
Abstract
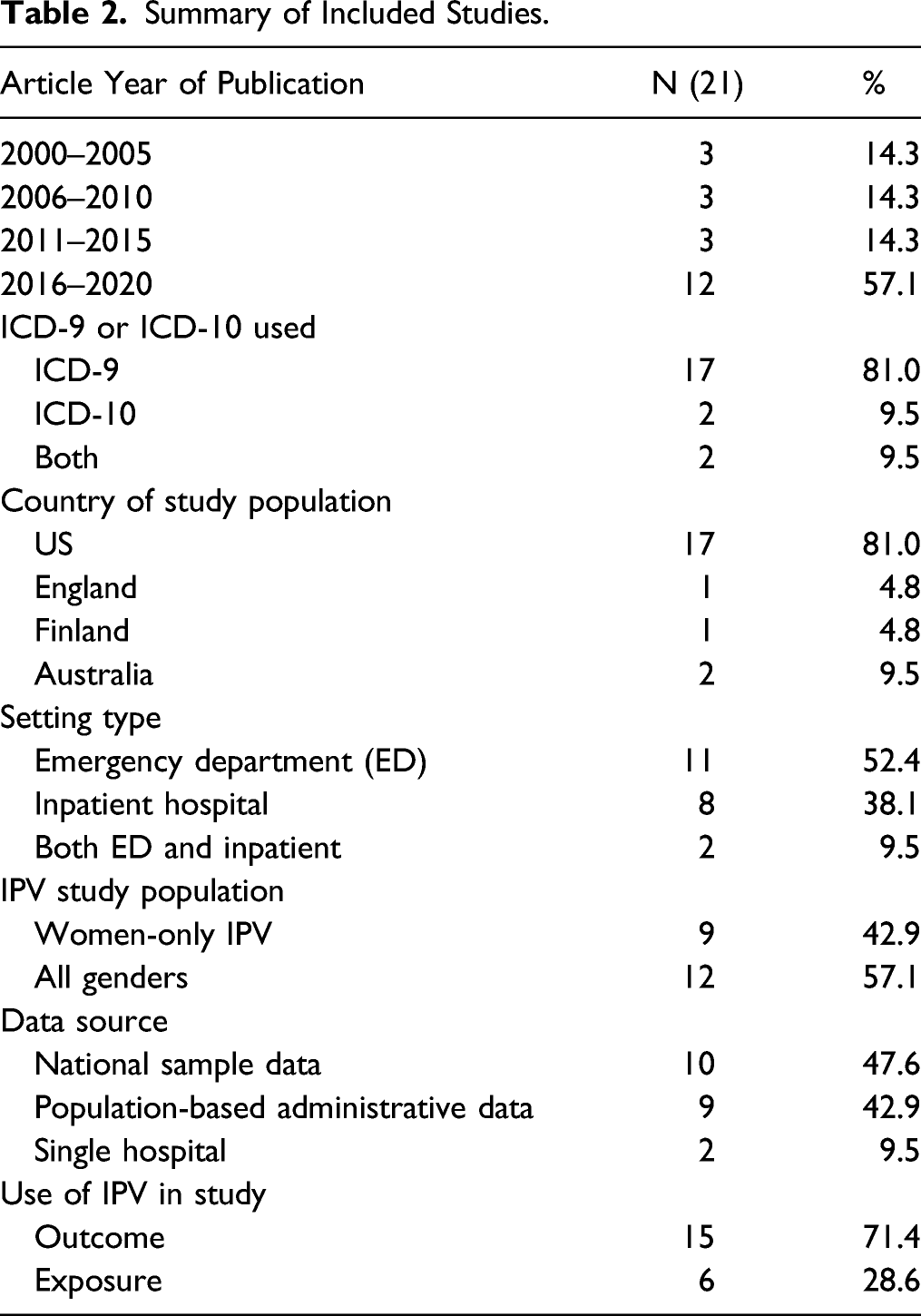
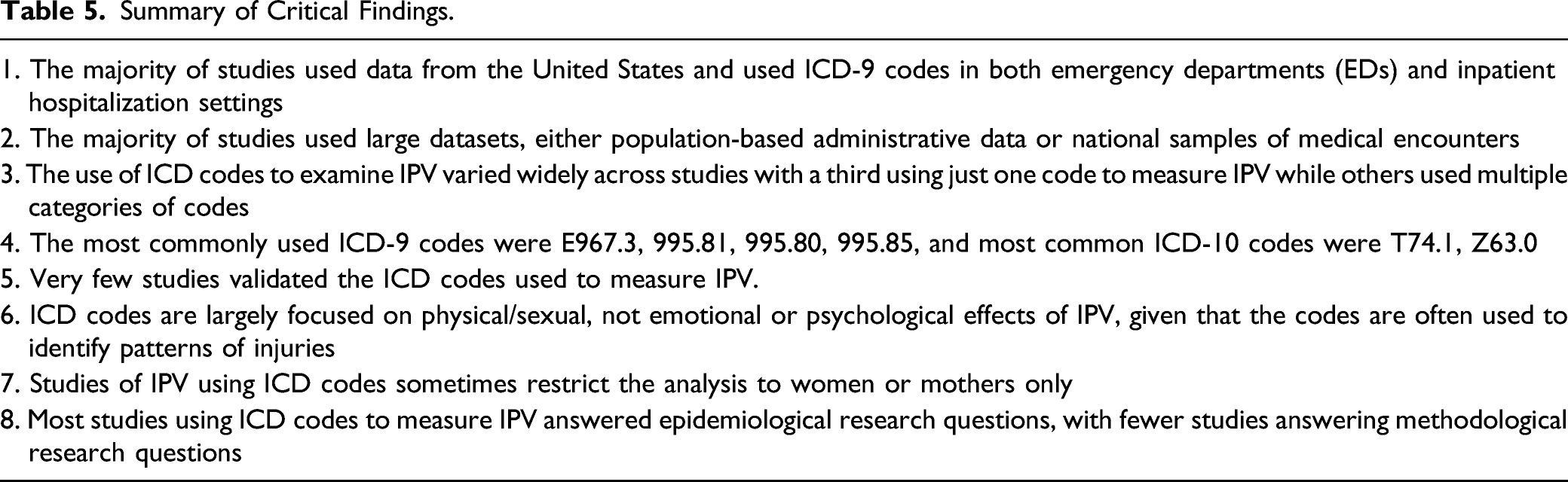
Intimate partner violence (IPV) is challenging to measure yet systematic surveillance of IPV is critical to informing public health prevention and response efforts. Administrative medical data provide opportunities for such surveillance, and often use the International Classification of Diseases (ICD). The primary purpose of this systematic review was to document which ICD codes have been used in empirical literature to identify IPV, understand the justification used to select specific codes to develop IPV case definitions, and identify the data sources and types of research questions addressed by the existing literature. We searched 11 databases and of the initial 2182 results, 21 empirical studies from 2000 to 2020 met the study inclusion criteria including using ICD codes to measure IPV. The majority of these studies (90.5%) used either national samples of data or population-based administrative data from emergency departments (52.4%) or inpatient hospitalizations (38.1%). We found wide variation of ICD diagnostic codes to measure IPV and categorized the sets of codes used based on the number of codes. The most commonly used ICD-9 codes were E967.3, 995.81, 995.80, 995.85 and the most common ICD-10 codes were T74.1 and Z63.0. Few studies validated the ICD codes used to measure IPV. Most included studies (81.0%) answered epidemiological research questions. The current study provides suggestions for future research, including justifying the selection of ICD codes and providing a range of estimates based on narrow and broad sets of codes. Implications for policy and practice, including enhanced training for healthcare professionals in documenting IPV, are discussed.
Keywords
Intimate partner violence (IPV) is a serious and preventable public health problem. The Centers for Disease Control and Prevention (CDC) defines IPV as any physical violence, sexual violence, stalking, or psychological harm by a current or former partner or spouse (Breiding et al., 2015). Globally, an estimated one in three women aged 15 years and older report experiencing physical and/or sexual intimate partner violence at least once in their lifetime (Devries et al., 2013; World Health Organization, 2021a). Experiencing IPV is associated with a range of negative short- and long-term health consequences, including physical conditions that impact cardiovascular, gastrointestinal, reproductive, musculoskeletal systems as well as mental health problems such as posttraumatic stress disorder (Black, 2011). IPV also results in significant costs to society, with one recent study in the United States suggesting a lifetime economic burden of $3.6 trillion for IPV (Peterson et al., 2018).
Systematic, ongoing public health surveillance of IPV is critical to informing public health prevention and response efforts. Accurate surveillance methods are needed for understanding burden, monitoring trends over time, identifying high-risk populations who might benefit from intervention and services, and allocating appropriate resources for public health issues like IPV (Breiding et al., 2015). Several complementary data sources including self-report surveys and administrative medical data may be used to document and monitor IPV, each of which provides unique information about the scope and nuance of this public health concern.
In both international and domestic settings, IPV is often assessed through population-based surveys that use self-report measures of IPV (World Health Organization, 2021a). Surveys to gather data on IPV include specialized surveys on interpersonal violence (e.g., National Intimate Partner and Sexual Violence Survey; Smith et al., 2017), modules on violence against women within larger national health surveys (e.g., the Demographic and Health Surveys; ICF, n.d.), and crime victimization surveys (e.g., National Crime Victimization Survey; Morgan & Truman, 2021). These data collection systems provide vital information about the population-level burden of IPV and offer researchers the flexibility to collect detailed contextual information on the nature of the IPV experience, as well as its causes and consequences. However, data from self-report surveys are subject to a number of limitations that may limit the generalizability of the information obtained. Individuals experiencing IPV at the time of the survey may be less likely to consent to completing surveys related to IPV (Kresnow et al., 2022; Waltermaurer et al., 2003). Given social expectations and stigma associated with IPV, individuals may also be reluctant to disclose experiences of IPV, particularly among males (Bates et al., 2019). Further, self-reported surveys are often costly to implement and the data may be delayed before it is made widely available to researchers.
Administrative medical data provide one alternate data source for ongoing public health surveillance of IPV. In addition to self-reported surveys, surveillance of IPV can occur through systematic, ongoing collection and analysis of existing records in emergency departments (EDs) and hospitals. Survey data are typically more detailed than data collected in administrative medical records because surveys are often intentionally developed to assess a range of victimization experiences. Survey data are able to capture a broader range of IPV experiences than medical records because medical records largely capture IPV experiences that are severe enough to warrant medical attention. However, administrative medical data are not subject to the same types of self-report biases as survey data because this data source allows for a secondary review of existing data, collected in the process of administering services for a full population of individuals who received medical services, and does not require consent from patients.
While healthcare data are often collected for other purposes (e.g., billing and reimbursement) and thus may lack particular details, another major benefit of using healthcare data is that these data can be relatively inexpensive to leverage for surveillance purposes (Centers for Disease Control and Prevention, 2018). As electronic health systems are improved to accelerate data quality and availability, administrative medical data may also provide a cost efficient and timely alternative for monitoring and responding to IPV. In addition, these data can be linked to other health system or administrative data to provide a more comprehensive picture of certain health issues or diagnoses (e.g., Rebbe et al., 2021). Finally, hospitals can serve as an important potential point of intervention for increasing safety and lessening the negative consequences experienced by IPV survivors (Niolon et al., 2017). Healthcare data can provide useful information for identifying populations in need of IPV services, developing targeted prevention efforts, and for evaluating the impact of these efforts in healthcare settings.
Administrative medical data often use standard classification systems like the International Classification of Diseases (ICD) for injury and disease. The ICD, Clinical Modification is used globally to code and classify diagnoses and procedures associated with healthcare utilization (e.g., visits at inpatient, outpatient, and physician offices) (World Health Organization, 2021b). For IPV, there is currently no consensus about which set of codes from the Ninth (ICD-9) or Tenth (ICD-10) Revisions are most appropriate for identifying patients experiencing IPV. Although there have been attempts to capture more detail around IPV especially in the ICD-10, there is significant variability in which codes researchers have used to identify IPV in prior research (Rovi & Johnson, 1999; Waller et al., 2000). Some of the variability may be due to the transition from and differences between the use of ICD-9 and ICD-10 within and across countries (Topaz et al., 2013). The terminology of the existing codes and specificity (or lack thereof) of the perpetrator have created inconsistency and ambiguity in identifying IPV, where some researchers have used a single code to identify IPV (Sprecher et al., 2004) whereas other researchers have used external cause of injury codes to more specifically identify the perpetrator’s relationship to the assault victim (Weiss et al., 2004). As a result, administrative medical data related to IPV are incomplete and underestimate the true prevalence.
Although an underestimate of the true prevalence of IPV, consistent, complete, and accurate coding of IPV in administrative medical data has the potential to improve patient care and increase understanding of the burden and impact of IPV on individuals and communities. The current study aims to (1) systematically document which specific ICD codes have been used to identify IPV in the empirical literature, (2) examine which datasets have been used to examine IPV with ICD codes, (3) examine the justification for specific ICD codes used in studies, and (4) identify what types of research questions have been answered in the existing literature. This systematic review highlights the range of codes and definitions researchers have used to identify IPV and provides recommendations to guide future research on IPV using ICD codes.
Methods
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines suggested by Moher et al. (2009). We also submitted registration of the study to Prospero, but this has been postponed because COVID studies are taking priority for review registration at this time. The systematic searching methods are driven by the aims of the research study articulated above.
Eligibility Criteria
The inclusion criteria for this study were empirical research studies, domestic or international, published in English in the last 20 years (2000–2020). Studies must have been published in peer-reviewed journal articles. Gray literature, books, conference proceedings, and dissertations were excluded. Articles must have used ICD-9 or ICD-10 codes to measure IPV (we searched ICD both with and without version number to determine inclusion). The articles must have included IPV only (not bound by gender or marriage status); studies could have included any age groups, and could be quantitative, qualitative, mixed methods, or any other methodological design. Design of studies was not a specific eligibility criterion, but more importantly, was the examination of IPV and ICD usage. Studies which did not examine or measure IPV using ICD codes were excluded.
Search Strategy
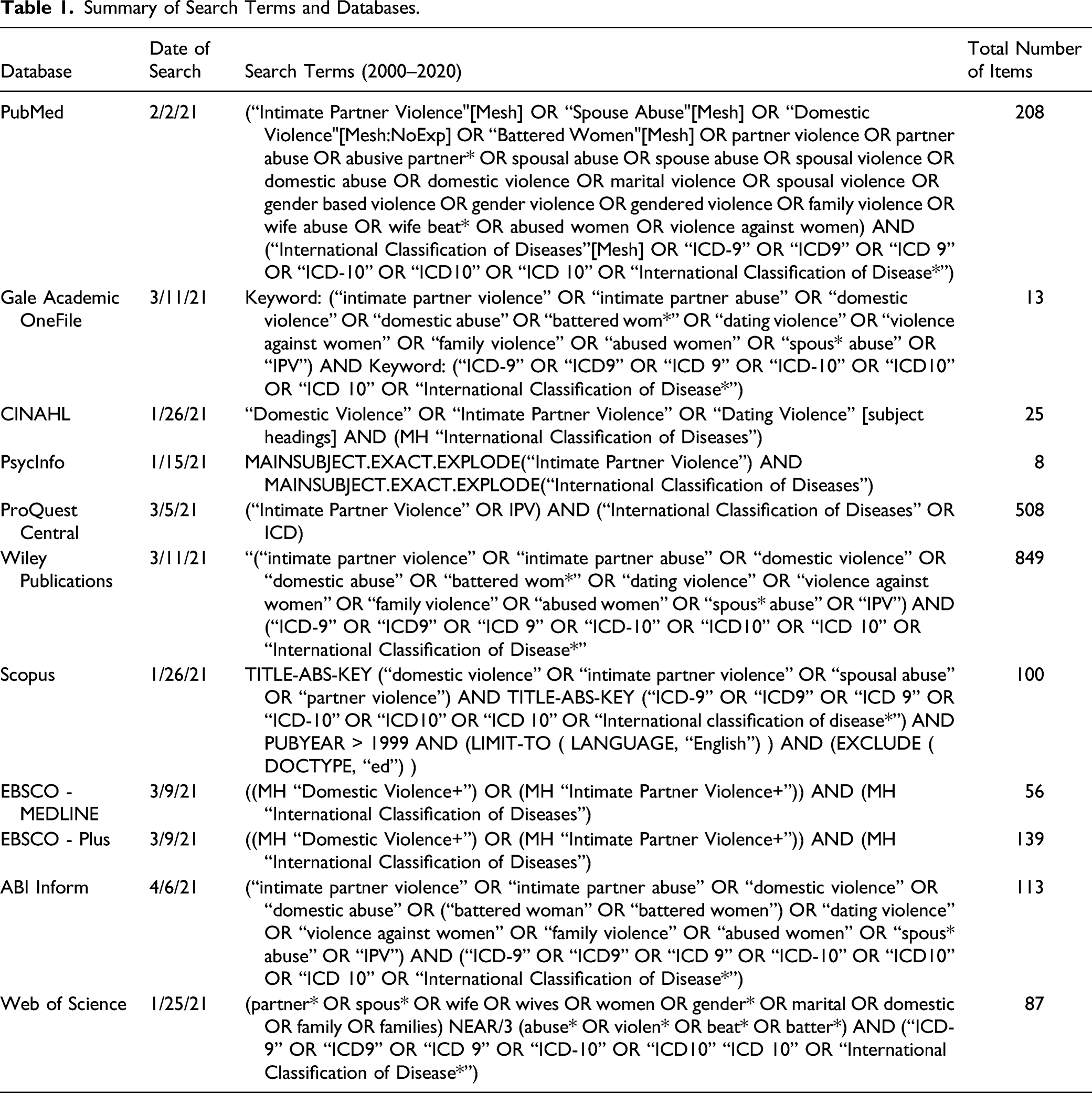
Eleven databases were systematically searched using MeSH, PICO terms, database thesauri, and keyword searching. Relevant limiters and filters were used when available to reduce results that did not meet inclusion criteria. All research team members participated in strategic searching. Systematic searching started on January 21, 2021 and was completed on April 6, 2021. Following consultation with a research librarian and co-author, we searched the following 11 electronic databases: PubMed, ABI Inform, Web of Science, Gale Academic OneFile, CINAHL PsycInfo, ProQuest Central, Wiley Publications, Scopus, EBSCO MEDLINE, EBSCO PLUS, and ABI Inform. We additionally used Google Scholar to conduct backward and forward citation checking of the articles that made it to full text data extraction phase. Backward and forward citation checking is the process of using the links from an article in Google Scholar to discover all articles that have cited the article (forward searching, published after the article) and all articles on the reference list of the article (backwards searching). This process allows for related articles (that may not have been identified during systematic searching) to be added and evaluated during the screening process. Forward searching also provides a final check during the writing process to find any newly published articles that cited articles that were not included in the data extraction step of the systematic review.
Summary of Search Terms and Databases.
Data Screening
The 2182 selected studies were transferred to Covidence for abstract and full-text screening. Covidence identified 659 duplicate articles. Covidence is the Information Science discipline’s industry standard software used for systematic reviews. It automates de-duplication, screening (abstract and full-text), data extraction, and quality assurance steps following the PRIMSA protocol. It allows researchers to work in teams to move through these steps while tracking the entire process and creating a PRISMA chart of the systematic review, which documents the reason any article that was retrieved in systematic searching was removed during screening (by inclusion and exclusion variables). It also standardizes data extraction and quality assurance steps based on PRISMA protocols.
Abstract screening was performed by all research team members, and each of the remaining 1523 abstracts were screened by two independent reviewers. Based on the abstracts, studies that did not meet the inclusion criteria were excluded, and if the two screeners did not agree, the abstract went to a third researcher to screen for a final decision. During the abstract screening process, 1360 studies were eliminated for not meeting the inclusion criteria. Next, 163 articles underwent full-text screening by two independent reviewers. Any disagreements were discussed by the research team, and 142 studies were omitted for not meeting the inclusion criteria. The most common reasons for exclusion were that the article did not examine IPV, did not use ICD codes to measure IPV, or the article was not empirical. In concluding the full-text screening process, 21 studies met our inclusion criteria and were moved to data extraction and quality assurance assessment. See Figure 1 for a PRISMA diagram of the search and screening process. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Flow Diagram of Search Strategy.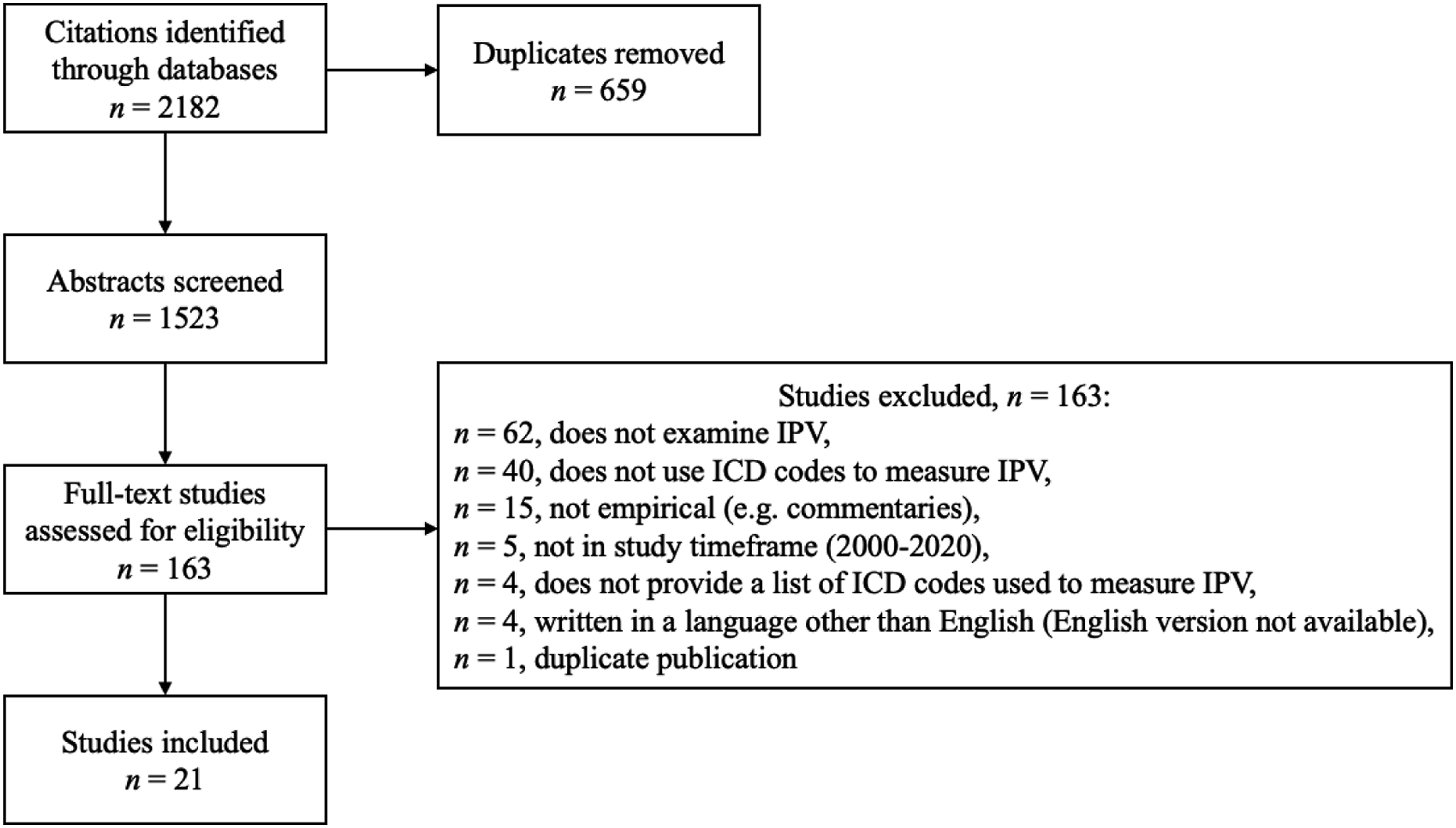
Data Extraction
The research team developed a data extraction form to collect information related to the ICD codes used (including justification and validation of codes), setting, country, data source, study years, study population, study research question, outcome variables, how IPV was used in the study, key results, and how diversity was addressed. Two members of the team used the form to extract data from the 21 studies. The research team held weekly discussions to discuss data extraction, serving to identify any issues or patterns and resolve points of uncertainty.
Results
Summary of Included Studies.
International Classification of Diseases Codes Used to Identify Intimate Partner Violence
ICD Codes Used by Study in Descending Order.
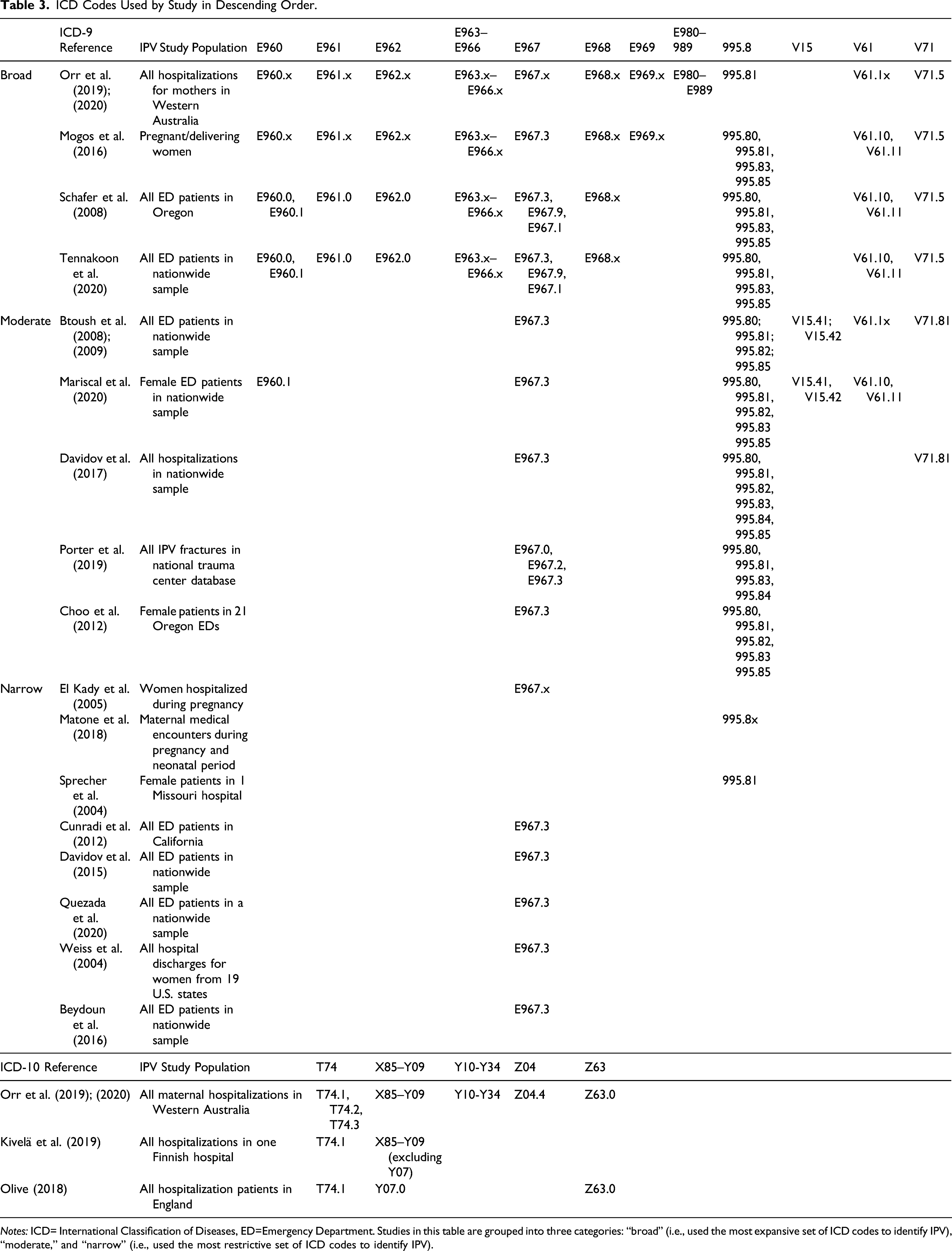
Notes: ICD= International Classification of Diseases, ED=Emergency Department. Studies in this table are grouped into three categories: “broad” (i.e., used the most expansive set of ICD codes to identify IPV), “moderate,” and “narrow” (i.e., used the most restrictive set of ICD codes to identify IPV).
Four studies used ICD-10 codes. Each included T74.1 (“Physical abuse, confirmed”), while two studies also included T74.2 (“Sexual abuse, confirmed”) and T74.3 (“Psychological abuse, confirmed”). Three of the studies included Z63.0 (“Problems in relationship with spouse or partner”) and a different three included all codes for assault (X85-Y09, although Kivelä et al. did not include Y07 because the Finnish version of ICD-10 does not include perpetrator designations for this code).
Broad versus Narrow Sets of Codes to Identify Intimate Partner Violence
The range of ICD-9 codes used to document IPV was apparent. Based on the number of ICD codes used to identify IPV, we grouped the studies into three categories: “broad” (i.e., used the most expansive set of ICD codes to identify IPV), “moderate,” and “narrow” (i.e., used the most restrictive set of ICD codes to identify IPV). We did not categorize the ICD-10 codes because of the limited literature (n = 4 studies), but the Orr et al. publications (2019, 2020) had the most expansive lists while Olive (2018) was the narrowest. Among studies using ICD-9 codes, some narrowly defined IPV with a single code, while others used a broader definition that included any cases where IPV may have been likely. Eight studies opted for a “narrow” definition of IPV. This was either done to minimize false positives or because there is disagreement about which ICD codes identify IPV, given the range of definitions and uses in the literature. These eight studies examined cases where the perpetrator was identified in the ICD codes as an intimate partner and excluded assault/violence perpetrated by others. Davidov et al. (2015) utilized a narrow definition of IPV using the ICD codes (including only ICD-9 code E967.3). However, in a subsequent paper, Davidov et al. (2017) noted that although E967.3 specifies perpetrator abuse, it is used infrequently and opted for an expanded definition.
Five papers, including Davidov et al. (2017), used a “moderate” definition of IPV and argued the use of limited ICD codes leads to an underestimation in the true prevalence of IPV. For example, Mariscal et al. (2020) studied IPV among female ED patients, but “included causes directly related to IPV and incidents in which women were abused or assaulted by another adult.” Mariscal et al. (2020) cited Btoush et al. (2008) to provide evidence that the expanded list of ICD-9 codes could capture various forms of IPV that present at an ED. They also cited research by Smith et al. (2017) to support this definition, who found women were more likely to be raped and abused by an intimate partner. Of the five papers that used a moderate definition of IPV, two restricted the sample to women patients.
Five studies opted for a “broad” definition of IPV using the most expansive sets of ICD codes. Schafer et al. (2008) estimated the sensitivity of diagnosis codes for female victims treated in EDs or hospitalized for IPV-related injuries by reviewing medical records to confirm visits resulted from intentional physical or sexual assault by an intimate partner in Oregon. They documented high predictive value positive (PVP) for a broad definition of ICD-9 codes that are not directly indicative of IPV, but were used in cases where IPV was present. Specifically, three primary ICD-9 codes (E967.3, 995.81, 995.8) detected 23% of all female IPV victims with a PVP of 95% (e.g., 95% of cases identified as IPV were verified as IPV after reviewing medical records). The addition of 12 provisional codes doubled sensitivity (i.e., 44% of female victims of IPV were identified) but adding provisional codes reduced PVP from 95% to 50%. Tennakoon et al. (2020) cited Schafer and colleagues when describing the definition and selection of IPV-related ICD codes. Orr et al. (2019) examined IPV among mothers and included a broad range of codes for interpersonal violence and assault, even if it was not known if the perpetrator was an intimate partner. Orr et al. (2020) used the same codes but defined the variable as “family and domestic violence,” which includes IPV. Family and domestic violence may be an accurate name for the broadest set of codes to define IPV, especially when the analysis is restricted to mothers.
No U.S. studies have leveraged ICD-10 codes to evaluate IPV given the relative recency of implementation in the U.S. (October 2015), but studies outside of the U.S. have used ICD-10 codes to measure IPV. Olive (2018) used a narrow definition and Orr et al. (2019) and Orr et al. (2020) used the most expansive list of ICD codes to measure IPV. Olive found 86% of IPV admissions were from code Z63.0, a code that was used by Orr et al. (2019) and Orr et al. (2020) but not used by Kivelä et al. (2019). Kivelä et al. (2019) is unique because the authors used the Finnish clinical modification of the ICD-10, which uses different code sections from the U.S. version to designate the perpetrator’s relationship in an assault. Orr et al. (2019) cited Olive (2018) to highlight the importance of using Z code relating to partner conflict that affects health status and also included codes for assaults and conflicts (Y10 to Y34).
Justifications for International Classification of Diseases Codes Used
Several studies did not describe why the ICD codes used in their study were selected to identify IPV (n = 11). Several of these studies used the single, most common ICD codes (i.e., E967.3 or 995.81) to measure IPV without describing why other codes were not used (n = 6). In contrast, 10 studies provided some justification about the selection of ICD codes:
ICD-9
Btoush et al. (2008) included codes recommended by other researchers and excluded codes such as rape and assault unless the documentation specified the violence was caused by partner/spouse. The authors excluded assaults where someone other than an intimate partner might have caused them. In contrast, Mariscal et al. (2020) included the codes for adult abuse and rape, citing that these forms of violence were more likely to be perpetrated against women by intimate partners. Davidov et al. (2017) justified using codes beyond those specifying the perpetrator because previous research identified that such codes are infrequently used. The authors stated that they wanted to maximize the sensitivity of identifying IPV in their study.
ICD-10
Olive (2018) used the labels of the codes in the ICD-10 to describe the reason for inclusion or exclusion in the study. Olive (2018) stated that the three ICD-10 codes used (T74.1 maltreatment (physical abuse) by spouse, Y07.0 other maltreatment by partner, and Z63.0 problems in relationship with partner) used most closely align with the World Health Organization (WHO) definition of IPV. The author excluded assault codes X85-Y09 because, with the exception of two codes, there are no victim-perpetrator relationship options for these assault classifications. The author included Z63.0 because it is labeled as “problems in relationship with spouse or partner,” which may capture multiple forms of conflict and victimization related to IPV.
Building upon Olive (2018), Orr et al. (2019) noted that they were broader in the selection of ICD codes. They categorized IPV variables into three topics: assault, partner conflict impacting health status, and all IPV. Orr et al. (2019) included all codes for “assault and conflict” and additional codes for external cause of injury and poisoning, including undetermined intent (ICD-10-AM: Y10 to Y34) for their population of hospitalized mothers. Kivelä et al. (2019) excluded Y07 because the Finnish version, which they used, did not designate a perpetrator in contrast to the U.S. version. Further, Kivelä et al. (2019) stated that they included the assault codes and physical abuse codes so as not to limit to the most “obvious and serious” IPV cases (p. 613).
Research Questions
Description of Reviewed Studies.
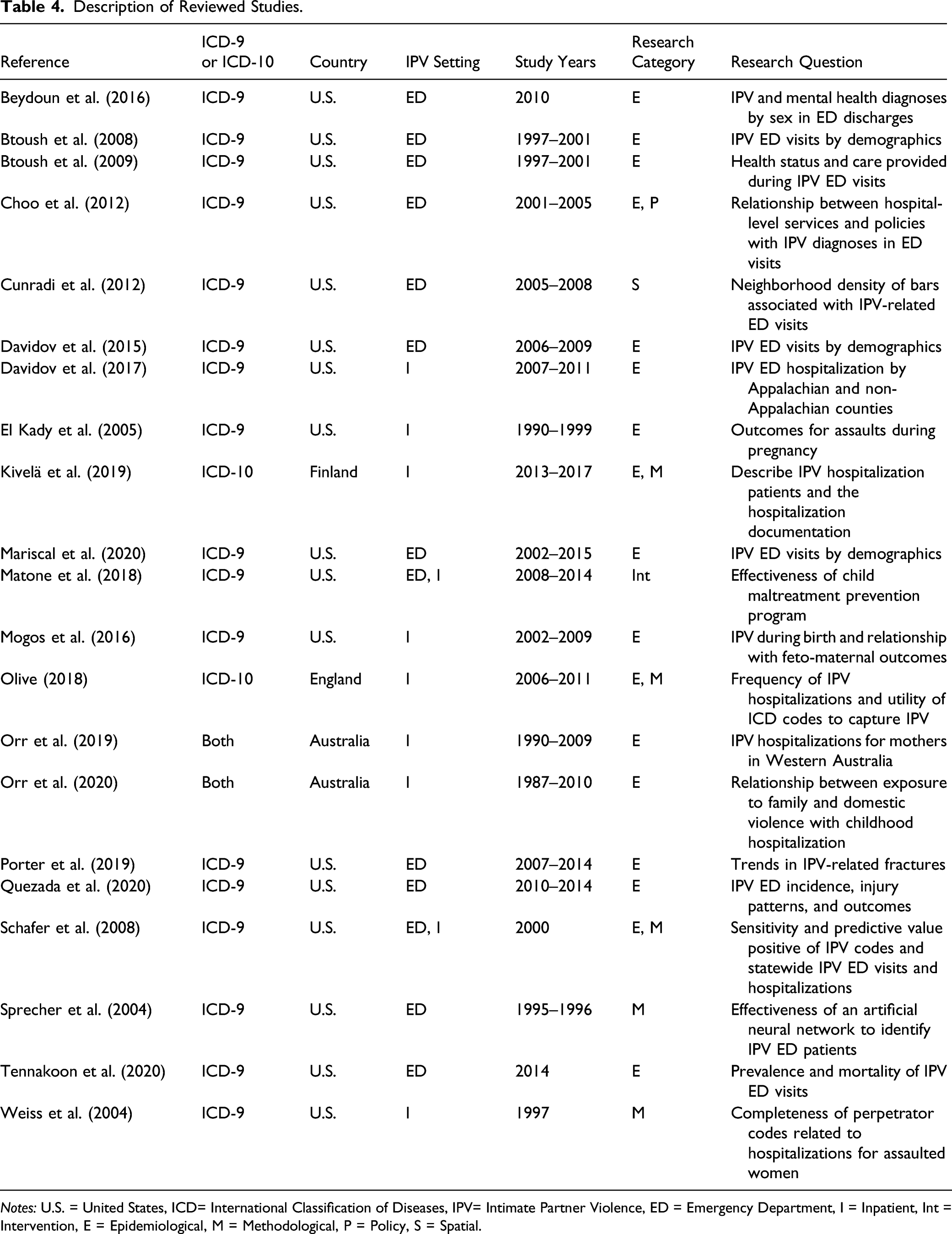
Notes: U.S. = United States, ICD= International Classification of Diseases, IPV= Intimate Partner Violence, ED = Emergency Department, I = Inpatient, Int = Intervention, E = Epidemiological, M = Methodological, P = Policy, S = Spatial.
Summary of Critical Findings.
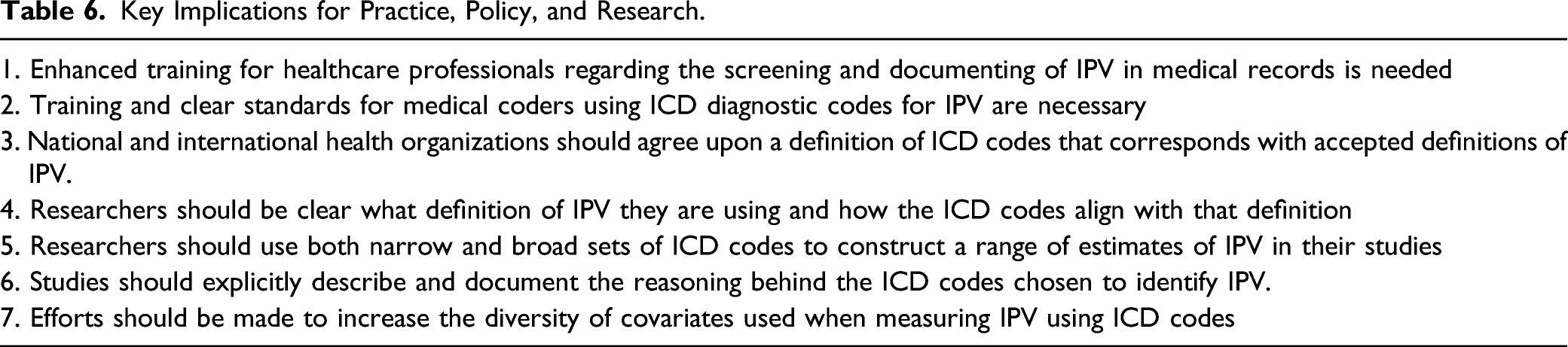
Key Implications for Practice, Policy, and Research.
Four studies included methodological questions as part of the study purpose. Weiss et al. (2004) assessed the completeness of perpetrator codes for women who had diagnoses of assault finding that only 8.8% included perpetrator codes, but that the majority of those codes were related to a spouse/partner (83.7%). Sprecher et al. (2004) tested the effectiveness of an artificial neural network to identify IPV patients in EDs. The tested model had 78% sensitivity and 89% specificity. Schafer et al. (2008) estimated the sensitivity and predictive value positive of three primary ICD codes related to IPV, estimating a predictive value positive of 94%, which reduced to 50% with the inclusion of 12 provisional IPV codes but increased sensitivity (51%). Olive (2018) used a mixed methods study to examine the utility of ICD-10 codes and found that 86% of IPV admissions used code Z63.0 (“Problems in relationship with spouse or partner”) while also identifying a disconnect between the language used by practitioners and those used by the ICD-10, raising concerns about its utility.
Discussion
This systematic review synthesized 21 empirical research papers that have used ICD diagnostic codes to measure IPV. Studies spanned various populations including all U.S. states (e.g., Btoush et al., 2008; Porter et al., 2019; Tennakoon et al., 2020), single U.S. states (e.g., Oregon-Schafer et al., 2008), European countries (Kivelä et al., 2019; Olive, 2018), and Western Australia (Orr et al., 2019). The results of this systematic review yield three key findings and related recommendations for policy, practice, and research. First, the results indicate that ICD codes are one tool to measure IPV in large population-based datasets, information that is difficult to determine and can inform policy and practice. Second, this study documents the lack of consensus about which codes best measure IPV. Third, the results of the present study underscore the benefits of providing broad, moderate, and narrow sets of ICD codes to measure IPV to understand the potential range of estimates.
Although an underestimate of the true burden of IPV, leveraging ICD codes to measure IPV can improve decision making related to affected individuals and families. Research using administrative medical and healthcare data has increased over time, likely as access to datasets has increased and computing power has enabled and facilitated easier analysis of this data (Jonson-Reid & Drake, 2008). These studies, such as the ones identified in this review, have the potential to increase and improve public health surveillance of IPV resulting in injuries that require medical attention. The current study shows the use of ICD codes to measure IPV has increased over time with more than half of the 21 studies published since 2016. The majority of studies identified used large datasets, either population-based administrative data or national samples of medical encounters.
Our results highlight that substantially different definitions for IPV exist in the literature, which may result in divergent prevalence estimates. Given the difficulty in measuring IPV, especially at the population level, the use of ICD codes can provide important information that may be used for the allocation of resources, but only if those estimates are consistent across studies, jurisdictions, and over time. Importantly, this review highlights that many studies did not describe why the ICD codes used in their study were selected to identify IPV, even in cases where the ICD codes did not identify the relationship between the victim and perpetrator as IPV. Some researchers justified the use of ICD codes based upon the population inclusion criteria. For example, Orr et al. (2019) and Orr et al. (2020) used the broadest set of ICD codes, but their population of interest was limited to mothers. Given that the mother was the victim of violence, as identified by ICD codes, they included all violence and labeled it as IPV or family and domestic violence.
One way to address the inconsistent measurement of IPV using ICD codes is to examine estimates using broad, moderate, and narrow sets of ICD codes for populations overall and when restricted to key subpopulations. More than one set of codes can be used to estimate IPV and codes may differ for women, mothers, or other populations. Schafer et al. (2008) highlighted the problems with narrow and broad definitions and stated “A short list of three ICD-9-CM case finding codes identifies nearly one-quarter of all victims seen in EDs and hospitals, minimizing false positives such that confirmatory medical record review is unnecessary...An expanded list of codes increases sensitivity at the expense of false positives” (p. 635). Using narrow and broad definitions may create balance by providing a range of potential estimates and address the tradeoffs. Further, if study findings hold for narrow and broad definitions of IPV, this can underscore the robustness of the research.
Implications for Research
Despite the potential benefits that administrative medical data holds for population-based surveillance of IPV, a key limitation is the lack of consensus on which ICD diagnostic codes are most appropriate for identifying IPV. We found wide variation in which codes were chosen to measure IPV, likely a result of the concerns about variability in the practice of recording codes. The variation of codes used in prior literature and the lack of consensus on which codes should be used indicates that future researchers using ICD codes to measure IPV should use both a broad and a narrow set of codes when examining epidemiological research questions. This approach is similar to that of Schafer et al. (2008) who used three “primary” codes (E967.3, 995.81, and 995.80) and an additional 12 “expanded” codes to identify medical encounters related to IPV in Oregon. This approach documents and estimate with high specificity paired with another estimate with enhanced sensitivity. A potential model of how to address this issue was done by Parks et al. (2012) regarding abusive head trauma (AHT). This publication by the Centers for Disease Control and Prevention summarizes the development and recommendation of a definition of AHT that includes both a narrow and broad definition for both ICD-9 and ICD-10 codes, which have been found to have high sensitivity and specificity (Berger et al., 2015) and applied in a variety of studies of AHT (Peterson et al., 2014; Rebbe et al., 2020; Zolotor et al., 2015). Additional research validating the diagnostic codes used for IPV (e.g., using chart reviews or interviews) would be useful to understanding what administrative medical data may be missing.
The included studies also highlighted the lag between changes in practice and published empirical studies. Although ICD-10 was implemented in the U.S. in October of 2015, none of the included studies from the U.S. used ICD-10 codes, even though we included studies published through 2020. The present study documented an increase in the number of studies that used ICD-9 codes over time, and it is expected that there will be an increase in the number of studies using ICD-10 codes over time. The transition from ICD-9 to ICD-10 codes will change the way IPV is documented and examined. The effect of this change must be assessed and acknowledged in research that explores changes over time across the transition from one coding system to the next.
Limitations of International Classification of Diseases Diagnostic Codes
ICD diagnostic codes are important because they can provide population-level documentation and contribute to public health surveillance of IPV; however, they have important limitations (Syed et al., 2021). Although some codes (i.e., E-codes) identify the relationship between the victim and perpetrator, they are underused and minimize the usefulness of medical data for understanding IPV (Waller et al., 2000; Weiss et al., 2004). In addition, diagnostic codes do not provide important information about the history of the relationship with the perpetrator, length of relationship with the perpetrator, particular forms of abuse (emotional, financial), or chronicity of the abuse. This suggests that administrative medical and healthcare data is not sufficient to understand IPV holistically. ICD codes are largely focused on physical/sexual violence, not emotional or psychological effects of IPV, given that the codes are often used to identify patterns of injuries. Data using ICD codes to measure IPV should clarify the types of IPV that can be examined. Future research should also consider whether ICD codes may be used in conjunction with other common elements in administrative data (e.g., chief complaints fields or triage notes) to better capture IPV.
Problems with Definitions of Violence (Interpersonal vs. Intimate Partner vs. Family Violence)
We found that IPV was often conflated with interpersonal violence. Authors reported including ICD codes where the perpetrator of the assault was unknown, and therefore cannot be determined to be IPV, but were included to enhance specificity (Davidov et al., 2017; Mariscal et al., 2020; Orr et al., 2019). We also identified instances where IPV was defined on a set of ICD codes used in prior research that purported to examine interpersonal violence. Moving forward, researchers should aim to be explicit about the definition of IPV or interpersonal violence they are using, how the ICD codes chosen to identify IPV align with that definition, and the assumptions or potential biases that the selected set of codes may introduce to subsequent analyses.
Inclusion of Diversity
Given the majority of studies (90.5%) used either a national sample of medical encounters or population-based administrative data, included studies reduced selection bias by using a census of records or a very large sample. However, these studies were also limited in regards to the covariates they could include for analysis because they relied on administrative data. Covariates typically included patient age, sex, race/ethnicity, and health insurance type. Other important sociodemographic information (e.g., socioeconomic status, gender identity, and sexual orientation) was largely missing from these studies in addition to information regarding the perpetrator, the length of the intimate relationships, the duration and severity of the IPV. Future efforts improving the quality and availability of such information in administrative datasets would enhance our understanding of IPV and the underlying factors driving inequities in risk for violence.
Implications for Practice and Policy
Many of the studies included in this systematic review expressed concerns regarding the variability of coding practices of IPV in medical records (El Kady et al., 2005; Mariscal et al., 2020; Mogos et al., 2016). There are myriad reasons why IPV may not be well-documented in medical records, including time constraints, lack of reimbursement incentive, and perceived lack of knowledge or power to change the problem. IPV can be a sensitive topic to discuss, and clinicians must feel comfortable and able to discuss the topic with care. Clinicians may lack the training to know if and how to safely elicit this information and be able to refer patients to appropriate resources (Paterno & Draughon, 2016). Clinicians may also have a misconception of patients’ risk of exposure to IPV, perceiving some individuals to have higher risk based on their demographic characteristics or stereotypes (e.g., may be less likely to ask about IPV for individuals in same-sex relationships). In addition, individuals experiencing IPV may feel guilt, shame, and/or discomfort that might make them reluctant to disclose to their clinician (Heron & Eisma, 2021). They may also fear repercussions or retaliation from abusive partners if they have access to the medical record (Randell et al., 2021). The promise of public health surveillance of IPV through medical records will continue to be hampered without addressing these barriers.
The United States Preventive Services Taskforce (USPSTF) recommends that clinicians screen for IPV in women of reproductive age and provide/refer those who screen positive to support services (Curry et al., 2018). While enhanced education for healthcare professionals is one important component of ensuring appropriate screening, there have been calls to also make use of electronic health records to prompt care and facilitate data collection along with cross-sector partnerships to connect patients to appropriate support services (Miller et al., 2015). These systems-level improvements may be useful for increasing screening and documentation of IPV in medical records. Clear standards and guidelines for which ICD diagnostic codes should be used are necessary and will ultimately allow for higher quality surveillance and understanding of the public health burden of IPV.
Strengths and Limitations
This review adds to the current knowledge of IPV by providing detailed information on empirical studies that used ICD codes to measure IPV. The inclusion of both ICD-9 and ICD-10 codes and our examination of studies from across the globe provide a broader understanding of the scope and methods of using administrative healthcare data to study IPV. The geographic variation of the studies increases the understanding of how ICD codes can and have been used to measure IPV. Our findings should be considered in light of several limitations. We included only peer-reviewed, empirical journal articles published in English so may have excluded important research published in other languages and reviews or commentaries addressing the use of ICD codes to identify IPV. Restricting to articles published in English only may have limited the generalizability of these findings and may explain the lack of information in non-Western countries in particular. There were also no studies that used ICD-10 codes in the U.S., despite ICD-10 having been in place for over 5 years. Even outside the U.S., there were a limited number of studies we identified based on our inclusion criteria. Although we searched several databases with broad search terms, our searches may have failed to identify all relevant studies. While we focus our review on ICD codes, future work examining how alternative classification systems (for example, Systematized Nomenclature of Medicine or SNOMED codes) capture IPV in administrative healthcare data is warranted. Finally, while medical records can enhance understanding about IPV, data from medical records are incomplete and underestimate the true prevalence of IPV.
Conclusion
This review provided a summary of 21 empirical research studies that have used ICD codes to measure IPV. This work highlighted the ability to use ICD codes to document IPV, examined the range of ICD codes used to document IPV, and categorized sets of ICD codes used to define IPV as narrow, moderate, or broad. More research is needed to validate and verify codes used to measure IPV to promote consistency across studies. This study underscores that creating national and international standards for documenting IPV using ICD codes would enhance understanding about IPV. The included studies also suggest that enhanced training for medical practitioners regarding the screening and documenting of IPV in medical records is needed to increase the accuracy of prevalence estimates. Finally, ICD codes provide an excellent opportunity to measure IPV, which may provide broader insights regarding this important public health problem.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received grant support for this research from the Blue Shield of California Foundation
Disclaimer
The findings and conclusions in this manuscript are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.