
Abstract
Polyvictimization is an important and fairly recent public health concept, with the term first used by Finkelhor et al. in 2007 to differentiate between experiences of one single type of victimization exposure—such as sexual violence or physical violence—and the experience of multiple types of victimization, or polyvictimization (Finkelhor et al. 2007a). Individuals who experience polyvictimization, as compared to those who experience one victimization type, are at greater risk for negative mental health outcomes (Cyr et al., 2017), including trauma-related symptomatology (Finkelhor et al., 2007a, 2007b). In addition, polyvictimization allows for an exploration of victimization profiles, including how certain victimization types tend to cluster together, and how exposure to one victimization type can increase the odds of exposure to different types of victimization (Finkelhor et al., 2007a; Fleckman et al., 2016). Understanding polyvictimization is essential in crafting more effective violence prevention strategies that address complex victimization experiences and target multiple health outcomes.
Among polyvictimization studies, the majority of the literature focuses on childhood experiences of polyvictimization (Ramsey-Klawsnik, 2017) given the harmful effects of child maltreatment and childhood violence exposure on related health outcomes (Cyr et al., 2014; Ford & Delker, 2018; Richmond et al., 2009; Schwab-Reese et al., 2018). A large volume of literature documents a variety of associated negative health outcomes of childhood polyvictimization, including: lower self-esteem; depression, anxiety disorders, psychosis, post-traumatic stress disorder (PTSD), and other mental health symptoms; risky behaviors, self injury, and suicide attempts; substance misuse; attention and cognitive difficulties; aggressive behaviors; delinquency and criminal activities; severe obesity; somatic complaints and physical health diagnoses; and poor perception of health (Curran et al., 2016; Cyr et al., 2014; 2017; Dierkhising et al., 2019; Fleckman et al., 2016; Hellström, 2019; Källström et al., 2017; Kennedy, 2017; Kerig, 2018; La Flair et al., 2013; Moeller et al., 1993; Samms-Vaughan & Lambert, 2017). Clearly, polyvictimization can have a wide array of negative associations with mental, behavioral, social, and physical health symptoms.
Discrepancies in the Literature
While mounting research has emerged over the last decade focusing on the impact of polyvictimization, one limitation of the existing literature is the variance in conceptual and operationalized definitions. A major variation is how “multiple” victimizations is defined. At the conceptual level, while most literature defines the term as multiple types of victimization (Chan et al., 2019; Finkelhor et al., 2007a; Ford & Delker, 2018; Grasso et al., 2016; Hooven et al., 2012; Kallstrom et al., 2017; Mitchell et al., 2020; Nguyen et al., 2019), the term has also been applied with slight variations. As a few examples from recent research, Hellström (2019) defined the term as exposure to violence in different settings (e.g., school, home, and community); Miller-Graff et al. (2019) used the term as varied types of violence by different perpetrators; Kennedy (2017) noted the term as cumulative forms of direct and indirect interpersonal violence. These varied conceptual definitions across studies show that the notion has been slightly differently applied to each violence context.
At the level of operationalized definitions, polyvictimization has been differently applied in research studies. La Flair et al. (2013) defined polyvictimization as experiencing more than one form of childhood abuse and neglect among four types of violence: sexual abuse, physical abuse, witness to domestic violence, and neglect by a parent or caregiver. On the other hand, Dierkhising et al. (2019) defined polyvictimization as high exposure (mean = 2.8 to 4.8) as opposed to low exposure (mean = 1.3 to 1.8) among 17 traumatic stressors. While some polyvictimization literature includes exposure only related to interpersonal violence (Carbonaro, 2019; La Flair et al., 2013; Miller-Graff et al., 2015), this study by Dierkhising et al. (2019) included multiple forms of maltreatment, victimization, and traumatic experiences that were not necessarily interpersonal violence (e.g., illness/medical trauma, serious injury/accident, natural disaster, or war). As such, the operationalized definitions of polyvictimization across studies have been wide-ranging.
Literature Reviews of Childhood Polyvictimization and Health Outcomes
To date, there has been no prior systematic review that synthesized both aspects of childhood polyvictimization and its related health outcomes. There have been a few systematic reviews on polyvictimization focused on prevalence of these experiences among certain clinical subgroups, including a study regarding polyvictimization among children with attention deficit hyperactivity disorder (ADHD) or autism spectrum disorder with samples from Spain, Hong-Kong, Norway, France, and the U.S. (Hellström, 2019). Additionally, there was a systematic review of poly-traumatization typologies with samples from Ireland, Australia, and the U.S. (Contractor et al., 2018). Further, there have been a few review papers that addressed the evidence, contexts, and information about older adults affected by polyvictimization (Ramsey-Klawsnik, 2017) and the factors associated with physical and sexual child abuse and polyvictimization in Africa (Meinck et al., 2015). A systematic review and meta-analysis reported the prevalence of polyvictimization among children and adolescents in low- and lower-middle income countries (Le et al., 2018), which provided a supplemental table that summarized associated health and well-being outcomes. However, out of the 30 studies reviewed by Le et al. (2018), a majority reported the associations between specific, individual forms of victimization and health outcomes, not multiple types of victimization and its associated health outcomes. As such, a deeper understanding of the impact of childhood polyvictimization on health outcomes is imperative across different country settings. Indeed, the prevalence and patterns of polyvictimization differ across countries and regions, as one recent meta-analysis reveals that the prevalence of polyvictimization in low-middle income countries was on average 38.1% (Le et al., 2018) whereas that of the U.S. was 10% (Turner et al., 2010) and that of China was 14% (Chan, 2013; Johnco et al., 2019). However, there is no previous systematic synthesis on this topic that includes all geographic areas regardless of health conditions. Thus, the purpose of this paper is to offer a scoping review of these general associations that are not limited by a country setting or clinical subgroups.
Study Purpose
Scoping reviews are performed to clarify concepts, determine the scope of a body of literature, identify knowledge evidences and gaps, and confirm the relevance of inclusion criteria and potential questions for systematic reviews as precursors to future review projects (Munn et al., 2018). The methodology, structure, and values of scoping reviews are well-documented (Arksey & O’Malley, 2005; Colquhoun et al., 2014; Levac et al., 2010; Munn et al., 2018; Peters et al., 2015). Following these guidelines, we performed a systematic scoping review to: (1) clearly indicate the volume of available studies on the topic of childhood (ages 0–19) polyvictimization and associated health outcomes. The polyvictimization was experienced during the childhood (developmental period) but the health outcomes assessed were not limited to childhood. (both published and unpublished literature), (2) determine the coverage of the body of literature on the topic, especially documenting the varied constructs of polyvictimization and health outcomes, (3) identify and analyze knowledge evidences and gaps, and (4) pose more specific research questions that can be valuably addressed by future systematic reviews. A systematic review and meta-analysis of these associations were considered, but with inconsistent definitions of polyvictimization, broad scope of health outcomes, and samples of varied regional aspects, it was inherently challenging to yield an accurate synthesis that can be used as a firm knowledge base to offer clinical implications and guide practice, program, policy, and research. Thus, this scoping review will help future systematic reviews to be more precise, answer clinically meaningful questions with less risk of bias of the emerging evidences, provide directions to future research priorities and evidence to inform practice, programs, and policy, and make sense of the landscape of the emerging evidences (Colquhoun et al., 2014; Munn et al., 2018).
Methods
Scoping Review Team
The study team consisted of four reviewers, a method expert, and three content experts. The reviewers searched, screened, and coded the literature, and the method and content experts ensured the review’s scientific credibility and content relevance in the violence literature field.
Population, Intervention, Comparison, and Outcomes
The Population, Intervention, Comparison, and Outcomes (PICO) elements used in the study were the following. (1) Population: 0–19 years old (the age range exposed to polyvictimization); (2) Intervention: not applicable (included studies were observational or retrospective); (3) Comparison group: those who have not experienced polyvictimization (e.g., those who experienced only one single-type victimization or no victimization experience in childhood); (4) Outcome: health outcomes. The age 19 was used following the definition by WHO and similar sources (Canêo & Neirotti, 2017; UNICEF, n.d.; WHO, n.d.). A number of childhood polyvictimization studies included age 18 (e.g., Butcher et al., 2016; Davis et al., 2020; Jativa & Angeles Cerezo, 2014; Kirchner et al., 2020; Kretschmar et al., 2017; Le et al., 2018; Sabri et al., 2012; Soler et al., 2013) and age 19 (Carbonaro, 2019; Juan et al., 2019; Kamndaya et al., 2017).
Search Strategy and Selection of the Literature
The literature search was conducted between June 8, 2020 and June 16, 2020. Six databases were searched using Georgia State University library system in Web Scale Discovery Service: Web of Science, PubMed, Embase, Medline with Full Text, APA Psycinfo, and ProQuest Central. Of these, Web of Science, APA Psycinfo, and ProQuest Central were additionally used to search for unpublished articles, conference proceedings, and dissertations. In addition, gray literature was searched through relevant organization websites such as Office of Juvenile Justice and Delinquency Prevention, American Institute for Foreign Study, and Substance Abuse and Mental Health Services Administration between May 29 and June 7, 2020.
The search terms were determined after consulting the method and content experts and two university librarians. The same search terms were used for all six databases: [(“poly-victimization” or “poly victimization” or “multi-domain victimization” or “polyvictimization”) AND (child or children or young person or adolescent or teenager or youth or young people) AND (health outcomes or health consequences or health implications or health impact)]. We only included studies that met the following eligibility criteria: (1) was an original article about childhood polyvictimization experience; (2) presented health outcomes (e.g., mental distress, PTSD, suicidal risks, depression, or substance abuse); (3) evaluated quantitative associations between childhood polyvictimization and health outcomes; (4) was written in English. We did not limit the years of publication as the concept of polyvictimization was recent (Finkelhor et al., 2007a). Studies were included regardless of the country/region of focus. As we reviewed studies, we established post-hoc exclusion criteria: (1) included traumatic events or life adversities that were beyond interpersonal violence victimization (e.g., poverty, parent lost job, no good friends, accidents, natural disasters, not living with mother, parental impairment, family member in jail, family substance use, or police arrest/detention) as part of the polyvictimization experience—in this sense, the experiences included in the study were distinguished from adverse childhood experiences (ACEs; i.e., potentially traumatic events that occur in childhood), which are a broader concept that includes life adversities and potentially traumatic experiences experienced in childhood besides experiencing violence, abuse, or neglect or witnessing violence (CDC, 2021); (2) did not meet the temporality of the timings of polyvictimization and health outcomes—health outcomes were assessed earlier in the life trajectory than polyvictimization occurred, or both victimization and health outcome measures were lifetime, thus temporality could not be established; (3) health outcomes were delinquency or criminal behaviors that were distant from direct health outcomes.
Two steps of screening process were involved to include eligible studies for this review, and then backward reference searching was made. First, abstract screening was performed. Duplicate articles were merged using Zotero (a reference management software), and Abstrakr (an abstract screening tool) was used for the abstract screening process. Abstracts were double screened by two reviewers based on Eligibility Criteria 1, 2, and 4, and discrepancies were resolved by the first author. Then, full text articles were retrieved except for conference abstracts or unavailable studies. Second, full-text screening was conducted. Three reviewers divided the studies and screened articles following the eligibility and post-hoc criteria. Then, the first author double-screened all articles. Discrepancies were resolved through discussions. An Excel spreadsheet was used for this process. Next, citation mining was conducted. The reference list of the included studies from full text screening was examined based on the title, abstract, and full text. Titles and abstracts were assessed by the first author, full-text was double-screened by the reviewer team, and then discrepancies were resolved through discussions.
Data Extraction
Following the aims of the study, we coded the operationalized definition of polyvictimization, documenting how victimization profiles were compared and what victimization types were included in each study, as well as the investigated health outcomes. The victimization classification method was not part of our study focus, but, based on the extracted data, we summarized general methodological approaches that studies have taken to operationally define polyvictimization in the studies (e.g., continuous vs. categorical). At the same time, we documented whether studies recorded victimization perpetrator types, frequency, and/or severity, as some definitions of polyvictimization noted victimization by multiple perpetrators or increased total exposure (frequency and severity) of victimization and accounting for the number and type of perpetrators, frequency of victimizations, and severity of victimizations may contribute to understanding the impact of victimizations. Finally, we extracted information such as author names, year of publication, country that the sample(s) were drawn from, sample size, and female percent in sample.
Results
Study Selection
Out of the six databases, a total of 389 studies were identified (Web of Science: 181, PubMed: 76, Embase: 69, Medline with Full Text: 28, APA Psycinfo: 33, and ProQuest Central: 2), of which 165 studies were duplicates. After duplicates were merged, 224 studies were double-screened. Abstract screening revealed that 139 abstracts were eligible, and 131 studies were located for full text screening. After the second double-screening process, 54 studies were eligible to be included. Citation mining added an additional 40 studies. The active gray literature search added two relevant reports/articles to the final set. Thus, the final set of included studies were 96 (Figure 1). Flow chart following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).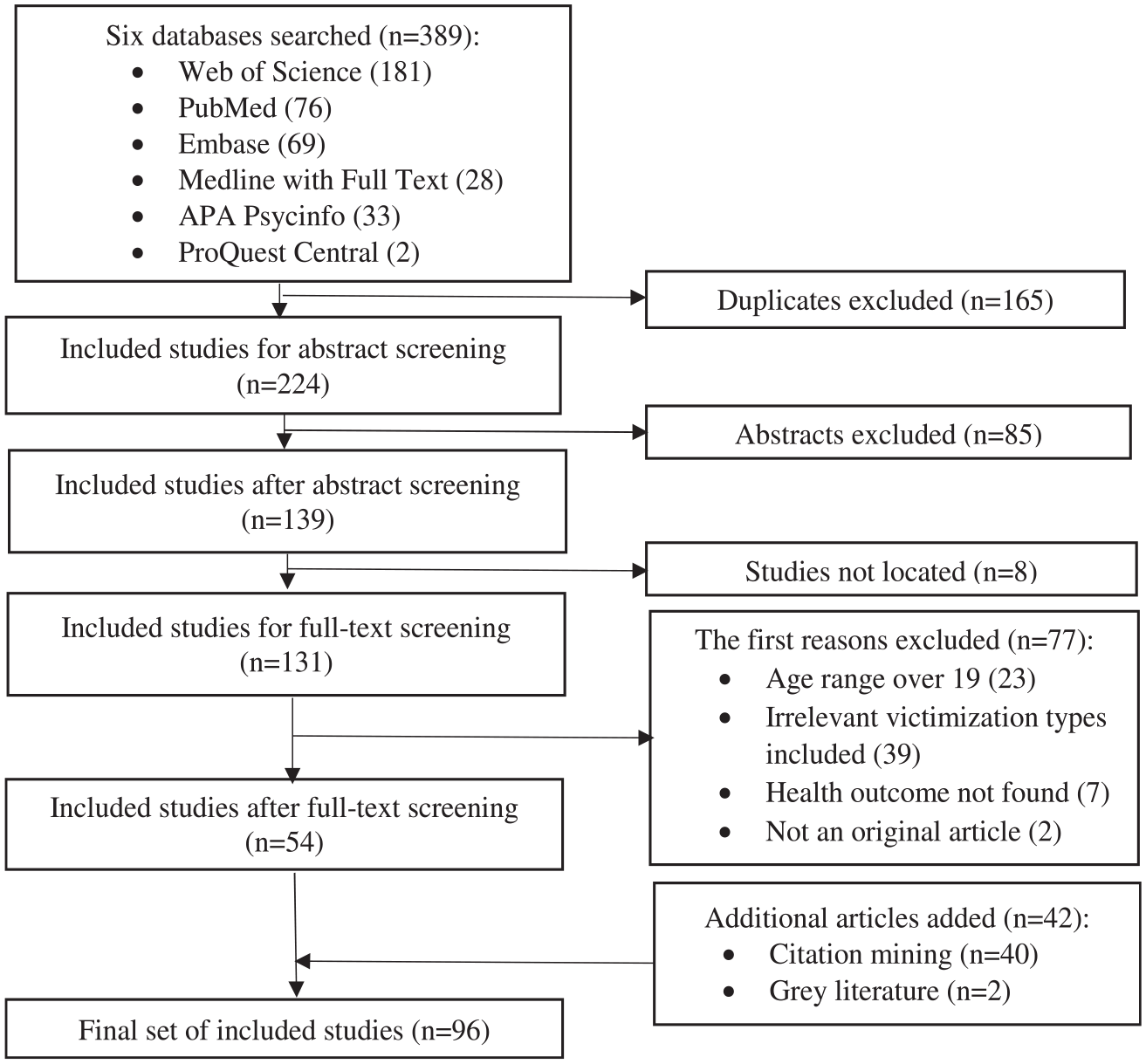
Study Characteristics
In the following sections, we summarize our review results including: polyvictimization construct; associated health outcomes; victimization perpetrator, frequency, and severity characteristics; countries samples were drawn from; female percent among study samples; and publication year.
Polyvictimization Construct
Victimization Types
Regarding the types of victimization included in the polyvictimization construct (Supplementary Appendix A), both specific domain and individual items of victimization differed widely. To iterate, the number and the types of victimization included in polyvictimization constructs varied extensively from using two victimization types with three individual items (Shevlin et al., 2015) to three victimization types with 14 items (Natukunda et al., 2019), 36 individual victimization items grouped into six broader types (Álvarez-Lister et al., 2014), 44 victimization items of 10 types (Michel-Smith, 2019), and to 75 items of 10 different types of victimization (Riedl et al., 2019). At times, direct violence exposure was classified as one type (Voith et al., 2014), while, at other times, direct violence exposure was often further classified into more detailed victimization types, such as sexual violence, physical violence, or conventional crime (e.g., Aho et al., 2016; Kirchner et al., 2020; Turner et al., 2017). As such, studies vastly differed in terms of what victimization items and types were included in the construct. However, as not every study documented the number of individual question items, our review did not summarize such information but documented the victimization domain/type investigated in the studies (Supplementary Appendix A).
Continuous Versus Categorical Variable
When it comes to the polyvictimization construct, 30.21% of included studies coded polyvictimization as a continuous variable; however, the majority of studies (72.92%) coded it as a categorical variable. Two common approaches were found for the construction of continuous polyvictimization variables, and four were noted for the construction of categorical polyvictimization variables. For continuous polyvictimization variables, the first common approach was a summary measure of the total number of individual victimization items experienced. For example, studies using this approach counts sexual harassment, non-penetrative sexual assault, and rape as unique items (not as one sexual violence domain). Whether the range of possible victimization types was 0–14, 0–36, or 0–75, the polyvictimization construct was a continuous variable that summed the number of different individual victimization items that respondents were exposed to among the items examined (e.g., Guerra et al., 2016; Turner et al., 2010, 2013a, 2013). A second common approach was to create the polyvictimization variable using the number of different domains of victimization experienced. For example, domains include any sexual violence, any non-sexual physical violence, and any verbal violence. In this case, the cumulative victimization domain/type had a lower range such as 0–3, 0–4, or 0–5 (e.g., Boxer & Terranova, 2008; Edwards et al., 2014; Edwards et al., 2003; Horn et al., 2018; Kennedy, 2017; Nguyen et al., 2019a).
In terms of categorical polyvictimization variables, one approach (14.58%) compared victimization profiles distinguished by different mixtures of violence types. Examples include no maltreatment, emotional abuse only, or physical abuse, sexual abuse, and neglect (Arata et al., 2007) or neglect only, physical abuse only, or physical abuse and neglect (Hahm et al., 2010) by mixture of different types.
A second approach to the categorical variable (7.29%) was to define polyvictimization as experiencing more than one type of violence (e.g., Charak et al., 2015; Hickman et al., 2013; Itani et al., 2018; Kamndaya et al., 2017; Natukunda et al., 2019; Sabri et al., 2012; Shevlin et al., 2015; Updegrove & Muftic, 2019). These studies compared the polyvictimization group with those who experienced none or one type of violence. In these studies, the group who experienced “more than one type of violence” was not further classified as those exposed to, for example, three types of violence or four types of violence victimization.
Third, a number of studies (29.17%) classified “more than one type of violence exposure” further and defined polyvictimization by different numbers/scores of victimizations experienced as an ordinal variable. The most basic structure is to group victimization profiles solely by the number of victimization types experienced, for example, no abuse, one, two, and three types of abuse experienced (Moeller et al., 1993; Raskauskas, 2010) or one, two, and three or more maltreatment types experienced (Richardson et al., 2008), defining beyond two or more types of violence exposure. However, in many cases, studies also applied cut-off points to define polyvictimization. That is, depending on the age group or the number of victimization items examined, the cut-off points for polyvictimization differed, for example, four or more victimization types experienced (Chan et al., 2017; Riedl et al., 2019), five or more victimizations experienced (Ellonen & Salmi, 2011; Turner et al., 2019), seven or more screeners endorsed (Turner et al., 2012), nine or more forms of victimization experienced (Soler et al., 2012), more than 10 forms of victimization experienced (Le et al., 2016), 14 or more items endorsed (Michel-Smith, 2019), or 37 or more episodes reported (Kirchner et al., 2020). At times, cut-off points were set at the top 10–13 percent of the victimized group (Aho et al., 2016; Finkelhor et al., 2011, 2011b; Jackson-Hollis et al., 2017; Mitchell et al., 2020).
Additionally, as part of the third approach to the categorical variable scheme, some studies defined polyvictimization even further, distinguishing low, mid, and high polyvictimization groups (de Azeredo et al., 2019; Fernández-Artamendi et al., 2020; Finkelhor et al., 2007a; Margolin et al., 2010; Segura et al., 2016). For example, de Azeredo et al. (2019) distinguished low levels of polyvictimization (scores of five to 10) and high levels of polyvictimization (scores greater than 10) using different cumulative scores of victimization, and Fernández-Artamendi et al. (2020) distinguished low, mid, and high polyvictimization levels according to the number of forms of victimization experienced and the age group: low polyvictimization (one to six forms of victimization (<14 years), one to eight forms of victimization (≥14 years)), mid polyvictimization (seven to 20 forms of victimization (<14 years), nine to 20 forms of victimization (≥14 years old)), and high polyvictimization (≥21 forms of victimization).
Still in the third approach in the categorical methods, chronic conditions, severity, and frequency status were also sometimes considered in addition to types of victimization. When the chronic condition of victimization was considered, one classification schema classified victimizations as no victimization, victimization in one stage of development (out of three stages: 0–5, 6–12, and 13–18 years old), victimization in more than one stage of development, victimization of multiple types in one stage of development, and victimization of multiple types in more than one stage of development (Mitchell et al., 2020). Further, when severity/frequency characteristics were considered, the classification could be made as no, low (low levels of one to five child maltreatment types), moderate (moderate/severe levels of one to three child maltreatment types), and severe (moderate/severe levels of four to five child maltreatment types) levels of victimization (Dovran et al., 2019). However, with all these different variations, these examples speak to one scheme that defines polyvictimization with the number of victimization experiences endorsed as an ordinal variable.
Lastly, analytical schemes (21.88%) such as latent class analysis or cluster analysis were used to identify victimization groups. Latent class analysis was the most commonly used as an analytical method to distinguish different victimization profiles (e.g., Aebi et al., 2015; Beck et al., 2014; Berzenski & Yates, 2011; Butcher et al., 2016; Cecil et al., 2014; Charak et al., 2016; Curran et al., 2016; Davis et al., 2019; Grasso et al., 2013, 2016; Kretschmar et al., 2017; Obsuth et al., 2018; Pears et al., 2008; Turner et al., 2016). In addition, cluster analysis was also used to define which victimization types are clustering to one another (e.g., Álvarez-Lister et al., 2014; Higgins, 2004; Holt et al., 2007; Holt & Espelage, 2003). At times, studies with longitudinal victimization characteristics examined changes over time; Turner et al. (2017) classified these as stable low, decreasing, increasing, and stable high polyvictimization groups, and Davis et al. (2020) separated groups as sustained polyvictimization, moderate/decreasing victimization, and low victimization.
Associated Health Outcomes
Supplementary Appendix A shows a wide range of associated health outcomes with polyvictimization. Among the 96 studies, 93 studies (96.88%) investigated mental, behavioral, and/or social health aspects, 11 studies (11.46%) examined physical health conditions, and 12 studies (10.42%) analyzed general health, such as quality of life, life satisfaction, overall health status, daily functioning, well-being, or coping capacity (these classifications are not mutually exclusive as some studies investigated more than one category of health outcomes).
Other Characteristics
Victimization Perpetrator, Frequency, and Severity
Twenty-one studies incorporated the victimization characteristics of perpetrator, frequency, and/or severity as part of the polyvictimization construct, while a majority of the included studies did not incorporate such aspects in the polyvictimization construct. The number of studies that incorporated one or a combination of these characteristics is summarized (Figure 2), and the studies that incorporated these aspects are identified (Supplementary Appendix A). Number of studies that did and did not report victimization perpetrator, frequency, and severity.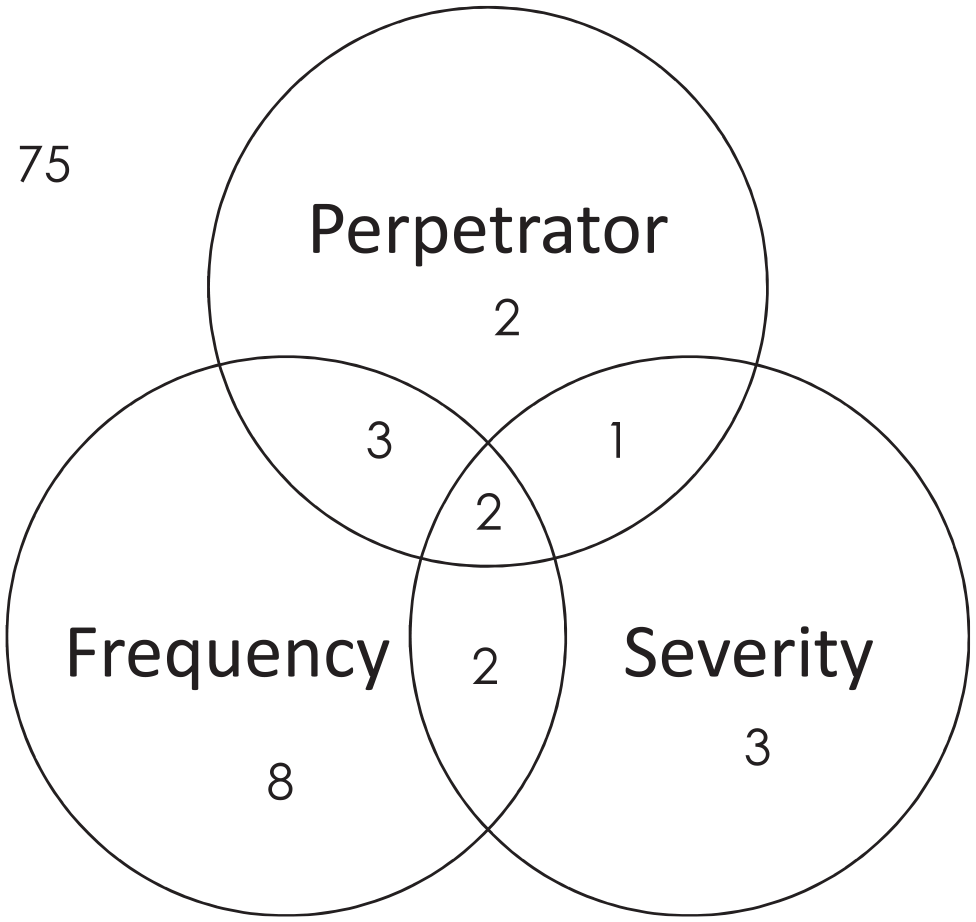
Country of Sample Recruitment
More than half of the studies (56.25%) had samples drawn from the U.S., 10 studies (10.42%) from Spain, five studies (5.21%) from Canada, four studies (4.17%) from Sweden, and three studies (3.13%) from England. One to two studies (1.04–2.08%) have been conducted on this topic with samples from other parts of the world (i.e., Austria, Brazil, China, Denmark, Hong-Kong, Australia, Belgium, Cambodia, Chile, Finland, Haiti, India, Kenya, Netherlands, Nigeria, Norway, South Africa, Switzerland, Taiwan, UAE, Uganda, and Vietnam) (Figure 3). Number of country of sample recruitment among the included studies (n = 96).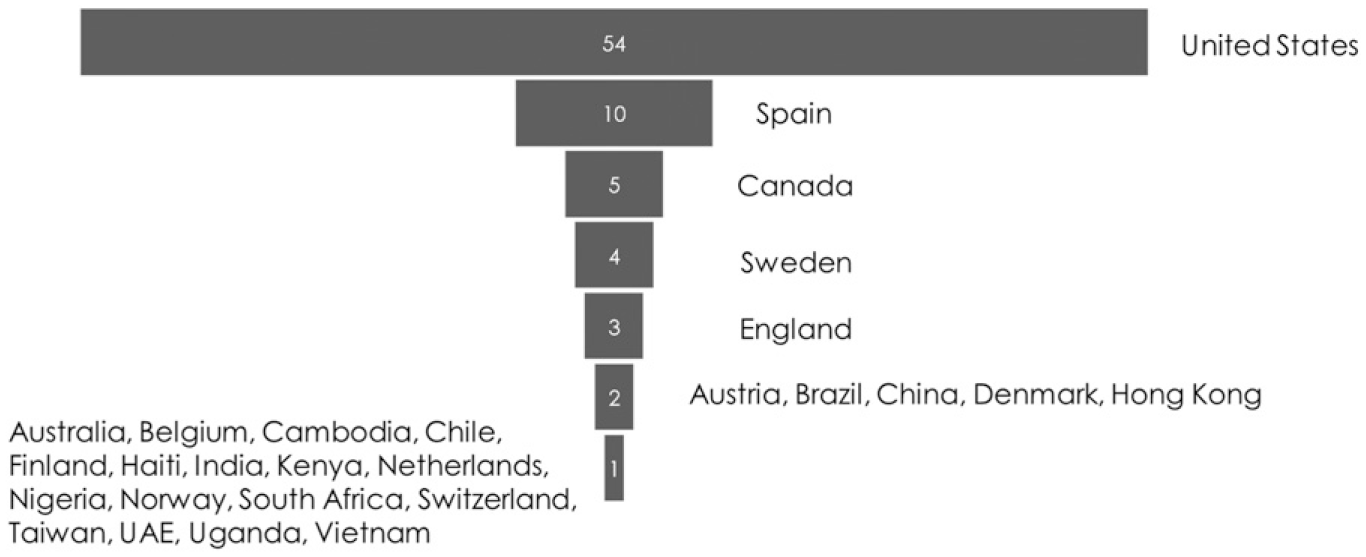
Female/Male Percent in Samples
87 studies reported what percent of their sample was female or male. While eight studies had female only samples and one study had a male only sample, generally, female percent was evenly distributed across different samples with a majority of sample being females (55.17%) or males (44.83%). Female percent is documented (Supplementary Appendix A).
Publication Years
Despite the fact that the term “polyvictimization” itself was first used in 2007 in the field of violence (Finkelhor et al., 2007a), while most studies (86.46%) were published after 2007, the concept of multiple types of violence exposure was used prior to 2007 as in seven studies (7.29%) and in 2007 in six studies (6.25%) included in our review (Supplementary Appendix A).
Discussion
Critical Findings.
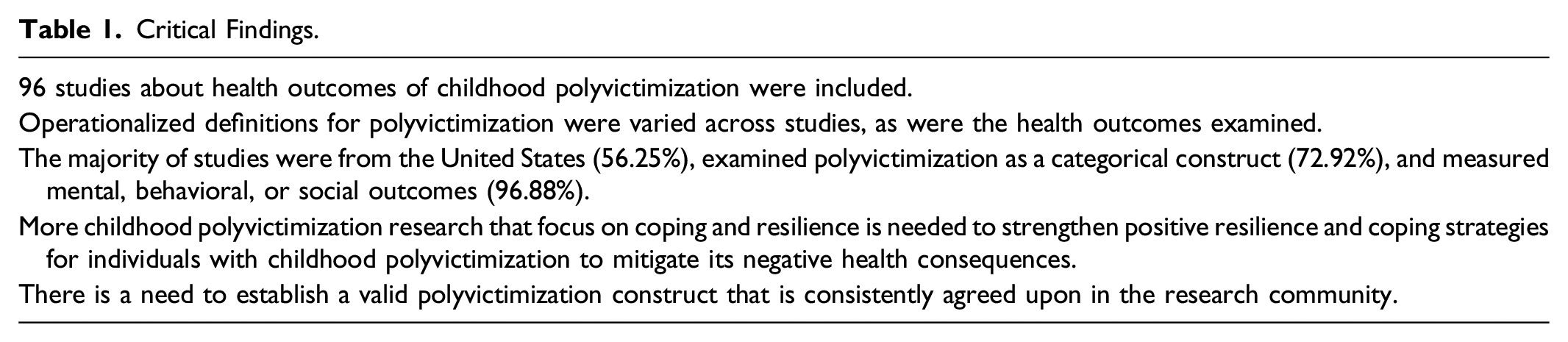
This review indicated the significant volume (96 studies) of currently available published and unpublished studies on childhood polyvictimization and its associated health outcomes and documented the varied constructs currently in play in the scientific literature focused on these associations. By examining these constructs, the review identified general patterns in operationally defining polyvictimization, consisting of varied approaches for constructing continuous (two identified) and categorical variables (four identified). These findings offer a valuable addition and summary of the current literature that can be referenced by future researchers as they make decisions for operationalizing polyvictimization. It is currently challenging to specifically summarize patterns of the types/number of victimizations which constitute polyvictimization given that they vary significantly from study to study. More research is warranted to assist researchers in the best approach for such classifications. These variations illuminate the importance of developing an agreed upon unbiased standard measurement of polyvictimization that can answer clinically meaningful questions across studies and contexts in evidence synthesis.
More specifically, a consensus on a polyvictimization construct amongst clinical and research experts, as well as the development of an instrument that would allow for unbiased standard measurement of polyvictimization, are warranted. While the existing literature on polyvictimization can inform these next steps, more research is also needed to examine what specific victimization types have sufficient strength of evidence and better understand the victimization thresholds that define polyvictimization. One way to achieve this goal would be developing a commonly agreed hypothesized measurement model based on theory and previous analytic research and testing validity and reliability of the construct by using statistical methods such as confirmatory factor analysis on different populations. A consistent and comprehensive body of measures that could include various approaches to delivery (e.g., clinical interview, self-report, record review, and multi-informant interview) and allow for the flexibility of the various types of study methods in this field of study would be beneficial to future research, clinical practice, and program evaluation. At the same time, an approach to instrument development that ensures a sound theoretical framework and practical approach to efficient and cost-effective assessment for clinical intervention programs for polyvictimized patient groups must be prioritized (Davis, 1996).
In terms of health outcomes, the majority of studies (93 studies, 96.88%) analyzed mental, behavioral, or social health outcomes while fewer studies investigated physical (11 studies, 11.46%) or general (10 studies, 10.42%) health outcomes. It may be that childhood polyvictimization has more direct relationships with mental, behavioral, and social health outcomes as they are highly impactful on the short-term outcomes of focus in childhood (school, peer, and relational success). It may be that physical and general health outcomes are there but not regularly assessed, or it may be that the mental, behavioral, and social health outcomes serve as mechanisms for more long-term health outcomes. Regardless, it is difficult to fully understand the true associations until there is an established operational definition of polyvictimization and more consistency among the health outcomes of study. Further, even when a consensus definition of polyvictimization is established, it is likely that victimization characteristics and other demographic or individual level factors may moderate or mediate the extent of health outcomes children experience. Thus, while this review clearly highlights the need of standard instrument development of polyvictimization, more longitudinal studies that follow youth transitioning from childhood to adulthood and that ensure a comprehensive approach to measuring health and well-being as well as potential mechanistic drivers of these associations are warranted to better explicate outcomes associated with childhood polyvictimization. There are existing datasets that would allow for such investigations (e.g., the National Longitudinal Study of Adolescent to Adult Health or the Longitudinal Studies of Child Abuse and Neglect) and this is an imperative next research step for this field of study.
As to knowledge evidences and gaps, the list of victimization types, polyvictimization construct schemes, and associated health outcomes are identified (Supplementary Appendix A); based on this list, future studies can navigate which investigations are further necessary for increasing our understanding of the impact of specific victimization types, strengthening current construct schemes, exploring additional analytic schemes, or analyzing certain health outcomes. In particular, more studies are needed that investigate coping strategies and resilience. It was surprising to note that despite all the studies focused on negative health outcomes of polyvictimization, there was only one study that investigated coping strategies as health outcomes (Kirchner et al., 2020). Thus, it is evident that childhood polyvictimization studies that focus on coping and resilience are much needed to understand how to best strengthen mental stamina for individuals who experienced violence victimization in childhood. In addition, given that most of the studies used samples from the U.S., more studies in different regional contexts should be also encouraged, especially for global settings where prevalence of polyvictimization may be higher (Le et al., 2018).
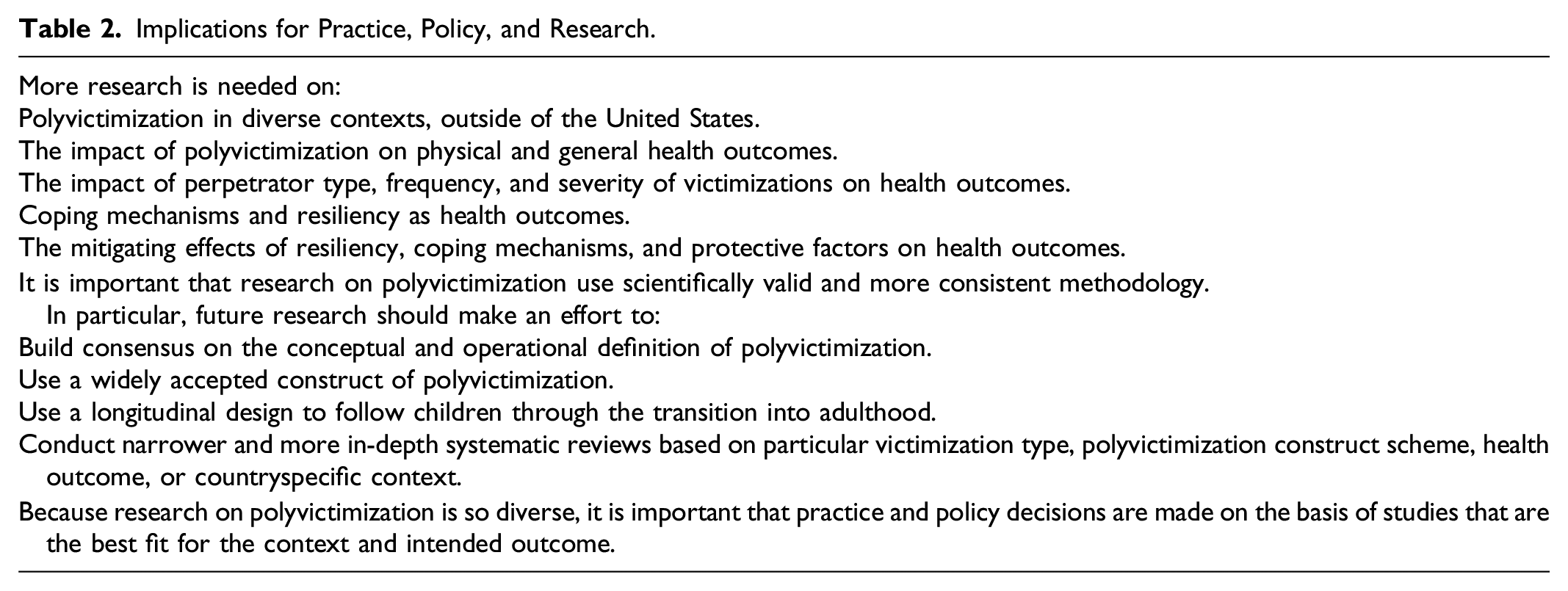
Implications for Practice, Policy, and Research.
Strengths and Limitations
Our review should be interpreted based on its strengths and limitations. Among many strengths, this review was conducted with a strong team of reviewers and experts both in methods and content. Additionally, it undertook the most rigorous approach, including double-screening, double-coding, searching for gray literature, and citation mining. Importantly, through citation mining, our team located seven additional studies dated prior to 2007 and six additional studies dated in 2007. Without the citation mining, based on the initial literature search alone, this review would have resulted in 54 studies, which is about a half of our final set of studies. This suggests the importance of citation mining in following the most rigorous systematic review approach to yield a complete and comprehensive set of eligible studies. Further, this was the first study that presented the varied construct of polyvictimization, which is a much-needed topic that has not been addressed in childhood violence research. Additionally, including samples from all countries and all years broadened the scope of the literature and advanced comprehensiveness of the review.
Nonetheless, this review has several limitations. First, this review was not able to comment on the robustness or rigor of the included studies. Next, although rigorous, human errors may have occurred in screening or coding studies. Lastly, as our review included studies with only English language, geographical and cultural diversity could have been limited.
Conclusions
To our knowledge, this is the first review of both published and unpublished studies that explores childhood polyvictimization and its associated health outcomes. This review covers the scope of the current literature, documents the varied constructs of polyvictimization and associated health outcomes, and highlights existing evidences and gaps. It is important to increase understanding of how polyvictimization can best be structured to improve the validity of research on this topic as well as what health outcomes should be prioritized when investigating, designing, and implementing secondary prevention interventions. Relatedly, examining approaches to strengthen positive resilience and coping strategies for individuals with childhood polyvictimization in order to reduce detrimental health consequences across the lifespan is an area of great need. This review can help direct future research to narrow the research gap and build consensus on this emerging and important topic of childhood polyvictimization.
Supplemental Material
sj-pdf-1-tva-10.1177_15248380211073847 – Supplemental Material for Childhood Polyvictimization and Associated Health Outcomes: A Systematic Scoping Review
Supplemental Material, sj-pdf-1-tva-10.1177_15248380211073847 for Childhood Polyvictimization and Associated Health Outcomes: A Systematic Scoping Review by NaeHyung Lee, Terri Deocampo Pigott, Ashley Watson, Katherine Reuben, Kathryn O’Hara, Greta Massetti, Xiangming Fang and Shannon Self-Brown in Trauma, Violence, & Abuse
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplement material for this article is available in online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.