
Abstract
At the front line of our medical system and population health, emergency medicine (EM) settings serve as a commonly perceived place for safety. Survivors of intimate partner violence (IPV) may present to the emergency department (ED) with injuries, illness, or specifically to seek help for IPV. In 2018, the U.S. Preventive Services Task Force (USPSTF) recommended screening women of reproductive age for IPV across all healthcare settings. Our objective was to examine the application of IPV interventions, resource allocation, and persistent barriers for screening within the EM setting following the USPSTF recommendation. This scoping review follows the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocols (PRISMA-P). Our initial search of two major databases, PubMed and CINAHL, found 259 articles. After screening for inclusion and exclusion criteria, 15 articles met the full study criteria. Inconsistencies in screening women for IPV in EM are still prevalent. No study used the same validated IPV screening tool and four did not specify the tool. Significant barriers to screening included time constraints, patient acuity, language barriers, staff education, and inability to connect patients to resources. There is a need for more consistent IPV screening in the EM setting, which may include the development of a standardized, inclusive screening tool, as well as additional research and sharing of best practices. Advancement of IPV identification must go beyond a recommendation with greater awareness and education changes at all levels: personal, institutional, and policy.
Keywords
Introduction
Intimate partner violence (IPV), commonly referred to as domestic violence (DV), is defined by the World Health Organization (WHO) as violence or behaviors perpetrated by a former or current partner, inclusive of physical, sexual, or psychological harm including acts of physical aggression, sexual coercion, psychological abuse, and controlling behaviors (WHO, 2012). As a longstanding societal phenomenon across the globe, IPV has been documented to have profound, damaging impacts on health (Potter et al., 2021). Despite the international community’s acknowledgment of this problem as set out in the 1993 Declaration on the Elimination of Violence Against Women, a 2010 global health data analysis found that approximately 30% of women aged 15 and older have experienced IPV in their lifetime (Devries et al., 2013). More recently, in the United States, the prevalence of IPV has been found to range from 27.8% to 45.3% for women and 18.5% to 38.6% for men (Willie & Kershaw, 2019).
Across all subtypes, whether physical, psychological, or emotional abuse, IPV is associated with poorer self-reported physical and mental health and remains a significant risk to a woman’s burden of disease and injury (Potter et al., 2021; Vos et al., 2006). Yet IPV can remain undetected if there are no structural avenues to address its existence and no opportunity is provided for disclosure. Screening is essential for the detection of violence and provides survivors with help-seeking opportunities to procure resources and assistance from housing, medical, legal, or community advocate services.
Historically, there has been advocacy for improved targeted screening for IPV in healthcare settings, as well as advocating for universal screening measures (Poirer, 1997). However, rates of IPV disclosure and use of screeners may differ from one hospital setting to another due to the severity of a patient’s condition, the primary complaint, a clinician’s preconceived conceptions of a “typical battered woman” profile, or even the time of presentation to an emergency department (ED) or clinic (Larkin et al., 1999). In the United States, chart reviews and self-reported analysis studies have consistently found low, inadequate screening rates for IPV, while often only occurring in primary care settings (Klap et al., 2007; Perone et al., 2022). The geographical location and type of healthcare setting can also influence the likelihood of screening and the availability of resources (Adjognon et al., 2023; Agronsky et al., 2023; Davidov et al., 2023). In addition, there is still no national consensus on the most appropriate IPV screening instruments for distinct medical specialties and care settings.
For survivors presenting to the ED, IPV injuries or impacts can either be the primary reason for the visit or be a hidden experience within one’s home (Ernest & Weiss, 2002). EDs are often considered to be the loophole to universal care in the United States, acting not only as a guaranteed healthcare site, but also in many ways as a gateway for social services, which sees everyone regardless of insurance status, demographics, or citizenship status (Anderson et al., 2016; Gordon, 2000). At the interface of multiple systems, EDs act as the “safety net for the safety net,” treating the outcomes of longstanding structural violence while attempting to address the impact of social determinants of health (Gordon et al., 2001). Screening for IPV plays a significant role in evaluating a presenting patient’s health and safety. If IPV is properly identified, EDs can integrate successful referral systems that can connect victims with trained advocates, counselors, childcare, legal, and employment services (Ernest & Weiss, 2002). However, if there are no consistent screening protocols implemented, survivors will not receive the help and attention they may be seeking.
Guidelines and recommendations have failed to ensure hospital-based screening and resource allocation conventions for IPV survivors due to a lack of consensus on optimal protocol use in the ED (Anglin & Sachs, 2003). Many healthcare providers report that they lack confidence and knowledge on how to adequately screen for IPV in the ED and how to successfully refer women to support services (Heron & Kellermann, 2002). Less than 20 years ago, the 2004 U.S. Preventive Services Task Force (USPSTF) recommendation found insufficient evidence to support any specific screening recommendations for women presenting with and experiencing IPV, yet screening instruments were noted to be an accurate tool in identifying IPV with minimal adverse effects on most women (Nelson et al., 2012). In 2013, the WHO published guidelines for clinicians to ask about IPV exposure only when assessing conditions that may have been caused by IPV, while that same year, the USPSTF published contradictory recommendations, suggesting that women of childbearing age routinely be screened for IPV (Feder et al., 2013). The WHO guidelines mentioned training providers to perform proper screening but did not expand further.
The most up-to-date United States guidelines are the 2018 USPSTF Statement titled, “Screening for Intimate Partner Violence, Elder Abuse, and Abuse of Vulnerable Adults.” This statement provides a B-level recommendation for healthcare clinicians, across all settings, to screen for IPV in women of reproductive age and, if women do screen positive for experiencing IPV, to provide or refer them to support services. While this recommendation did acknowledge that available screening instruments can be used to identify IPV, there was no specific screener identified nor was there any additional detailed commentary about what kind of “support services” should be provided. The recommendation did note several effective screening instruments that accurately detect past-year IPV in adult women: Humiliation, Afraid, Rape, Kick (HARK); Hurt, Insult, Threaten, Scream (HITS); Extended-Hurt, Insult, Threaten, Scream (E-HITS); Partner Violence Screen (PVS); and Woman Abuse Screening Tool (WAST). Despite providing a range of tools, there was no conclusive commentary on which was the most appropriate to use or under what setting the implementation was most important (this recommendation predominantly noted primary care as a resource for IPV screening and data collection). Given the ambiguity of the 2018 USPSTF recommendations, further research is needed to guide the implementation of IPV screening in EDs.
Objective
The purpose of this scoping review is to provide a focused review of peer-reviewed literature on IPV screening in EDs published after the recommendation of the updated 2018 USPSTF Statement. We seek to identify whether the gap not addressed by the USPSTF recommendations regarding which screening tool to use in EDs and how to implement screening and referral programs has since been filled by relevant research.
The primary objective of this scoping review is to identify the prevalence, type of screener, and application of IPV screening for women in ED settings since 2018. Additionally, secondary objectives include (a) examining what barriers continue to exist for the implementation of IPV screening in emergency medicine (EM), and (b) identifying IPV survivor resources that are currently offered or are still needed.
Methods
This protocol was drafted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocols (PRISMA-P). Registration for this scoping review was not required.
Types of Sources and Search Strategy
We included only peer-reviewed articles published in English where the full text was available and excluded: theses, dissertations, editorials, and reviews. We searched both PubMed and CINAHL. We conducted the article searches in May of 2022. The search terms used for PubMed can be found in Appendix A and include terms for each concept pertinent to the research question, for example, setting (EDs), IPV, screeners, and interventions.
Article Selection
Inclusion criteria included the following: studies conducted in the United States, participants were at least 18 years or older, published in or after 2018, included an IPV screener(s) or resource referral, study setting was within the ED, and EM service/care utilization or outcomes for IPV were defined in the article’s primary outcomes. The target study population was identified as (a) women being screened for IPV or (b) EM clinicians. Studies with additional population demographics beyond our specific inclusion criteria were still included if the population of women experiencing IPV could be distinguished and analyzed in comparison to other groups. Reasons for exclusion included the incorrect population demographic (i.e., exclusively men, the elderly [ages >65], children/adolescents [ages<18]), and if the medical and/or healthcare settings did not solely focus on EM, such as primary care settings, urgent care centers, or general hospital visits.
Studies underwent abstract and full-text reviews for inclusion prior to data extraction. We used Covidence as a shared platform to track inclusion/exclusion and data extraction (Covidence Systematic Review Software, 2022). All four reviewers participated in each step of the article review process, two of whom have a strong background in IPV research and three having experience in emergency clinical care. The first step was study title and abstract screening, which was divided across the reviewers, with each study being reviewed by two team members. The second step was a full-text review, following the same reviewer format as step one. The final step was full-text extraction. During the study title and abstract screening, the researchers found it important to restrict the eligibility of studies to be included if they referenced retrospective chart reviews or studies that began before 2018. We added this refinement to the protocol to highlight the concentrated influence of policy and guidelines on clinical practice and referral programs. Data extraction/charting was performed in pairs by the four reviewers within the Covidence platform. Final consensus for an article was achieved through discussion between the two reviewers, and when necessary (and on rare occasions), the senior author made any final decisions if consensus was not mutually reached among the original reviewers. Inter-rater reliability was calculated using Cohen’s kappa. Cohen’s kappa was interpreted as having an average fair agreement [0.21–0.40] for the title and abstract review and moderate agreement [0.41–0.60] for the full-text review (McHugh, 2012).
Extraction and Synthesis
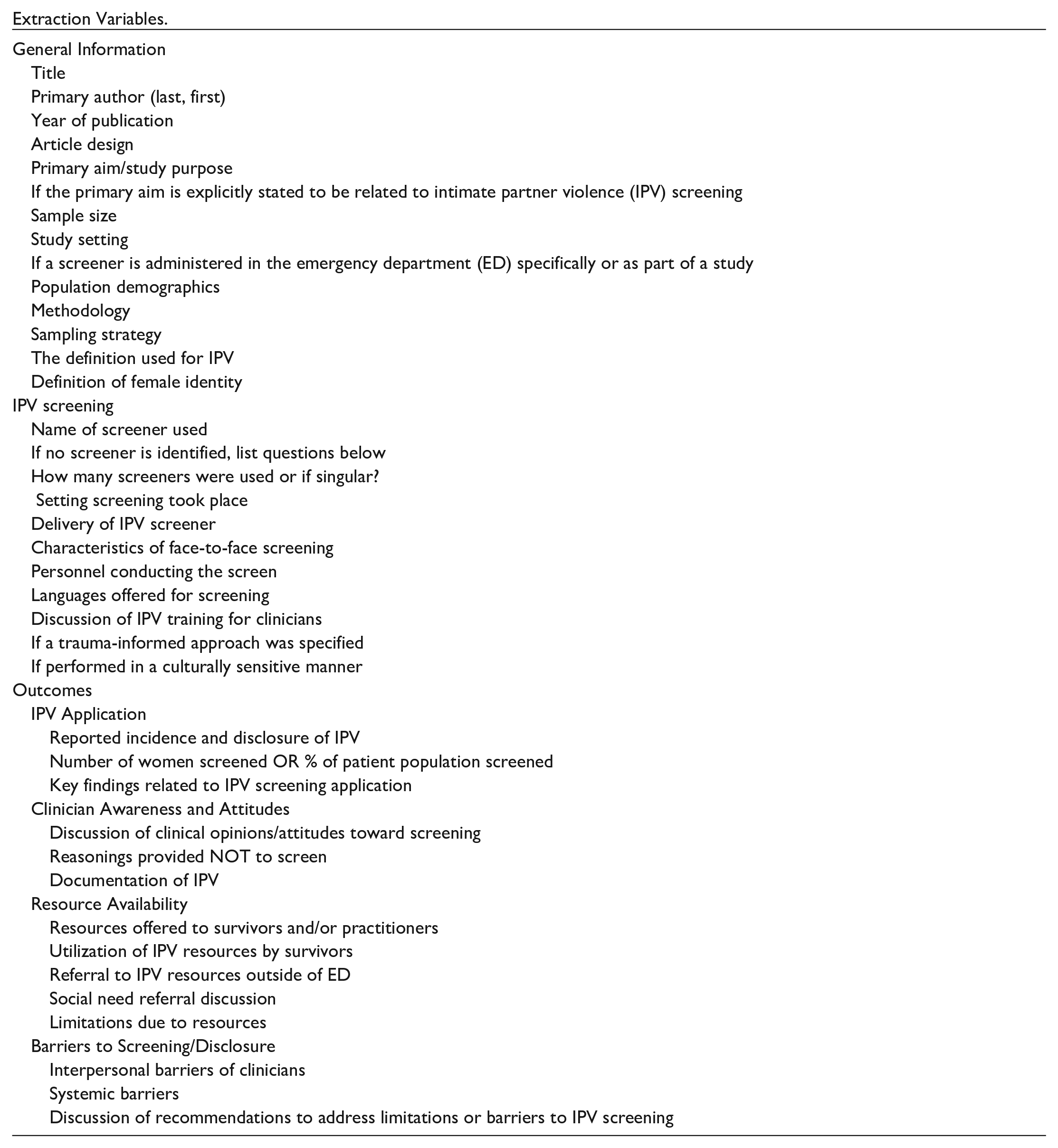
All the variables and themes included in the extraction form can be found in Appendix B. In the category “delivery of IPV screening intervention,” reviewers had the option to choose all that apply: person, computer/tablet, paper, audio/video. The authors decided to include the item “If performed in a culturally sensitive manner” under the criteria for IPV Screening to account for and acknowledge the researchers’ cultural relevance, contextuality, appropriateness, mutual respect, and flexibility with the study population. While this item was presumably subjective, the study authors noted the importance of including this variable as an appropriate measure to help determine the cultural knowledge or competency of the study, if any. If an article did not include a definition of IPV or made reference to an established definition of the term, it was assumed that the researchers used the definition identified by the screening tool within the study.
Extraction items were chosen based on the three main objectives of this review: IPV screening, survivor resources, and barriers for clinicians to screen and refer. Themes were analyzed based on the identification of this data, such as IPV prevalence, attitudes toward screening, systemic barriers to screening, and individual article recommendations. For articles that had missing data, two identifiers were used: (a) Unspecified if the articles did not clearly address the information, or (b) Not applicable if the information was not possible to extract given the study’s design or statistical analysis.
Results
Selection of Sources as Evidence
The search returned 259 articles for review. We removed 79 articles that were duplicates with an additional 132 articles excluded during the title and abstract screening. 48 articles remained for full-text review; 33 articles were further excluded in this stage, per inclusion and exclusion criteria. Ultimately, 15 articles met the study criteria for data extraction (Figure 1). Based on Covidence’s analysis software, title, and abstract inter-rater reliability between all four reviewers had a proportionate agreement ranging from 0.642 to 0.938, with Cohen’s kappa = 0.318 (95% confidence (CI) [−0.135, 0.683]), which corresponds with a fair agreement. The full-text review had a proportionate agreement ranging from 0.571 to 1.0, with Cohen’s kappa = 0.466 (95% CI [0.0, 1.0]), corresponding with a moderate agreement.
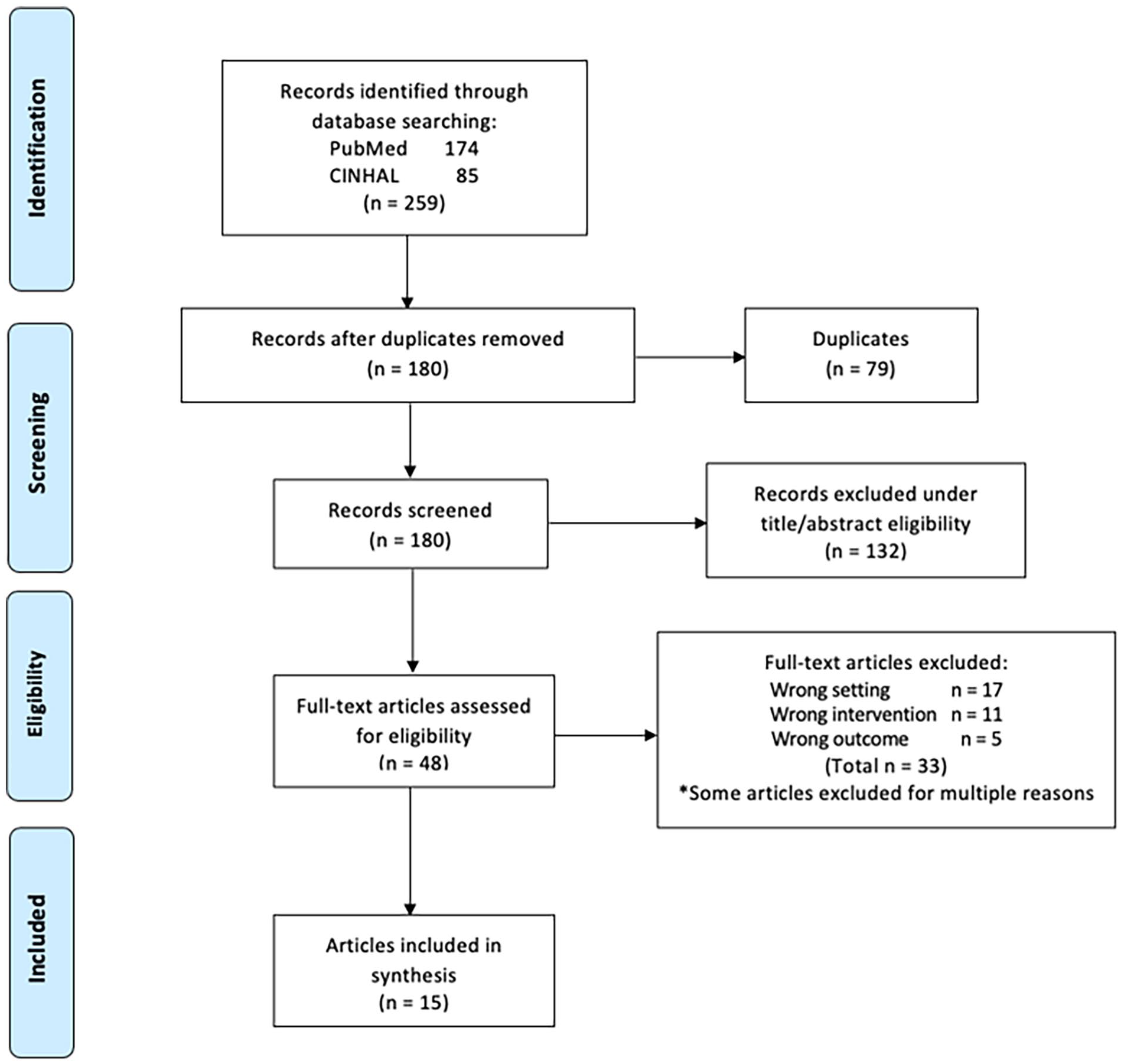
Flow diagram for article screening and data extraction.
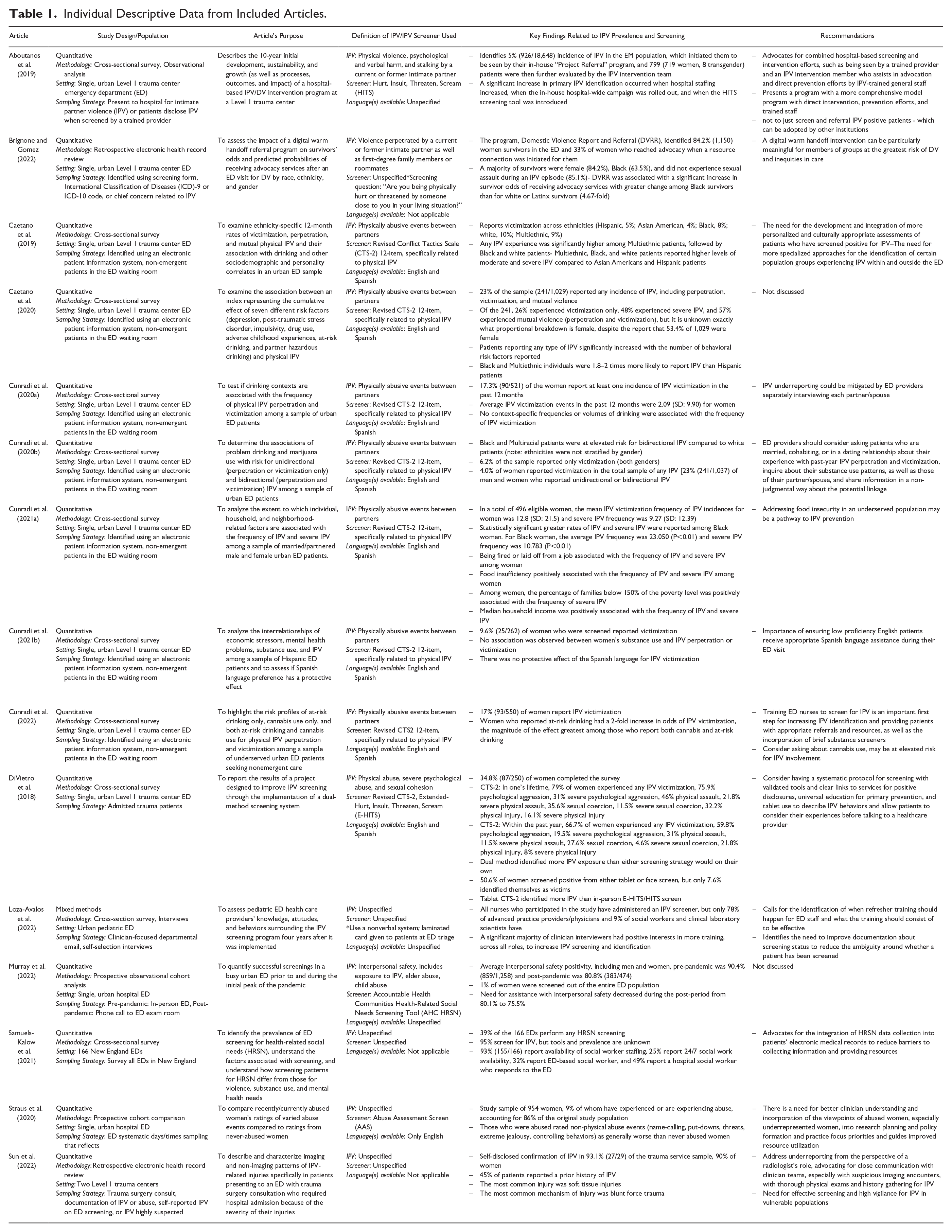
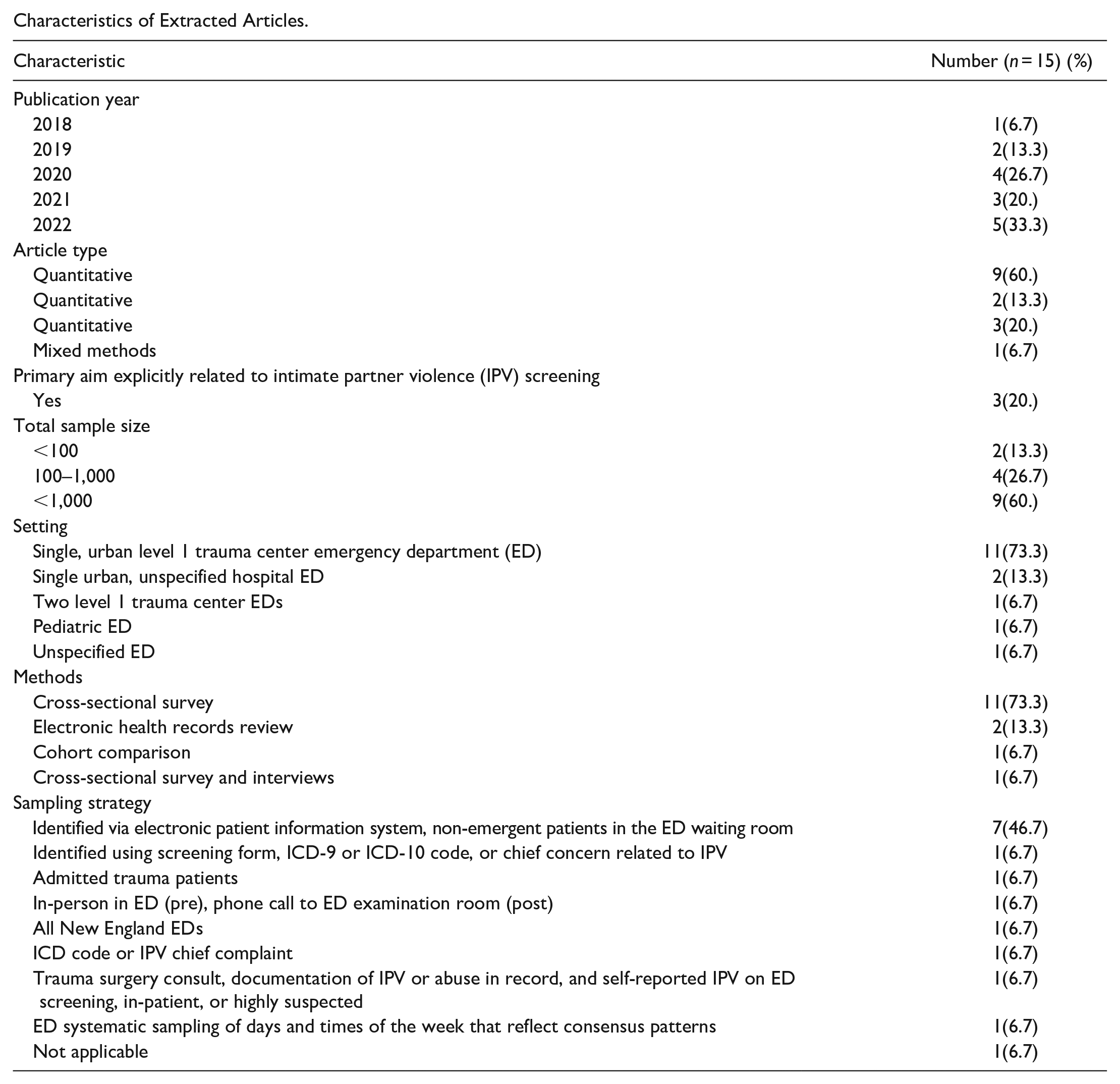
Out of the 15 final articles, 7 were cross-sectional surveys from a single, large-scale study (Caetano et al., 2019). All seven of these articles were included separately in the analysis of the characteristics as each article contributed differently to our main aims (Caetano et al., 2020; Cunradi et al., 2020a, 2020b, 2021a, 2021b, 2022). The other eight articles include quantitative and mixed-method study designs, including an observational analysis, cross-sectional surveys, retrospective electronic health records reviews, interviews, and cohort analyses. Appendix C includes an outline of the general extraction variables for all 15 articles and Table 1 describes the study design, setting, IPV definition used, IPV screener, key findings, and recommendations of each included article.
Individual Descriptive Data from Included Articles.
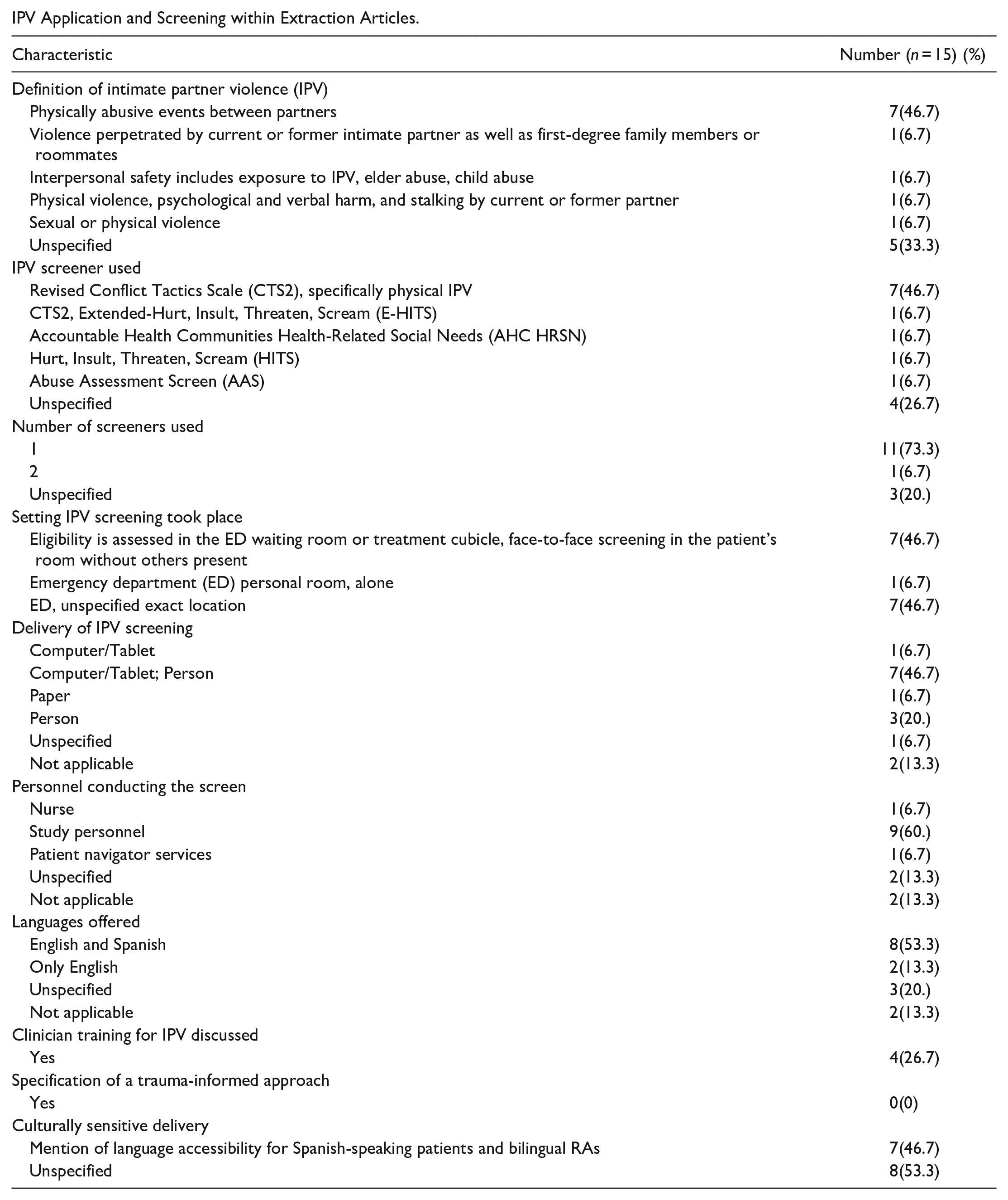
The definition of IPV and delivery of IPV screening varied across the articles (Appendix D). No two individual studies used the same definition of IPV, with the exclusion of the seven interrelated sub-analysis articles. Furthermore, only 20% of the articles had a primary aim explicitly related to IPV screening. The articles also varied in their definition of sex/gender. For the context of female identity, the seven interrelated sub-analysis articles coded gender as dichotomous (excluding three transgender patients), four articles mentioned self-reported gender, one article only included sex as a variable but not gender, and three did not specify how a patient’s sex or gender identity was derived. While Table 1 shows that eight articles had the option of Spanish or English IPV screening, this language inclusion is represented in only two broader studies (Caetano et al., 2019; DiVietro, 2018). Additionally, the seven interrelated articles are the only ones to touch on the topic of encompassing a culturally sensitive delivery, incorporating an aspect of language accessibility by the dual offering of languages and hiring bilingual research assistants, but there is no other information given beyond this description. No studies indicated the use of a trauma-informed approach when screening.
Screening Tools and Questions
The application of IPV screening tools and identification questions also varied throughout all the articles. The validated screening tools used were AAS, HITS, E-HITS, CTS-2, and the AHC health-related social needs (HRSN); three articles were missing screener information. Out of the 15 articles, 8 articles used the Revised CTS-2 (including the 7 sub-analysis articles) which is specifically designed for physical IPV. Each of the remaining validated tools listed was used in one of the remaining articles.
Several articles used screening questions based on non-validated measurement tools. Brignone and Gomez (2022) included the question for IPV incidence: “Are you being physically hurt or threatened by someone close to you in your living situation?.” DiVietro (2018) utilized the Revised CTS-2 and E-HITS screener but also noted that 6 months into the study, the hospital’s EMR system added mandatory abuse screening questions for the ED which included: “Do you feel that you are treated well? What happens when you argue or fight? Are you or have you been threatened? Has anyone ever threatened to hurt you? Does anyone try to keep you from having/contacting friends or doing things outside the home? Do you feel unsafe going back to your home?.” These additional questions were study-specific, and no specific screener was cited as their origin.
Information for in-person/face-to-face IPV screening was limited given the small number of articles that utilize in-person screener delivery. Within the seven sub-analysis articles, the face-to-face screening approach and script used are detailed as follows: “The next section concerns resolving couple conflict. No matter how well a couple gets along, there are times when they disagree, get annoyed with the other person, want different things from each other, or just have spats or fights because they are in a bad mood, are tired, or for some other reason. Couples also have many ways of trying to settle their differences. Please tell me how many times in the past 12 months your spouse or partner did each of these things to you, and how many times you did them to your spouse or partner. . .” (Cunradi et al., 2020b). DiVietro (2018) also noted that at the end of each study screening, the research associate would always offer the option for the patient to speak with a member of the social work team regardless of the patient’s IPV status. For the non-validated measurement tools, the delivery of screening questions was most often administered by an individual (study personnel or hospital staff) or self-reported through a computer/tablet system.
IPV Prevalence
The methods for the analysis of the incidence of IPV types (victimization, perpetration, and mutual) and the percentage of the population experiencing IPV varied depending on the article’s purpose and the methodology by which the authors reported the results. For six of the articles, the IPV victimization and incidence rates could not be broken down by gender, even when the number of women in the study was included. Disclosure of positive IPV identification across all articles for women ranged from 4.0% to 84.2% depending on the chosen study sample demographics, size, and methodological approach. The only study that asked participants whether they identified as “victims” themselves was DiVietro (2018), and they reported a 7.6% response among all participants without specifying statistics specific to gender.
Emergency Clinicians and IPV Screening
Only one article (Loza-Avalos, 2022) focused on clinicians’ feelings or attitudes toward IPV screening. Findings from Loza-Avalos (2022) indicated that most providers who voluntarily participated in the study felt that screening should occur whenever possible. However, many advanced practice providers/physicians indicated discomfort with performing the screening due to a lack of training and knowledge about both IPV screening and proper referrals. Overall, the entire ED staffing community in this survey favored registered nurses (RNs) performing the screening, including the RNs themselves. This study also identified four main reasons that providers gave to not screen: patient acuity, the presence of multiple caregivers, language barrier, and ongoing medical assessment. Of note, in Brignone and Gomez (2022) providers were significantly less likely to administer the IPV intervention that directly connected patients to referral services for patients experiencing sexual assault but did not explore further the reasons behind this disparity.
The consequence of human bias about IPV is acknowledged in multiple articles. Brignone and Gomez (2022) discussed how provider bias in IPV screening and delivery may also involve stereotyping and dismissiveness of experiences, especially among racial and ethnic minorities. Similarly, Loza-Avalos (2022) indicated that a few providers in the study reported subconscious biases that influenced who they chose to screen for IPV/DV. DiVietro (2018) noted that the EMR mandatory screening questions identified significantly less IPV than the dual method, which included both face-to-face screening using HITS and a tablet-based self-administered screening using CTS-2. This was potentially the nature of how the questions were asked, with the clinician looking at the computer screen, thus discouraging disclosure of a sensitive topic. Straus (2020) ultimately argued that clinicians may also tend to lean toward a “never abused” women perspective when screening, which underestimates the harm of non-physical assaults of IPV, including emotional and psychological abuse.
Systemic Barriers
The issue of systemic barriers to IPV screening is sparingly discussed. Cunradi et al. (2020a, 2021a) identified the systemic barrier of time constraints as contributing to the lack of data concerning psychological abuse, injury, and sexual coercion among patients. Similarly, Samuels-Kalow (2021) highlighted that busy, high-acuity, high-need EDs may reduce screening due to time and priority constraints, which would thereby reduce the use of appropriate interventions. Sun et al. (2023) discussed the significant underreporting of IPV in the trauma registry due to poor patient disclosure and underdiagnosis by clinicians, which is further amplified among non-white or non-English-speaking patients who are more likely to encounter barriers to healthcare access, are less inclined to present at a hospital or may not feel comfortable disclosing IPV to law enforcement or social workers. Recommendations to address these issues include improving clinician training, incorporating behavior questions regarding related IPV risk factors into screening protocols, developing more personalized and culturally appropriate measures, and increasing proper documentation/education for both the providers and patients.
Survivor Resources
Five of the 15 articles discussed social needs referrals, including social work, community referrals, food security resources, and counseling. Four articles indicated that resources or referrals were offered to the survivors who disclosed an IPV experience, two of which had referrals to resources outside of the ED. One article (Samuels-Kalow, 2021) indicated that the application of HRSN screening was limited because of the restricted availability of social workers in the ED.
Aboutanos et al. (2019) had a significant focus on referrals and resources for survivors. These referrals included resources outside of the ED but also prioritized connecting patients with resources within the hospital. The types of services that were provided to IPV patients included educational materials (i.e., information packet on IPV, education on IPV and sexual violence), mental health (i.e., in-house and community counseling/case management, and private counseling), legal support (i.e., victim witness, court accompaniment for protective orders, and police involvement), community programs (i.e., PERK, community referrals, and Virginia Victims Fund), safety planning (i.e., crisis intervention, hotline referral, and Fear to Freedom kit), and social service resources (i.e., shelter, transportation, and Victim Crisis Fund). Brignone and Gomez (2022) had an automated referral process to a local DV agency, of which 32.7% of women who screened positive were connected to services. DiVietro (2018) had the option for patients to speak with the social work team at the end of the study.
Discussion
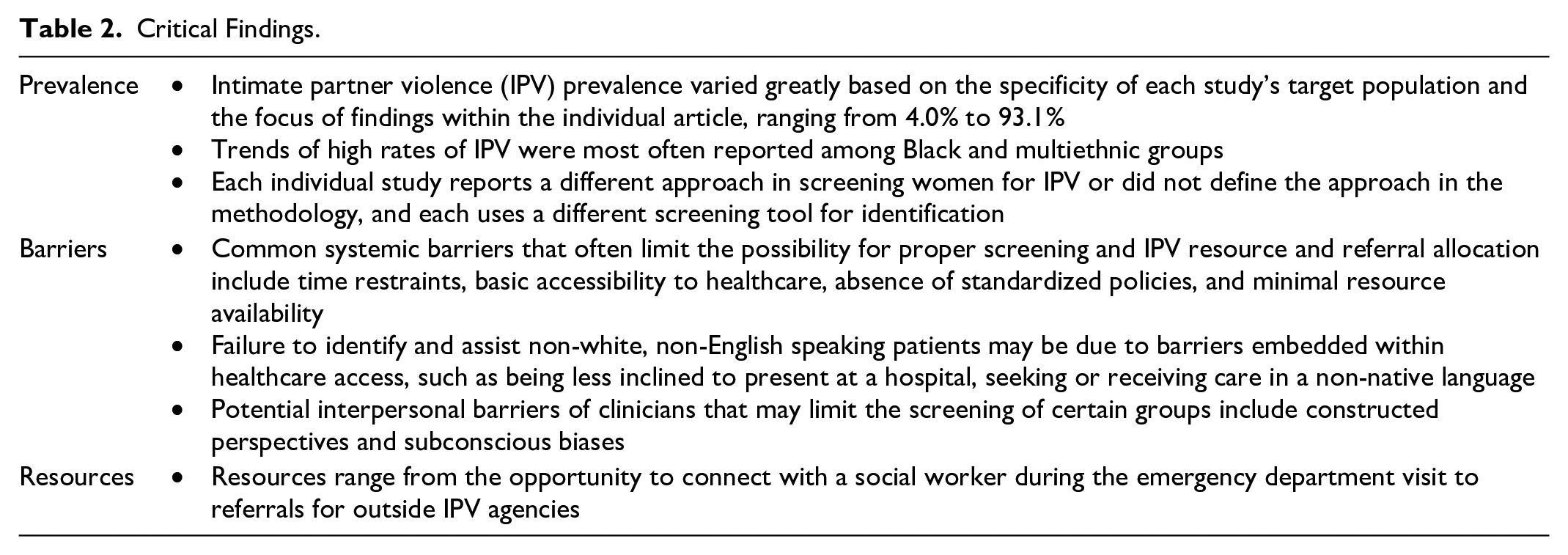
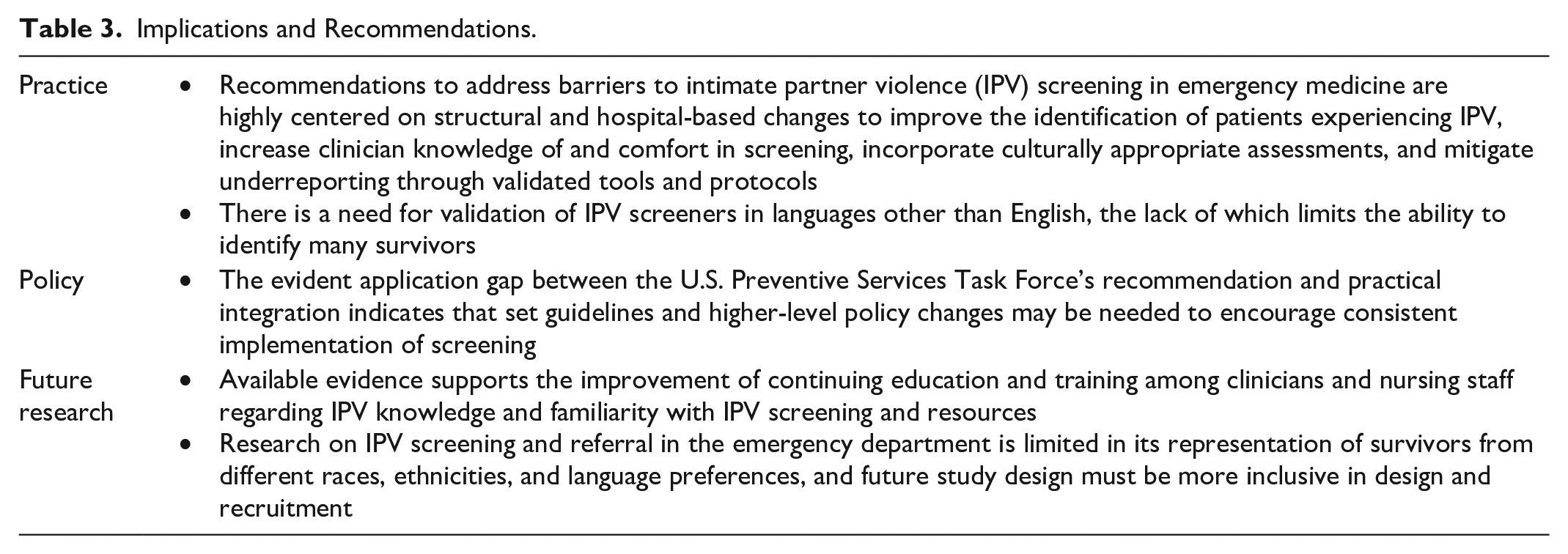
The 2018 USPSTF recommendation encouraging all healthcare providers to screen for IPV among women of reproductive age was intended to improve and guide IPV screening in clinical settings. However, due to the great ambiguity of this statement, this has not come to fruition. In our review focused on identifying the latest research trends or changes for IPV screening in the field of EM, we found limited literature on this subject. The 15 publications assessed, representing eight independent studies and seven articles that utilized the same data source for analysis, show limited progress in IPV screening standardization. The variation in the articles’ methodologies, key findings around IPV prevalence, and how EM systems are currently designed to screen for IPV reinforces that this issue still faces great barriers in practice, policy, and inclusivity (Tables 2 and 3).
Critical Findings.
Implications and Recommendations.
The USPSTF recommendation was a step forward for the formalization of screening practices and resource management; however, the lack of evidence and investigative literature creates challenges for measurable change and impact. This statement offers five different validated screening tools for healthcare utilization (HARK, HITS, E-HITS, PVS, and WAST), but that variance alone fosters vague guidance for sensitivity and specificity. Only two out of the eight independent studies used one of the aforementioned screening tools. Additionally, in Caetano et al. (2019), the researchers use a revised version of an unmentioned screener (CTS-2), which only examines physical IPV, thus discounting and arguably minimizing the identification of other domains/types of violence that a survivor may be experiencing.
Inconsistent definitions of IPV across the studies included in this review may hinder researchers’ ability to compare IPV screening tools across populations and settings, limiting our ability to improve future screening tools and provide recommendations for improving implementation. Given the diversity of EM settings and the populations they serve, we believe further discussion to support the recommendation of a single standardized, inclusive IPV screening tool is warranted. To ensure inclusivity and cultural relevancy, this tool should be validated across diverse populations and multiple languages, and be adaptable to the variation of resource availability across different ED settings. We recognize that there are limitations that can occur with the use of a single standardized IPV screener, including potentially missing culturally specific understandings and experiences of violence. In addition, broader systemic barriers to screening and IPV resource and referral allocation include time restraints, accessibility to healthcare services, and minimal resource availability, which should be considered as part of the development of any future IPV screening tools. Clinical practices must also discuss the acceptable and responsible delivery of screeners in the ED, whether that be done through trained hospital staff or personnel, the option for self-reported mechanisms, or other technological means. To support the vision of the USPSTF recommendation, the use of a standardized IPV screening tool would allow for more consistency in reporting IPV prevalence and related outcomes, which in turn could provide stronger support for policies that affect both survivors and the healthcare system they access for care.
Beyond the IPV screening tool itself, many of the issues discussed around the barriers to screening survivors for IPV in EM are due to the provider’s lack of knowledge or confidence around the subject of DV. Furthermore, interpersonal barriers of clinicians, such as implicit biases, may influence the patients who are screened, and in turn, affect the inclusion of historically marginalized participants in research. A potential solution to this could be addressed through hospital-directed education protocols and module requirements for the ED clinical staff. Other notable constraints to screening include systemic barriers within the ED, limitations of the broader medical system, or underlying social issues that present in ED environments. Recommendations for responses to these barriers within the studies reviewed seem to weigh toward restructuring individual hospitals’ delivery and response systems, including increased collaboration with administration and consistent implementation at all hospital levels. Such restructuring will require attention to the setting context (e.g., urban vs rural) and the necessary resources for implementation. Encouraging education and subject knowledge for EM practitioners and staff can also prompt a change in the clinical ED culture concerning IPV competency, the delivery of the screening, and overcoming barriers that may be unknowingly present in personal biases and systemic frameworks.
Finally, there is a need to address the lack of diversity in research participant inclusion, the paucity of IPV screening tools available in languages other than English, and the limited diversity of ED settings in the available research. There is evidence that specific population groups, often non-white or from marginalized communities, are at high risk of experiencing IPV (Dutton et al., 2000; Erez et al., 2009; Lee & Hadeed, 2009). Yet, there is a gap in research on IPV screening and referrals in the ED specific to historically marginalized groups, such as racial/ethnic minority and/or non-English language preference survivors. To address this gap, inclusivity in research must be a priority from study design through recruitment, analysis, and eventual implementation stages (Ruzycki & Ahmed, 2022). Furthermore, policy-level regulations, whether hospital-based or governmental, can assist in the progress of inclusive IPV screening. Solutions include the adoption of screeners that are offered in an assortment of languages, or by the funding of trained medical translators, either in-person or with technological assistance. Lastly, the majority of studies included in this review occurred in urban settings and/or in EDs in hospitals that are trauma centers. To better understand and characterize the experiences of IPV happening across our country, future research should examine IPV screening in a broader range of ED settings, which may include EDs in rural environments and community-based hospitals.
Limitations
The main limitation of this scoping review is primarily the number of included articles. The articles analyzed here represent only 5.8% (15/259) of the original article search pool. It is possible that excluded articles had information that could have been potentially beneficial to the study’s purpose but did not provide data in a form that allowed for clear extraction per the inclusion criteria. For instance, studies that examined IPV screening or prevalence in many sectors of healthcare, including EM, but did not provide distinct setting statistics were excluded because the data specific to the ED could not be isolated. There were also cases where the information or intervention took place too far back in time for the data to be reflective of the potential influence of the 2018 USPSTF. Another limitation is the publication time frame, as recent or current research in EM would not yet be available in the peer-reviewed literature. It is also critical to acknowledge that this review focused on women of reproductive age. The IPV survivor population also includes men, non-binary gender-conforming individuals, youth, and geriatric populations.
Conclusion
This scoping review gathers the most recent evidence on IPV screening in EM since the USPSTF 2018 recommendations. Clinically, there remains a need for ongoing emergency physician and nursing staff training concerning IPV screening as well as referral program development to address barriers such as time, provider confidence, and access to resources. Moreover, there is a large gap in practice and research regarding the incorporation of trauma-informed, culturally specific, and linguistically accessible screening. Our findings suggest that a strong, validated protocol for IPV screening accompanying a respected and established guideline is needed for communities to reduce under-screening and increase resource connections. The solution to identifying IPV in EM will need to be multi-faceted, inclusive of institutions, political administration, and hospital-based regulations, to ensure satisfactory screening, resources, and referrals so that every patient in need can be connected to services that can assist them through their healing and safety journey.
Footnotes
Appendix A
Appendix B
Extraction Variables.
| General Information |
| Title |
| Primary author (last, first) |
| Year of publication |
| Article design |
| Primary aim/study purpose |
| If the primary aim is explicitly stated to be related to intimate partner violence (IPV) screening |
| Sample size |
| Study setting |
| If a screener is administered in the emergency department (ED) specifically or as part of a study |
| Population demographics |
| Methodology |
| Sampling strategy |
| The definition used for IPV |
| Definition of female identity |
| IPV screening |
| Name of screener used |
| If no screener is identified, list questions below |
| How many screeners were used or if singular? |
| Setting screening took place |
| Delivery of IPV screener |
| Characteristics of face-to-face screening |
| Personnel conducting the screen |
| Languages offered for screening |
| Discussion of IPV training for clinicians |
| If a trauma-informed approach was specified |
| If performed in a culturally sensitive manner |
| Outcomes |
| IPV Application |
| Reported incidence and disclosure of IPV |
| Number of women screened OR % of patient population screened |
| Key findings related to IPV screening application |
| Clinician Awareness and Attitudes |
| Discussion of clinical opinions/attitudes toward screening |
| Reasonings provided NOT to screen |
| Documentation of IPV |
| Resource Availability |
| Resources offered to survivors and/or practitioners |
| Utilization of IPV resources by survivors |
| Referral to IPV resources outside of ED |
| Social need referral discussion |
| Limitations due to resources |
| Barriers to Screening/Disclosure |
| Interpersonal barriers of clinicians |
| Systemic barriers |
| Discussion of recommendations to address limitations or barriers to IPV screening |
Appendix C
Characteristics of Extracted Articles.
| Characteristic | Number (n = 15) (%) |
|---|---|
| Publication year | |
| 2018 | 1(6.7) |
| 2019 | 2(13.3) |
| 2020 | 4(26.7) |
| 2021 | 3(20.) |
| 2022 | 5(33.3) |
| Article type | |
| Quantitative | 9(60.) |
| Quantitative | 2(13.3) |
| Quantitative | 3(20.) |
| Mixed methods | 1(6.7) |
| Primary aim explicitly related to intimate partner violence (IPV) screening | |
| Yes | 3(20.) |
| Total sample size | |
| <100 | 2(13.3) |
| 100–1,000 | 4(26.7) |
| <1,000 | 9(60.) |
| Setting | |
| Single, urban level 1 trauma center emergency department (ED) | 11(73.3) |
| Single urban, unspecified hospital ED | 2(13.3) |
| Two level 1 trauma center EDs | 1(6.7) |
| Pediatric ED | 1(6.7) |
| Unspecified ED | 1(6.7) |
| Methods | |
| Cross-sectional survey | 11(73.3) |
| Electronic health records review | 2(13.3) |
| Cohort comparison | 1(6.7) |
| Cross-sectional survey and interviews | 1(6.7) |
| Sampling strategy | |
| Identified via electronic patient information system, non-emergent patients in the ED waiting room | 7(46.7) |
| Identified using screening form, ICD-9 or ICD-10 code, or chief concern related to IPV | 1(6.7) |
| Admitted trauma patients | 1(6.7) |
| In-person in ED (pre), phone call to ED examination room (post) | 1(6.7) |
| All New England EDs | 1(6.7) |
| ICD code or IPV chief complaint | 1(6.7) |
| Trauma surgery consult, documentation of IPV or abuse in record, and self-reported IPV on ED screening, in-patient, or highly suspected | 1(6.7) |
| ED systematic sampling of days and times of the week that reflect consensus patterns | 1(6.7) |
| Not applicable | 1(6.7) |
Appendix D
IPV Application and Screening within Extraction Articles.
| Characteristic | Number (n = 15) (%) |
|---|---|
| Definition of intimate partner violence (IPV) | |
| Physically abusive events between partners | 7(46.7) |
| Violence perpetrated by current or former intimate partner as well as first-degree family members or roommates | 1(6.7) |
| Interpersonal safety includes exposure to IPV, elder abuse, child abuse | 1(6.7) |
| Physical violence, psychological and verbal harm, and stalking by current or former partner | 1(6.7) |
| Sexual or physical violence | 1(6.7) |
| Unspecified | 5(33.3) |
| IPV screener used | |
| Revised Conflict Tactics Scale (CTS2), specifically physical IPV | 7(46.7) |
| CTS2, Extended-Hurt, Insult, Threaten, Scream (E-HITS) | 1(6.7) |
| Accountable Health Communities Health-Related Social Needs (AHC HRSN) | 1(6.7) |
| Hurt, Insult, Threaten, Scream (HITS) | 1(6.7) |
| Abuse Assessment Screen (AAS) | 1(6.7) |
| Unspecified | 4(26.7) |
| Number of screeners used | |
| 1 | 11(73.3) |
| 2 | 1(6.7) |
| Unspecified | 3(20.) |
| Setting IPV screening took place | |
| Eligibility is assessed in the ED waiting room or treatment cubicle, face-to-face screening in the patient’s room without others present | 7(46.7) |
| Emergency department (ED) personal room, alone | 1(6.7) |
| ED, unspecified exact location | 7(46.7) |
| Delivery of IPV screening | |
| Computer/Tablet | 1(6.7) |
| Computer/Tablet; Person | 7(46.7) |
| Paper | 1(6.7) |
| Person | 3(20.) |
| Unspecified | 1(6.7) |
| Not applicable | 2(13.3) |
| Personnel conducting the screen | |
| Nurse | 1(6.7) |
| Study personnel | 9(60.) |
| Patient navigator services | 1(6.7) |
| Unspecified | 2(13.3) |
| Not applicable | 2(13.3) |
| Languages offered | |
| English and Spanish | 8(53.3) |
| Only English | 2(13.3) |
| Unspecified | 3(20.) |
| Not applicable | 2(13.3) |
| Clinician training for IPV discussed | |
| Yes | 4(26.7) |
| Specification of a trauma-informed approach | |
| Yes | 0(0) |
| Culturally sensitive delivery | |
| Mention of language accessibility for Spanish-speaking patients and bilingual RAs | 7(46.7) |
| Unspecified | 8(53.3) |
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.