew Price, Yan Quidé, Patricia Resick, Barbara Rothbaum, Arlete Maria dos Santos Fernandes, Soraya Seedat, Brian Smith, Maria Steenkamp, and Kate Walsh.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Manuscript preparation for this article was supported by the National Institute of Alcohol Abuse and Alcoholism (NIAAA) grants T32AA007455 (PI: Larimer), K99AA026317 (PI: Dworkin), R00AA026317 (PI: Dworkin), and R01AA027499 (PI: Bedard-Gilligan).
Notes
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.