
Abstract
Gender-based violence (GBV) is a pervasive public health issue that harms victims. Bystanders’ interventions are crucial in preventing the risks of GBV; however, numerous barriers impede their willingness and behaviors to intervene. As a part of efforts to thwart these barriers, this study used a systematic review and meta-analysis to identify such barriers and assess their impact on bystanders’ engagement to intervene. The researchers explored academic databases and included 38 studies in the analysis; we extracted and coded the identified barriers (e.g., lack of responsibility, rape myth) and allocated them to six domains: failure to notice, failure to perceive risk, failure to take responsibility for engaging, lack of bystander efficacy/competency, failure to take an action, and failure of previous intervention attempts. We calculated the overall and domain-specific effect sizes (ES) and performed moderator analysis. The overall ES of the barriers identified in the review were small but statistically significant. The most potent bystander intervention barrier domain was failed previous intervention attempts; the greatest specific barriers therein were negative emotions and feelings of uncertainty after engaging in bystander behaviors. University/college populations were more vulnerable to barriers to intervention than community members. Moreover, the barriers were more prohibitive in incidents of violence against women and sexual assaults than in intimate partner violence. Bystander-focused programs that address negative emotions and feelings arising from prior intervention experiences are needed to foster continued bystander engagement and assistance in GBV; moreover, tailored program content should also be provided for groups most vulnerable to intervention barriers.
Introduction
Gender-based violence (GBV), which encompasses acts of violence directed at individuals based on their sex or gender, manifests in various forms, such as intimate partner violence (IPV), dating violence, violence against women, and sexual assault (UNHCR: The UN Refugee Agency, 2023). This issue poses a serious problem, as the prevalence of GBV is high worldwide, regardless of geographic region and ethnicity (United Nations, 2022). The devastating consequences range from psychological effects (Marchesani, 2015) to severe physical harm, including homicide (Kim et al., 2022).
Recently, prevention strategies with a more socio-ecological perspective have been gaining traction, assuming that the problem of such violence is not limited to perpetrators and victims but extends to the entire community (Mulla et al., 2022). Several prior studies (Taylor et al., 2019; Truman & Morgan, 2014) indeed demonstrated that many GBV incidents have occurred in public settings with the presence of other people, so-called bystanders. Bystanders who witness or are aware of violence can potentially intervene in the situation. Such prosocial responses from others can alleviate perpetrators’ behaviors and empower victims to seek help and escape crises (Gracia et al., 2018). Therefore, defining bystanders’ roles and enhancing their competencies are essential goals to reduce the risk of GBV.
According to the situational model of bystander behavior suggested by Latane and Darley (1970), bystanders are likely to undergo several steps when engaging in GBV situations: they (a) become aware of the situation, (b) interpret it as problematic, (c) take responsibility, (d) know what to do, and (e) take action. However, for each step, there are potential barriers that may prevent bystanders from successfully intervening. For example, Burn (2009) noted that bystanders may fail to notice the situation (step 1) due to sensory distractions or self-focus. Bystanders may also fail to perceive (step 2) an ambiguous or seemingly negligible situation as “risky.” They may fail to take responsibility (step 3) if they consider that a situation is not their concern (Park & Ko, 2020) or assume that someone else will step in when several other people are present. Moreover, a lack of perception of a victim’s worthiness owing to gender-based beliefs can also hinder individuals from assuming responsibility. For example, bystanders were less willing to intervene for victims with a “sexualized” appearance than those with a “non-sexualized” appearance (Gramazio et al., 2021). Bystanders may also fail to take responsibility (step 4) because they lack skills or knowledge (Yule et al., 2022). Finally, they may fail to act (step 5) if they experience audience inhibition, and bystanders may fear criticism of their actions for not conforming to societal norms.
Additional factors and circumstances that could negatively impact bystanders’ intervention intentions and actions have also been identified. For instance, Leone and Parrott (2019) reported that alcohol intoxication decreased bystanders’ intervention behaviors. Moschella-Smith et al. (2022) also reported that, among surveyed college students, those younger than 25 years and those identifying as women were the most likely to engage in bystander intervention behaviors. Recently, scholars have recognized the consequences of intervening experiences as essential factors in predicting the bystander’s later intervention behavior (Krauss et al., 2021; Moschella and Banyard, 2021). Moschella and Banyard (2021) report that bystanders could experience positive and negative feelings after intervening. However, experiencing negative emotions (e.g., “Wished I hadn’t stepped in”) or feeling uncertainty (e.g., “Felt confused about what to do”) while intervening in situations could decrease the likelihood of bystanders intervening in similar situations (Moschella & Banyard, 2021, p. NP3829). In addition, approximately 17%–20% of student bystanders have experienced undesirable consequences, including physical harm and trouble, which are also associated with lower efficacy and effectiveness of later bystander behavior (Krauss et al., 2021).
Understanding the mechanisms underlying these barriers can minimize their effects, consequently enhancing bystander willingness and intervention behaviors. Despite the extensive literature on the subject, there remains a gap in research that systematically reviews these barriers and quantifies their impact on bystander interventions. Furthermore, while scholars have examined barriers in a range of situations, including sexual assault, IPV, teen dating violence, and same-sex IPV, from both men’s and women’s perspectives, there is still a need for more evidence to understand the differing impacts of barriers based on specific circumstances and bystander groups.
This study addresses this gap in the literature by systematically reviewing the barriers that bystanders may encounter in the process of their engagement and evaluating their impact. Drawing from the five categories of barrier domain proposed by Burn (2009), we incorporated an additional domain, “the consequences of intervening,” as suggested by Moschella and Banyard (2021). This study, therefore, utilized six domains: (a) failure to notice, (b) failure to perceive risk, (c) failure to take responsibility for engaging, (d) lack of bystander efficacy/competency, (e) failure to take an action, and (f) failure of previous intervention attempts. The specific objectives of this study were as follows: (a) to systematically review the barriers that affect bystander engagement in intervention, (b) to determine the overall effect size (ES) of these identified barriers, (c) to ascertain the domain-specific ESs of the barriers, and (d) to explore the impact of various moderators (e.g., types of bystander populations and their genders, types of GBV situations, and publication types and years) on ESs.
Methods
Study Design
This systematic review and meta-analysis was performed using five steps: (a) literature search, (b) data extraction and coding, (c) allocation of data to the theoretical framework, (d) bias assessment, and (e) data analysis. The reported findings are in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (PRISMA; Moher et al., 2009).
Searching Strategies
In this review, we focused on the literature addressing the correlates of bystander interventions; “bystander intervention” is defined as the intent to engage (e.g., willingness to intervene) or actions taken (e.g., reporting to police) by individuals who are not directly involved in incidents of GBV as either the victim or the perpetrator. Therefore, we included studies that accessed bystander intentions and behaviors in intervening during GBV incidents and those that explored these correlates using bivariate correlations with Pearson’s r.
We systematically searched seven databases to find relevant literature: PubMed, CINAHL (Cumulative Index of Nursing and Allied Health Literature), Medline, Scopus, Web of Science, PsycArticles, ProQuest Dissertations, and Theses Global. We used three categories of search keywords, including Medical Subject Headings (MeSH) terms: (a) bystander* OR friend*; (b) IPV OR sexual violence OR sexual assault OR rape OR domestic violence OR dating violence; and (c) help OR willingness OR engag* OR intent* OR interven* OR report OR behavior. The final search date was December 31, 2022.
Studies were excluded if they (a) were reviews or qualitative studies, (b) lacked statistical data from bivariate Pearson correlation, (c) focused on violence unrelated to GBV, such as school or workplace bullying, or (d) were written in languages other than English. Following the coding process, additional exclusions were made for studies that (e) did not identify the barriers of bystander intervention, (f) failed to address specific types of barriers, or (g) primarily focused on predicting “no intervention” (i.e., the bystander’s lack of intervention or unwillingness to act).
Initially, we identified 1,507 studies, of which 1,464 were from databases and 43 from manual searches in Google Scholar and C University’s online library search platforms. After removing duplicates, 1,207 studies remained. We divided these studies into three subsets, and each author independently screened and assessed the titles and abstracts in one subset. The authors scored the relevant literature with five, irrelevant studies with zero, and vague studies with three. We then switched the sets and cross-checked the scores given by other authors. Finally, we selected 348 studies that scored five or three from the three authors for full-text assessment. Thereafter, we carefully evaluated the eligibility of the studies by reading the full texts and rerating their scores. Following this rigorous process, 65 studies that scored five were selected.
Data Extraction and Coding
We used a Microsoft Excel spreadsheet to extract and code the data from 65 studies. The extracted data included titles, authors, publication years, study regions, publication types (peer-reviewed journal articles or theses/dissertations), target participants (university/college populations, high school populations, community members, or duty soldiers), participant gender (women only, men only, or mixed sex/gender), proportion (%) of women among the participants, sample sizes, correlates of bystander intervention, correlation coefficients, dependent variables, and instruments used to measure the dependent variables. The second and corresponding authors initially coded the data, and the first author cross-checked the accuracy of the data. We coded 914 independent correlates and their corresponding coefficients.
Theoretical Allocations of the Data
The authors theoretically defined six barrier domains based on the models of Burn (2009) and Moschella and Banyard (2021), as shown in Table 1: (a) failure to notice, (b) failure to perceive risk, (c) failure to take responsibility for engaging, (d) lack of bystander efficacy/competency, (e) failure to take an action, and (f) failure of previous intervention attempts. Among the 914 individual correlates identified, the first author selected barriers that negatively impacted bystander intervention based on the model. This selection was confirmed by the corresponding author through cross-checking. This process identified 194 separate barriers to bystander intervention in 41 studies. The barriers identified in each study were categorized into six domains, as shown in Table 2. The allocation was carried out through several discussions among the authors until a 100% agreement was reached.
Barriers of Bystander Intervention and Allocated Variables.
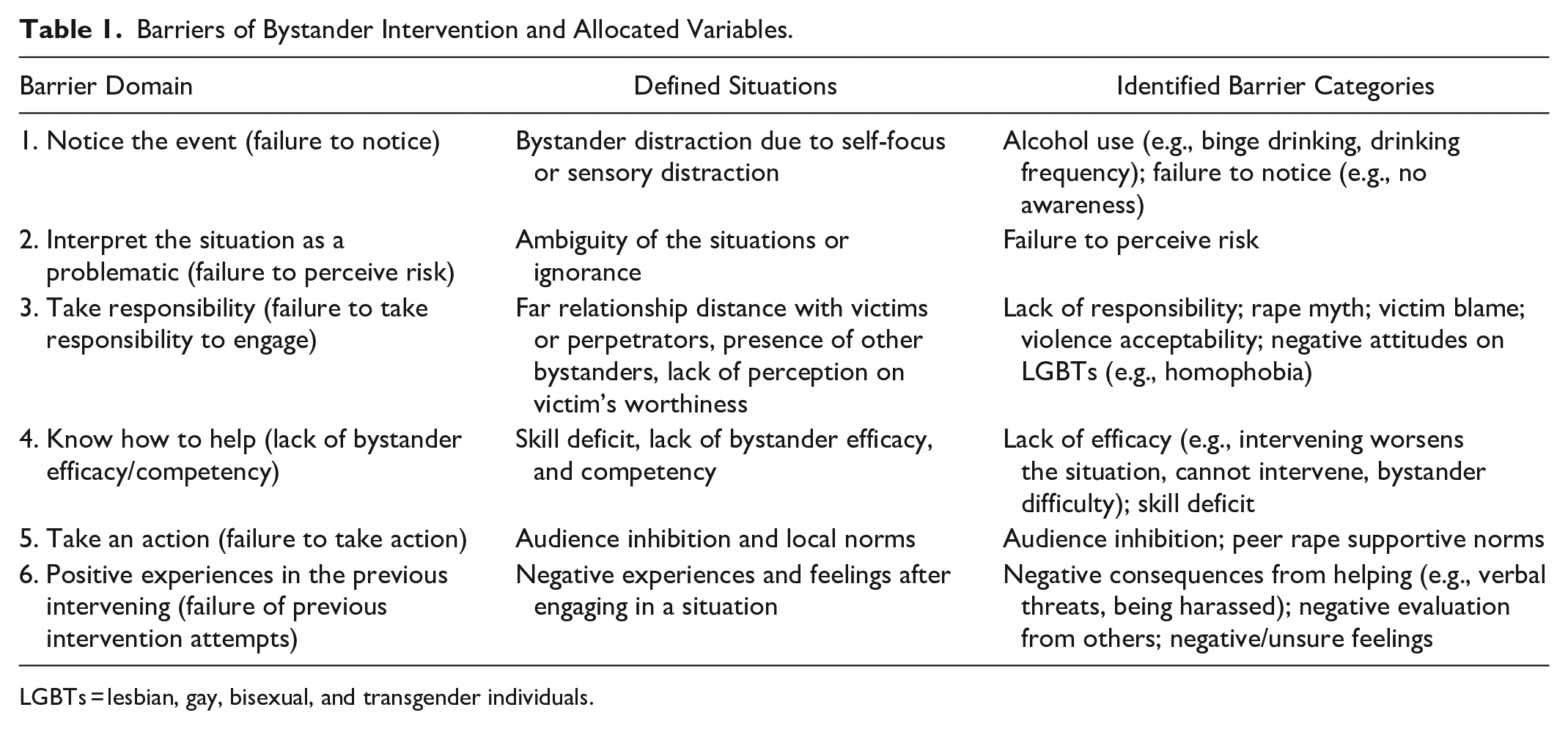
LGBTs = lesbian, gay, bisexual, and transgender individuals.
Lists of Included Studies.
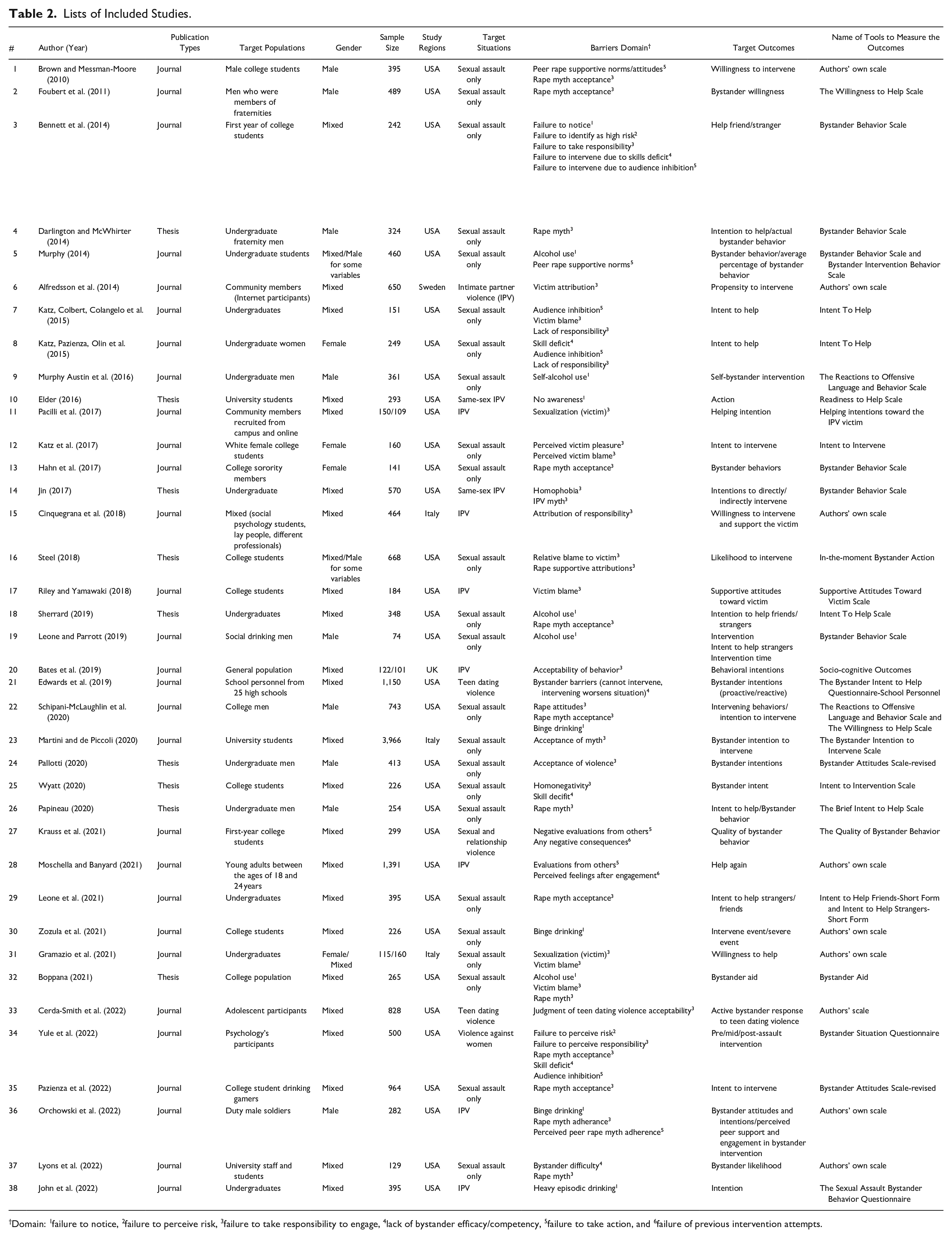
Domain: 1failure to notice, 2failure to perceive risk, 3failure to take responsibility to engage, 4lack of bystander efficacy/competency, 5failure to take action, and 6failure of previous intervention attempts.
Thereafter, as per the exclusion criteria mentioned above, any separate barrier that did not clearly specify and define the types of barriers it represented was excluded. For instance, the “perceived barrier” found in one of the included studies (Chabot et al., 2018) was excluded because its specific types or definitions were unclear, making categorization within a particular barrier domain challenging. In addition, barriers correlating to “no intervention” (predicting bystanders’ lack of intervention or unwillingness to intervene) were also excluded. Throughout this process, we identified 176 distinct barriers in the 38 studies included in the meta-analysis. Figure 1 illustrates the specific search procedure; Table 2 lists the included studies.
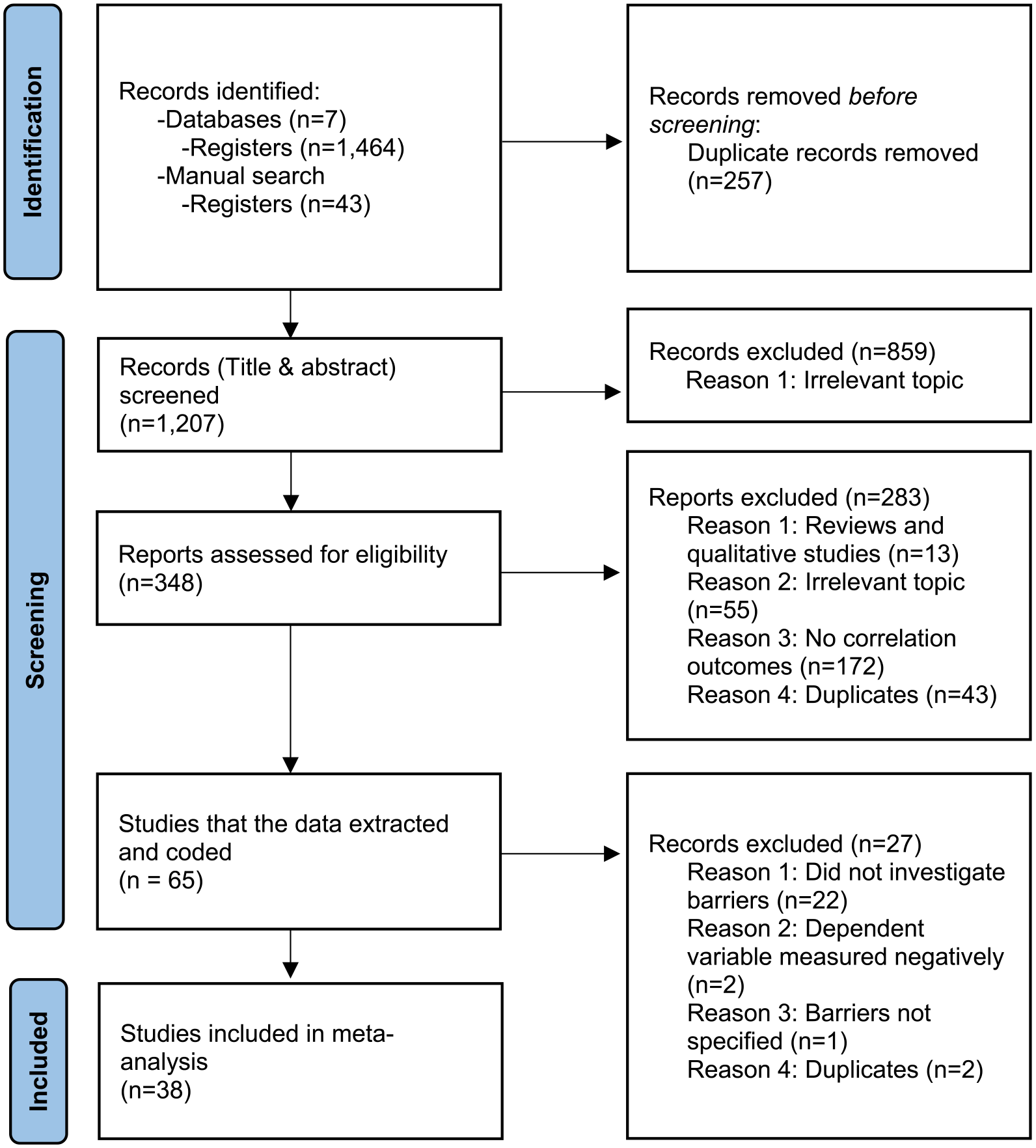
Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flow diagram.
Risk of Bias Evaluation
We evaluated the risk of bias in the 38 studies through discussion based on the Quality Assessment and Validity Tool for Correlational Studies (Wong & Cummings, 2007) criteria: (a) clear aims and objectives, (b) sample size justification, (c) reliable measurement tools, (d) a clear description of the statistical analysis, and (e) clear reporting of the results. Each item was assessed as either “−” (low risk of bias), “+” (potential risk of bias), or “?” (unclear). Figure 2 shows the evaluation results.
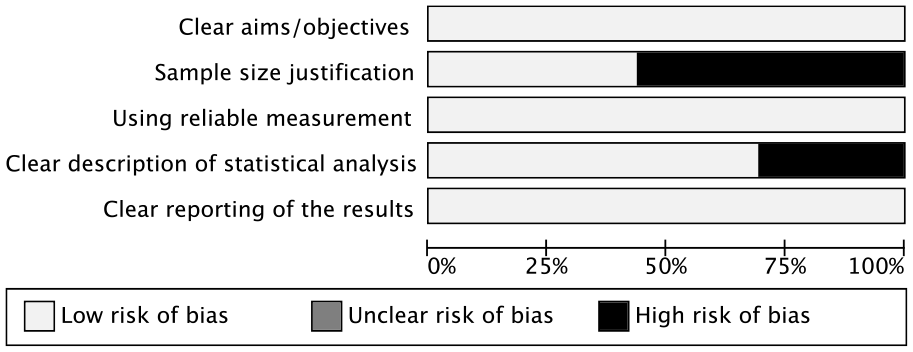
Risk of bias of the included studies.
Data Analysis
Heterogeneity, the variation of the outcomes among the included studies, was assessed using I2 statistics. Heterogeneity is generally considered low, moderate, or high based on an I2 of ≤25%, about 50%, or ≥75%, respectively (Higgins et al., 2003). In addition, we assessed publication bias in the included studies by creating a funnel plot and conducting Egger’s regression test. We also examined ES, which refers to the strength of the relationship between the variables. Small ES is between 0.2 and 0.5, medium ES is between 0.5 and 0.8, and ES > 0.8 is large (Cohen, 1992). To calculate ES, we transformed all extracted correlation coefficients (Pearson’s r) into Fisher’s Z-scores and weighted them by the studies’ inverse variances and sample sizes. We then performed a meta-analysis of variance and meta-regression to test the effects of moderators on ESs, such as target populations and their genders, target situations, publication types, and years. Finally, we used comprehensive meta-analysis software to analyze the data and RevMan to evaluate the risk of bias in the included studies.
Results
Characteristics of Included Studies
The publication years of the studies included in the analysis were between 2010 and 2022, with the majority (n = 33, 86.8%) being conducted in the United States. Three studies were conducted in Italy (8.0%), whereas the rest were conducted in the United Kingdom (n = 1, 2.6%) and Sweden (n = 1, 2.6%). Of the 38 studies, nine (23.7%) were theses or dissertations, and 29 (76.3%) were peer-reviewed journal publications. These studies have examined various target situations to investigate the impact of barriers to engagement. However, most studies focused on sexual assault situations (n = 24, 63.2%), with fewer examining IPV (n = 8, 21.1%), same-sex IPV (n = 2, 5.3%), dating violence (n = 2, 5.3%), violence against women (n = 1, 2.6%), and sexual and relationship violence (n = 1, 2.6%). The sample size ranged from 74 to 3,966, with a total sample size of 93,908. The majority targeted university/college populations, including students and staff (n = 30, 78.9%); a few targeted community members (n = 5, 13.2%), high school populations (n = 2, 5.3%), and male duty soldiers (n = 1, 2.6%). In addition, most studies (n = 26, 68.4%) targeted participants of mixed sex/gender, including both men/males and women/females, whereas a few studies exclusively focused on either women/female (n = 3, 7.9%) or men/male (n = 9, 23.7%) participants.
Heterogeneity and Publication Bias
We observed a high level of heterogeneity among the included studies (I2 = 94.48%, p < .001), which could be attributed to variations in population parameters. Therefore, we utilized a random-effects model to account for the differences between studies (Borenstein et al., 2009). In addition, we found no potential evidence of publication bias per the funnel plot, as it appeared symmetrical (Figure 3). Egger’s regression test result also statistically confirmed a lack of evidence of publication bias among our included studies (Intercept = 1.24, SE = .66, 95% CI [−0.07, 2.56]).
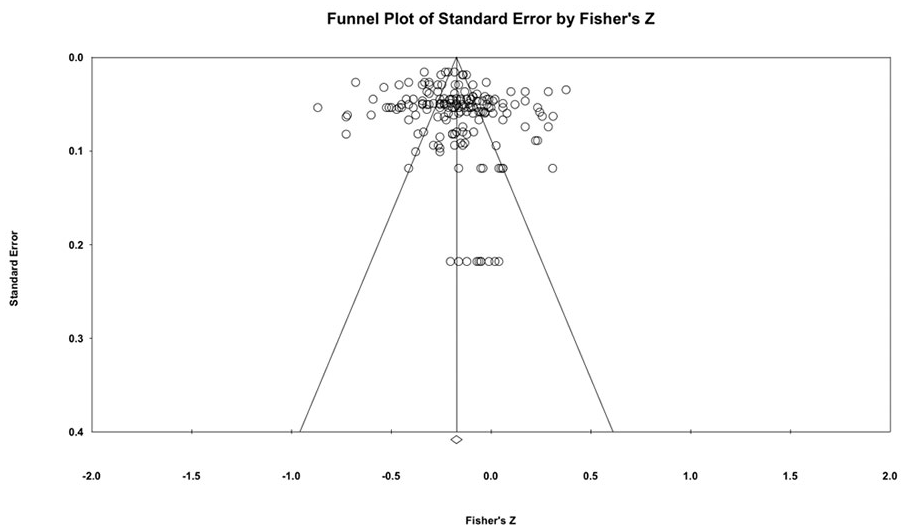
Assessing publication bias.
Overall and Domain-specific ESs
Figure 4 shows the overall ES and ES of each domain. Our findings reveal that overall barriers systematically identified in this study were significantly and negatively associated with bystander intervention, with a small ES (Zr = −0.18 [−0.21, −0.15]). The sixth domain, which encompasses barriers related to the failure of previous intervening attempts, showed the largest ESs with statistical significance (Zr = −0.22 [−0.37, −0.08]). Thus, the most significant and powerful barrier domain associated with bystander intervention was the failure of previous intervention attempts, followed by lack of efficacy/competency (Zr = −0.21 [−0.31, −0.12]), failure to take responsibility (Zr = −0.19 [−0.23, −0.16]), and failure to take an action (Zr = −0.18 [−0.24, −0.12]). The ESs of the failure to notice and perceive risk domains were not statistically significant.
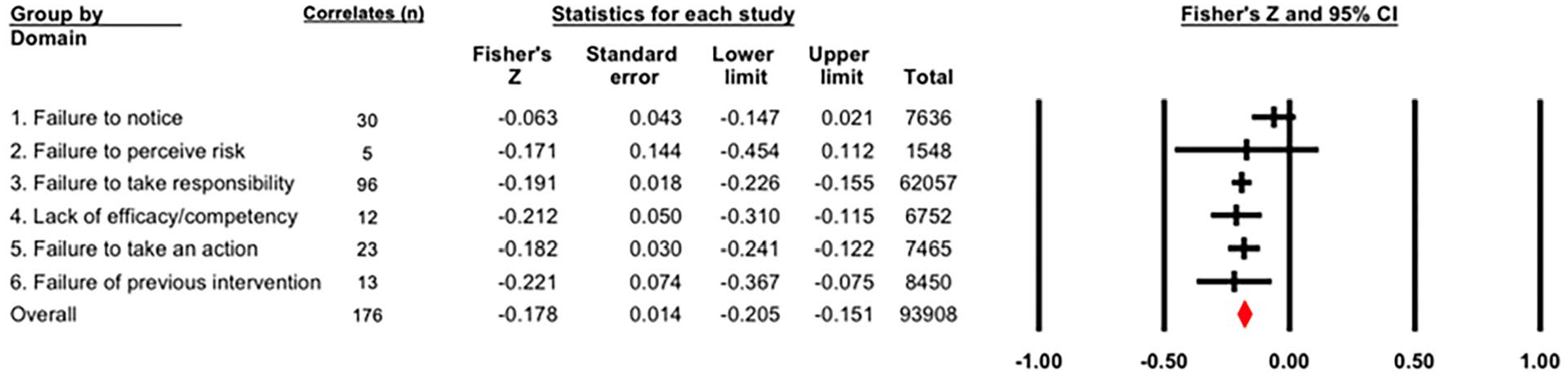
Overall and domain-specific effect sizes.
ESs of the Specific Barriers in Each Domain
Figure 5 illustrates the ESs of the individual barriers within each domain. Neither alcohol use and lack of awareness (in the first domain) nor failure to perceive risk (in the second domain) were statistically significant. We classified five barriers within the third domain; among them, lack of responsibility showed an ES that, although small, was the largest in this domain (Zr = −0.32 [−0.52, −0.11]), followed by rape myth (Zr = −0.20 [−0.24, −0.16]), victim blame (Zr = −0.16 [−0.26, −0.07]), and negative attitudes toward lesbian, gay, bisexual, and transgender individuals (LGBTs; Zr = −0.10 [−0.20, −0.01]). The acceptability of violence was not statistically significant. Both lack of efficacy and skill deficits, which were the fourth domain categories, demonstrated small yet statistically significant ESs. However, skill deficit (Zr = −0.26 [−0.37, −0.14]) showed a larger ES than lack of efficacy (Zr = −0.16 [−0.32, −0.002]). Audience inhibition (Zr = −0.18 [−0.31, −0.06]) and peer rape supportive norms (Zr = −0.18 [−0.25, −0.11]), which were in the fifth domain, demonstrated small but significant ESs. Among the three barriers in the sixth domain, negative and unsure feelings experienced by the bystander when previously engaging with GBV situations demonstrated a medium ES with statistical significance (Zr = −0.55 [−0.81, −0.28]). This ES was the largest compared to negative evaluations from others (Zr = −0.22 [−0.42, −0.03]) and negative consequences of intervening (Zr = −0.08 [−0.14, −0.03]).
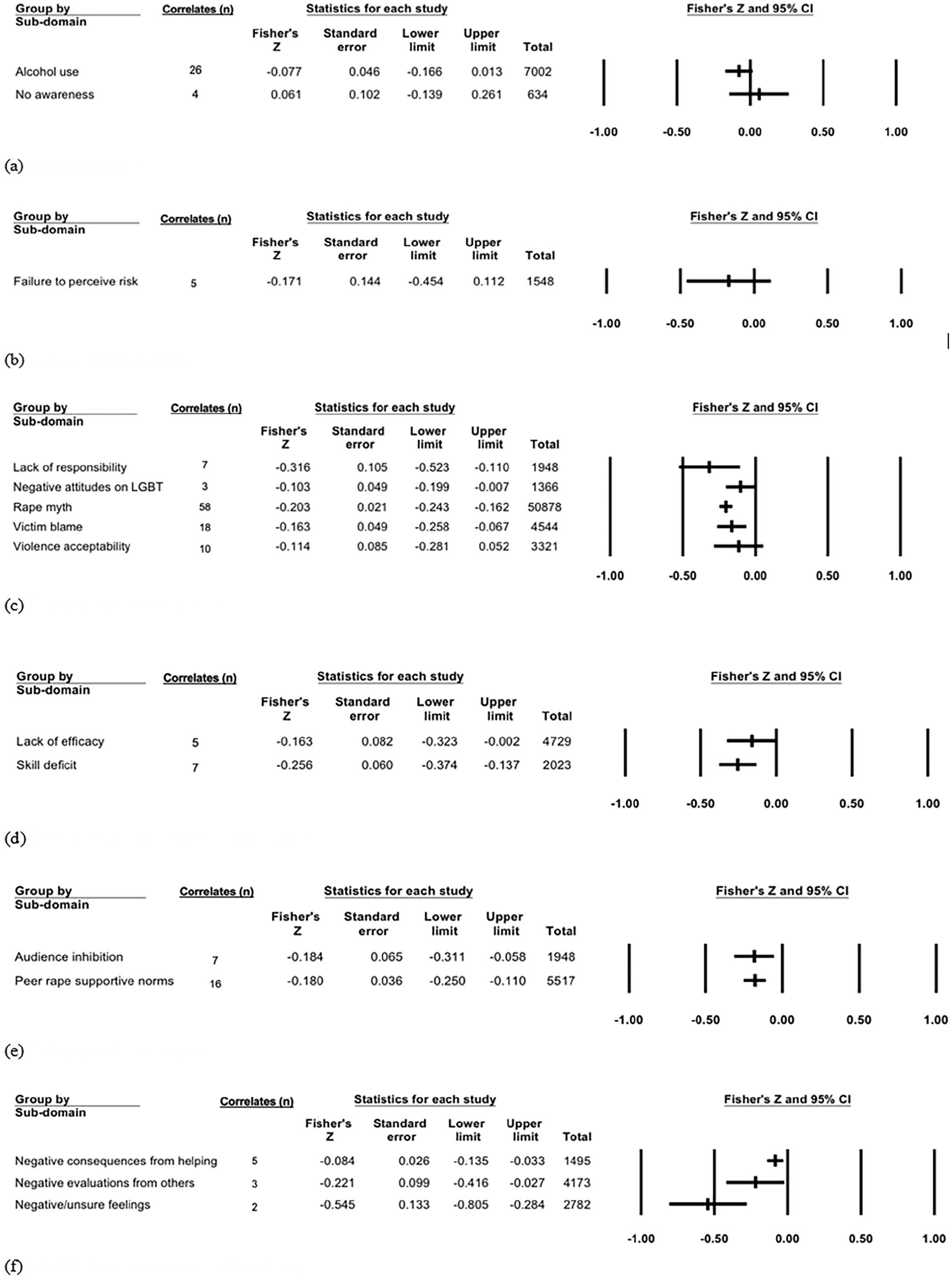
Effect sizes of individual barriers within each domain: (a) failure to notice, (b) failure to perceive risk, (c) failure to take responsibility, (d) lack of bystander efficacy/competency, (e) failure to take action, and (f) failure of previous intervention attempts.
Effect of Moderators on the ESs
We performed a moderator analysis to identify the effect of moderators on ESs. In terms of target populations, university/college populations exhibited larger ESs (Zr = −0.19 [−0.22, −0.16]) than community populations (Zr = −0.11 [−0.20, −0.02]), indicating that the strength of the association between the barriers and bystander intervention was stronger in university/college populations than in communities. The moderating effects on the high school population and male duty soldiers were not significant. Concerning gender, females had the largest ES (Zr = −0.22 [−0.29, −0.16]), followed by participants of mixed genders (Zr = −0.18 [−0.22, −0.14]) and male (Zr = −0.15 [−0.20, −0.10]). An additional meta-regression analysis revealed a trend toward a decrease in ES as the proportion of women increased; however, this trend did not reach statistical significance (Slope = −0.001 [−0.003, 0.001]). The target situations varied among the included studies; however, violence against women (Zr = −0.19 [−0.27, −0.10]) and sexual assault situations (Zr = −0.19 [−0.22, −0.15]) had similarly larger ESs than IPV (Zr = −0.17 [−0.30, −0.06]). The moderating effects of teenage dating violence and same-sex IPV were not statistically significant. Finally, there were no significant moderating effects of the publication year or sample size on ESs. Theses and dissertations had a larger ES (Zr = −0.19 [−0.25, −0.14]) than peer-reviewed journal articles (Zr = −0.16 [−0.20, −0.13]).
Discussion
This study reviewed the barriers that bystanders encounter when intervening in GBV situations and assessed the extent of the barriers’ negative associations with bystander intervention in such situations. The overall ES of the barriers was Zr = −0.18 [−0.21, −0.15] with statistical significance, indicating that the barriers identified in this study have a small but significant negative impact on engaging in bystander intervention.
We established six domains of barriers and categorized the identified barriers based on their concepts. The barriers related to failure to notice and perceive risk did not appear to significantly impede engagement in bystander intervention, which is contrary to previous studies suggesting that greater knowledge and perception of sexual violence and relational abuse led to bystander behaviors (Moschella-Smith et al., 2022; Mulla et al., 2022). Previous qualitative studies also do not support our findings, establishing a failure to identify risk as a central barrier to college students’ intervention behaviors (Hoxmeier et al., 2019). These inconsistent findings indicate the need for further research, particularly to explore the possible and detailed mechanisms between awareness and bystander interventions. As many existing programs aim to teach GBV knowledge and signs to promote awareness and risk perception among bystanders (Park & Kim, 2023), our findings should be revisited through additional research.
One variable allocated to the first barrier domain (failure to notice) was bystander alcohol consumption. Our study found that bystanders’ alcohol use was not a significant barrier to intervention. The findings align with those of Murphy (2014) but diverge from Leone and Parrott’s (2019) report which emphasizes the influence of alcohol intoxication on bystander intervention. The study suggests that men, who are typically more inclined to assist strangers, become less likely to intervene in situations of sexual aggression when intoxicated than when they are sober. According to the authors, this might be due to alcohol consumption altering one’s focus from subtle cues to more prominent and immediate ones, heightening their concern for peer approval. The inconsistencies observed across studies concerning the relationship between alcohol consumption and bystander intervention underscore the need for further investigation.
The sixth domain, failure of previous intervention attempts, was not initially proposed by Burn (2009) but was later proposed by Banyard et al. (2021). For this reason, there has been relatively little research in this domain compared to other domains. Nevertheless, our findings indicate that the failure of previous intervention attempts in GBV situations constitutes the most significant barrier to bystander interventions. Specifically, bystanders’ negative emotions or uncertain feelings resulting from their previous intervention attempts comprised the variable with the strongest negative association with bystander intervention, making it the most influential barrier variable in our study. Given its high impact and the high prevalence of people (17%–20%) who experienced negative consequences after intervening (Krauss et al., 2021), more research is needed to explore and demonstrate the mechanism behind this phenomenon. In addition, evidence-based interventions aimed at alleviating bystanders’ negative feelings and emotions resulting from previous bystander engagement should be developed and implemented.
The remaining domains (failure to take responsibility to engage, lack of bystander efficacy/competency, and failure to take an action) demonstrated similar effects and were all significant barriers. This finding aligns with a previous report that identified skill deficits and lack of intervention responsibility as the most common reasons for inhibiting college students’ interventions in sexual assault situations (Bennett et al., 2014). Previous studies have yielded inconsistent results when comparing the impact of two predictors on bystander intervention: a lack of efficacy and competency, and a lack of responsibility (Bennett et al., 2014; Hoxmeier et al., 2019). These inconsistencies might stem from the inherently contextual nature of predicting bystander intervention. Factors such as the bystander’s perception of the situation and their experiences of uncertainty play a significant role (Hoxmeier et al., 2019). However, our findings show that the lack of bystander efficacy and competency has a more significant negative impact on bystander intervention than the failure to take responsibility for engaging.
Our moderator analysis yielded interesting results identifying university and college populations as the group most affected by barriers. This finding may be related to the campus culture among university and college students. Hoxmeier et al. (2020) pointed out that a significant number of college students refrained from intervening in potentially risky GBV situations—such as when they witnessed an individual taking a person who was intoxicated into their bedroom—because of uncertainty over whether consent for sexual activity had been given. This uncertainty may lead many university and college students to view such situations as ambiguous; thus, they may not have as much responsibility to intervene as other community members. Nonetheless, failing to achieve the second step of bystander behavior (i.e., failing to perceive risk) was not a significant barrier in accordance with the findings of this study. Therefore, further studies are needed to address this matter, especially focusing on exploring the impact of failing risk perception on the possibility of bystander intervention among university and college student populations.
Furthermore, the reviewed studies involving only women demonstrated higher ES than those involving only men, suggesting that women are more susceptible to these barriers than men. However, as the proportion of women did not significantly influence ES, this interpretation should be considered with caution. Scholars have widely studied gender differences in bystander interventions, with previous research suggesting that women might have higher bystander intentions than men (Hackman et al., 2022; Moschella-Smith et al., 2022). However, these findings are inconsistent across cultures and contexts. For example, a study conducted in Ecuador found that women faced significant intervention difficulties and were less likely than men to intervene as bystanders (Lyons et al., 2022). Therefore, simply comparing gender/sex in terms of bystander intervention may not be meaningful, as women and men may have different ways of perceiving GBV situations and motivating themselves to intervene (Labhardt et al., 2017).
Previous studies have identified various conditions and barriers that can affect women’s willingness to intervene as bystanders, including many related to personal safety concerns (Labhardt et al., 2017; Yule & Grych, 2020). For example, women are more likely to feel confident about intervening when they can take control of a situation, receive support from others, or perceive a situation as less dangerous (Labhardt et al., 2017). Although women’s higher awareness of GBV as a risk to themselves may make them more interested in and knowledgeable about violence prevention (Park & Kim, 2022), their focus on safety may also make them perceive barriers more strongly than men when taking on a bystander role (Yule & Grych, 2020). This interpretation may explain why the effects of existing bystander intervention programs are less pronounced in women than in men (Park & Kim, 2023) and why women in cultures where violence against women is prevalent, such as Ecuador, have reported more difficulties engaging in GBV situations (Lyons et al., 2022). Although further studies are essential to explore the differences between men and women in bystander engagement and intervention, sociocultural contexts must also be examined. We also suggest that bystander education programs should be tailored to different gender-specific needs and concerns and focus on educating women about safe and effective intervention strategies.
Although the differences were small, we found a stronger relationship between barriers to bystander intervention in cases of violence against women and sexual assault than in cases of IPV. These results contradict those of Moschella and Banyard (2021), who found that intervening in dating violence incidents was more likely to be associated with negative consequences, such as feeling apathetic about intervening or encountering disparaging reactions from others. Conversely, interventions for sexual assault incidents were more likely to be associated with positive outcomes (Moschella & Banyard, 2021). Given that victims of violence against women and sexual assault are predominantly female, the stronger associations identified in this study may be related to the perpetuation of rape myths or victim blaming, both of which assume that female victims have provoked or can control the situation (Wijaya et al., 2021) or have provided their consent (Hoxmeier et al., 2020). Moreover, in cases of sexual violence, one might misread an action, viewing it as the initiation of an intimate relationship. Consequently, bystanders may be less sympathetic than in IPV situations (Weiner, 2018).
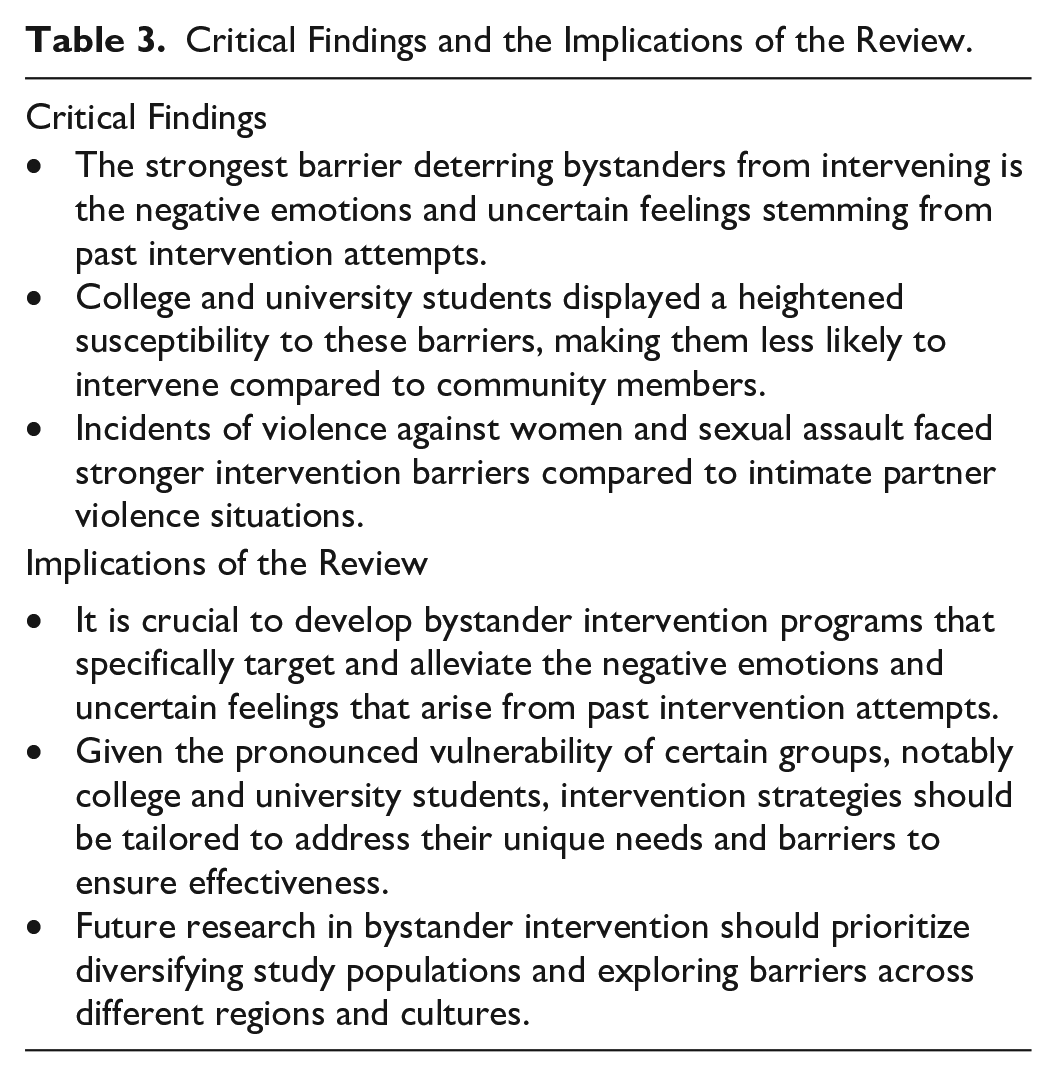
The findings of this review and meta-analysis have important implications for future research (see Table 3). First, the overall ES of the identified barriers in this study was small, suggesting that other significant barriers remain to be explored. Future studies are needed to broaden the scope to incorporate potential barriers beyond those proposed by existing models. Second, there is a lack of diversity in existing bystander-related literature. Most studies, including those in our review, have focused on white, young, and highly educated populations, with few or no studies examining bystander intervention in minority populations such as LGBT individuals and people of color in community settings (DeGue et al., 2014; Kirk-Provencher et al., 2023; Mennicke et al., 2022). Future studies should aim to expand the study populations and regions to address this gap. It is also important to consider that the predictors of and barriers to bystander intervention may vary depending on cultural and generational factors. Therefore, future research should explore cultural and generational influences on bystander intent and intervening behaviors. Finally, bystander training that focuses on alleviating the negative consequences experienced by bystanders and increasing bystander efficacy is required (Krauss et al., 2021). Safety considerations are crucial for minimizing adverse outcomes and encouraging prosocial bystander behaviors. For instance, the “With-You” program developed and evaluated by Park and Kim (2021) exemplifies a bystander education intervention emphasizing safety. This program educates bystanders on how to evaluate situations and includes specific methods for collaborating with victims in creating safety plans.
Critical Findings and the Implications of the Review.
Regarding the study’s limitations, first, our review and meta-analysis only included studies that (a) calculated bivariate correlations using Pearson’s r and (b) were written in English. Therefore, our results may differ from those that would be obtained from an analysis of the entire pool of literature. Second, the primary objective of this study was to explore specific barriers to bystander intervention and calculate the barriers’ ESs based on theoretical models presented by Burn (2009) and Moschella and Banyard (2021). Therefore, we excluded barriers that did not specify their type or definition; this exclusion may have affected the overall ES of the barriers. Third, in our literature search, we exclusively used MeSH terms like “bystanders” and “friends” to identify related articles. As a result, we may have missed pertinent studies using terms such as “stranger” or “acquaintance” to describe bystanders. Lastly, some moderator analyses were conducted with an extremely limited number of studies, sometimes as few as one or two. Consequently, caution is advised when generalizing the findings.
Conclusion
GBV remains a significant public health concern that has devastating consequences for victims. Bystanders can play a pivotal role by intervening in GBV situations; however, barriers continue to hinder bystanders’ active involvement. Through a systematic review and meta-analysis, we successfully mapped these barriers and illustrated their dimensions and power. The most potent barrier to GBV intervention for bystanders was the ineffectiveness of previous intervention attempts; as a consequence of the failure to affect a positive outcome, these bystanders experience negative emotions and feelings of uncertainty that inhibit their further intervention. Therefore, future bystander-related programs should be particularly mindful of this factor and focus on mitigating bystanders’ negative emotional experiences related to previous intervention attempts. Our findings also indicated that university/college populations are particularly vulnerable to these barriers, suggesting that interventions should be tailored to these specific groups. The potency of barriers was also higher in instances of violence against women and sexual assault than in cases of IPV, indicating the need for additional research and intervention strategies for these specific scenarios. The findings of the current study provide important notes for bystander-related education programs, indicating that they should aim not only to increase their efficacy and responsibility but also to address past failures and negative experiences associated with intervention attempts. We believe that the barriers identified in this study can contribute significantly to developing more effective and targeted bystander education programs, thereby promoting a proactive community response against GBV.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) under Grant number 2021R1F1A1048142.