
Abstract
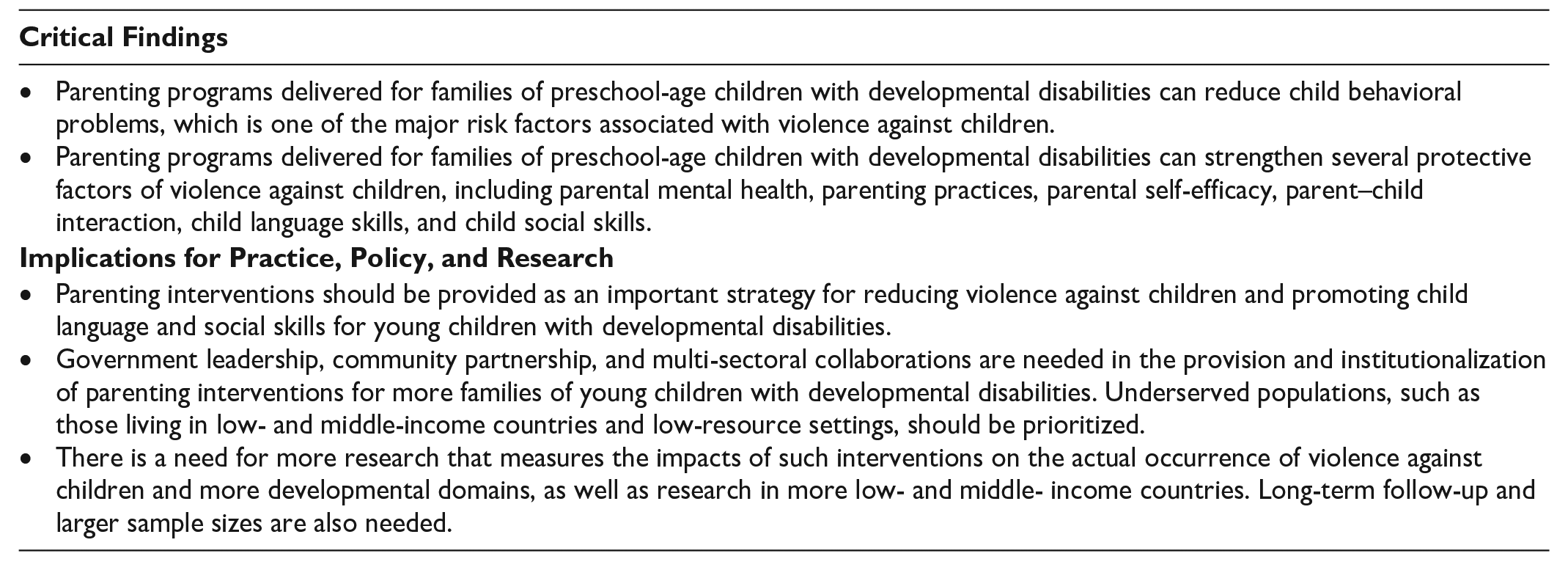
Global guidelines emphasize the critical role of responsive caregiving in terms of reducing violence against children and promoting early childhood development. However, there is an absence of global evidence synthesis on the effects of early childhood parenting programs for children with developmental disabilities. This systematic review and meta-analysis aims to investigate the effectiveness of parenting interventions delivered for preschool-age children with developmental disabilities in reducing violence against children, altering violence-related factors, and promoting child development. We searched for randomized controlled trials with inactive control. Estimates were pooled using robust variance estimations. Meta-regressions were conducted to explore sources of heterogeneity. In all, 33 studies met the inclusion criteria. The results showed that parenting programs improved child behavior, parental mental health, parenting practices, parental self-efficacy, parent–child interaction, child language skills, and child social skills post-intervention. No studies provided data on the actual occurrence of violence against children. Effects might vary by diagnosis, delivery modality, and world region. The findings supported the delivery of parenting programs to alter factors associated with violence against children and promote child language and social skills for families of young children with developmental disabilities, especially attention deficit hyperactivity disorder, autism, intellectual disability, and language disorders. More research using rigorous methods, long-term follow-ups, and transparent reporting is needed, particularly within more low- and middle-income countries.
Keywords
Developmental disabilities are a range of childhood conditions that affect the development of a child’s physical, cognitive, socio-emotional, language, or behavioral functioning (Centers for Disease Control and Prevention, 2022). Some examples of developmental disabilities are attention-deficit/hyperactivity disorder (ADHD), autism, intellectual disability, learning disorders, and language disorders. The global prevalence of all types of childhood developmental disabilities remains unknown, primarily due to sparse data (Black & Lawn, 2018). However, research suggests that at least 53 million children under age 5 worldwide are affected by intellectual disability, autism, ADHD, epilepsy, and vision or hearing loss, with the risk being higher in low- and middle-income countries (LMICs) than in high-income countries or regions (Olusanya et al., 2018).
Children with disabilities are more than twice as likely to experience various forms of violence, including physical, emotional, and sexual violence, as well as neglect (Fang, Cerna-Turoff et al., 2022). Research indicates that these children are at a higher risk of developing behavioral problems, which constitute one of the major risk factors for violence (Pardini, 2008; WHO, 2016). Caregivers of children with developmental disabilities also face greater challenges attending to their children’s needs, which results in elevated levels of parental mental health problems (e.g., stress, depression, and anxiety) and chronic diseases (Hastings et al., 2012; Scherer et al., 2019). Long-held stigma and discrimination against disabilities in some cultures further exacerbate the social isolation experienced by families of children with developmental disabilities (Chan & Lam, 2018). Adversities cluster to heighten the risk of violence against children and reduce child learning opportunities, perpetuating a vicious circle of poor development.
Early childhood is the period when a child is most sensitive to the environment. While it is a window of opportunity for child growth, it also presents greater vulnerability (Black et al., 2017). On one hand, protecting young children with developmental disabilities from violence can increase the opportunities to achieve developmental goals and form the foundation for subsequent skill acquisition; on the other hand, exposing them to violence can amplify the negative consequences of disabilities.
Parents, or primary caregivers, are the architects of a child’s environment and parenting is among the strongest influences on children. Global guidelines, such as the Nurturing Care Framework, the INSPIRE Framework, and the 2016 Lancet early childhood development (ECD) series (The Lancet, 2016; WHO, 2010, 2016), all emphasize responsive caregiving as a key strategy to promote child protection and development. Parenting interventions are structured programs that are designed to improve the quality of parenting and promote positive parent–child interaction, by changing parental attitudes, knowledge, and practices. These programs offer caregivers alternatives to abusive and harsh parenting practices and are among the evidence-based interventions that have the greatest potential to reduce violence against children (WHO, 2016). ECD parenting interventions also enable caregivers to provide optimal childcare and foster child development (Kamel et al., 2019).
Reviews of ECD parenting programs in the general population found links to reduced incidence of physical abuse and better child social, communicational, and cognitive development (Britto et al., 2015; Early Childhood Peace Consortium, 2018). Meta-analyses further showed the effectiveness of such programs delivered for caregivers of non-disabled children aged 0 to 3 years in producing meaningful changes in various factors linked to experience of violence, such as promoting child cognitive, motor, and socio-emotional development; parent–child attachment and interaction; parenting knowledge; and positive parenting practices, as well as reducing child behavioral problems and parental mental health symptoms (Benzies et al., 2013; Britto et al., 2017; Geeraert et al., 2004; Jeong et al., 2021). Four systematic reviews synthesized the evidence of such programs for children with developmental disabilities, also finding that they were effective in altering factors associated with violence against children, for example reducing child behavioral problems (Fang, Barlow et al., 2022; Skotarczak & Lee, 2015; Tellegen & Sanders, 2013), promoting positive parenting practices (Skotarczak & Lee, 2015; Tellegen & Sanders, 2013), and reducing parental stress (Singer et al., 2007). However, all four reviews included a wide age range, from infancy to 17 years old and did not test the effects on wider developmental domains. Moreover, Fang, Barlow et al. (2022) included only programs implemented in mainland China.
Sustainable Development Goal 4 envisions that, by 2030, children with disabilities have equal access to quality ECD care and services. The Nurturing Care Framework further considers parenting support as one of the central pillars for the attainment of SDGs. However, there is an absence of global evidence synthesis to advance our understanding of the impacts of ECD parenting programs for children with developmental disabilities. This review addresses the research gap by assessing the effectiveness of parenting interventions for preschool-age children with developmental disabilities in reducing violence against children and promoting ECD. Limiting the scope to the preschool period serves to narrow down clinical variation. This choice is also influenced by the fact that many developmental disabilities are often not diagnosed before the age of 3 (Boyle et al., 2011). This can be attributed to factors such as delayed symptom manifestation, varying developmental trajectories among children, and the intricate nature of assessments. Limited awareness, cultural factors, and healthcare accessibility also contribute to the difficulties associated with early identification. Furthermore, parenting programs for preschool- and school-age children may be designed to address different parenting needs and dimensions (Webster-Stratton & Reid, 2018).
This review will answer the following questions:
How effective are parenting interventions specifically tailored to preschool-age children with developmental disabilities in reducing the incidence of violence against children and changing related factors such as child behavioral problems, parenting styles, parental competence, parental mental health, and parent–child interaction?
To what extent do parenting interventions for preschool-aged children with developmental disabilities promote positive child developmental outcomes, including cognitive, social, motor, language, adaptive living skills, and diagnostic symptoms?
Methods
This review was conducted using the Cochrane Handbook and reported following PRISMA guidelines (Higgins & Green, 2011; Page et al., 2021). It was pre-registered with PROSPERO (CRD42022320519). We executed sensitive searches in seven international and three Chinese regional databases, as well as seven gray literature repositories, to identify studies published in English or Chinese up to December 2022. We also hand-searched reference lists of relevant reviews and included studies. Search terms included both free-text and medical subject headings that describe population (e.g., preschool children with developmental disabilities), outcome (e.g., child development and violence against children), and design (e.g., randomized controlled trial) of interest (Supplemental Appendices). We did not include terms to specify the type of intervention because the search strategies were also designed to identify studies that evaluated the impacts of early childhood interventions delivered in educational settings as part of the curriculum (Fang, Liu et al., 2023) and clinical therapies, the results of which are reported separately (in preparation).
Eligible interventions were parenting programs that were designed to reduce violence against children or promote child development by increasing parenting knowledge and skills and changing parenting attitudes and behaviors. The programs should be delivered to caregivers of preschool-age children with developmental disabilities. The diagnosis must be made by a professional using reliable screening and assessment. Children should be aged between 3 and 6 or be enrolled in preschool programs and have not entered primary education. The age range was determined by considering regional differences in preschool enrolment: for instance, preschool age is often 3 to 5 years old in the United States but 3 to 6 in China. Studies were eligible for inclusion if they were randomized controlled trials (RCTs) with an inactive control group (i.e., service-as-usual, waitlist, or no treatment), and assessed one of the following outcomes: violence against children (physical, emotional, or sexual violence, or neglect), factors associated with violence against children (child behavioral adjustment, parental mental health, parenting style, parental self-efficacy, or parent–child interaction); or other child developmental outcomes (cognitive, language, social, motor, or adaptive living skills, or diagnostic symptoms). Studies were excluded if children were only at risk for developmental disabilities or if the control group comprised children having no or completely different diagnoses from the intervention group.
Duplicates were removed prior to screening. Two bilingual authors, ZF and CZ, independently screened all references and assessed subsequently retrieved full texts. Disagreements were resolved through discussion with XL. Data were extracted using a standardized Excel spreadsheet, which includes study settings; program features; participant characteristics; outcome measures and point of estimates at post-intervention and follow-up timepoints; and quality assessment criteria. XL extracted 70% of the included studies and ZF extracted the remaining 30%. Data extraction sheets were then exchanged to ensure accuracy.
The Cochrane Risk of Bias Tool (Higgins et al., 2019) was used to assess sequence generation, treatment allocation concealment, blinding of assessors, incomplete outcome data, selective outcome reporting, and other sources of bias, in particular baseline group balance, difference in participant characteristics, and funding sources that may affect the validity of the study. We did not assess the blinding of participants or practitioners to group assignment, as it is not feasible in a parenting intervention. We added four more quality criteria to assess the use of the intent-to-treat method, protocol registration, observational measures, and the level of program developer involvement. XL assessed the quality of all studies and ZF checked for concordance. Conflicts were resolved in the discussion.
Effect sizes were converted to Cohen’s D with a 95% confidence interval (CI) using sample size, mean, and standard deviation. When there were multiple intervention arms, we extracted each intervention group with reference to a common comparator. Robust variance estimation, which allows the inclusion of multiple effect sizes from each study while accounting for effect size dependencies, was used to pool effect sizes in each outcome domain (Tanner-Smith et al., 2016). We created random-effects models, assuming a within-study effect size correlation of .8. Small sample adjustment was used to further reduce type I error (Fisher & Tipton, 2015). Forest plots were created to visualize the results. We quantified heterogeneity with I2 statistics. Separate analyses were conducted for different time points: immediate post-intervention, short-term follow-up (26 weeks post-intervention), and long-term follow-up (over 26 weeks post-intervention) (if any). When a meta-analysis included more than 10 studies, sensitivity analyses were conducted by removing studies that have fewer than six criteria rated as being at low risk of bias for each time point. Publication bias was assessed using funnel plots and Egger’s test (Sterne et al., 2011). Trim-and-fill analysis was also performed to assess the potential impact of publication bias on the meta-analysis results.
When a meta-analysis included more than 10 studies, subgroup analyses were conducted to assess the impact of diagnosis by testing interactions between treatment and subgroups rather than conducting separate meta-analyses for different diagnoses, to reduce type I errors (Brookes et al., 2004). Meta-regressions were also built to investigate other sources of heterogeneity. Potential moderators were home-grown versus imported program, delivery format (individual vs. in groups), delivery mode (in-person vs. online), country income level, and world region. Sensitivity analyses were also conducted to examine the robustness of these results. All data and analysis code will be made available upon request. Data were analyzed using R, version 4.0.3 (R Core Team, 2020) and the package robumeta (Fisher & Tipton, 2015).
Results
Search Results
The search resulted in 18,736 unique references, of which 33 RCTs with inactive control (assessing 35 programs and involving 2,752 families) met the inclusion criteria and were included in the review. Due to missing data, 31 studies were included in the meta-analysis. Figure 1 presents the flow chart. The full references to the included studies are shown in the Supplemental Appendices.
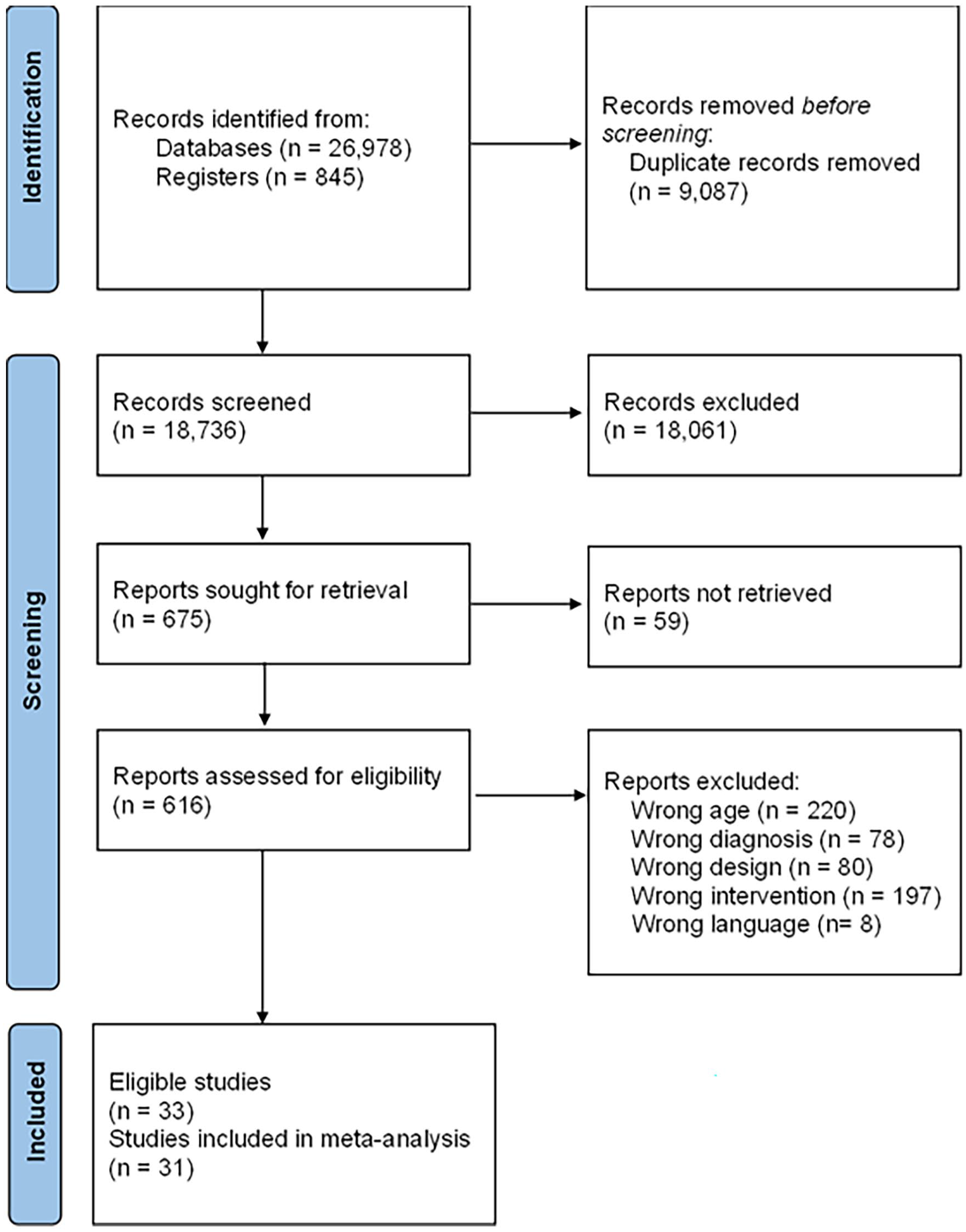
Flow chart.
Study Characteristics
Table 1 presents the characteristics of the included studies and programs. A total of 22 different parenting program brands were identified across the 33 included studies, such as Parent–Child Interaction Therapy, New Forest Parenting Package, Incredible Years, and Triple P. Despite some studies utilizing the same brand, the distinct populations and settings involved in each study led us to treat them as different parenting interventions. All programs were rooted in social learning and attachment theories, with the exception of the Parent-Delivered Qigong Massage Program in the United States (Silva et al., 2011). This unique program was built upon principles of Chinese medicine, incorporating parent-conducted massages to enhance child development, including emotional and behavioral adjustment. Half (17) of the programs provided individualized parenting support, while one-third (11) were group-based interventions. There were also two programs offering both tailored and group services and three not indicating delivery format. Most (26) of the programs used in-person delivery, two were online, four combined in-person and online delivery and one did not report delivery modality.
Characteristics of Included Studies and Programs.
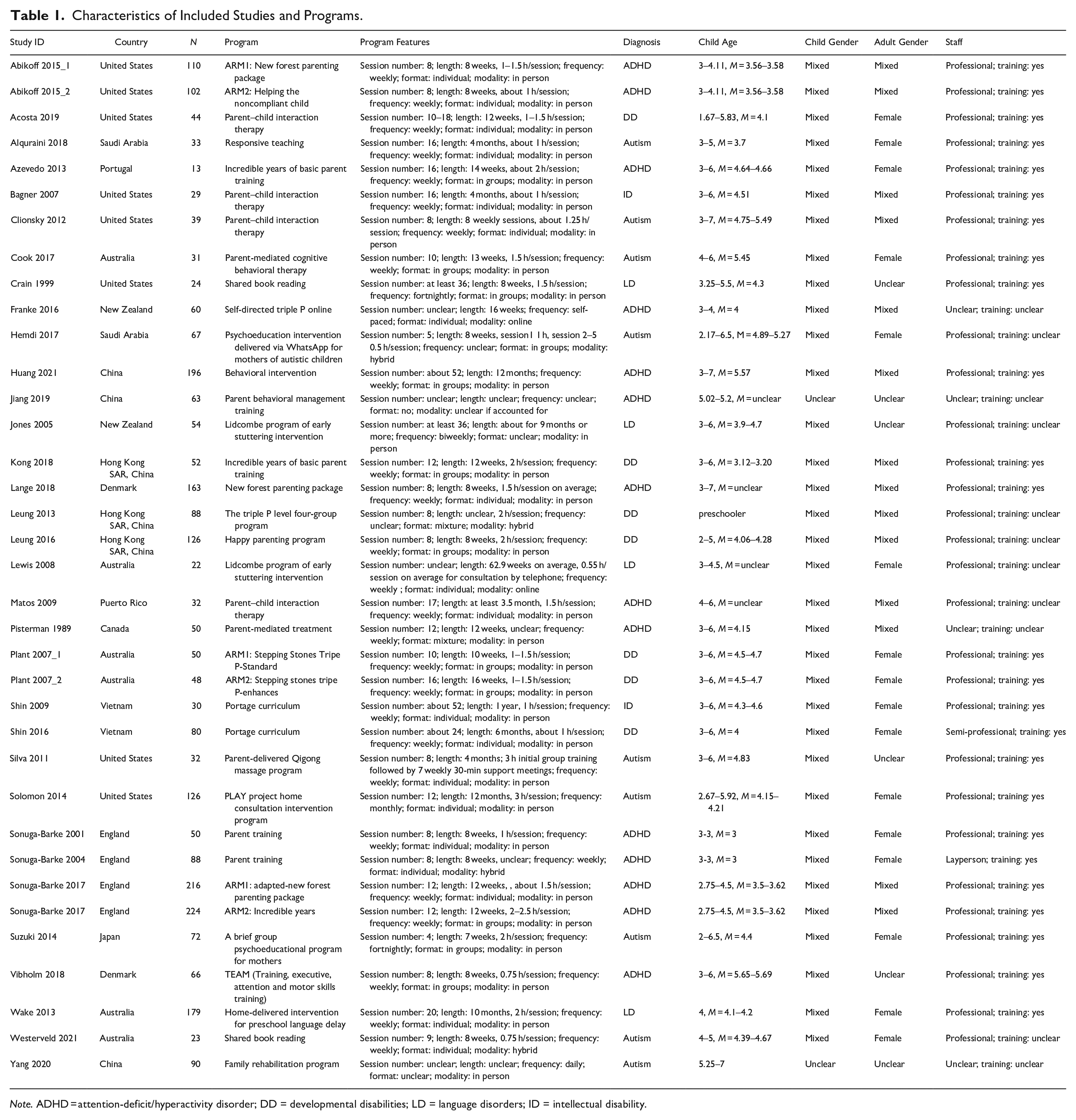
Note. ADHD = attention-deficit/hyperactivity disorder; DD = developmental disabilities; LD = language disorders; ID = intellectual disability.
In all, 31 of all studies involved a mix of boys and girls. Child diagnosis was ADHD in 36% (12) of the studies, autism in 27% (9), language disorders in 12% (4), and intellectual disability in 6% (2). There were also 6 (18%) involving multiple types of developmental disabilities. There were 15 (45%) studies involving only female caregivers, 13 (39%) having both male and female caregivers, and 5 (15%) not reporting adult gender. The adult participants were parents in all studies (23) that reported an adult’s relationship with the child, with one also having grandmothers. Most programs (82%, 27) had professional practitioners, one program had semi-professionals, and another had a layperson as a deliverer. The remaining studies did not provide such information. Two-thirds (22) of the studies reported staff training. Slightly over half (19) conducted fidelity measures.
Of the 33 included trials, 28 (85%) were conducted in high-income countries or regions, including the United States (7), Australia (5), the United Kingdom (3), Hong Kong SAR China (3), Denmark (2), New Zealand (2), Saudi Arabia (2), Canada (1), Japan (1), Portugal (1), and Puerto Rico (1). Three trials were conducted in an upper-middle-income country (China), one in a lower-middle-income country (Viet Nam in 2015), and one in a low-income country (Viet Nam in 2008). With regard to world regions (based on WHO classification), almost half (N = 16) were from the Western Pacific, 27% (9) from the Americas, 18% (6) from Europe, and 6% (2) from the Eastern Mediterranean. No trials were identified in South-East Asia or Africa. Two of the included studies were reported in Chinese.
Outcomes and Measures
The 33 included studies provided 327 effect sizes of 11 outcome domains associated with risk or protective factors of violence against children. Of the 327 estimates, 60% (196) were parent report, 24% (77) used observational measures, 9% (30) were teacher report or therapist report, and 2% (5) used standardized tests. Eighty-eight percent (288) reported using validated measures.
A range of outcome measures was used across the included studies. Child behaviors, for instance, were assessed through various scales, such as the Conners Rating Scale-Revised, the Child Behavior Checklist, the Eyberg Child Behavior Inventory, the Vineland Adaptive Behavior Scales, the Strengths and Difficulties Questionnaire, the Disruptive Behavior Scale for Children, the Revised Family Observation Schedule (observational), the Swanson Nolan and Pelham-IV, as well as the Aberrant Behavior Checklist. Similarly, parental mental health was evaluated using a variety of assessments, including the Parenting Stress Index-Short Form, the Depression Anxiety Stress Scale 21, the Hospital Anxiety and Depression Scale, the Family Strain Index, the Arabic Scale of Happiness, the Parent Problem Checklist, the Center for Epidemiologic Studies Depression Scale, the General Health Questionnaire, the Short-form Health Survey, the Zarit Caregiver Burden Interview, and the Beck Depression Inventory. The two studies reported in Chinese utilized standardized tools that had been translated and validated within the local context. A comprehensive list of the outcome measures employed in each study is provided in the Supplemental Appendices.
Risk of Bias
In all, 22 out of the 33 studies adopted an intent-to-treat approach to analyze their data. To mitigate potential bias arising from self-reporting, 19 studies utilized observational measures. In efforts to counteract selection bias, 12 studies utilized computer software to generate random sequences, while three engaged third-party entities for independent sequence generation. Three studies employed a random lottery method, and one study employed the odd-even method, with the allocator being blinded. One study did not report details on sequence generation and only mentioned no blinding during randomization; thus, it was rated at a high risk of bias. Inadequate information on sequence generation and/or allocation bias hindered the assessment of the risk of selection bias in 15 studies.
In all, 17 studies implemented blinding of outcome assessors to minimize detection bias. However, two studies involved non-blinded outcome assessors and were thus considered high risk for detection bias. The remaining 14 studies did not provide sufficient details on assessor blinding, posing challenges in assessing their risk of detection bias. Due to the nature of parenting interventions, blinding caregiver participants or practitioners to group assignments was not feasible.
In all, 26 studies reported implementing statistical methods to account for dropouts, while two studies did not address the missing follow-up data, potentially introducing participant attrition bias. Five studies did not explicitly indicate the existence of dropouts. The risk of selective reporting was low in all studies except two, where data on certain outcomes were unavailable due to computer failure or errors in electronic setup; no indications of selective reporting were found in the remaining studies.
Regarding baseline comparability, three studies reported significant group differences in outcome measure, and an additional four studies reported potentially unbalanced baseline data in other participant characteristics (e.g., child diagnosis, maternal age, maternal depressive symptoms, and parental education level). However, it remains unclear whether such imbalances might have arisen due to chance. Furthermore, one additional study did not report baseline comparability and was thus judged to be at high risk of bias. We did not identify any source of bias that might have been caused by funding sources. The program developer was involved as a co-investigator in seven studies, an advisor in six studies, and an implementer in three studies. Six studies did not involve program developers, with the remaining 14 studies not providing such information. Nine trials were pre-registered.
Figure 2 provides an overview of quality assessment weighted by sample size. More details about quality assessment are presented in the Supplemental Appendices.
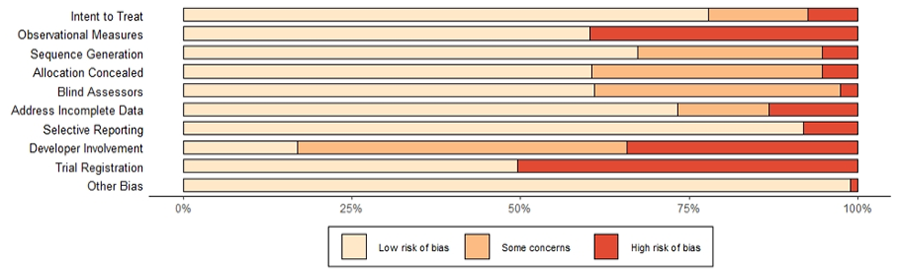
Risk of bias summary.
Meta-Analyses: Effects of Parenting Programs on Violence against Children and Associated Factors Post-Intervention
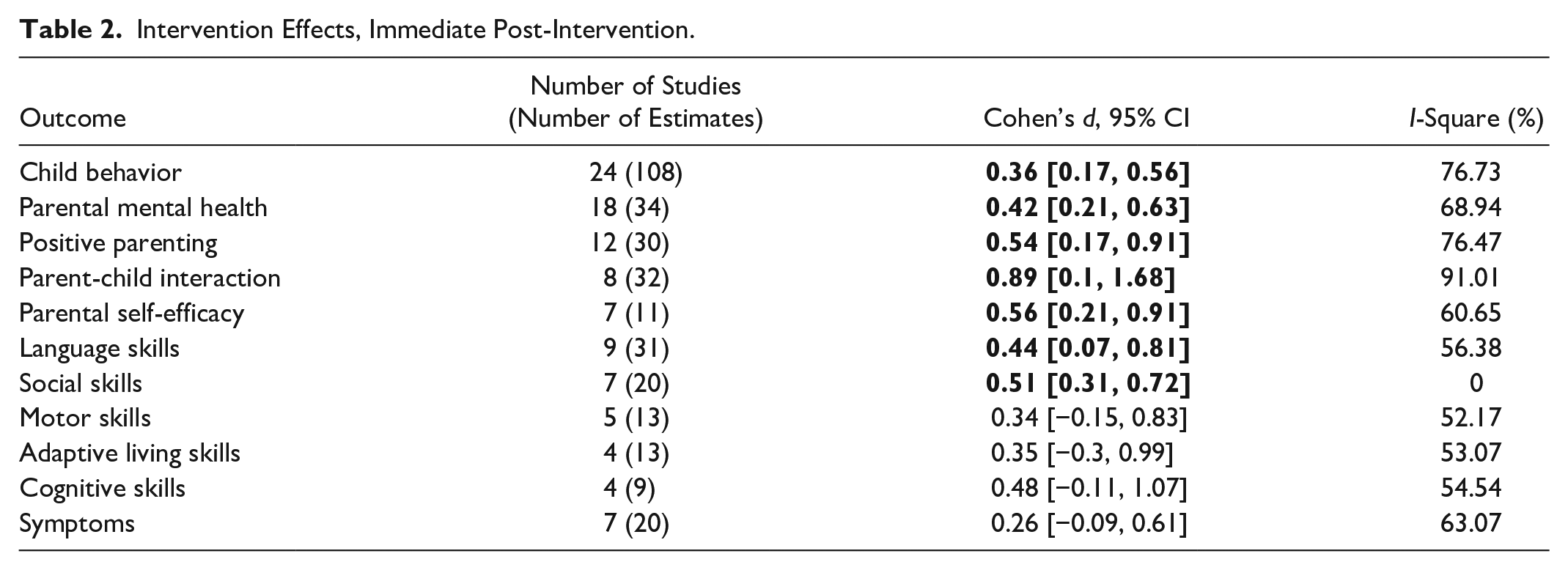
No studies reported the actual incidence of violence against children. Meta-analyses (Table 2) found that parenting programs were more effective in altering multiple factors associated with violence against children than inactive controls at immediate post-intervention. Specifically, the results showed small effects in reducing child behaviors (d = 0.36, 95% CI [0.17, 0.56], I2 = 76.73%; 24 studies, 108 estimates) and parental mental health problems (d = 0.42, [0.21, 0.63], I2 = 68.94%; 18 studies, 34 estimates); medium effects in promoting positive parenting practices (d = 0.54, [0.17, 0.91], I2 = 76.47%; 12 studies, 30 estimates) and parental self-efficacy (d = 0.56, [0.21, 0.91], I2 = 60.65%; 7 studies, 11 estimates); and a large effect in increasing positive parent–child interactions (d = 0.89, [0.1, 1.68], I2 = 91.01%; 8 studies, 32 estimates). Sensitivity analyses yielded similar results: child behavior (d = 0.34, [0.05, 0.64], I2 = 80.56%; 16 studies, 84 estimates), parental mental health (d = 0.37, [0.2, 0.53], I2 = 21.62%; 13 studies, 22 estimates), and positive parenting (d = 0.55, [0.13, 0.97], I2 = 78.53%; 11 studies, 28 estimates).
Intervention Effects, Immediate Post-Intervention.
Meta-Analyses: Effects of Parenting Programs on Other Child Developmental Outcomes Post-Intervention
A smaller number of studies assessed other child developmental outcomes. Results showed small to medium effects favoring the parenting programs post-intervention in improving child language (d = 0.44, [0.07, 0.81], I2 = 56.38%; 9 studies, 31 estimates) and social skills (d = 0.51, [0.31, 0.72], I2 = 00.00%; 7 studies, 20 estimates). No intervention effects were detected with regard to child cognitive ability (d = 0.48, [−0.11, 1.07], I2 = 54.54%; 4 studies, 9 estimates), motor skills (d = 0.34, [−0.15, 0.83], I2 = 52.17%; 5 studies, 13 estimates), adaptive living skills (d = 0.35, [−0.3, 0.99], I2 = 53.07%; 4 studies, 13 estimates), or diagnostic symptoms (d = 0.26, [−0.09, 0.61], I2 = 63.07%; 7 studies, 20 estimates).
Meta-Analyses: Effects of Parenting Programs at Short-Term Follow-Up
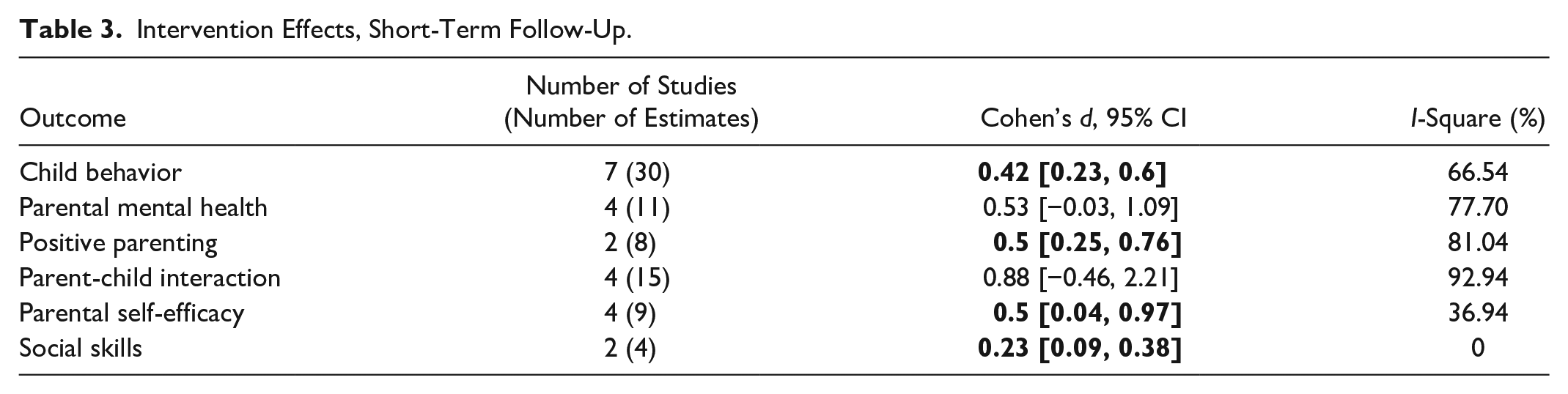
Only nine studies provided short-term follow-up data. The effects (Table 3) in child behaviors (d = 0.42, [0.23, 0.6], I2 = 66.54%; 7 studies, 30 estimates), positive parenting (d = 0.50, [0.25, 0.76], I2 = 81.04%; 2 studies, 8 estimates), parental self-efficacy (d = 0.50, [0.04, 0.97], I2 = 36.94%; 4 studies, 9 estimates), and child social skills (d = 0.23, [0.09, 0.38], I2 = 00.00%; 2 studies, 4 estimates) were maintained with generally consistent magnitudes (except for social skills, which became trivial), whereas the effects in parental mental health (d = 0.53, [−0.03, 1.09], I2 = 77.70%; 4 studies, 11 estimates) and parent–child interactions (d = 0.88, [−0.46, 2.21], I2 = 92.94%; 4 studies, 15 estimates) faded out. There were insufficient studies to conduct sensitivity analyses. All forest plots are in the Supplemental Appendices.
Intervention Effects, Short-Term Follow-Up.
Publication Bias
The funnel plots (Supplemental Appendices) were asymmetrical, with significant Egger’s coefficients for child behaviors (b = 0.18, p = .016) and positive parenting (b = 0.38, p = .008) but not parental mental health (b = 0.07, p = .685). Their asymmetry might stem from publication bias (where significant studies are more likely to be published than nonsignificant ones) or selective reporting (where researchers choose to report only certain significant results). Small study effects could also contribute to the asymmetry, as smaller studies with larger standard errors tend to report larger effect sizes and become published. Methodological differences, notably diverse measures in use, could also play a role in the asymmetry.
The trim-and-fill method imputed 15 hypothetical studies to the left side of the funnel plot for child behavior. The recalculated pooled effect size with imputed studies was generally consistent with the original estimate (d = 0.32, [0.21, 0.43]). For positive parenting, five hypothetical studies were imputed to the left of the funnel plot, yielding an effect size that is also similar to the main estimate (d = 0.49, [0.24, 0.73]). No hypothetical studies were imputed for parental mental health. These findings suggest that the observed effects remain robust after considering potential publication bias.
Subgroup Analyses and Meta-Regressions: Differences in Program Effects by Diagnosis
The meta-regressions (Table 4) showed that, compared to programs involving families of children with different developmental disabilities, programs solely including children with intellectual disability were more likely to reduce child behaviors (b = 0.95, [0.22, 1.67]) and those only involving autistic children were more likely to promote positive parenting (b = 1.21, [0.23, 2.19]). Programs targeting one diagnosis were not more effective than those including multiple diagnoses in terms of improving parental mental health. Sensitivity analyses produced highly consistent results (Supplemental Appendices).
Meta-Regression Coefficients and 95% Confidence Intervals.
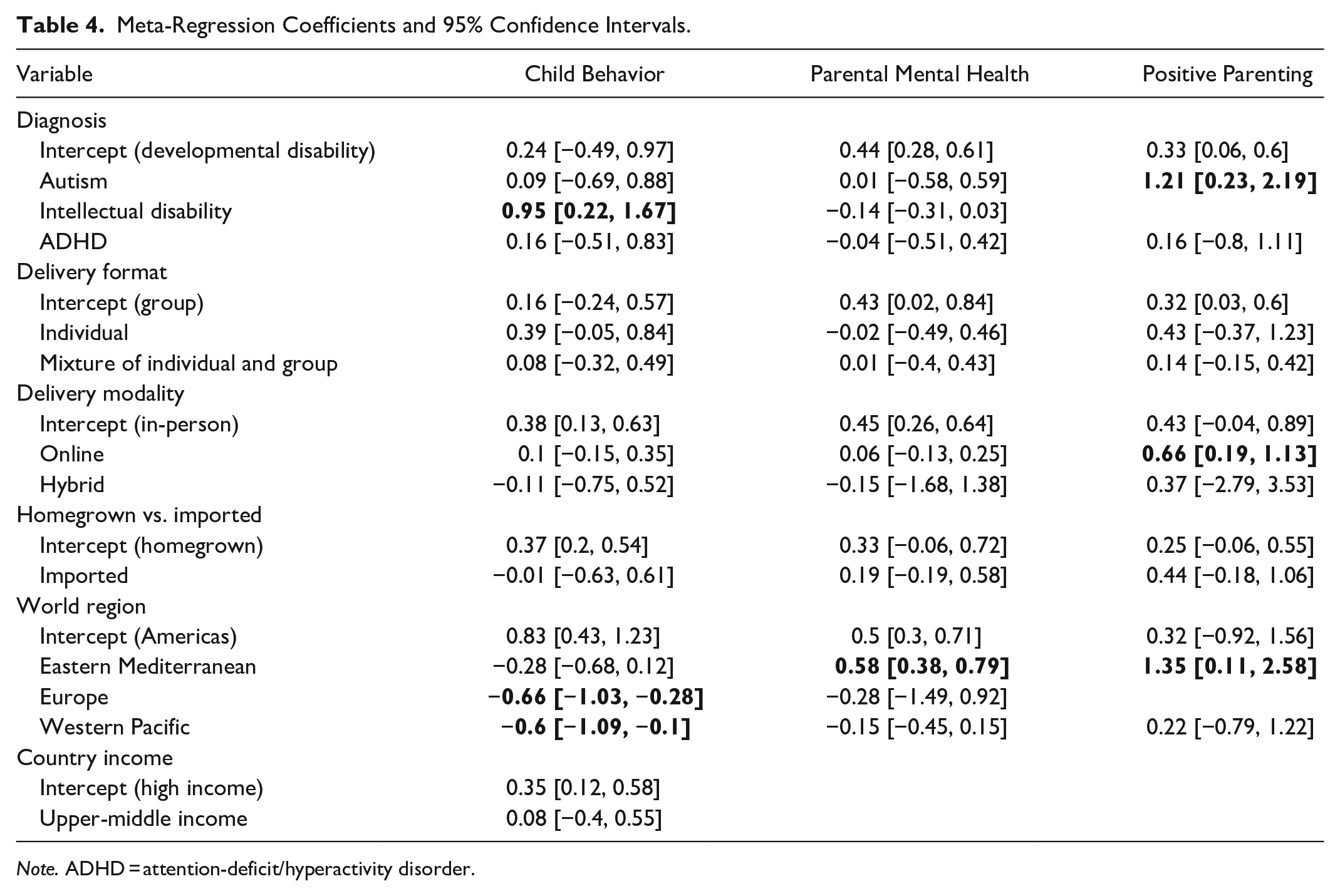
Note. ADHD = attention-deficit/hyperactivity disorder.
Subgroup Analyses and Meta-Regressions: Differences in Program Effects by Setting, Delivery Modality, and Program Origin
Regional differences were found in treatment effects. Compared to programs in Americas, those tested in Europe (b = −0.66, [−1.03, −0.28]) and Western Pacific (b = −0.60, [−1.09, −0.1]) had smaller effects in reducing child behaviors, while trials in Eastern Mediterranean were more likely to improve parental mental health (b = 0.58, [0.38, 0.79]) and positive parenting (b = 0.35, [0.11, 2.58]). Online delivery (b = 0.66, [0.19, 1.13]) was more likely to increase positive parenting than in-person and hybrid delivery. There were no significant differences in terms of delivery format, program origin, or country income level. Sensitivity analyses yielded consistent results (Supplemental Appendices), except that the effects of interventions delivered in the Western Pacific on child behavior were no longer distinguishable from those in the Americas or Eastern Mediterranean.
Discussion
Summary of Findings
This global systematic review is the first to assess the effectiveness of parenting interventions in reducing violence against children and promoting ECD for preschool children with developmental disabilities. In all, 33 RCTs with inactive control were identified, involving 2,752 families of children aged 2 to 7 years from 13 countries or regions (mostly high income) in four world regions. In all, 31 of the 33 studies provided data for the meta-analyses, with more studies reporting violence-related factors than child development outcomes and no studies reporting the actual occurrence of violence against children.
We found that, compared to inactive control at post-intervention, parenting programs reduced child behavioral problems (d = 0.36 [0.17, 0.56]), which is a major risk factor for violence against children. The effect was maintained in the sensitivity analysis (d = 0.34 [0.05, 0.64]), suggesting a high degree of certainty. Research indicates that Hedges’ g and Cohen’s d produce similar estimates (Lin & Aloe, 2021). Therefore, the effect size is consistent with Skotarczak and Lee (2015) (Hedges’ g = −0.39 [−0.15, −0.63]) involving children with developmental disabilities but weaker than Tellegen and Sanders (2013) (d = −0.54 [−0.37, −0.70]) and Fang, Barlow et al. (2022) (Hedges’ g = −1.37 [−2.03, −0.71]). However, Tellegen and Sanders (2013) included only Stepping Stones Triple P (SSTP) programs for children with developmental disabilities between 2 and 15 years old, and Fang et al. (2022) focused on parenting programs for children with developmental disabilities at all ages delivered in mainland China where there is a substantial service gap and potentially more space for change.
The results showed a small effect on improving parental mental health (d = 0.42 [0.21, 0.63]), which was generally maintained in the sensitivity analyses (d = 0.37 [0.2, 0.53]). This is in line with previous reviews involving children with developmental disabilities with broader age ranges (Singer et al., 2007: d = 0.29, unclear CI; Tellegen & Sanders, 2013: d = 0.26 [0.12, 0.41]) but stronger than a recent review on parenting interventions delivered for families of non-disabled children under three (Jeong et al., 2021), which detected no significant reduction in parental depression (standardized mean difference = −0.07 [−0.16, 0.02]). The reason can be twofold. First, caregivers of children with developmental disabilities experience higher levels of mental health problems than those of children without developmental disabilities, resulting in more potential for change (Scherer et al., 2019). Second, we had a broader definition of mental health problems, including not only depression but also stress and anxiety.
We found a medium effect on improving parenting practices (d = 0.54 [0.17, 0.91]), which is smaller than the review of SSTP (d = 0.73 [0.55, 0.90]) (Tellegen & Sanders, 2013) but stronger than two reviews of parenting programs for families of non-disabled infants and toddlers (Benzies et al., 2013; Jeong et al., 2021). The sensitivity analysis also suggested a high level of certainty (d = 0.55 [0.13, 0.97]). However, it should be noted that the SSTP review focused on the reduction of dysfunctional parenting (i.e., laxness, over-reactivity, and verbosity), whereas our review measured the increase in positive parenting.
We also detected a medium effect size in terms of improving parental self-efficacy (d = 0.56 [0.21, 0.91]), which is comparable to the SSTP review (d = 0.52 [0.32, 0.73]) and the review on infants without disabilities (d = 0.62), as well as an improvement in parent–child interaction (d = 0.89 [0.1, 1.68]), with an effect size larger than reviews on programs for Chinese families of children with developmental disabilities (g = 0.47 [0.21, 0.73]) (Fang, Barlow, et al., 2022) and young children without disabilities (Barlow et al., 2016: d = 0.48 [0.17, 0.79], focusing on group-based parenting interventions; Jeong et al., 2021: SMD = 0.39 [0.24, 0.53]). Nonetheless, our pooling was based on a very small number of studies (parental self-efficacy: n = 7; parent–child interaction: n = 8) and should be interpreted with caution.
With regard to other child developmental domains, the results showed small to medium effects in improving child language (d = 0.44 [0.07, 0.81]) and social skills (d = 0.51 [0.31, 0.72]), stronger than findings of reviews on non-disabled children under three (SMD = 0.23–0.35) (Britto et al., 2015; Geeraert et al., 2004; Jeong et al., 2021). No effect was found on the child’s motor, adaptive living, or cognitive skills, or diagnostic symptoms. However, caution is needed in interpreting the findings because none of the meta-analytic models included more than 10 studies, leading to limited statistical power.
The effects on child behaviors, positive parenting, parental self-efficacy, and social skills might have been maintained at short-term follow-up. A review of parenting interventions for families of non-disabled children also indicated sustained effects on child behaviors (van Aar et al., 2017). However, the evidence is much more limited in our review, given the small number of studies providing follow-up data. No studies provided long-term follow-up data.
Similar to Fang et al. (2022), we found that some treatment effects might vary by diagnosis. For instance, preliminary evidence suggested that programs for families of children with intellectual disabilities led to more significant improvements in child behaviors, whereas interventions focused on autistic children demonstrated a stronger impact on promoting positive parenting. However, this review also tended to show that programs involving multiple types of developmental disabilities may have effects that were comparable to those designed for a specific diagnosis (e.g., autism, ADHD, or intellectual disability). This might lend support to the delivery of parenting interventions that do not separate certain diagnoses from others and create a better sense of inclusivity.
Consistent with Fang et al. (2022) and another review on parenting interventions for families of non-disabled children (Leijten et al., 2016), we did not identify significant group differences in terms of homegrown versus imported programs. This supports the use of evidence-based parenting interventions across cultures. However, there was little reporting of local adaptations, limiting our understanding of the true extent of adaptations and their impacts on treatment effects. Our results were in line with Fang et al. (2022), finding no significant differences between different delivery formats, although some evidence favoring a combination of individual and group delivery was identified in two previous reviews on children with developmental disabilities (Skotarczak & Lee, 2015; Tellegen & Sanders, 2013), which had smaller sample sizes (n = 11–12) than our analyses (n = 12–24) and Fang et al. (2022, n = 23). We also found that digitalized parenting programs might be more likely to increase positive parenting practices than in-person or hybrid programs, potentially due to the benefits of digital delivery in promoting participant engagement and learning, which are indicated in a forthcoming systematic review on adaptations of parenting interventions during the COVID-19 pandemic (Fang, Martin, et al., n.d.).
We did not have enough studies in LMICs to test the impact of country income levels, but there were some differential effects by world regions, with interventions yielding stronger effects on child behaviors when delivered in the Americas and on parental mental health or positive parenting when delivered in Eastern Mediterranean. However, the meta-regressions were underpowered by the small number of studies and inconsistent reporting of program features and the results should be thus interpreted with caution.
Strengths and Limitations
This review has several strengths. Sensitive searches were conducted in a number of international and regional databases and gray literature repositories using both English and Chinese languages. Two studies reported in Chinese were included, and our analysis found no language-related biases that could have impacted the outcomes. We included only RCTs with inactive control to reduce heterogeneity and increase the precision of estimates. Effect sizes were pooled using robust variance estimation, a state-of-the-art method that allowed for the inclusion of multiple estimates from each study to enhance the power of analysis. We focused on preschool-aged children to further reduce heterogeneity and identified more observational measures than all previously published reviews on parenting interventions for families of children with developmental disabilities.
In all the studies where data were available, a diverse group of male and female preschoolers were included. Families participating in the studies represented a wide range of cultures from regions such as the Western Pacific, Americas, Europe, and Eastern Mediterranean, encompassing various ethnicities such as White, Asian, Black, Hispanic, and Arabic, as well as those of mixed heritage. Socioeconomic status data for families, where accessible, reflect a mix of different socioeconomic levels. This diversity underscores the potential applicability of parenting programs for families of children with developmental disabilities in a variety of contexts, encompassing both high- and low-resource settings, and spanning across different cultural backgrounds and ethnicities, mirroring the adaptability of parenting programs designed for the broader population.
A major limitation of this review is the small number of included studies, especially in developmental outcome domains (except child behaviors), which undermined the reliability and generalizability of the findings. There were also high levels of heterogeneity across multiple outcomes, likely stemming from the diverse cultural and socioeconomic backgrounds of participants, as well as variations in program delivery methods. Our ability to identify potential moderators was limited by the small number of studies and suboptimal reporting of key program and participant features (e.g., socioeconomic status). There was also limited reporting on the cultural and linguistic diversity among participants, which, in turn, limited our ability to evaluate their potential impact on the estimates.
Although we included only RCTs with inactive control, the risk of bias varied across studies and remained high or unknown in several domains. For instance, due to the lack of information, we were not able to assess the risk of bias pertaining to sequence generation, allocation concealment, missing data, and program developer involvement in multiple studies. Although there has been an increase in the use of observational measures compared to previous reviews, over half of the 327 estimates included were based on parent reports, which could be subject to social desirability and recall biases. In addition, the outcome measures utilized in the included studies exhibited considerable diversity. Furthermore, the psychometric properties, such as reliability and validity, of the outcome measures may vary across different populations and languages. However, it remains uncertain whether all of the measures were validated in local languages and specifically among disabled children and their families. Such variability could potentially contribute to increased heterogeneity and influence the precision of the estimates.
Only 9 of the 33 studies provided follow-up data and no studies assessed long-term effects, limiting our understanding of program impacts on violence against children beyond the immediate post-intervention time point. Moreover, only five studies were conducted outside of high-income countries/regions, which restricts the extent to which the findings can be generalized to LMICs. It is also noteworthy that no studies originated from South-East Asia or Africa. However, these regions exhibit some of the highest rates of developmental disabilities, potential loss of developmental capabilities due to stunting and poverty, and prevalence of violence on a global scale (Lu et al., 2016; UNICEF, 2020). Furthermore, the review only identified four specific types of developmental disabilities, so the findings might not be as applicable to other diagnoses. Male caregivers were also underrepresented in the studies. Last, due to resource constraints, we were not able to conduct searches in other widely used languages, such as Russian or Spanish.
Implications
Children with developmental disabilities and their families have been experiencing inequities in accessing quality support. Such exclusion results in great risks of violence against children and further limitations in opportunities for child learning and development. Early childhood is a critical time for children to receive the necessary care and protection they need, with responsive parenting being a central pillar of providing this care and protection (WHO, UNICEF, & World Bank Group, 2018). This review has confirmed that parenting interventions are an important strategy for preventing violence against children, by targeting factors associated with violence within families of young children with developmental disabilities, particularly those with attention deficit hyperactivity disorder, autism, intellectual disability, and language disorders. These interventions also hold promise in fostering language and social skills among these children.
Policymakers and practitioners should consider tailoring parenting interventions to the unique needs of families of children with developmental disabilities. This may include the integration of disability-specific content and strategies to ensure that interventions are accessible and relevant to these families. There needs to be close partnerships with communities to ensure that interventions are consistent with cultural norms and values and actively address stigma and stereotypes around disability to promote better participation and acceptance. In addition, fostering partnerships across various sectors (e.g., health, education, and social service) is essential to address the multiple risks to child protection and development that children with disabilities and their families face.
The complex needs of children with developmental disabilities, coupled with limited access to support and social marginalization, have imposed considerable strain on their families. This heightened stress contributes to an increased susceptibility to adversities. Consequently, there is a compelling need for parenting interventions that address caregiver mental health and well-being as well (Fang, Lachman et al., 2022). We advocate for more implementation of evidence-based parenting interventions for children with developmental disabilities in LMICs or resource-limited settings. Policymakers should also prioritize initiatives that reach these underserved populations. We also advocate for government leadership to institutionalize and scale-up interventions that have already shown positive effects in local settings, irrespective of program origin. Future delivery may also make use of digital modalities to increase program reach while maintaining program effects.
This review underscores the need for further research with larger sample sizes to measure the effects of parenting programs in reducing the actual incidence of violence against children with disabilities, providing more direct evidence of the impact of parenting interventions on violence reduction. In addition, there is a need for more studies to evaluate the effects of parenting programs on more developmental domains, such as cognitive skills, motor skills, and adaptive living. Future research can also investigate how treatment effects may vary between programs designed for a specific diagnosis, those delivered to multiple types of diagnoses, and programs that mainstream disabilities within general parenting supports, which are theorized to reduce social isolation and thus parental mental health problems. There is a need for more rigorous RCTs to minimize the risk of bias and better trial reporting to increase transparency. Formative research conducted using a participatory approach in collaboration with local stakeholders is equally important, especially in terms of understanding the diversity of contextual and cultural preferences in providing and receiving disability-inclusive parenting support. There needs to be more programs that are embedded within existing systems of service delivery to reach the most underserved populations. Future studies should also collect more long-term follow-up data to understand the incidence and risks of violence against children, along with child development, extending beyond the research timeframe. In addition, investigating the impacts of digital parenting programs remains an essential avenue for exploration. We also call for increased diversity in study participants and more comprehensive reporting of both participant and contextual characteristics. For example, there is an urgent need for more studies among families of children residing in LMICs to address the gaps in evidence, particularly in Southeast Asia and Africa. In addition, there can be more studies focusing on other types of developmental disabilities, such as learning disorders or cerebral palsy, and involving more male caregivers.
Summary of Findings Tables
Supplemental Material
sj-docx-1-tva-10.1177_15248380231207965 – Supplemental material for Parenting Interventions That Promote Child Protection and Development for Preschool-Age Children with Developmental Disabilities: A Global Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-tva-10.1177_15248380231207965 for Parenting Interventions That Promote Child Protection and Development for Preschool-Age Children with Developmental Disabilities: A Global Systematic Review and Meta-Analysis by Zuyi Fang, Xinran Liu, Cheng Zhang, Jamie M. Lachman and Dongping Qiao in Trauma, Violence, & Abuse
Supplemental Material
sj-docx-2-tva-10.1177_15248380231207965 – Supplemental material for Parenting Interventions That Promote Child Protection and Development for Preschool-Age Children with Developmental Disabilities: A Global Systematic Review and Meta-Analysis
Supplemental material, sj-docx-2-tva-10.1177_15248380231207965 for Parenting Interventions That Promote Child Protection and Development for Preschool-Age Children with Developmental Disabilities: A Global Systematic Review and Meta-Analysis by Zuyi Fang, Xinran Liu, Cheng Zhang, Jamie M. Lachman and Dongping Qiao in Trauma, Violence, & Abuse
Footnotes
Data availability
All data and analysis code will be made available upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is part of the Global Parenting Initiative, which is funded by The LEGO Foundation, Oak Foundation, the World Childhood Foundation, The Human Safety Net, and the UK Research and Innovation Global Challenges Research Fund (ES/S008101/1).
The review was pre-registered with PROSPERO (CRD42022320519).
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.