
Abstract
The Asian American, Native Hawaiian, and Pacific Islander (AANHPI) population is rapidly growing in the United States. Despite sexual violence being a persistent and significant public health issue, research on this topic among AANHPIs is lacking. The study objective is to conduct a systematic scoping review on the published literature on non-partner sexual violence among AANHPIs to identify gaps and priorities to inform actionable research. The systematic review was conducted following the PRISMA Protocol for Systematic Reviews. Database searches were conducted of MEDLINE, Embase, PsycINFO, and Cochrane Central of Clinical Trials, along with and AgeLine and CINAHL for peer-reviewed articles describing non-partner sexual violence among AANHPIs. The search was limited to articles in English published after 1990. Each citation was reviewed by two trained independent reviewers, with a third researcher resolving any conflicts. Of the 998 articles screened and subsequently 496 full-text articles assessed for eligibility, 38 articles were included in the final analysis. The majority of studies did not report disaggregated data for AANHPI subgroups, with most focusing on East Asian subgroups and little evidence on NHPI communities. Most studies were cross-sectional, quantitative, and employed non-probability sampling. There was a lack of studies on effectiveness of interventions and validity of sexual violence-related measures. Our review provides a first step in mapping the extant literature on non-partner sexual violence among this underserved and under-researched population and will serve as a guide for future research, policy, and intervention.
Introduction
The World Health Organization (WHO) reports that globally, 7% of women and girls 15 years and older have experienced non-partner sexual violence over their lifetime (World Health Organization, 2013). Sexual violence is a widespread issue in the United States, where 1 in 5 women report having experienced sexual violence in their lifetime (Breiding, 2014). However, gender-based violence in the United States generally remains an underfunded issue relative to its incidence, which annually is higher than that of other chronic diseases such as cardiovascular disease, cancer, diabetes, and HIV/AIDS combined according to data from 2013 (Waechter & Ma, 2015). Costs associated with rape and attempted rape (including treatment for the victim/survivor and loss of earnings) are estimated to be over $900 billion dollars each year (Waechter & Ma, 2015).
Asian American, Native Hawaiian, and Pacific Islander (AANHPI) populations are one of the fastest growing racial/ethnic minority groups in the United States, with the collective population estimated to reach 33.4 million individuals by 2050 (Hixson et al., 2012; Islam et al., 2010). AANHPI populations experience a variety of health disparities, though often masked by the aggregation of AANHPI subgroups (Islam et al., 2010). The lack of research and data on AANHPI contribute to the limited understanding of the prevalence of sexual violence and related help-seeking behaviors in the community. Furthermore, the model minority myth, or the idea that Asian individuals experience positive health outcomes, is a falsely constructed and harmful notion that masks the true health disparities among many Asian subgroups (Lam & Hui, 2016; Yi et al., 2016).
According to 2019 Census estimates, nearly one-third of all foreign-born individuals in the United States were born in Asian countries, constituting a large proportion of immigrants (US Census Bureau, 2019). As of 2017, 59% of Asian Americans (AAs) were estimated to be born in another country (López et al., 2017). Immigrants face a variety of health disparities, partly driven by lack of culturally and linguistically competent health care and social service access (S. Lee et al., 2010). Studies that characterize the broader needs of AA immigrant populations suggest that the lack of institutional support, such as lack of interpretation services, culturally competent health practitioners, and health insurance for undocumented individuals, contribute to negative health outcomes in the community (G. Kim et al., 2011; Sudhinaraset, Ling, et al., 2017; Sudhinaraset, To, et al., 2017).
CDC’s National Intimate Partner and Sexual Violence Survey (NISVS) is an ongoing, nationally representative telephone survey dedicated to solely monitoring intimate partner and sexual violence among adult women and men in the United States. NISVS data indicates that 19.3% of all women have experienced rape in their lifetime, while 43.9% are estimated to have experienced other types of sexual violence (Breiding, 2014). Overall, 31.9% of Asian and Pacific Islander (API) women have experienced other sexual violence not including rape (e.g., sexual coercion, unwanted sexual contact, and unwanted non-contact sexual experiences), which is lower than that of all other racial/ethnic groups (Breiding, 2014). Lifetime prevalence rates of rape or stalking for API women are not available due to unreliable estimates stemming from insufficient case counts in data sources. Data specific to Native Hawaiian and Pacific Islander (NHPI) groups are often missing or aggregated with AAs due to small sample sizes. One study reported higher prevalence of sexual violence among NHPIs compared to white and AA counterparts, where NHPIs reported experiencing two to three times more sexual assault over a 12-month period (Crisanti et al., 2011).
AANHPI survivors of sexual violence likely face heightened barriers to reporting assaults, which is reflected through the low prevalence of help-seeking behaviors observed across various mental and physical health concerns (Abe-Kim et al., 2007; Gandhi et al., 2018; W. Kim & Keefe, 2010; Tran et al., 2016). Yet, little is known on help-seeking behaviors following sexual violence among AANHPI survivors, and to date, no literature is available on help-seeking behaviors of NHPI populations in regard to sexual violence. While mental health disorders, such as depressive episodes and post-traumatic stress disorder (PTSD), are often associated with help-seeking behaviors among sexual violence survivors, some studies suggest that AAs may display lower help-seeking behaviors following non-partner sexual violence experiences as well (M. Y. Lee & Law, 2001; Lewis et al., 2005). Additionally, one study also suggests that AA individuals are less likely to use formal reporting and support structures (i.e., healthcare professionals), and instead turn to friends and family first (M. Y. Lee & Law, 2001). Family- and community-level barriers, such as cultural stigma around sex and mental health and subsequent shame and guilt surrounding sexual violence and its impact, also contribute to negative attitudes and lower likelihood of help-seeking among AANHPI individuals (M. Y. Lee & Law, 2001). Furthermore, the internalization of the model minority myth further constrains help-seeking, as AA individuals may perceive themselves as less in need of help (P. Y. Kim & Lee, 2014; M. Y. Lee & Law, 2001).
Non-partner sexual violence against AANHPI individuals in the United States is inextricably shaped by the intersection of both racism and sexism. Intersectionality theory contends that AANHPI women’s experience of racism is inseparable from their experience of sexism due to their embedded social identities (Crenshaw, 1989; Essed, 1990). In particular, the exotification and fetishization of AANHPI women are contributors to the unique violence that survivors experience (Mukkamala & Suyemoto, 2018). For example, the archetypes of being passive, submissive, or exotic are often ascribed to Asian women, which is derived from a history of sexual violence toward them. The long history of U.S. militarization of Asian countries and the sexual exploitation and violence toward Asian women in those respective regions (e.g., Vietnam, Korea, and Hawaii) continue to be perpetuated as commonplace tropes in media (Matsumoto, 2020; Medeiros, 2018).
Accordingly, the objective of the current scoping review is to systematically review the peer-reviewed literature regarding non-partner sexual violence among AANHPIs to characterize the knowledge gaps and identify actionable research priorities faced by this under-researched population. A scoping review uses systematic and rigorous methods but differs from a systematic review in that it does not have a specific research question. Instead, scoping reviews seek to provide a broad overview of the available literature, and as a result, often include a greater number and range of study designs (Pham et al., 2014).
Methods
Inclusion and Exclusion Criteria
This scoping review on non-partner sexual violence was part of a larger scoping review that aimed to capture peer-reviewed literature on various types of gender-based violence among AANHPI populations. The inclusion criteria for the larger review included articles that reported on Asian American and Native Hawaiian (AANH) populations residing in the United States as well as Pacific Islanders residing in the United States or Pacific Islands and published after 1990. Sexual and gender minority populations were included in the search. Exclusion criteria included articles not in English, non-research articles (e.g., letters to the editor), and articles that focused on non-survivors (e.g., perpetrators, witnesses, and service providers). The current review focuses specifically on non-partner sexual violence among adults and excludes articles strictly reporting on intimate partner violence or childhood sexual violence. Non-partner sexual violence was defined as all contact and non-contact sexual violence, including rape, attempted rape, sexual harassment, stalking, and sexual coercion.
Search Strategy
The literature search was conducted in December 2019 following the PRISMA Protocol for Scoping Reviews (Moher et al., 2015). A database search was conducted of MEDLINE, Embase, PsycINFO, and Cochrane Central of Clinical Trials, using the Ovid Search Platform along with and AgeLine and CINAHL using the EBSCO search platform for peer-reviewed articles describing gender-based violence among AANHPIs. The Ovid Medline search strategy is included as an appendix to this article (See Appendix A).
Review Process
Duplicate articles were identified and removed from the database prior to and during screening. Each citation was reviewed by two trained independent reviewers (OP, SM, CL, SLee, DC) and conflicts were resolved by a third reviewer. Citations were managed using Covidence, software to systematic review data management (Covidence, 2021). Thematic synthesis was guided by an approach outlined by Arksey and O'Malley (2005), which involved description of data by themes identified a-priori (i.e., see key categories outlined in Table 2) and an iterative six-stage process: (1) identifying the research question, (2) identifying relevant studies, (3) study selection, (4) charting the data, (5) collating, summarizing and reporting the results, and (6) an optional consultation exercise (Arksey & O'Malley, 2005).
Results
Description of Studies
The preliminary search of the electronic databases identified 1073 potentially relevant articles. After removal of duplicates, 998 articles remained. Screening by title and abstract resulted in 496 articles for full-text review. Most common reasons for exclusion were 1) not a research article; 2) wrong study population; and 3) article did not disaggregate results specifically for AANHPI individuals. Full-text review resulted in 252 articles focused on all types of gender-based violence. Among the 252 articles, 38 articles focused on non-partner sexual violence among AANHPI adults and were analyzed for the current scoping review. Figure 1 is a consort diagram outlining the search process, including reasons for excluding studies at each stage. Summary of search strategy per PRISMA guidelines.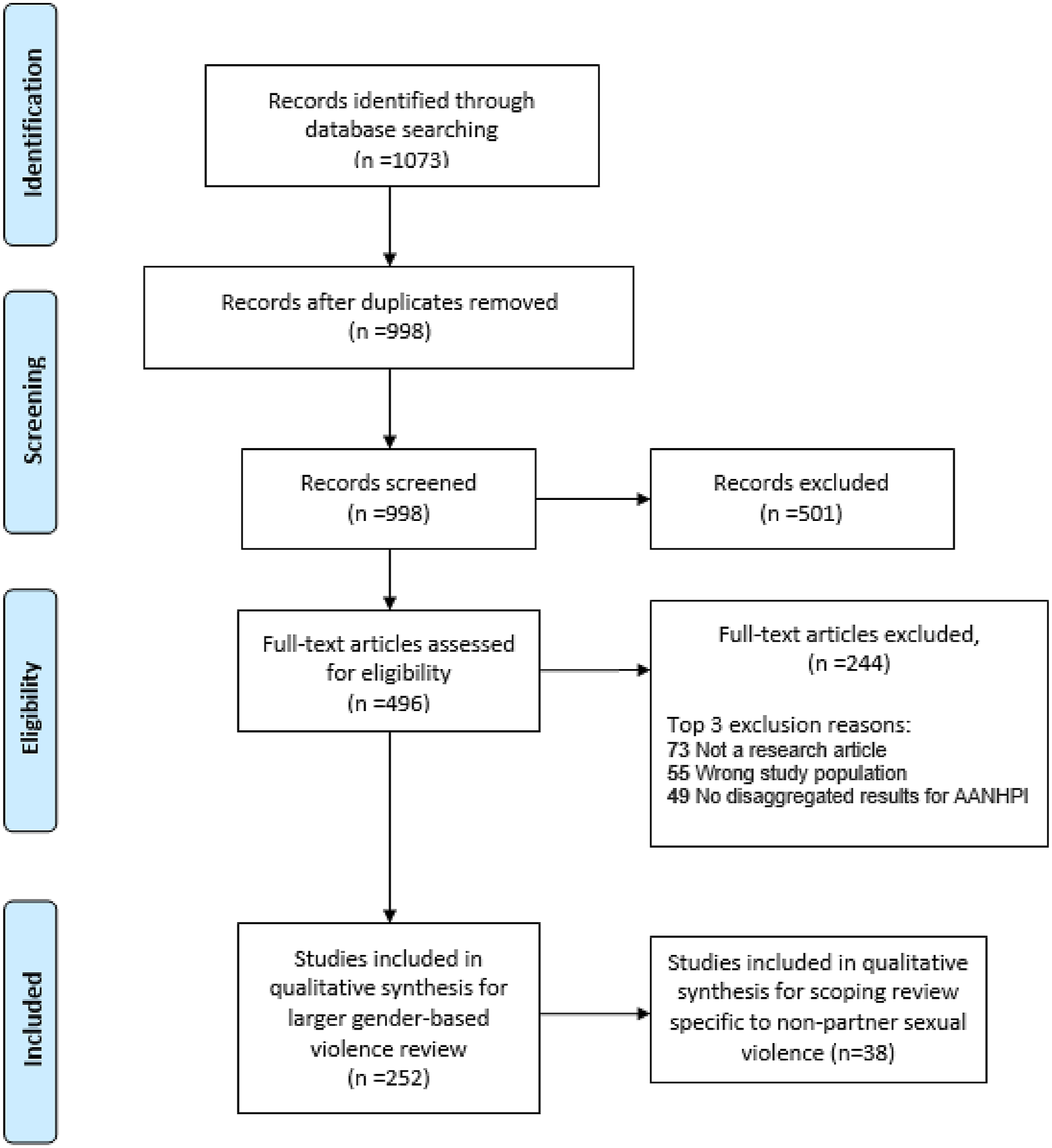
Ethnic Grouping of Included Studies.
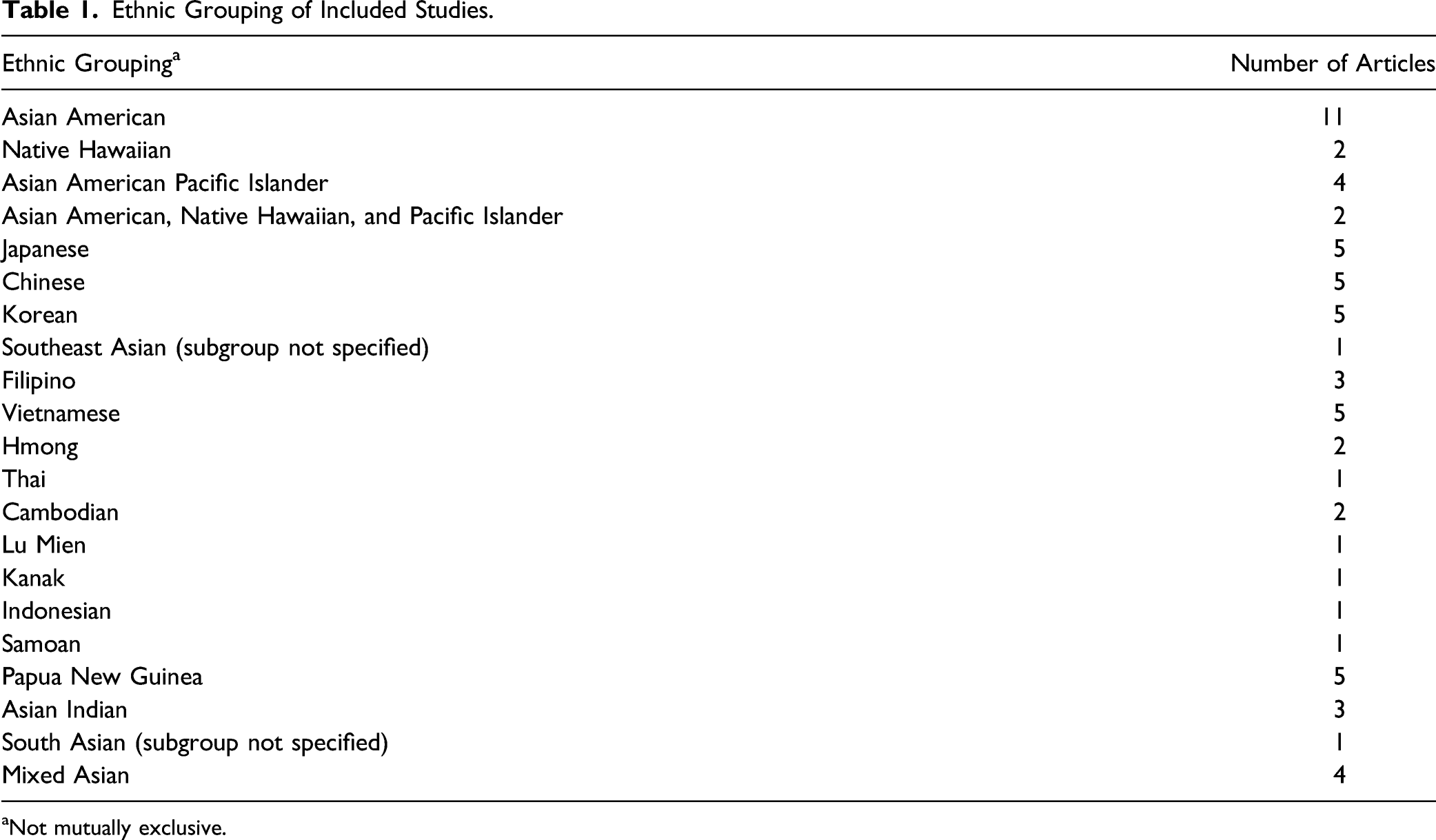
aNot mutually exclusive.
Study Characteristics of Included Studies.
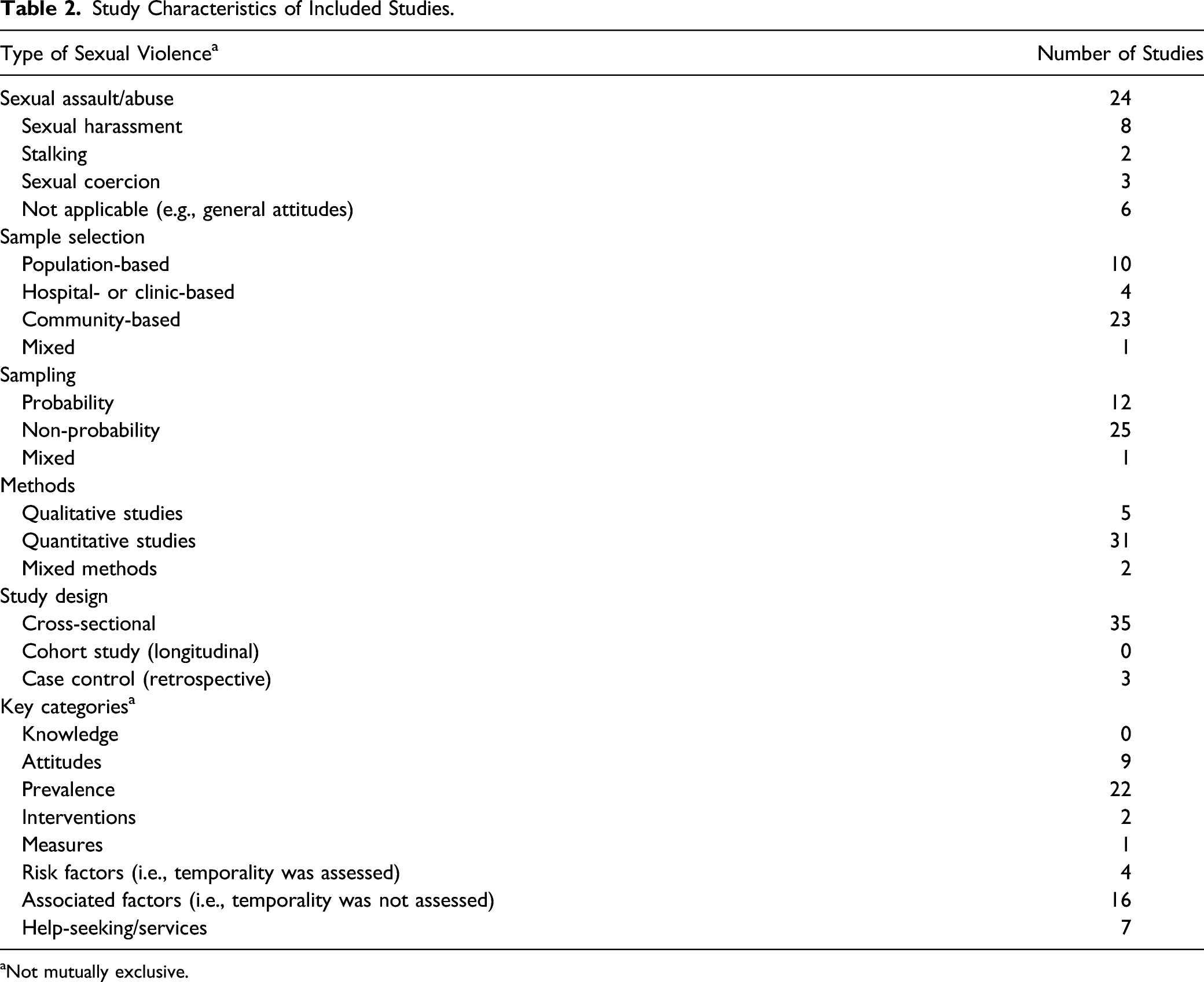
aNot mutually exclusive.
Prevalence
Our review found 22 studies on the prevalence of non-partner sexual violence among AANHPIs (Blaisdell-Brennan & Goebert, 2001; Buchanan et al., 2018; Crisanti et al., 2011; Dibble et al., 2007; Dir et al., 2018; Foynes et al., 2014; Hahm et al., 2017, 2012; Ho et al., 2018; Jewkes et al., 2013; Jewkes, Fulu, et al., 2017; Jewkes, Jama-Shai, & Sikweyiya, 2017; Kalof et al., 2001; Lokuge et al., 2016; McLaughlin et al., 2019; Mills & Granoff, 1992; Morris & Balsam, 2003; Roberts et al., 2011; Urquiza & Goodlin-Jones, 1994; Vang & Bogenschutz, 2014; Yoshihama, 2001b; Yoshihama & Horrocks, 2005). A majority of the studies assessed lifetime sexual violence by asking respondents about their history of different types of sexual harassment and sexual assault.
Most of the studies were conducted in the United States, and four were conducted in Papua New Guinea (Jewkes et al., 2013; Jewkes, Fulu, et al., 2017; Jewkes, Jama-Shai, & Sikweyiya, 2017; Lokuge et al., 2016). The studies based in Papua New Guinea showed that around 15% of women in Papua New Guinea reported health service visits due to rape by a non-partner during the study period from August 2010 to April 2013 (Jewkes et al., 2013; Jewkes, Jama-Shai, & Sikweyiya, 2017; Lokuge et al., 2016).
Studies Conducted With Multiple Race/Ethnicities
Studies assessing racial/ethnic differences in prevalence between AANHPIs and non-AANHPIs showed consistent results. According to several population-based studies, rates of sexual violence were lower among AA women compared to non-AA racial/ethnic groups (Foynes et al., 2014; McLaughlin et al., 2019; Morris & Balsam, 2003; Roberts et al., 2011; Urquiza & Goodlin-Jones, 1994). Specifically, two studies reported that the lifetime prevalence of rape (2.96%), sexual assault (7.98%), and stalking (5.37%) were lowest among AA women compared to African Americans, Whites, and Latinas (McLaughlin et al., 2019; Urquiza & Goodlin-Jones, 1994). In college-based samples, 4% of AA women reported a lifetime history of sexual assault in which the victim was physically incapacitated (e.g., due to alcohol consumption) compared to 11% of White women, and 34% of AA students reported at least one sexual harassment experience compared to 39% of White students (Dir et al., 2018; Kalof et al., 2001). In addition, AA college students reported substantial sexual harassment including unwanted gender-based harassment (32.8%), unwanted sexual attention (10.9%), and sexual coercion (3.2%); overall sexual harassment among AA students was 33%, which was the second highest after White students (Kalof et al., 2001).
Studies Conducted in Asian Americans Only Samples
Some studies included multiple AA subgroups, but did not present disaggregated results by AA subgroup. A couple of community-based studies indicated that roughly 15% of AA women had a history of rape in their lifetime (Hahm et al., 2012, 2017). Two school-based studies showed that more than half of AA college women experienced at least one form of sexual harassment: 66.7% reported having at least one sexual harassment experience during the past year in college (Buchanan et al., 2018) and 91% of participants reported at least one sexual harassment event within the past 24 months (Ho et al., 2018). Two studies reported that around 35% of Japanese American women had experienced sexual violence perpetrated by a non-partner, such as unwanted touching of breasts and genital areas, stalking, and being forced to have sex during their lifetimes (Yoshihama, 2001b; Yoshihama & Horrocks, 2005). One study focused on sexual minority women and reported that 20% of AANHPI lesbian individuals experienced sexual abuse during adulthood (Dibble et al., 2007).
Studies comparing differences in prevalence across AANHPI subgroups were inconclusive. A community-based study in Hawaii found that lifetime prevalence rate of sexual assault among indigenous Hawaiian women (19.0 per 100 women) was higher than Japanese and Filipino women (7.5 per 100 women, 7.9 per 100 women, respectively) (Blaisdell-Brennan & Goebert, 2001). Another study in Hawaii showed similar patterns (Crisanti et al., 2011). In contrast, a study using a school-based sample reported that the number of Japanese college women who had been raped, sexually assaulted, and touched or forced to touch their perpetrator was highest compared to Native Hawaiian and other AA (Chinese, Filipino, Mixed Asian) women during their lifetime (Mills & Granoff, 1992).
Measures
One study examined the validity of a measure for sexual harassment frequency and labeling—Sexual Experiences Questionnaire (SEQ)—among AA women (Buchanan et al., 2018). Psychometric testing showed high reliability and validity and confirmed a three-factor structure (i.e., gender harassment, unwanted sexual attention, and sexual coercion) of the SEQ, aligning with findings from previous studies (Buchanan et al., 2018).
Attitudes
A total of nine articles discussed AA attitudes and perceptions around non-partner sexual assault; no studies explicitly included attitudes and perceptions from NHPI respondents (Devdas & Rubin, 2007; Foynes et al., 2014; Ho et al., 2018; Koo et al., 2015; J. Lee et al., 2005; M. Y. Lee & Law, 2001; Schneider et al., 2009; Tummala-Narra et al., 2017; Tummala-Narra et al., 2019).
Studies Conducted With Multiple Race/Ethnicities
A study comparing AAs with Hispanics and Whites found that Whites perceived the benefits of treatment for rape injuries (physical and mental) to take effect more quickly than AAs, potentially pointing toward the belief held by AAs that the consequences of sexual assault linger and that the course to recovery takes longer (Schneider et al., 2009). This study also found that relative to women, men are more likely to view rape victims as responsible for their assault; however, no ethnic differences were found between AAs, Whites, and Hispanics on their views of victim blaming, victim responsibility, and victim judgment. In addition, AA college students were more likely to endorse victim blaming attitudes compared to their White counterparts (J. Lee et al., 2005).
Studies Conducted in Asian American Only Samples
One study examined sexual violence-related attitudes among AA women and men and reported that compared to Japanese, Korean, and Southeast Asians (i.e., Cambodian, Laotians, and Vietnamese), Chinese Americans perceived sexual violence against women as a less serious problem (M. Y. Lee & Law, 2001); no significant differences were reported in perceptions between the women and men. A study among South Asian American women found that first generation (foreign-born) South Asian American women had higher rape myth acceptance than that of second-generation (U.S.-born) South Asian American women and European American women, suggesting that generational status has an influence on beliefs about rape (Devdas & Rubin, 2007). Similarly, participants in a qualitative study among Asian Indians spoke of a shift in cross-generational perspectives on sexual violence: responses to sexual violence differed between the United States and Indian contexts, and participants also noted that over time, older, first generation immigrant Asian Indians were more willing to talk about sexual violence (Tummala-Narra et al., 2019). Another study, with a woman-only sample, reported that there was a positive association between identification with Asian culture, and acceptance of sexual harassment myths (Ho et al., 2018). In contrast, another study among Asian Indians reported no association between ethnic identity and rape myth acceptance (Tummala-Narra et al., 2017).
Sexual Assault Disclosure and Help-Seeking
A total of seven studies addressed sexual assault disclosure and help-seeking by survivors of non-partner sexual violence (Akutsu et al., 2006; Foynes et al., 2014; Kelly-Hanku et al., 2015; Koo et al., 2015; Mills & Granoff, 1992; Roberts et al., 2011; Tummala-Narra et al., 2019). Five of the studies were conducted in the United States with data aggregated for AAs (Japanese, Chinese, Korean, Taiwanese, Filipino, Cambodian, Vietnamese, Iu Mien, Indonesian, Indian, and Mixed Asian) but none discussed differences across AA subgroups (Akutsu et al., 2006; Foynes et al., 2014; Koo et al., 2015; Mills & Granoff, 1992; Roberts et al., 2011); the studies focused primarily on East and Southeast Asians. One study conducted by Kelly-Hanku et al. (2015) was based in Papua New Guinea, and one study by Tummala-Narra et al., (2019) was conducted among Asian Indians (Kelly-Hanku et al., 2015; Tummala-Narra et al., 2019).
Lack of knowledge on what is considered sexual assault, fear of reprecussions from authorities, cultural concerns about disrupting peace within family and social circles, fear of reliving the experience, and belief in the futility of reporting were observed to be barriers preventing disclosure and help-seeking (Kelly-Hanku et al., 2015; Koo et al., 2015; Mills & Granoff, 1992; Tummala-Narra et al., 2019). One qualitative study among AA college women asked about help-seeking attitudes and participants expressed that AA women victims are not likely to report instances of rape by a non-partner due to beliefs of negative consequences of on relationships with parents and friends, as well as due to mistrust of authorities (Koo et al., 2015). AAs, like other racial/ethnic minority groups, were also less likely than White individuals to receive treatment for PTSD related to unwanted sex (Roberts et al., 2011). The importance of help-seeking was emphasized in one study that observed AA women who reported a history of sexual assault to have an increased likelihood of an earlier intake after initial evaluation for mental health services (Akutsu et al., 2006).
Qualitative data revealed that South Asian American survivors face barriers to help-seeking, including the fear of discrimination, lack of culturally informed interactions with law enforcement and mental health providers, and cultural and religious stigma from family and community members (Tummala-Narra et al., 2019). Another study examined the role of Asian cultural values in disclosure of sexual abuse using the Asian Values-Revised Scale, a self-report measure assessing the adherence to Asian cultural values such as conformity to norms, family recognition through achievement, emotional self-control, collectivism, humility, and filial piety (Foynes et al., 2014). Study findings revealed that stronger endorsement of Asian values was associated with lower odds of disclosure of sexual abuse in very close victim-perpetrator relationships compared to disclosure of physical abuse, but ethnicity itself was not associated with frequency of disclosure (Foynes et al., 2014). In not very close victim–perpetrator relationships, neither ethnicity nor Asian values was associated with disclosure of sexual abuse. Accordingly, study authors suggested that AAs who have stronger Asian values may be more hesitant to disclose sexual abuse perpetrated by a very close perpetrator compared to a not very close perpetrator as a way of preserving relationships or social integrity (Foynes et al., 2014).
Risk Factors for Non-Partner Sexual Violence
Among a sample of Thai and Vietnamese women who work in massage parlors (n = 43), lack of legal documentation and sex work history was associated with non-partner sexual violence (Nemoto et al., 2004). Dir et al. (2018) used native language as a proxy for acculturation and found that non-native English speakers experienced a lower rate of sexual assault in which the victim was physically incapacitated compared to native English speakers (Dir et al., 2018). First generation Japanese immigrants experienced sexual violence (i.e., unwanted touching, sexual assault, stalking, exhibitionism, obscene phone calls, and voyeurism) at a higher prevalence compared to 1.5 (foreign-born but grew up in United States) or higher generation individuals (Yoshihama, 2001a). Other studies reported no difference in history of rape between 1.5- and second-generation immigrants (Hahm et al., 2012). Urquiza & Goodlin-Jones, 1994 studied history of child sexual violence as a risk factor for prevalence of adult rape, although reported no significant relationships among AA participants (Urquiza & Goodlin-Jones, 1994).
Cross-Sectional Factors Associated With Non-Partner Sexual Violence
In total, 16 articles discussed various cross-sectional factors (i.e., no temporal relationships were assessed) associated with non-partner sexual violence (N. T. Buchanan et al., 2009; Buchanan et al., 2018; Crisanti et al., 2011; Devries et al., 2011; Dir et al., 2018; Hahm et al., 2012, 2017; Jewkes, Jama-Shai, & Sikweyiya, 2017; Kelly-Hanku et al., 2015; McLaughlin et al., 2019; Nemoto et al., 2004; Nguyen et al., 2010; Nusbaum et al., 2005; Pape et al., 2016; Tummala-Narra et al., 2019; Yoshihama, 2001a). Articles were mostly quantitative. Most studies did now show disaggregated data for subgroups of AANHPIs, with only four studies focusing on specific subgroups (Hahm et al., 2017, 2012; Nemoto et al., 2004; Yoshihama, 2001a). Most studies were conducted with individuals identifying as women, with only a few studies that include men (N. T. Buchanan et al., 2009; Crisanti et al., 2011; Jewkes, Jama-Shai, & Sikweyiya, 2017; Kelly-Hanku et al., 2015; McLaughlin et al., 2019).
Physical Health and Well-Being
Three studies looked at associations between non-partner sexual violence and life satisfaction. The results were inconclusive, with two studies reporting a negative association between life satisfaction and attempted/completed sexual assault (Crisanti et al., 2011; Kelly-Hanku et al., 2015) and one study demonstrating no association between sexual harassment and life satisfaction (N. T. Buchanan et al., 2009). Other studies looked at more specific aspects of sexual and physical health. History of rape was observed to be associated with increased risk behaviors for sexually transmitted diseases, driven by inconsistent condom use by participants, and non-consensual, unprotected anal sex (Hahm et al., 2017; Kelly-Hanku et al., 2015). Another study reported an association between history of sexual coercion and greater number of sexual concerns presented during gynecological care (Nusbaum et al., 2005). A study by Hahm et al. (2012) also reported an association between rape and lower perceived control and power within a relationship (Hahm et al., 2012). A qualitative study in Papua New Guinea reported that fear of being sexually assaulted during transportation was a barrier to women attending mammogram screenings (Pape et al., 2016).
Substance Use
Few studies discussed relationships between non-partner sexual violence and substance use. Prevalence of rape in which the victim was physically incapacitated was associated with heavy drinking and higher frequency of alcohol-related consequences, such as negative impact on functioning and feeling of shame (Dir et al., 2018; Nguyen et al., 2010). Higher prevalence of rape in which the victim was physically incapacitated was also associated with holding more beliefs about alcohol’s ability to lower sexual inhibitions (Dir et al., 2018). Alcohol abuse and using alcohol as a coping mechanism were also factors associated with a history of rape (Hahm et al., 2017; Jewkes, Fulu, et al., 2017). Moreover, studies reported a relationship between history of rape or attempted sexual assault and use of other substances, such as cigarettes, marijuana, and illicit drugs (Crisanti et al., 2011; Hahm et al., 2017; Jewkes, Fulu, et al., 2017).
Mental Health
Eight studies explored the relationship between non-partner sexual violence and mental health, although they reported conflicting results. Crisanti et al. (2011) observed an association between unwanted sexual experiences and poor mental health in the past 30 days among AAs (Crisanti et al., 2011), while Yoshihama (2001a) reported no association between history of sexual violence and recent psychological distress among Japanese Americans (Yoshihama, 2001a). Likewise, some studies reported depression and suicide attempts to be associated with a history of r rape (Hahm et al., 2017; Jewkes, Jama-Shai, & Sikweyiya, 2017), while others did not observe significant associations (N. T. Buchanan et al., 2009; Buchanan et al., 2018). Two studies suggested that PTSD symptoms were associated with a history of sexual coercion, unwanted sexual attention, and rape in AA participants (Buchanan et al., 2018; Jewkes, Jama-Shai, & Sikweyiya, 2017). One qualitative study among Asian Indians observed traumatic stress (including depressive symptoms, anxiety, nightmares, flashbacks, and suicidal ideation) to be a result of experiencing sexual violence (Tummala-Narra et al., 2019). Conflicting information was found in other studies that did not observe a relationship between non-partner sexual violence and mental health outcomes (N. T. Buchanan et al., 2009; McLaughlin et al., 2019).
Studies Using an Intersectional Approach
A limited number of studies explicitly applied an intersectional approach in understanding or assessing non-partner sexual violence among their participants. A few studies briefly acknowledged the role of gender and race (Ho et al., 2018; Kalof et al., 2001; Koo et al., 2015; Nemoto et al., 2004). Only two studies in our review used an explicit intersectional approach (Buchanan, Bergman et al., 2009; Buchanan, Settles et al., 2018). In a multiracial sample of college students (n = 2189; Asian/Pacific Islander n = 179), Buchanan et al. (2009) found the following: as measured by mean scores on validated sexual and racial harassment scales, study results showed that AA students reported the second highest level of sexual harassment compared to Black, multiracial, and White students; AA students reported the third highest level of racial harassment compared to their counterparts but when disaggregated by gender and race, Asian men reported the highest level of racial harassment compared to any other gender and/or racial group. Group membership had unique, additive, and interactive effects on the relationship between sexual and racial harassment on psychological well-being. Lastly, group membership moderated the relationship between harassment and psychological outcomes. In a more recent study by Buchanan et al. (2018) conducted among AA college women (n = 129), authors found that while sexual and racial harassment was a significant concern and highly correlated with one another, the interaction of race and gender was not significant likely due to the small sample size.
Interventions
Two studies described interventions addressing non-partner sexual violence experienced by API individuals (Dobbin & Kalev, 2019; Lokuge et al., 2016), but neither of the studies rigorously evaluated their efficacy or effectiveness. One paper presented descriptions and outcomes of an intervention to support survivors of gender-based violence in Lae, Papua New Guinea (Lokuge et al., 2016). The Médecins Sans Frontières (MSF)-supported program provided health services such as physical treatment, preventative care, medical examination, and counseling free of charge to survivors of gender-based violence. The majority of these patients received medical treatment for physical health, particularly post-exposure prophylaxis treatment for potential HIV infection. Outcome measures were assessed for patients over 16 years of age who received repeated sessions of mental health counseling; patients reported improvements in mental health functioning (85.0%) (Lokuge et al., 2016).
Dobbin and Kalev (2019) presented the results of sexual harassment training programs implemented by companies among women in management (Dobbin & Kalev, 2019). This retrospective study looked at interview data of operational policies and demographic censuses from 805 companies in the private sector. The proportion of women in management was used as the main outcome measure; sexual harassment often led victims to quit their positions, decreasing opportunities for rising to management. Results were presented for White, Black, Hispanic, and AA women, but without disaggregated data for AA subgroups. The authors observed that the proportion of AA women in management decreased following implementation of sexual harassment grievance procedures for employees, while the proportion increased after sexual harassment training for managers (Dobbin & Kalev, 2019).
Discussion
The current scoping review systematically aimed to summarize the peer-reviewed literature on non-partner sexual violence among AANHPIs. Overall, like many other health outcomes for AANHPIs (e.g., Alzheimer’s disease and diabetes) (Lim et al., 2020), this review found that AANHPIs are an understudied racial/ethnic minority group with regard to non-partner sexual violence. Specifically, data on national prevalence, knowledge related to sexual violence, risk factors, validation of instruments to measure sexual violence-related constructs, and effectiveness of intervention data were lacking. A major structural-level factor that impedes research with AANHPIs, including studies that disaggregate data across AANHPI subgroups, is the persistence of the model minority myth that depicts AANHPIs a monolithic, socioeconomically successful, and healthy group of individuals (Yi et al., 2016). As such, in addition to the systematic and rigorous collection of data for AANHPIs, it is important that future data collection is conducted in non-English languages to capture the experiences of diverse AANPHI populations, including those with limited English proficiency. It is also essential to include understudied Asian subgroups such as Southeast Asian or Pacific Islander populations, as current literature focuses disproportionately on East Asians.
Our review also demonstrated that there are a lack of studies that have considered how the intersection of racial/ethnic and other identities, and particularly the racialized fetishization of woman, impacts sexual violence victimization. Indeed, the majority of sexual violence research has focused on White women and generally few sexual violence studies have integrated both the impact of racism and sexism together, failing to capture the complexity of AA women’s experiences (N. T. Buchanan et al., 2009; Buchanan et al., 2018). Similarly, other multiply marginalized populations such as AANHPI sexual and gender minorities are severely understudied; a large body of research demonstrates how sexual and gender minority populations experience a disproportionate burden of adverse health outcomes, including sexual violence (Blondeel et al., 2018; Plöderl & Tremblay, 2015). Future studies should explicitly use an intersectionality framework (Bowleg, 2012; Crenshaw, 1989) and consider the impact of current sexual exploitation of AAHNHPI girls and women in their study design, analysis, and interpretation of results. Lastly, our review shows that sexual violence research among AANHPI men is similarly lacking, despite national surveillance data indicating non-partner sexual violence as a significant issue for men (Tjaden & Thoennes, 2000). In sum, additional research is needed among understudied and marginalized AANHPI subgroups, including but not limited to AANHPI sexual and gender minorities and AANHPI men.
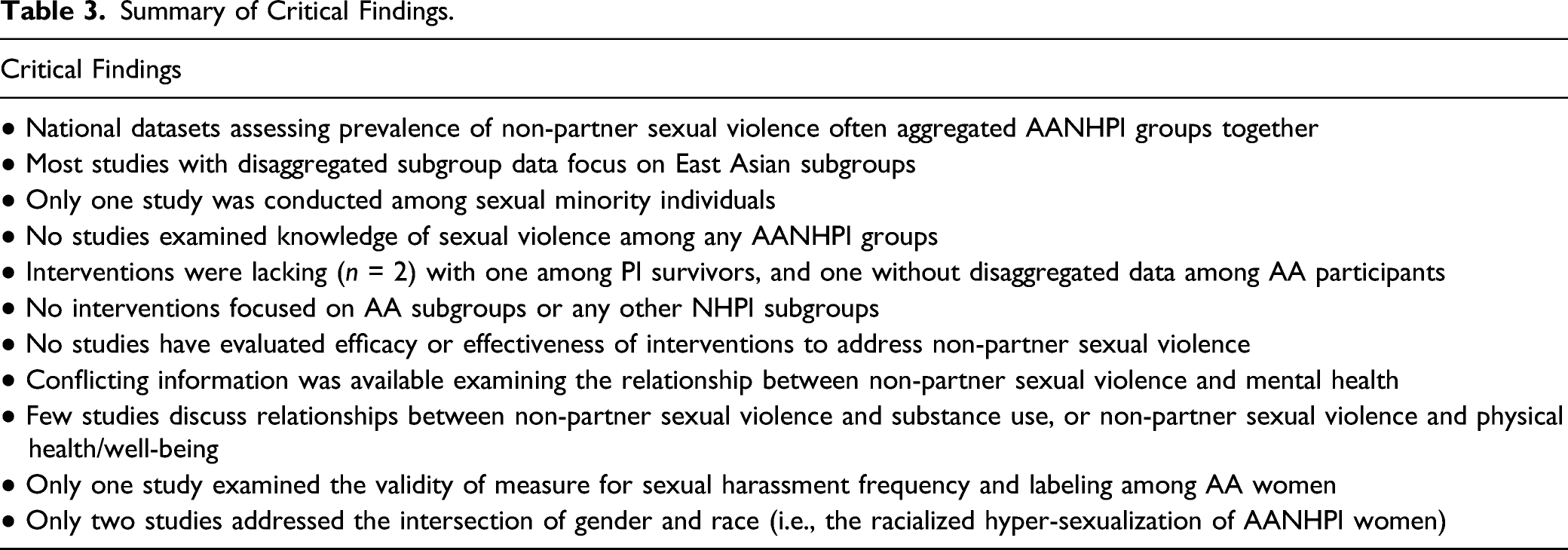
Summary of Critical Findings.
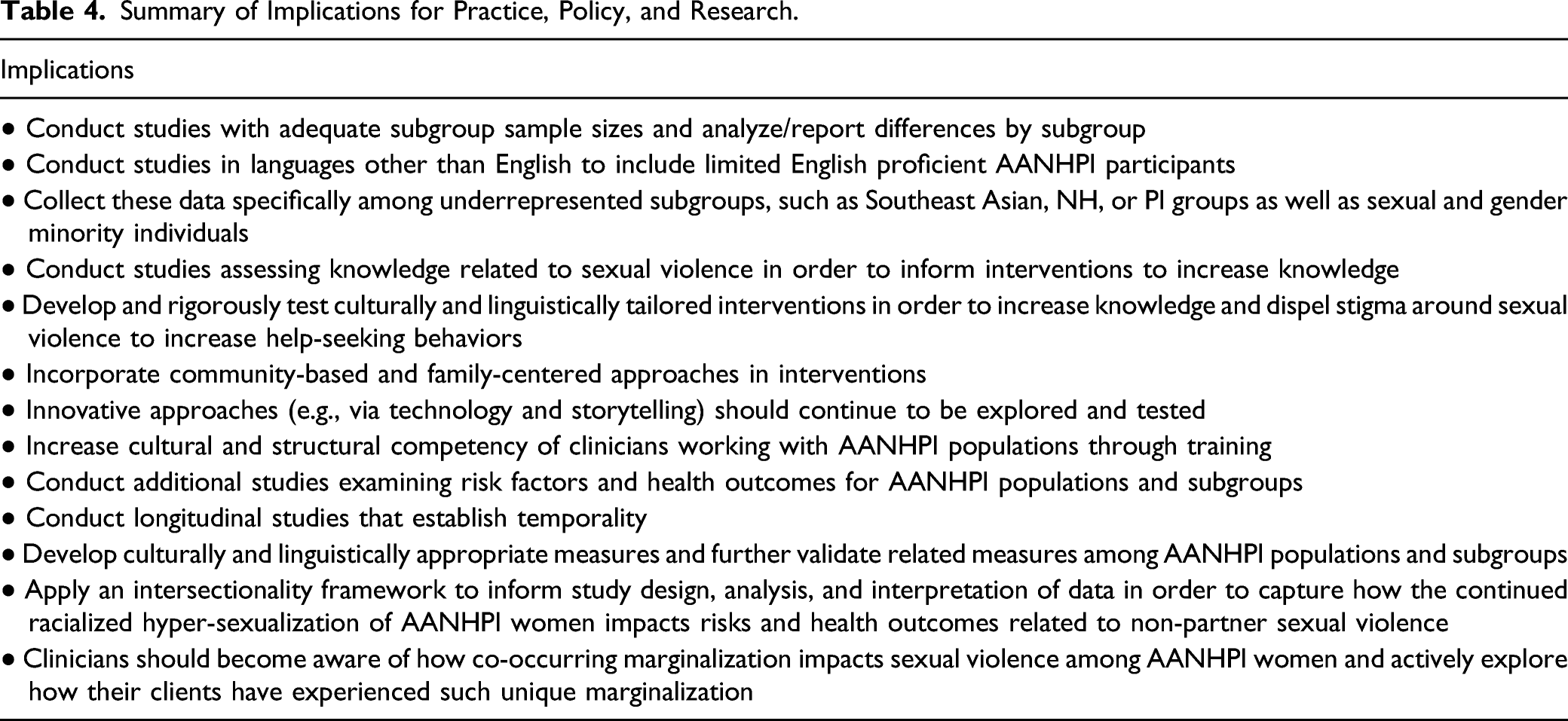
Summary of Implications for Practice, Policy, and Research.
This study was characterized by some limitations. First, this review did not assess the methodological quality of the included studies, which was beyond the scope of this review. Second, there is likely literature that provides important contextual information in informing non-partner sexual violence that was not included. For example, culturally specific stigma around sex is an important factor that shapes risk and adverse outcomes related to sexual violence but studies on such topics may have been missed if not explicitly linked to non-partner sexual violence. Lastly, the review excluded non-English articles and may have missed valuable scholarship from other countries of origin of AA and PI communities.
This study sought to systematically review the extant literature on non-partner sexual violence among AANHPIs with the goal of providing a road map for future actionable research priorities. Sexual violence is a significant and persistent public health issue and AANHPIs are a rapidly growing racial/ethnic minority group in the United States. Taken together, it is critical that additional rigorous research is conducted among this underserved population with specific attention to the unique historical, cultural, and linguistic characteristics that the diverse AANHPI subgroups hold.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health–National Institute on Minority Health and Health Disparities [grant number U54MD000538] and National Heart, Lung, and Blood Institute [grant number R01HL160324].
OVID Medline Search Strategy—Run December 3,2019
1
Domestic Violence/or Gender-Based Violence/or Intimate Partner Violence/or Spouse Abuse/or Rape/or Child Abuse, Sexual/
2
((Molestat* or violen* or abuse*) adj2 sex*).ti,ab
3
(commerc* adj3 exploit* adj3 (girl* or child* or wom#n)).ti,ab
4
Enslavement/or Human Trafficking/
5
((human or sex*) adj2 (slav* or traffick*)).ti,ab
6
((Force* or trade or trading or traded or coerc*) adj3 sex*).ti,ab
7
(genital mutilation or genital cutting or female circumcision or clitoridectom* or Infibulation).ti,ab
8
Circumcision, Female/
9
Sexual Harassment/or Sexual Harassment.ti,ab
10
(Infanticide/or Infanticide.ti,ab.) and ((girl* or female).mp. or female/) [mp=title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier, synonyms]
11
(((early or arrang* or forced or child*) adj2 marriage*) or (child* adj2 bride*)).ti,ab
12
1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11
13
oceanic ancestry group/or pacific islander/or torres strait islander/
14
(Pacific Islander* or Hawaiian*).ti,ab
15
exp Pacific islands/
16
(Melanesia or Melanesian or Melanesians or Fiji or Fijian or Fijians or New Caledonia or New Caledonian or New Caledonians or Papua New Guinea or Papuan or Papuans or Vanuatu or Vanuatuan or Vanuatuans or Micronesia or Micronesian or Micronesians or Guam or Palau or Palauan or Palauans or Polynesia or Polynesian or Polynesians or Pitcairn Island or Samoa or Samoan or Samoans or Tonga or Tongan or Tongans).ti,ab
17
(Asian American or Asian Americans or Taiwanese American or Taiwanese Americans or Chinese American or Chinese Americans or Indian American or Indian Americans or Filipino or Filipinos or Vietnamese American or Vietnamese Americans or Japanese American or Japanese Americans).ti,ab
18
Asian American/or Asian continental ancestry group/
19
13 or 14 or 15 or 16 or 17 or 18
20
12 and 19