
Abstract
A professional’s response to a client’s disclosure of intimate partner violence (IPV) is shown to significantly impact client outcomes. The quality of a professional’s response is largely influenced by that professional’s beliefs or biases surrounding IPV. This systematic review examined empirical studies conducted in North America and published between 2000 and 2020 evaluating training effects on biases held by professional groups toward victim-survivors of IPV. Search and extraction were conducted in accordance with preferred reporting items for systematic reviews and meta-analyses standards across seven electronic databases. A total of 17 studies met inclusion criteria. Participant groups included professionals from medical, academic, and social/community service disciplines. All included studies reported significant gains on at least one measure of bias. Upon visual inspection, we found no correlations between characteristics of training interventions and reported outcomes on measures of bias. We discuss results in terms of challenges to measuring bias and functional relationships between training interventions, measures of bias, and professional behavior. Variation presented across studies within and between disciplines in regards to training methodology and measurement of bias. Experts in the field of IPV call for a more cohesive approach. We propose the behavior analytic conceptualization of bias as a framework through which interdisciplinary efforts might be unified toward addressing IPV-related biases. Through this lens, we discuss environmental cues within professional settings that might be influencing problematic IPV-related bias. We offer preliminary recommendations for curricular enhancements. We advocate for revision of terms commonly used in IPV-related research and intervention to better reflect and honor diversity across persons experiencing IPV.
The National Coalition Against Domestic Violence defines intimate partner violence (IPV) as physical or sexual assault, intimidation, and/or other abusive behavior willfully perpetrated by one intimate partner against another within a systematic pattern of power and control (2020). IPV is a problem of social significance across all sub-cultures—race, gender, sexual orientation, age, socioeconomic status, religion, nationality, and geographic location (National Coalition Against Domestic Violence, 2020). In the United States, there are more than 10 million victims of physical IPV each year (National Coalition Against Domestic Violence, 2020) and greater than 80 million men and women report experiencing psychological aggression within an intimate partner relationship across their lifetime (Smith et al., 2017).
Problematic attitudes or biases about IPV present a significant barrier to victim-survivor help-seeking and potentially perpetuate IPV (Maiuro et al., 2000; Peters, 2008; Postmus et al., 2011). A large body of research supports the efficacy of educational initiatives for addressing problematic IPV-related biases. The current systematic review summarizes empirical studies in the literature measuring the effects of training on IPV-related attitudes and biases evidenced by professionals. We evaluate factors potentially hampering the collective application of these findings toward widespread change. We discuss IPV-related bias through a behavior analytic lens. We offer suggestions, informed by behavior analysis, to further current interdisciplinary efforts toward identifying best practices for addressing problematic IPV-related biases.
Impact of Professional Response on Client Outcomes
The complex array of needs associated with IPV-victimization may necessitate involvement of medical, social services, and law enforcement agencies (Colarossi & Forgey, 2006; Harris et al., 2002; McCauley et al., 2003). Professionals in these fields are positioned to assist victim-survivors of IPV. A professional’s response to disclosure of IPV victimization can significantly impact outcomes for the victim-survivor. Acknowledgment and validation of IPV disclosure may reinforce survivor help-seeking behavior (Gadomski et al., 2001). Victim-survivors have indicated feeling better able to protect themselves and their children after having disclosed their experience with IPV to a responsive professional (Saunders & Anderson, 2000). Victim-survivors who receive social support and access to resources are more likely to leave an abusive relationship (Bell & Naugle, 2005). By contrast, victim-survivors encountering negative or indifferent treatment from service providers have described the experience as secondary victimization (Khaw et al., 2021; Postmus et al., 2011). Unsupportive responses can suppress help-seeking behavior (Stockwell et al. 2017), thereby perpetuating patterns of IPV (Rose & Saunders, 1986).
Attitudes, Beliefs, and Bias Related to IPV
How a professional responds to disclosure is influenced by that professional’s attitudes (Gover et al., 2011; Kulkarni et al., 2015; Saunders, 2015) or biases related to IPV. The term bias is not prevalent in the current IPV literature. Studies we reviewed more commonly referred to beliefs or attitudes held by professionals. Researchers also targeted myths or stereotypes associated with IPV. Each of these terms describes a category of variables impacting bias. Fishbein (1963) operationally defines beliefs as the probability of a relation between a concept and other concepts. They define attitudes as evaluative mediators, or feelings, associated with those probabilities. Myths are collections of beliefs and associated attitudes that are culturally accepted and socially shared, but generally false (Peters, 2008). Stereotyping occurs when culturally accepted beliefs about a specific group are applied to individual members of that group based solely on their membership in the group (Grant, 2020; Heilman, 2012).
Bias is behavior (thoughts, feelings, and actions) related to a category of stimuli systematically influenced by social and contextual cues (De Houwer, 2019). The term bias, as defined here, encapsulates the aforementioned terms and concepts put forth in the literature to describe this phenomenon. For clarity and conciseness, we use the term bias throughout the following review.
Problematic bias related to IPV
IPV-related bias is what a professional does in response to IPV-related stimuli, under the influence of their beliefs and attitudes about IPV, within the context of their past and present exposure to social and contextual cues related to IPV. Whether a bias is problematic depends on the impact of the behavior on the behaver and/or others (De Houwer, 2019; Matsuda et al., 2020). Problematic IPV-related biases are those that negatively impact victim-survivor recovery. Biases related to IPV typically factor into one or more of the following categories: Victim-blaming, minimization, and exoneration of the perpetrator (Peters, 2008). Victim-blaming biases are the most prevalent (Maiuro et al., 2000).
Victim-blaming bias
Professionals evidence victim-blaming bias when they attribute causal factors for the abuse to characteristics and/or behaviors of the victim-survivor. For instance, clinical professionals might pathologize the victim, assigning diagnostic labels in the absence of addressing IPV as causal. Professionals might imply that a victim elicits or perpetuates abusive behavior through their actions. Victim-blaming bias is also demonstrated when professionals place responsibility for controlling or ending the abuse on the victim-survivor. Professionals may compel victims to leave their abuser. Assistance from professionals may be contingent, overtly or covertly, upon the victim-survivor ending the abusive relationship. For example, social welfare caseworkers in a New York TANF office disclosed a greater willingness to provide aid waivers for clients who took steps toward leaving abusive relationships (Hagen & Owens-Manley, 2002). Healthcare workers have acknowledged making reduced efforts with patients who have historically returned to their abusers (Tarzia et al., 2021). Child welfare workers espousing victim-blaming bias may use a victim’s continued relationship with an abuser as justification to remove children from the care of the victim-survivor (Fusco, 2013; Langenderfer-Magruder et al., 2019; Saunders & Anderson, 2000).
Problematic Bias and Dynamics of IPV
Problematic biases related to IPV are largel attributable to a poor understanding of the complex dynamics contributing to IPV (Perrin, 2017; Tarzia et al., 2021). IPV is marked by a chronic pattern of coercive control functioning to maintain one partner’s power over the other (Notestine et al., 2017). Questioning why a victim stays with an abuser, for example, implies that he or she could choose to leave the abusive relationship (Perrin, 2017). This perspective fails to consider how prolonged exposure to terror tactics and restricted access to resources might impact stay-leave decisions.
Misperceptions about IPV may also inform less appropriate and potentially dangerous clinical and legal interventions (Saunders et al., 2005). For example, professionals advising a victim to leave the perpetrator may not realize leaving is likely to escalate the violence. Coercive control is a hallmark of IPV. When victims attempt to separate, abusers tend to escalate and/or change tactics to regain control over the victim-survivor (Bancroft, 2002). Faulty beliefs or biases about IPV may also inform inappropriate child custody outcomes (Perrin, 2017). Shared custody arrangements often require continued communication between parents regarding visitation and other childcare matters, thereby presenting ongoing opportunities for an abuser to threaten, harass, and exercise control over their former partner (Crossman et al., 2016; Perrin, 2017).
Addressing problematic IPV-related bias
A large volume of research supports the effectiveness of various training platforms for changing professional biases toward IPV (e.g., Campbell et al., 2001; Colarossi & Forgey, 2006; Dubowitz et al., 2011; Knapp et al., 2006; Mason et al., 2017; McColgan et al., 2010; McMahon et al., 2013; Mills & Yoshihama, 2002; Nicolaidis et al., 2005; Oehme et al., 2016; Saunders et al., 2005; Short et al., 2002; Young et al., 2008). Nonetheless, problematic IPV-related biases persist across a range of professional arenas including faith-based (e.g., Drumm et al., 2018), child protection (e.g., Saunders & Anderson, 2000), social welfare (e.g., Saunders et al., 2005), and medicine (e.g., Gadomski et al., 2001).
IPV is a complex issue. The needs of victim-survivors of IPV often span and intersect multiple service domains (e.g., law enforcement, judiciary, social services, child welfare, medical) (Colarossi & Forgey, 2006; Harris et al., 2002; Kulkarni et al., 2015; McMahon et al., 2013). A multi-disciplinary approach would best serve efforts to address problematic IPV-related bias. Significant theoretical differences and methodological variability presents within and across associated disciplines. This has hindered progress toward identifying best practices for systemic change (Bell & Naugle, 2008; Colarossi & Forgey, 2006; Haas et al., 2011; Maiuro et al., 2000; Mason et al., 2017; Miller et al., 2012). Experts advocate for increased collaboration across disciplines to enhance overall effect (Colarossi & Forgey, 2006; Harris et al., 2002; Haas et al., 2011). This will first require an enhanced understanding of training strategies most efficacious for exacting change.
The purpose of the current project was to analyze trends across the existing literature toward identifying best-practice strategies for reducing problematic IPV-related bias evidenced by professionals. We conducted a systematic review of empirical studies in the literature measuring the effects of training on professionals’ IPV-related biases. We summarized professional populations with which current research on IPV biases has been conducted. We compared training methodology in terms of the instruction’s duration, format, and supplementary supports. We evaluated the characteristics of tools used to measure training effects. We analyzed evidence of training impact on measures of bias. Results should inform best-practices toward a more unified approach to addressing problematic biases held by professionals toward clients who have experienced IPV.
Method
We planned and conducted this review in adherence to the preferred reporting items for systematic reviews and meta-analyses (PRISMA) standards of quality (Page et al., 2021).
Search Strategy
The researchers conducted the search for the current review in January 2021. We utilized the search formula: ab(“domestic violence” OR “intimate partner violence”) AND ab(bias OR attitude) AND ab(intervention OR train* OR educ*) AND ab(professional OR therap* OR police OR worker OR court OR judge). Search parameters included empirical studies published in a peer-reviewed journal in the English language between the years 2000 and 2020. We selected search terms through a systematic, iterative process. We gleaned prospective terms from keywords associated with publications addressing bias and/or addressing IPV and from consultation with professionals published in these areas. We conducted search probes systematically across databases to identify terms with the greatest sensitivity and specificity. We chose the final search terms based on search yield toward a formula that was both parsimonious and broad enough to capture literature specific to the topic of this review.
Consistent with recommendations for best practices for systematic review (Bramer et al., 2017), we conducted searches across general databases (i.e., MEDLINE, PsycINFO, and ProQuest Psychology) and specialized databases (i.e., Sociology Database, Family Studies Abstracts, Criminal Justice Database, and Public Health Database). The researchers reviewed reference lists for included studies. We accessed for further consideration all references deemed likely to meet inclusion criteria. We contacted presenters of relevant conferences cited in reference lists via email to request access to presentation materials. For studies that did not include specific items used to measure attitude or bias in the published article, the researchers contacted the corresponding author via email to request access to the measurement tool. This process yielded additional resources. The characteristics of the search are summarized in Figure 1.
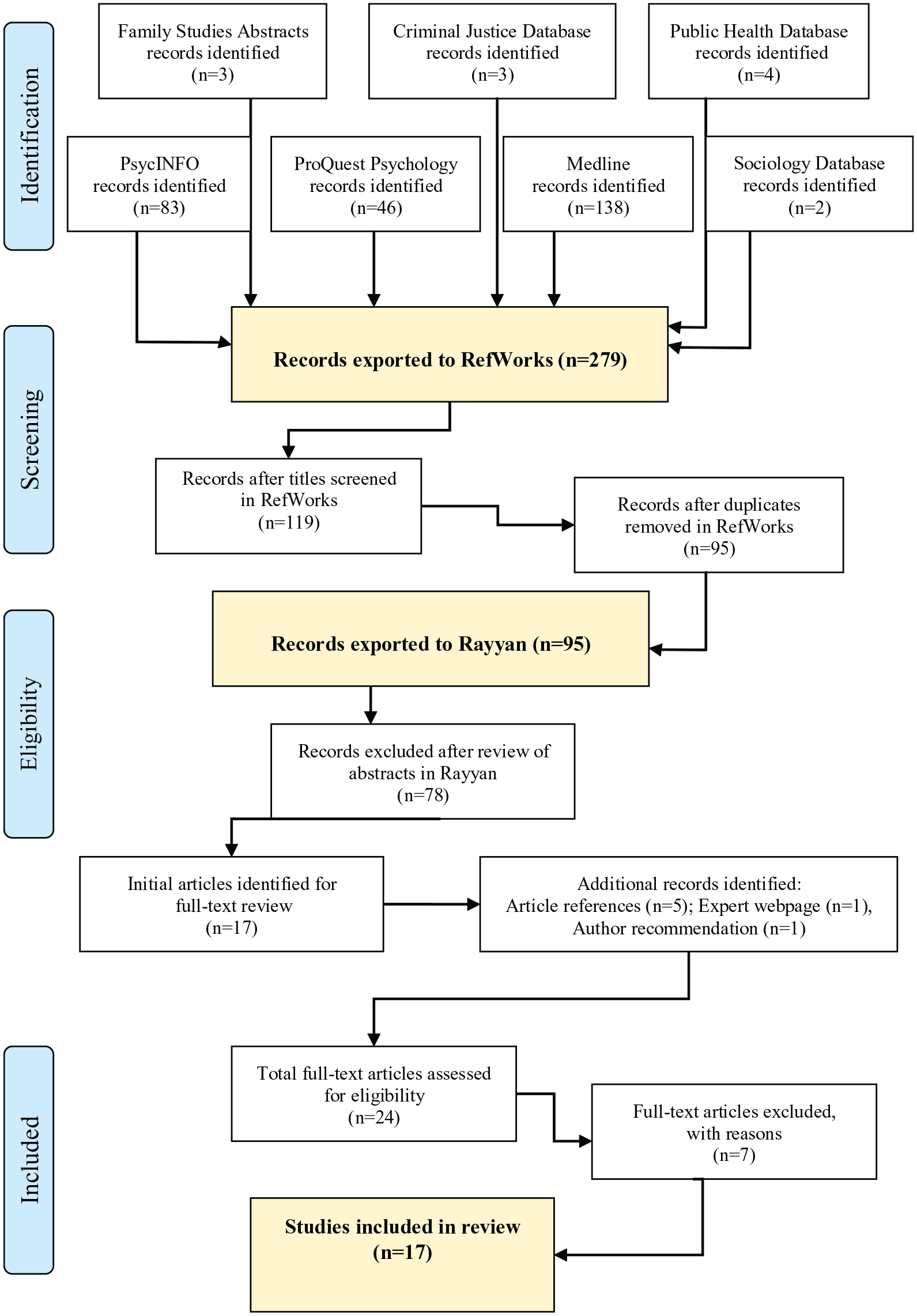
Preferred reporting items for systematic reviews and meta-analyses outcome.
Data Extractions
The first author conducted all screening and eligibility assessments. They imported search results to RefWorks, a reference management software product, for screening and sorting. Then they exported unduplicated potential articles for inclusion to Rayyan, a citation manager that facilitates review and categorization of abstracts. They reviewed in full-text format articles meeting inclusion criteria in the citation and/or abstract. Search results are depicted in Figure 1.
Exclusion Criteria
The research team did not include in this systematic review theoretical papers, meta-analyses, and other non-empirical articles. We excluded empirical studies if at least one outcome was not identified as bias or attitude toward DV or IPV and/or if the study did not include an intervention targeting that outcome. We excluded studies for which the participant group was not identified by profession. We also excluded studies if they were published before 2000 or after 2020; if they were published in a language other than English; or if they were not conducted in North America.
Inclusion Criteria
We included in this review studies meeting the following criteria. Studies were peer-reviewed, empirical studies conducted in North America and published in the English language between 2000 and 2020. The participant population was identified by category of profession. Biases or attitudes held by the participant group related to IPV or DV was a measured outcome. An intervention was applied to address bias or attitudes held by a professional group toward IPV or DV.
Study Quality Assessment
The research team assessed study quality using the Quality Index (Downs & Black, 1998), a tool for rating study methodology. The Quality Index includes 27 items: 10 on reporting standards, 3 on external validity, 7 on internal validity, 6 on confounding/selection bias, and 1 on power. The scale yields profile scores and overall study quality scores. We included in this review studies meeting inclusion criteria with an overall study quality score above 0.70 (corresponding to good quality).
Coding and Data Collection
The researchers manually extracted from each study information specific to the aim of this review. Using a hybrid (deductive-inductive) approach, we extracted and analyzed content related to key findings. We used defined codes to collect information where consistencies presented across studies (e.g., participant group, training format). Where subjectively greater variability was evident across studies, (e.g., supplemental training supports), we recorded descriptive information. We organized data on a Microsoft Excel spreadsheet formatted for study questions and then sorted into data summary tables (see Tables 1, 2, and 3).
Chart of Included Studies.
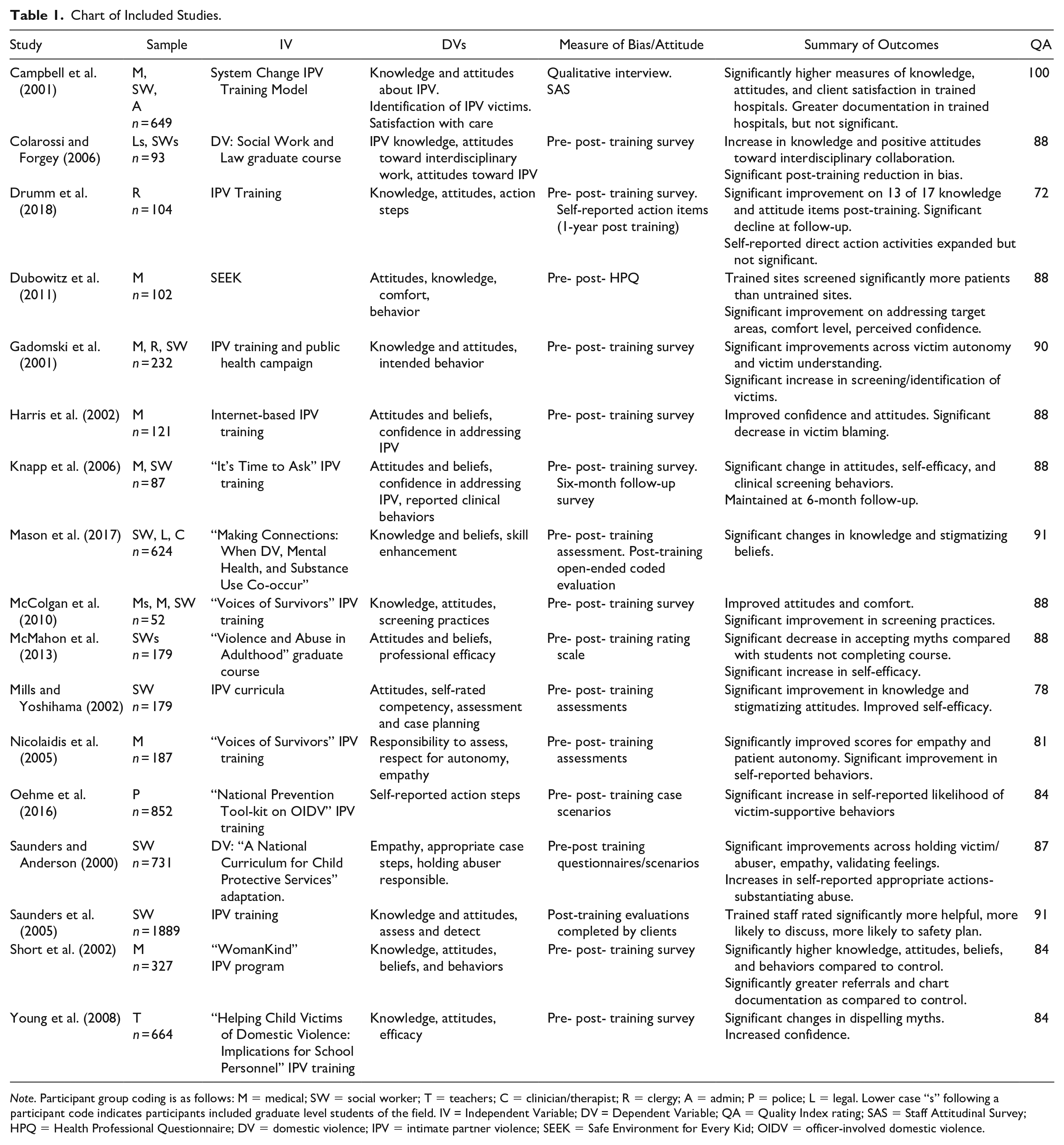
Note. Participant group coding is as follows: M = medical; SW = social worker; T = teachers; C = clinician/therapist; R = clergy; A = admin; P = police; L = legal. Lower case “s” following a participant code indicates participants included graduate level students of the field. IV = Independent Variable; DV = Dependent Variable; QA = Quality Index rating; SAS = Staff Attitudinal Survey; HPQ = Health Professional Questionnaire; DV = domestic violence; IPV = intimate partner violence; SEEK = Safe Environment for Every Kid; OIDV = officer-involved domestic violence.
Across Study Comparison: Survey Measures of Training Effect.
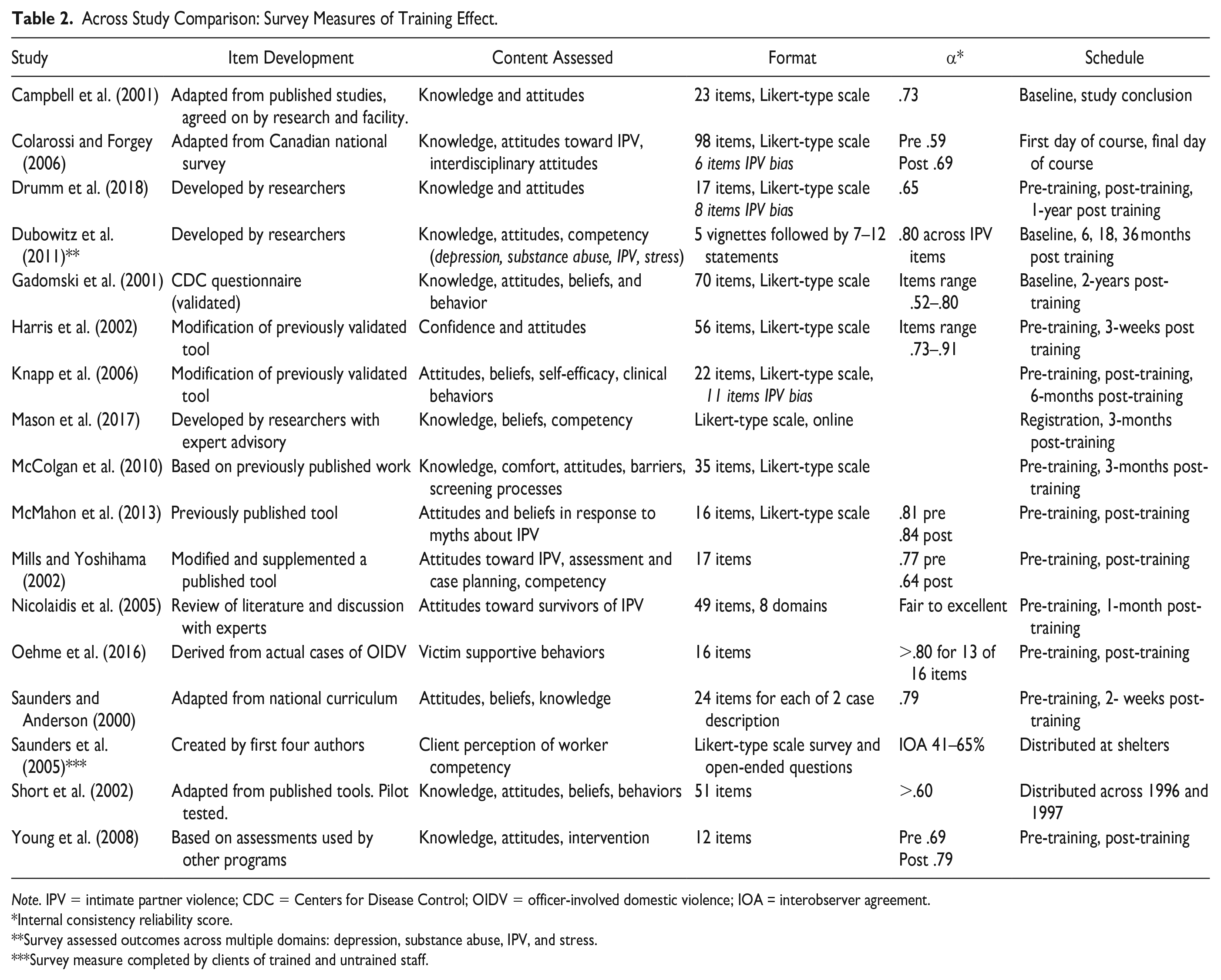
Note. IPV = intimate partner violence; CDC = Centers for Disease Control; OIDV = officer-involved domestic violence; IOA = interobserver agreement.
Internal consistency reliability score.
Survey assessed outcomes across multiple domains: depression, substance abuse, IPV, and stress.
Survey measure completed by clients of trained and untrained staff.
Summary of Training Interventions.
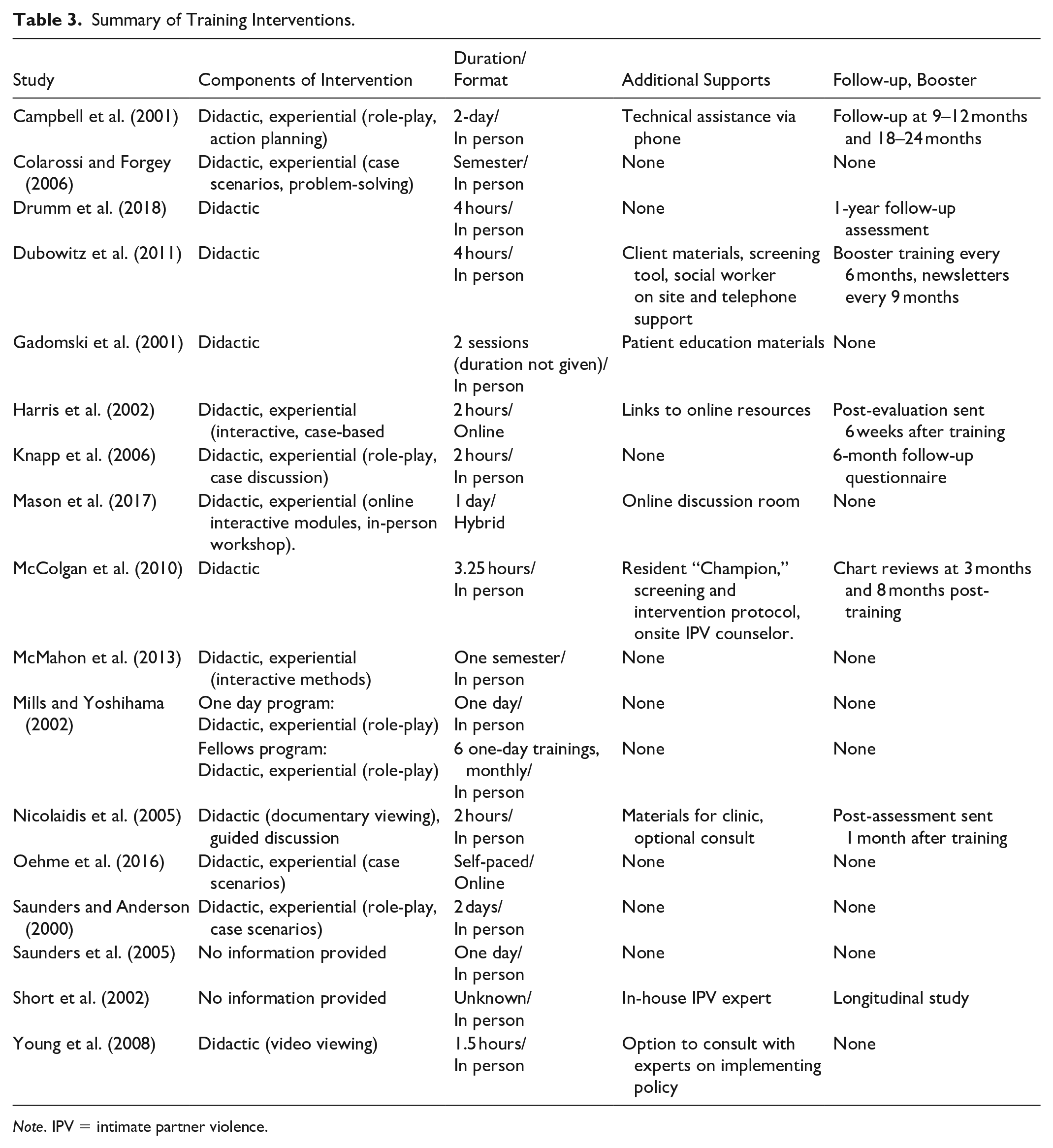
Note. IPV = intimate partner violence.
Sample characteristics
We coded participant groups according to profession into the following categories: medical, social work, teacher, clinician/mental health therapist, clergy, administration, police, and legal (see Table 1). We calculated sample size as the total number of participants.
Measurement characteristics and outcomes
Table 1 includes characteristics of survey instruments and behavioral change indicators. We summarized results for each included study. Statistical significance of reported outcomes is noted where appropriate.
Table 2 summarizes and compares survey measures of training effect across studies. We coded survey item format as Likert-type scale or open-ended. We tracked the total number of items comprising each measure. For studies measuring multiple outcomes, we listed the subset of total survey items pertaining to bias. Substantial variability presented across measures in item development, content areas assessed, and schedule of measure distribution. Therefore, we recorded descriptive data to better convey nuances across studies. We included measures of internal reliability as reported within each study (e.g., as a range, for pre versus post, etc.).
Training characteristics
The researchers coded training components (Table 3) as didactic (lecture-based presentation of information for passive learner consumption) and/or experiential (active learning through experience). We coded training format as in-person, online, or hybrid. We recorded training duration as total hours and/or number of sessions over time. We used descriptive data to capture characteristics of supplemental training supports. For studies with post-training follow-up, we described the nature of the follow-up action and the time frame in which the follow-up action took place.
Data Synthesis
We compared training protocols across studies. We evaluated characteristics of surveys used across studies to measure bias in terms of tool developed, content areas assessed, format of the measure, schedule of measure administration, and internal consistency (see Table 2). We examined differences in training components, instructional format, duration/frequency of training, supplementary training supports, and follow-up if applicable (see Table 3). We analyzed evidence of the impact of training on measures of bias across survey measures (see Table 1).
Inter-Observer Agreement
Search formula
A trained research assistant confirmed the reliability of the search formula across one major database (MEDLINE) and one subject-specific database (PsycINFO). We calculated agreement by dividing the total number of articles recalled across MEDLINE and PsycINFO databases in searches conducted by the first author (n = 138 and n = 83 respectively) by the total number of articles recalled across MEDLINE (n = 167) and PsycINFO (n = 78) databases by the research assistant and multiplying by 100. Agreement was calculated at 90%.
Criteria for inclusion and exclusion
A research assistant trained by the first author reviewed the title and abstract for 30% (n = 29) of the 95 total articles identified at the screening stage. For each article, the assistant coded to include or exclude from further screening. Total count inter-observer agreement measured 100%.
Results
The final analysis included 17 studies (see Table 1). We excluded seven studies during full-text review. Donnelly et al. (2016) was excluded due to a disqualifying score on the Quality Index. Study quality scores as measured by the Quality Index (see Table 1) ranged from 72 to 100 with a median score of 88 across included studies and a mean score of 86.5. Studies with scores in the lower range were generally those that did not include a control group. We excluded another six studies (Berger et al., 2002; Buranosky et al., 2012; Feigelman et al., 2011; Haas et al., 2011; McCauley et al., 2003) because they did not specifically measure bias related to IPV.
Characteristics of Included Studies
Study characteristics are summarized in Table 1. All included studies exposed the participant group to an educational intervention targeting IPV-related biases and empirically evaluated the effects of training protocols on measures of professional biases toward IPV. Participant groups ranged from n = 52 to n = 1887 with a median participant count of n = 187.
Included studies were conducted across a variety of professional disciplines. Four research teams conducted studies in medical settings with medical professionals. Three conducted studies within a medical setting with multidisciplinary participant groups. Three conducted studies with professional social workers as participants. Two (Gadomski et al., 2001; Mason et al., 2017) incorporated professional training into community-wide IPV initiatives. These studies included as participants frontline DV workers, substance misuse counselors, mental health counselors, child welfare workers, clergy, and professionals from the justice sector. Colarossi and Forgey (2006) and McMahon et al. (2013) were unique in that each provided training as semester-long graduate-level social work courses. Other researchers conducted studies with school personnel (Young et al., 2008), church pastors (Drumm et al., 2018), and with police officers (Oehme et al., 2016).
Pre-Post Training Survey Measures
All included studies measured IPV-related bias using self-report survey tools. While all included studies offered some description of the survey measure, only six of the 17 listed all survey items within their publication. Table 2 compares tools across studies in terms of content, format, and schedule of distribution based on information provided by the authors in their published study. Authors of three studies measured biases held by participants using matched pre-post training responses to case scenarios and vignettes. Seven measured biases using Likert-type scale tools administered before and after training. Most studies calculated post-training gains from matched pre-post response sets. Campbell et al. (2001) and Knapp et al. (2006) used unmatched pre-post training surveys.
Survey measure construction
Total number of items on pre-post surveys ranged from 12 to 98, with a mean of 37.7. McMahon et al. (2010) and Nicolaidis et al. (2005) used surveys measuring bias toward IPV exclusively. Survey tools in other studies measured multiple IPV-related outcomes. These included IPV bias, IPV knowledge, sense of responsibility for addressing indicators of IPV, level of comfort in addressing indicators of IPV, and/or self-perceived competence in addressing IPV. Dubowitz et al. (2011) evaluated professional attitudes, knowledge, comfort, and behavior in relation to client indicators of IPV as well asdepression, substance misuse, and stress. Studies using a single survey tool to capture participant responses across multiple outcomes typically reported alpha coefficients specific to each outcome category. Studies did not consistently account for potential interaction effects between items (e.g., impact of questions about IPV knowledge on items intended to measure bias).
Survey measure distribution
Schedules for distribution of post-training measures varied (Table 2). Most studies (n = 14) distributed a single post-training survey. Of these, six distributed surveys immediately after training. When distribution was delayed, latency between completion of training and the post-training survey ranged from 2 weeks to 3 months. Gadomski et al. (2001) is an outlier, surveying 2 years after study initiation. Three studies used repeated post-training measures. Two studies (Saunders et al., 2005; Short et al., 2002) did not report on a specific period for post-survey distribution.
Survey measure development
Methods for survey item development also varied across included studies (Table 2). Gadomski et al. (2001) used a previously validated survey measure created by the Centers for Disease Control. McMahon et al. (2013) included a tool previously validated by Postmus et al. (2011). Nine studies adapted surveys from previously published research. Nicolaidis et al. (2005) developed survey items based on a review of the IPV literature and consultation with IPV experts. Mason et al. (2017) convened an expert panel from which the training curriculum and pre- and post-training surveys were developed. Oehme et al. (2016) used scenarios taken from case files. Three studies (Drumm et al., 2018; Dubowitz et al., 2011; Saunders et al., 2005) used tools developed by the respective research teams. Thirteen of the 17 included studies reported on statistical measures of internal consistency, citing values ranging from .52 to .91 with a median value of .77 (see Table 2). Studies that evaluated alpha scores across pre- and post-training administrations generally indicated test-retest reliability.
Training Methodology
Variation presented in training methodology across studies (see Table 3). Fourteen of the 17 studies provided training onsite. Harris et al. (2002) and Oehme et al. (2016) used an online training format. Mason et al. (2017) took a hybrid approach, providing training through online modules followed by an in-person workshop session. Duration of training intervention ranged in length from a full college term to a single training session as brief as 90 minutes. Most training required between 2 hours and 2 days of classroom time. Three research teams presented materials to participants using a didactic approach. Nine studies supplemented didactic instruction with an experiential component (e.g., role-play, case scenarios, workgroups). Saunders et al. (2005) and Short et al. (2002) did not provide specific information on components of training.
Several studies offered supplemental post-training support (Table 3). These included support from experts in IPV provided online, onsite, and/or via telephone. Written supports were formal protocols for addressing aspects of IPV (e.g., screening and referring) and patient resource handouts. Dubowitz et al. (2011) supplemented initial training with booster training sessions at 6-month intervals and newsletters to participating sites every 9- months.
Post-Training Outcomes
All included studies reported statistically significant improvement across at least one measure of problematic IPV-related bias evidenced by professionals. Most studies distributing post-training surveys after a delay of several weeks or months reported maintenance of gains over time. Drumm et al. (2018) reported significant improvements in IPV-related bias immediately post-training, but participants completing the same survey tool at 1-year post-training showed significant evidence of change toward baseline.
Discussion
We conducted a systematic review of empirical studies in the literature conducted in North America between 2000 and 2020 that measured the effects of training on IPV-related biases held by professionals. Seventeen studies met criteria for inclusion. Participant groups represented professionals in medical, teaching, law enforcement, mental health, and religious and social services sectors. All included studies reported post-training changes in the intended direction on at least one measure of IPV-related bias.
The purpose of the current project was to analyze effective training protocols across the existing literature toward identifying best practices for addressing problematic IPV-related bias in professional settings. Experts in the field of IPV-related bias note significant variation across studies and across and within disciplines (Colarossi & Forgey, 2006; Haas et al., 2011; Maiuro et al., 2000; Mason et al., 2017; Miller et al., 2012). Our results support this conclusion. We found pronounced differences in how bias was defined and measured and in how training was conducted. This variation largely precluded identification of best-practice strategies. Experts advocate for a more unified approach to studying IPV-related bias in professional settings (Mills & Yoshihama, 2002; Peters, 2008; Saunders & Anderson, 2000). We respectfully propose an approach that might facilitate future cross-disciplinary efforts toward more cohesive and efficacious intervention.
Defining and Measuring IPV-Related Bias
All included studies identified biases held by the participant group related to IPV or DV as a measured outcome. We found significant variation across studies in how authors defined and measured IPV-related bias. This presented a challenge in our efforts to conduct across-study comparisons and to synthesize study findings toward identifying best practices.
Measuring bias by proxy
Variation across studies may be attributable in part to a cognitive conceptualization of bias. From this perspective, bias is a latent mental construct that cannot be directly observed. Bias is evaluated indirectly by measuring observable behaviors assumed to be driven by and/or indicative of bias (De Houwer, 2019). The self-report tools used in the included studies exemplify this approach. Each included study defined and measured bias in terms of participant responses to specific items on the self-report tool or tools used for that study. For example, Colarossi and Forgey (2006) defined and measured attitude as endorsement of myths and stereotypes. McMahon et al., 2013 evaluated attitudes as responses to victim-blaming statements and beliefs as responses to myths and stereotypes about victims. Nicolaidis et al. (2005) gleaned data on attitudes from responses to questions about victim autonomy and empathy toward patients who stay in abusive relationships.
Variability in measurement protocols
While each of the included studies reported positive treatment effects specific to IPV-related bias, none of the studies based their findings on the same survey measure of bias (Table 2). Two research teams (Gadomski et al., 2001; McMahon et al., 2013) used previously validated survey measures in their original forms. The majority (n = 9) modified existing measures. Others (n = 6) elected to create a new tool or tools. In line with previous expert appraisals (e.g., Maiuro et al., 2000; Mason et al., 2017), lack of standardization in assessment protocol and survey tools hampered our interpretation of results across studies.
Toward Standardizing Measurement
The IPV research offers several empirically validated self-report measures of bias related to IPV. Examples include the Domestic Violence Myth Acceptance Scale (DVMAS) (Peters, 2008) and the Domestic Violence Blame Scale (DVBS) (Petretic, 2004). At least two scales, the Health Care Provider Survey for Domestic Violence (Maiuro et al., 2000) and the Survivor-Defined Advocacy Scale (Kulkarni et al., 2015), were designed and validated for use specifically in evaluating biases held by professionals toward clients with an IPV history. Studies support the utility of these scales for identifying professional biases toward IPV to inform training needs and to measure training effects (Kulkarni et al., 2015; Maiuro et al., 2000; Petretic, 2004).
The use of standardized measurement tools would facilitate comparison of results across studies. For example, McMahon et al. (2013) evaluated participant bias using a tool previously implemented and validated by Postmus et al. (2011). The authors compared their findings with results reported by Postmus et al. (2011). Both studies found that previous IPV-related training did not correlate with changes in attitudes. Comparisons also highlighted areas for further clarification (e.g.., clearly defining what constitutes “previous training”).
Reconciling standardization and specificity
The included studies were conducted with a range of professional groups, each impacted by unique contextual variables. When existing measures are not appropriate for a given research question or sample, editing a previously validated survey or creating a new survey is indicated (Phillips, 2017). Researchers might bridge specificity and standardization by combining an established measure of IPV-related bias with study-specific measures. If it is not feasible or advisable to use multiple measures (e.g., when resources are limited and/or when carryover effects are a concern), items from standardized measures could be integrated into study-specific tools to facilitate cross-study comparison. Mills and Yoshihama (2002), for example, incorporated into their survey tool several items from the Inventory of Beliefs about Wife Beating (Saunders et al., 1987). The Postmus et al. (2011) measure used in McMahon et al., (2013) contained items taken from the DVBS and the DVMAS. A more standardized approach to measuring biases toward IPV would aid in interpretation of results across studies and in replication and extension of findings.
Multi-point distribution of surveys
The schedule and frequency of survey measure distribution varied widely across included studies (Table 2). Studies employing multi-point distribution schedules (e.g., Drumm et al., 2018; Dubowitz et al., 2011; Knapp et al., 2006) yielded a more complete assessment of learning. Surveys distributed exclusively after training (e.g., McMahon et al., 2013; Oehme et al., 2016) cannot predict persistence of training gains. For studies using a single post-training measure distributed after some delay (e.g., Gadomski et al., 2001), potential confounding variables including maturation reduce the confidence with which changes can be attributed to the training.
Limitations of Self-Report Tools: A Call for Multi-Method Assessment
As noted above, all included studies elected to measure participant bias in terms of responses on self-report measures. Self-report tools are useful for assessing training needs and measuring training effects (Kulkarni et al., 2015; Maiuro et al., 2000; Petretic, 2004). Responses on self-report tools can be predictive of intentional, overt behaviors (Barnes-Holmes et al., 2006; Staniec, 2019). However, reliance exclusively on self-report tools may yield an incomplete (Saunders, 2015) or inaccurate (Sanchez-Prada et al., 2021) estimate of IPV-related bias.
Response bias
Self-report measures are susceptible to influences of social desirability (Dubowitz et al., 2011; Saunders & Anderson, 2000; Saunders et al., 2005). Response bias occurs when participants consciously adjust their responses to self-report items to align with a position they are more comfortable acknowledging (Drake, Primeaux, & Thomas, 2018). Response bias may be more likely with socially sensitive topics (Drake, Codd, & Terry, 2018), including IPV (Saunders & Anderson, 2000; Saunders et al., 2005).
Explicit and implicit bias
Self-report instruments capture explicit biases, which require active attending (Stockwell et al., 2017). Measures of explicit bias can predict intentional overt behaviors (Barnes-Holmes et al., 2006). However, these tools are less likely to capture implicit biases (Drake, Primeaux, & Thomas, 2018; Staniec, 2019). Implicit biases are more automatic or inceptive relational responses (Barnes-Holmes et al., 2006) and are thus less susceptible to conscious manipulation (Baker et al., 2016). Implicit biases are thought to operate at a reduced level of awareness (Scanlon & Barnes-Holmes, 2013). Professionals may not be fully cognizant of their implicit biases, and by extension, of how their implicit biases might manifest in professional interactions.
Multi-method assessment of bias
Multi-method protocols, incorporating measures of implicit and explicit bias, may produce more comprehensive estimates of IPV-related bias. A series of recent studies (Ferrer-Perez, Bosch-Fiol, et al., 2020; Ferrer-Perez, Sanchez-Prada, et al., 2020; Sanchez-Prada, et al., 2021) combined self-report measures of IPV bias with the Gender Violence Implicit Association Test (GV-IAT), a measure of implicit bias. Across all three studies, participants evidenced significantly greater problematic bias on implicit measures than on explicit measures. Sereno (2022) measured IPV-related bias evidenced by dependency professionals toward parents with a history of IPV victimization. The researcher combined explicit measures with the Implicit Relational Assessment Procedure-Intimate Partner Violence (IRAP-IPV). In line with the GV-IAT studies, participants showed greater evidence of problematic bias on the IRAP-IPV than on the explicit measures.
These findings do not discount the value of self-report measures of bias. Rather, results support the use of multi-method protocols (Ferrer-Perez, Bosch-Fiol, et al., 2020; Ferrer-Perez, Sanchez-Prada, et al., 2020; Sanchez-Prada, et al., 2021; Sereno, 2022). Including measures of implicit and explicit bias may yield a more representative estimate of bias. Further, comparisons across explicit and implicit measures can give insight into factors impacting bias and self-reporting of bias. For example, Ferrer-Perez, Bosch-Fiol, et al. (2020) found significant between-group differences on the implicit measure related to participant gender, political affiliation, knowledge, and history. On the explicit measure, between-group differences were significant for gender and political affiliation only. Combining explicit and implicit measures may also control for measurement error (Ferrer-Perez, Sanchez-Prada, et al., 2020).
Are Results Reflective of Behavior in Professional Settings?
While study results are promising, we cannot assume that post-intervention changes in bias reflected on self-report tools would be evidenced in professionals’ interactions with clients (Colarossi & Forgey, 2006; Harris et al., 2002; Nicolaidis et al., 2005; Young et al., 2008). None of the included studies collected direct observation data specific to IPV-related bias. Confidentiality is of paramount importance to victim-survivor safety. As such, it may not be appropriate for research teams to conduct direct observations. See Btoush and Campbell (2009) for a discussion of ethical concerns when including victim-survivors of IPV in research. Three studies included in this review (Dubowitz et al., 2011; McColgan et al., 2010; Short et al., 2002) provided on-site IPV experts as a component in their intervention protocol. Authors did not indicate that experts observed or supervised trained professionals in vivo. Future studies might consider opportunities for embedded IPV experts to assess bias in professional–client interactions. Alternatively, quality of interactions might be measured through client feedback. Two included studies (Campbell et al., 2001; Saunders et al., 2005) support client satisfaction surveys as a compelling option for discretely assessing bias in vivo. Across both studies, clients rated trained staff significantly more positively than untrained staff. Evaluations that include a client feedback component would also communicate to professionals and to clients the essential importance of giving voice to those most intimately impacted by IPV. The now oft-cited slogan, “Nothing about us without us” applies here.
Curricula and Training Protocols
Studies have suggested that IPV training effects are enhanced when training is provided over longer periods (Buranosky et al., 2012; Rose & Saunders, 1986) and/or when training includes experiential components (Buranosky et al., 2012). Collectively, the results of the current review do not support those findings. Studies incorporating training as brief as 1-hour reported results comparable with those incorporating training spanning multiple class periods. Likewise, participants attending didactic presentations showed post-training changes in bias commensurate with those exposed to more experiential curricula.
Curricular content
Content of training was a variable of interest to our research question. In reviewing the included studies, we did not code for training content as articles did not provide sufficient detail. Authors of included studies typically provided a general overview of curricular content. Some studies (e.g., Dubowitz et al., 2011; Nicolaidis et al., 2005) implemented curricula discussed elsewhere in the literature. For example, Nicolaidis et al. (2005) implemented the Voices of Survivors program. Dubowitz et al. (2011) implemented the Safe Environment for Every Kid (SEEK) model. This model is noted to be empirically validated. Future efforts might consider implementing an already validated curricula. As noted above in our discussion of survey measures, standardization would promote comparisons across studies and would facilitate replication toward a better understanding of best practices.
Component analyses
Component analyses would also enhance our understanding of effective intervention. Most training protocols in reviewed studies included multiple components. Which components caused changes in measured outcomes could not be ascertained (Colarossi & Forgey, 2006; Gadomski et al., 2001; McColgan et al., 2010). Component analyses might clarify aspects of IPV training programs causally related to desirable outcomes. Efforts might start with empirically validated training protocols (e.g., SEEK). Having identified components key for exacting meaningful change, researchers could systematically manipulate training format and schedule toward designing maximally effective and minimally resource-intensive curricular interventions.
Summary
Studies included in the present review enhance the literature. This research validates the prevalence of and significance of problematic IPV-related biases in professional settings. Further, results of these studies support the malleability of problematic biases in response to training interventions. The collective impact of the reviewed research has been limited. Within and across disciplines, studies differ significantly in theoretical approach and methodology (Haas et al., 2011; Maiuro et al., 2000; Mason et al., 2017). Experts advocate for a more unified approach to evaluating and addressing IPV-related biases (Mills & Yoshihama, 2013; Peters, 2008; Saunders & Anderson, 2000).
Future Directions: IPV-Related Bias Through a Behavior Analytic Lens
Relative to other social sciences, behavior analysis is new to the IPV table. With respect for the considerable work done in this area, we offer a conceptualization of bias that might facilitate multidisciplinary collaboration toward addressing IPV-related biases in professional settings. From a behavior analytic perspective, the term bias describes a pattern of behavior in response to a category of stimuli (Matsuda et al., 2020) systematically influenced by social and contextual cues (De Houwer, 2019). Conceptualizing bias as behavior may benefit collaborative efforts to address problematic IPV-related bias.
Behavior analysis defines bias as a behavioral response to a stimulus under the systematic influence of variables in context. Bias as behavior is directly observable and measurable. As noted previously, studies included in this review reflect a cognitive conceptualization of bias as an unobservable mental construct. Researchers evaluated problematic IPV-related bias by proxy, relying on measures of observable responses thought to be driven by biased cognitions. Resulting challenges hampered cross-study comparisons. Through a behavior analytic lens, bias can be operationally defined and directly observed. Researchers can then measure bias as rate of response within controlled conditions. As such, a behavioral conceptualization may facilitate comparison, replication, and extension of research findings within and across disciplines toward greater impact.
Behavior analysis assigns causation to the environment. In other words, bias is not a characteristic of or within the individual. Rather, bias is a behavioral response exhibited by the individual under the systematic influence of variables in the environment. Social and contextual cues related to IPV impact a professional’s responding to stimuli associated with IPV through that professional’s experiential history related to IPV. This includes direct experiences with stimuli (Stockwell et al., 2017) related to IPV (e.g., personal relationships, interactions with clients, workplace performance contingencies, etc.) as well as indirect experiences (e.g., exposure to myths and stereotypes about IPV through media, academic or workplace training, etc.) (Buranosky et al., 2012). A professional’s collective experiences related to IPV inform learned relations (beliefs or attitudes) between stimuli associated with IPV. These relations or rules influence how the professional responds to stimuli within the category (Greenwald & Banaji, 1995; Scanlon & Barnes-Holmes, 2013). Researchers operating from a behavioral perspective systematically evaluate conditions within the environment under which problematic bias is evidenced, toward enhanced prediction and control. Resulting analyses pinpoint salient environmental variables and describe functional relations, thereby guiding prescriptive strategies for addressing problematic IPV-related bias as behavior.
To illustrate, we ask the reader to consider a medical professional responding to patient disclosure of IPV victimization. The professional’s behavior (e.g., facial expression, verbalizations, clinical actions) would be influenced by myriad variables including personal history, clinical training, and workplace policies. A history of exposure to faulty rules (e.g., victim-blaming rhetoric) or competing contingencies in the workplace could contribute to problematic bias. By contrast, victim-supportive factors (e.g., effective training and workplace policies) would influence a less problematic response. Analysis of variables impacting the professional’s response to disclosure in this setting would inform targeted strategies for reducing problematic bias and for increasing victim-supportive behavior.
A behavioral conceptualization of bias need not negate a cognitive conceptualization of bias. De Houwer (2019) offers that these approaches are complementary. Cognitive research seeks to understand mental processes mediating implicit bias. Behavioral research describes environmental factors influencing implicit bias. Collectively, this research ultimately seeks to ameliorate associated problematic behavior. A behavior analytic conceptualization of bias may enhance the current literature by shifting the focus of multi-disciplinary efforts toward evaluating observable behavior within context (De Houwer, 2019).
Applications for a Behavior Analytic Overlay
We analyzed included studies collectively and through a behavior analytic lens. Based on those findings, we respectfully offer the following recommendations.
Educate Professionals on Dynamics Contributing to IPV
Include education on dynamics contributing to IPV as a standard component in training curricula. Experts suggest that problematic IPV-related biases are related to a skewed, inaccurate, and/or incomplete understanding of IPV dynamics (Donnelly et al., 2016; Haas et al., 2011; Saunders, 2015). Professionals operating solely from a topographical or typographical knowledge of IPV may evidence increased problematic bias (Bonem et al., 2008; Eilers, 2019; Perrin, 2017).
It is unclear how and to what extent interventions reviewed for this study addressed IPV-related dynamics. Training curricula varied across studies (see Table 1), and authors generally discussed training content in broad strokes. Four authors (Drumm et al., 2018; Saunders & Anderson, 2000; Saunders et al., 2005; Short et al., 2002) do mention content related to IPV dynamics. Young et al. (2008) specifically mention addressing power and control. None of the researchers directly evaluated the impact of this content on post-training measures of bias.
The current literature would benefit from systematic analyses of correlations between a professional’s behavior related to IPV and their understanding of dynamics contributing to IPV. Areas for consideration informed by the literature include factors influencing help-seeking behavior and stay-leave decisions (Bell & Naugle, 2005, 2008; Miller et al., 2012) and recognition of the effects of prolonged coercive control on victim-survivor behavior (Miller et al., 2012).
Address IPV-Related Bias Directly
Interventions intended to reduce problematic IPV-related bias should directly target bias as a behavioral outcome. Awareness of one’s biases can reduce or mitigate the potential negative impact of biases in professional interactions (Baker et al., 2016; Perrin, 2017; Saunders, 2015). Trainers should educate professionals about implicit and explicit biases related to IPV from a behavior analytic perspective. Associated competencies might include recognizing how social and contextual variables (e.g., cultural misconceptions and myths about IPV) influence problematic bias, potentially outside of the awareness of the behaver. Professionals could be given strategies for managing biased behavior. For example, mindfulness-based interventions have proven efficacious for increasing awareness of and reducing reactivity to variables associated with problematic bias (Burgess et al., 2017).
Interventions might prompt participants to examine how IPV-related bias intersects with other problematic biases. IPV-related biases likely stem from gender bias (Eilers, 2019; Perrin, 2017; Peters, 2008), which promote notions of females as sensitive and gentle and males as more forceful or domineering (Drake, Primeaux, & Thomas, 2018). Ferguson and Negy (2004) found both gender and ethnicity significantly impacted biased responses to IPV scenarios. For example, all ethnic groups judged IPV to be significantly more criminal when perpetrated by a male on a female. White participants were more strongly critical when the perpetrator was of African American descent. Exploration of interrelated biases should extend beyond gender and ethnicity, honoring factors including but not limited to age, religion, socioeconomic status, neurodiversity, physical ability, and trauma history. Biases specific to partnering with other disciplines should be evaluated as well (Colarossi & Forgey, 2006; Mason et al., 2017).
Evaluate Contextual Variables in the Professional Setting
Bias is highly influenced by cultural/contextual variables (Cabrera et al., 2020). The characteristics of a workplace setting impact the degree to which larger cultural biases manifest within that setting (Nelson & Bridges, 1999). Yang (2020) discusses the effects of mindfulness on implicit gender and race biases in the workplace. They suggest environments mirroring equitability support reduced problematic biases, whereas indicators that inequitable behavior is tolerated or endorsed will strengthen problematic biases. Professional settings should evaluate contextual variables potentially contributing to problematic IPV-related bias, including informational and assessment materials specific to IPV.
Gendered language as context
Gendered language is prevalent in IPV-related literature and materials. For example, several included studies (e.g., Colarossi & Forgey, 2006; Mason et al., 2017; McColgan et al., 2010) administered survey tools that identified males as perpetrators of IPV and females as victims. Gendered language perpetuates patriarchal views, strengthening relations between gender-identifying terms, gender biases, and IPV biases. Further, gendered language in training and assessment tools fails to account for diversity among IPV victim-survivors (Donnelly et al., 2016). It is generally agreed that women in heterosexual relationships represent the overwhelming majority of IPV victims (Moreira & Pinto da Costa, 2020). Researchers (e.g., McColgan et al., 2010) predicate their gendered approach on this. However, data indicates high rates of IPV victimization for women in bisexual and lesbian relationships as well (Rolle et al., 2018). Prevalence of IPV victim-survivors among gay and bisexual men has been reported at rates significantly higher than those found for heterosexual men (Callan et al., 2021). Estimates of IPV victimization among transgender people is as high as one in two (Yerke & DeFeo, 2016). Associating traditionally female terms and pronouns with victimization and traditionally male terms and pronouns with battery behavior might inform biased responses that discount the experiences of victim-survivors outside these narrowly defined parameters. The use of gender-neutral terms and phrasing may promote less biased and more inclusive interactions between professionals and clients. For example, Harris et al. (2002) and Nicolaidis et al. (2005) supplanted gendered pronouns on their respective survey measures with the gender-neutral term, patient.
Workplace policies as context
Workplace policies and procedures function as contextual variables to influence IPV-related bias evidenced by professionals. Several included studies did acknowledge the role of the environment. For example, Gadomski et al. (2001) created screening tools, patient education materials, and policies to support their training intervention. Campbell et al. (2001) included culture of the emergency department (evidenced by protocols, educational materials, and staff training specific to IPV) as a targeted outcome measure. While none of the included studies directly evaluated the impact of workplace culture on measures of IPV-related bias, relevant anecdotal findings gleaned across studies inform recommendations for environmental considerations.
Organizations should ensure existing policies and procedures are relevant to the setting and of sufficient scope. At the time Oehme et al. (2016) was conducted, many states required IPV-related training for police officers. No states mandated training specific to officer-involved domestic violence (OIDV), despite a prevalence rate of up to 40%. Victim-supportive policies (e.g., screening for IPV victimization) should be evaluated in light of performance contingencies. For example,lack of time to spend with patients is an oft-cited variable precluding IPV screening in medical care settings (Gadomski et al., 2001; Harris et al., 2002; McColgan et al., 2010). Bonus structures that reward high numbers of patient contacts may inadvertantly reduce IPV screening behavior. Organizations should be cognizant of less explicit contingencies potentially impacting workplace culture. Oehme et al. (2016) reference “Code of Silence,” an implicit expectation that officers do not report misconduct evidenced by other officers, as a contextual variable influencing officer behavior surrounding OIDV. Of note, Oehme et al. (2016) further cite evidence that officer adherence to the Code of Silence correlates with behaviors of their peer group and perceptions of the policing department as just and fair.
Limitations of the Current Systematic Review
As noted throughout, variation in approaches to addressing IPV-related biases presents within and across disciplines. This variation extends to terms used across studies to refer to or describe bias. The terms included in the search formula for the current review were those we systematically determined to yield a broad array of potential publications across databases within the purview of the topic. Our decision to omit other terms potentially referring to bias (e.g., “myth” or “stigma”) may have limited the search yield.
A single researcher conducted the literature search and sifted the contents for the article identification process. Due to limited resources, we did not calculate inter-observer agreement for coding or for content analysis. While best practice guidelines recommend at least two separate reviewers conduct a database search and sift, Siddaway et al. (2019) note that this is often not practical or possible. In our method we incorporated strategies recommended to facilitate a high-quality review performed by a single researcher; we planned and conducted the search and sift according to PRISMA established standards for quality reporting, and we provided a transparent and thorough description of the search procedure and results (Siddaway et al., 2019). We measured inter-observer agreement at the screening stage at 100%. We calculated inter-observer agreement across search yield at 90%. This discrepancy is likely attributable to the 3-month delay between the date of the initial search and the date of the search conducted by the research assistant. Publication delays and periodic database updates are likely to impact search results across time (Barroso et al., 2003; Gusenbauer & Haddaway, 2020).
We included studies conducted in North America only. As IPV is prevalent across the globe (World Health Organization, 2021), the narrow geographic focus of the current review might be seen as a limitation. Variables contributing to biases surrounding IPV are largely social (Ferrer-Perez, Bosch-Fiol, et al., 2020). They are shaped by the verbal community within the context of cultural systems. A central function of research measuring IPV-related biases is to increase understanding of these factors toward informing strategies for addressing public policies (Ferrer-Perez, Sanchez-Prada, et al., 2020). As such, a cultural-specific and/or geographic-specific focus may be advantageous. Future studies might compare IPV-related biases across countries or cultures. A cross-geographical evaluation of the prevalence of bias, nature of bias (e.g., minimization, blaming, etc.), and other associated factors could inform areas in which standardized intervention might be appropriate and those in which more geographically specialized interventions are necessary.
Two of the studies included in the review (Colarossi & Forgey, 2006; McMahon et al., 2013) describe outcomes related to students enrolled in Master’s level social work courses. Our decision to include these studies may be a limitation. We predicated inclusion of these studies on graduate students as a “professional group.” Those pursuing degrees beyond the undergraduate level are commonly referred to as professional students. However, contingencies influencing professional training within a graduate program may differ from those influencing professional training in applied settings (e.g., organizational requirements, funding and resources, etc.). Professional-level students may also lack applied experiences as compared to professionals in the field. At least two previous studies (Drake, Codd, &Terry, 2018; Scanlon et al., 2020) found no statistically significant differences in measures of bias between professionals and professionals-in-training. These studies were not specific to IPV-related bias. Additional research is needed in this area. Future studies might consider evaluating training protocols targeting bias across students and more experienced participant groups. Comparisons could enhance our understanding of how formal education, field experience, and practical training intersect.
Conclusion
IPV is a societal ill with high associated costs. In the United States, estimates of the economic impact of IPV range from $5.8 billion to $12.6 billion annually (DV, 2020). The emotional and psychological impact of IPV can span generations. How a professional responds in relation to IPV can impact client outcomes. Interactions informed by problematic biases may alienate victim-survivors, thereby perpetuating IPV. When professionals evidence behavior indicative of survivor-supportive biases, clients are more likely to feel empowered to act toward safety. The literature supports malleability of biases held by professionals. Variation within and across disciplines has hampered collaborative efforts. Intentional cultural evolution requires an analysis of the variables influencing individual behavior and application of that analysis to impact actions at a societal level (Biglan & Embry, 2013). A behavior analytic overlay may aid in unifying existing theories and interventions targeting problematic IPV-related biases to this end.
Implications of the Review for Practice, Policy, and Research
Standardization in research and training methodology is recommended to facilitate replication and extension of findings and to promote best practices intervention strategies within and across disciplines.
Behavior analysis offers a conceptualization of bias through which interdisciplinary efforts toward understanding and addressing IPV-related bias might be unified.
Pairing empirically validated measures of explicit and implicit bias is recommended to provide a more accurate measure of the presence of and the nature of biases held by professionals toward victim-survivors of IPV.
Terminology used to describe and measure IPV in policy and in practice should reflect and honor diversity across individual and cultural experiences of IPV.
Summary of Critical Findings
The current review identified a total of 17 studies in the literature, conducted in North America and published between 2000 and 2020, that empirically evaluate training effects on biases held by professional groups toward victim-survivors of IPV.
All included studies report significant post-training changes in the intended direction for at least one measure of bias.
We found substantial variability across included studies in training methodology and in measurement of biases.
Lack of consistency in methodology limits analysis and application of the collective findings.
Supplemental Material
sj-pdf-1-tva-10.1177_15248380231171186 – Supplemental material for A Systematic Review of Empirical Studies Measuring Training Effects on Biases Evidenced by Professionals toward Intimate Partner Violence
Supplemental material, sj-pdf-1-tva-10.1177_15248380231171186 for A Systematic Review of Empirical Studies Measuring Training Effects on Biases Evidenced by Professionals toward Intimate Partner Violence by Michelle Sereno, Robyn Catagnus, Annette Griffith and Heidi Eilers in Trauma, Violence, & Abuse
Supplemental Material
sj-pdf-2-tva-10.1177_15248380231171186 – Supplemental material for A Systematic Review of Empirical Studies Measuring Training Effects on Biases Evidenced by Professionals toward Intimate Partner Violence
Supplemental material, sj-pdf-2-tva-10.1177_15248380231171186 for A Systematic Review of Empirical Studies Measuring Training Effects on Biases Evidenced by Professionals toward Intimate Partner Violence by Michelle Sereno, Robyn Catagnus, Annette Griffith and Heidi Eilers in Trauma, Violence, & Abuse
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Transparency
This review was planned and conducted in adherence to the PRISMA (preferred reporting items for systematic reviews and meta-analyses) standards of quality for reporting systematic reviews.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.