
Abstract
Emergency medical services (EMS) professionals are exposed to the trauma experienced by their patients regularly. This exposure to others’ traumatic experiences is known as vicarious trauma or indirect trauma. When it becomes problematic for the worker’s well-being, the resulting symptoms are referred to as vicarious traumatization or secondary traumatic stress. Existing literature highlights the importance of recognizing vicarious trauma and subsequent symptoms experienced by these professionals, as well impacts this may have on their workplaces. However, comprehensive reviews of vicarious traumatization among those involved in responding to prehospital emergency medical situations are limited. A four-phase Preferred Reporting Items for Systematic Reviews and Meta-Analyses selection process was employed to identify publications from 1995 to 2022 that considered the epidemiology of vicarious traumatization among EMS professionals. Trained reviewers screened articles based on inclusion criteria: (a) EMS professionals; (b) vicarious traumatization/related terms; and (c) analysis of epidemiological data on prevalence, risk/protective factors, or manifestations. Initially, 4,147 unique manuscripts were identified. After removing duplicates, one reviewer screened titles, and additional articles were identified through bibliography searches. Two reviewers independently screened abstracts, resolving disagreements during full-text screening, where a third reviewer settled any conflicts. A total of 31 articles were included in this review. Findings regarding the epidemiology of vicarious traumatization are summarized. The occupational hazard of vicarious/indirect trauma is unavoidable, but vicarious traumatization/secondary traumatic stress can be mitigated with improved workplace measures.
Keywords
Emergency medical services (EMS) professionals such as paramedics, other ambulance staff, firefighters, dispatchers, and other rescue workers bear witness to the traumatic experiences of others regularly in their work. For example, they often hear the stories of what happened to victims of violence or disasters during their everyday work or help in the aftermath of a mass casualty event. This occupational exposure to the traumatic experiences of others is commonly referred to as vicarious trauma or indirect trauma (Molnar et al., 2017). EMS personnel specifically are required to intervene regularly in horrific scenes that include loss of life, permanent disability, injury, and illness. These scenes may be human-made (domestic abuse, homicides, suicides, sexual assault or other violent crimes, nuclear explosions, motor vehicle crashes, terrorism, etc.) or they may be natural disasters (hurricanes, tornadoes, earthquakes, landslides, etc.) (Naushad et al., 2019), but no matter which one, the consistent long-term exposure to vicarious trauma can, without sufficient resources, lead to adverse effects on these professionals. Indirect trauma, as it is referred to in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), is considered a DSM-5 criterion A stressor for posttraumatic stress disorder (PTSD) (American Psychiatric Association, 2014).
A range of impacts from vicarious trauma are possible. Individuals who encounter vicarious trauma may experience neutral or positive outcomes including vicarious resilience, posttraumatic growth (PTG), and compassion satisfaction. Vicarious resilience is a process characterized by the positive effects on professionals from observing resiliency in those they are helping (Hernández et al., 2007). PTG goes beyond vicarious resilience, which refers to as stress-induced improvements in psychological functioning that exceed pre-traumatic states (Schubert et al., 2016). Lastly, compassion satisfaction is a sense of fulfillment and pleasure that professionals experience in their work of helping others (Figley & Stamm, 1996).
Conversely, individuals may experience negative outcomes or manifestations related to vicarious trauma that are collectively known as vicarious traumatization or secondary traumatic stress (Canfield, 2005; Mccann & Pearlman, 1990; Molnar et al., 2017; Pearlman & Saakvitne, 1995). Secondary traumatic stress, defined as “the natural and consequent behaviors and emotions resulting from knowing about a traumatizing event experienced by a significant other – the stress resulting from helping or wanting to help a traumatized or suffering person” (Figley, 1995, p. 7), will be used synonymously with vicarious traumatization in this systematic review. To understand the prevalence of vicarious traumatization/secondary traumatic stress (VT/STS) among employees, workplaces, as well as researchers, most commonly utilize the Secondary Traumatic Stress Scale (STSS) and/or Professional Quality of Life Scale (ProQOL), but other measurement scales are used as well (Molnar et al., 2017). Manifestations of VT/STS, or the way that having these symptoms look in terms of people’s behaviors or consequences, may include relationship problems, burnout, diagnoses of PTSD, unhealthy behaviors, and compassion fatigue among others (Figley, 2002; Molnar et al., 2020; Pines & Aronson, 1988). Because workers in professions exposed to vicarious trauma can also be diagnosed with PTSD, especially since the addition of indirect trauma to the qualifying events for DSM-V criteria, PTSD is another commonly used outcome that is measured to estimate the prevalence of VT/STS. Thus, studies that utilized PTSD specifically as a possible outcome of vicarious/indirect trauma among this population of workers will be included in this review.
Existing literature highlights the importance of recognizing vicarious trauma and subsequent outcomes experienced by EMS professionals and how their employing organizations are affected. However, comprehensive reviews of vicarious trauma among professionals involved in responding to prehospital emergency medical situations are limited. While a 2019 review article conducted by Greinacher, Derezza-Greeven, et al. (2019) examined the existing literature on vicarious traumatization among first responders, this review expands upon it, specifically focusing on prehospital EMS, and delving deeper into the prevalence, risk factors, and protective factors associated with VT/STS. Additionally, this review explores the literature on manifestations and interventions related to VT/STS. By comprehensively investigating these factors, this review enhances our understanding of what is known concerning professionals engaged in prehospital emergency work, while also identifying remaining gaps in the literature.
This is a systematic review of the literature on vicarious trauma and consequent outcomes in all professions working to help those who are experiencing a prehospital medical emergency, including dispatchers, firefighters (typically cross-trained as emergency medical responders or emergency medical technicians), emergency behavioral health workers, and disaster response workers. Studies included in the systematic review discuss the epidemiology of vicarious traumatization/secondary traumatic stress among these professionals, specifically (a) prevalence of VT/STS, (b) risk and protective factors for VT/STS, and (c) positive and negative impacts of experiencing vicarious trauma. The goals are to (a) summarize the epidemiologic research on prevalence, risk and protective factors, and associated effects on health and well-being; (b) analyze types and quality of methodologies and procedures employed in these studies; and (c) utilize this synthesis of this body of work to make recommendations for future research.
Methods
Information Sources and Search Strategy
Based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Page et al., 2021), a comprehensive systematic search was conducted across five prominent research databases: PsycArticle, Psychology and Behavioral Science Collection, PsycInfo, PTSDpub, and PubMed. The population of literature under study was predetermined through collaborative efforts between two authors, focusing on all medically focused first responders. Law enforcement workers were not included due to the uniqueness of the types of stress they are exposed to, such as the added direct trauma experiences of responding to criminal behaviors (Arble et al., 2018). The selection of disciplines for inclusion in the study was based on a previous systematic review on the subject of vicarious traumatization (Molnar et al., 2020). The search strategy was implemented with specific restrictions, including (a) articles available in English, (b) publications published between January 1995 (chosen because it was the year Figley, 1995 first defined secondary traumatic stress) and December 2022, and (c) articles that underwent peer review. To maintain the focus on peer-reviewed research publications, it was decided that books, book chapters, book reviews, dissertations, and theses would be excluded from the search. The database search was meticulously carried out to identify relevant research publications encompassing the field of prehospital EMS and topics related to vicarious trauma. The search terms included disciplines within the prehospital EMS domain (list available in Appendix A), combined with keywords related to vicarious trauma or related terminologies (list available in Appendix A). The selection of search items was based on a prior literature review conducted by the two of the authors (Molnar et al., 2020) to ensure the relevance and comprehensiveness of the search strategy.
Inclusion Criteria
Studies discovered in the database searches noted above were considered for inclusion in this systematic review if they met the following inclusion criteria: (a) a sample including at least 50% emergency medical professionals (unless a study included a sample clearly broken down by profession where the results for EMS were clear), (b) empirical research studying vicarious trauma/indirect trauma or vicarious traumatization/secondary traumatic stress; and (c) analysis of the epidemiology of vicarious traumatization/secondary traumatic stress, including prevalence, risk and protective factors, or manifestations.
Study Selection and Data Extraction
Research publications were selected to be included in the systematic review following the PRISMA Statement protocol (Figure 1) (Liberati et al., 2009). Two authors extracted the articles from the electronic databases. Once duplicate articles were removed from the electronic search results, a single reviewer screened the articles based on the title. Additionally, articles were identified by hand-searching bibliographies of all included articles. Two reviewers asynchronously screened the abstracts of the articles. The two reviewers compared their decisions: all disagreements were left to the full-text screening stage. The full-text screening process was conducted by the same two reviewers. In cases of disagreement, a third reviewer (the senior author of the article) independently screened the full-text using the same criteria to reach a final decision.
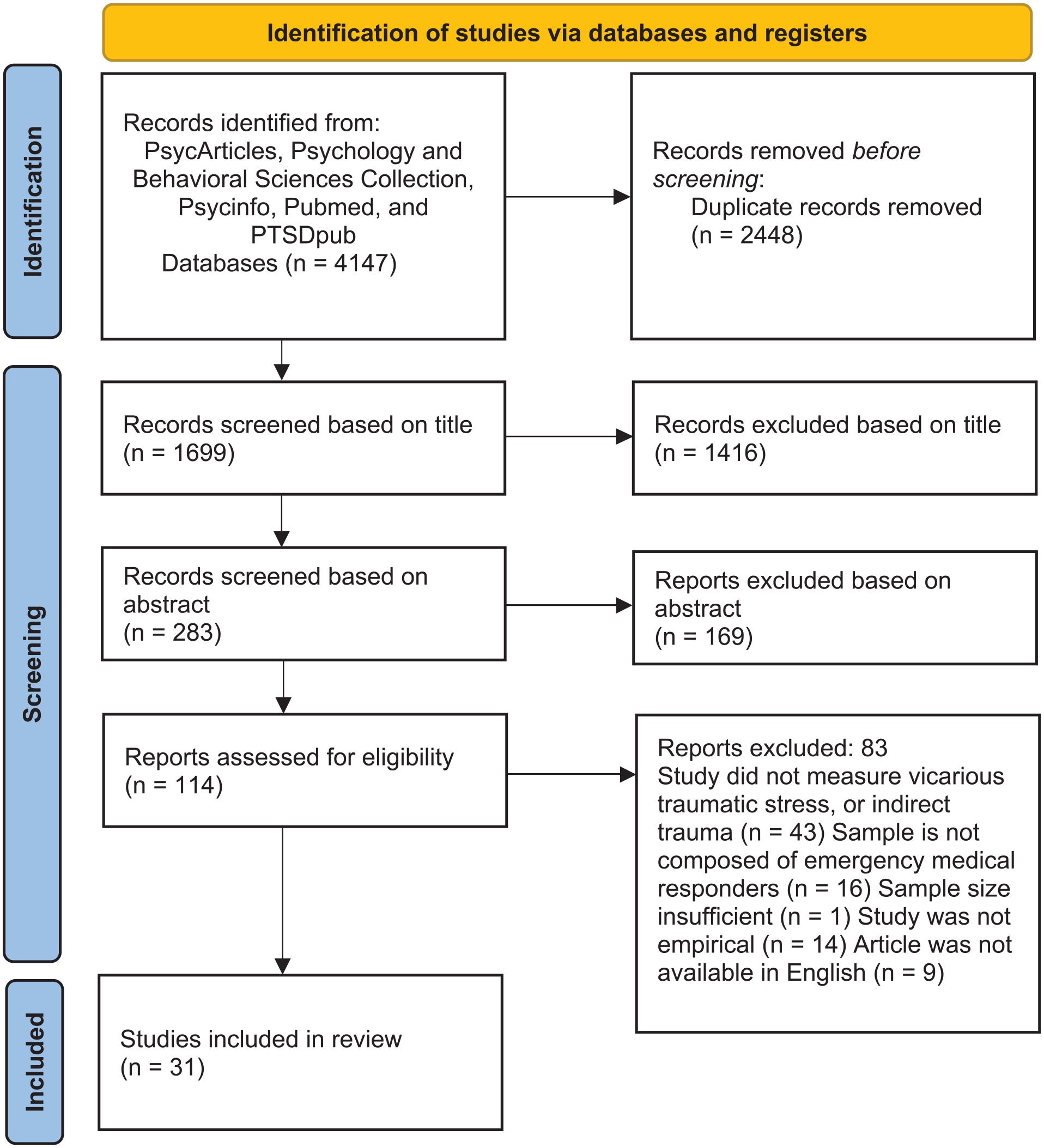
Results of the search strategy based on the PRISMA statement (Page et al., 2021).
Assessment of Risk of Bias
The risk of bias of the included studies was assessed independently by two of the authors using the Joanna Briggs Institute Critical Appraisal Checklists (Joanna Briggs Institute, 2014). These checklists evaluate the various aspects of papers with different methodologies including sample characteristics, exposure assessment, consideration of confounding factors, outcome measurement, and appropriate statistical techniques. To minimize bias and ensure reliability, distinct criteria were applied based on the study design. For cohort studies, the focus was on assessing the similarity of groups, adequacy of follow-up time, and loss to follow-up. For cross-sectional studies, the emphasis was on clearly defining inclusion criteria and study settings. Disagreements between the reviewers were resolved by discussion.
Results
In total, 4,147 articles resulted from the electronic search and 1,699 research articles remained after removing duplicates; 1,416 were excluded after reviewing the titles and an additional 169 were removed after reviewing the abstracts, leaving 114 articles. After full-text reviews, 31 articles were included in the final analysis.
Out of the 82 articles removed after a full review, the majority were excluded due to their failure to measure VT/STS, the primary focus of the study. Additionally, several articles featured samples that were not representative of the intended population, often consisting of emergency department workers rather than individuals working as prehospital providers in the field. Furthermore, several articles lacked empirical measurements and others were not available in English. The final article had an insufficient sample size of EMS; while some EMS workers were included in the study, they did not provide a breakdown of the results by occupation, making it impossible to discern the specific impact of EMS workers and rendering it ineligible for inclusion.
Analysis
The articles were categorized into whether they addressed (a) prevalence of vicarious traumatization or secondary traumatic stress, found in Table 2; (b) risk and protective factors for vicarious traumatization or secondary traumatic stress, found in Table 3; and/or (c) manifestations of vicarious traumatization or secondary traumatic stress among professionals involved in the prehospital emergency medical process, found in Table 4. Many fell into multiple categories. By examining existing systematic reviews, key areas were identified that have consistently been considered in prior reviews and deemed crucial for advancing our understanding of VT/STS. By adopting these categories, this study strove to provide insights that are not only relevant to the current state of knowledge but also valuable for informing future investigations in this field. After categorization, a narrative analysis of the included articles was conducted.
Of the 31 articles included in this systematic review, 11 (35.5%) addressed prevalence; 26 (83.9%) described risk and/or protective factors; 8 (25.8%) described manifestations of VT/STS; and 2 (6.5%) articles presented an intervention to decrease stress, burnout, and VT/STS. Table 1 describes each of the 31 studies organized alphabetically by the first author. Figure 2 describes additional characteristics across the 31 studies.
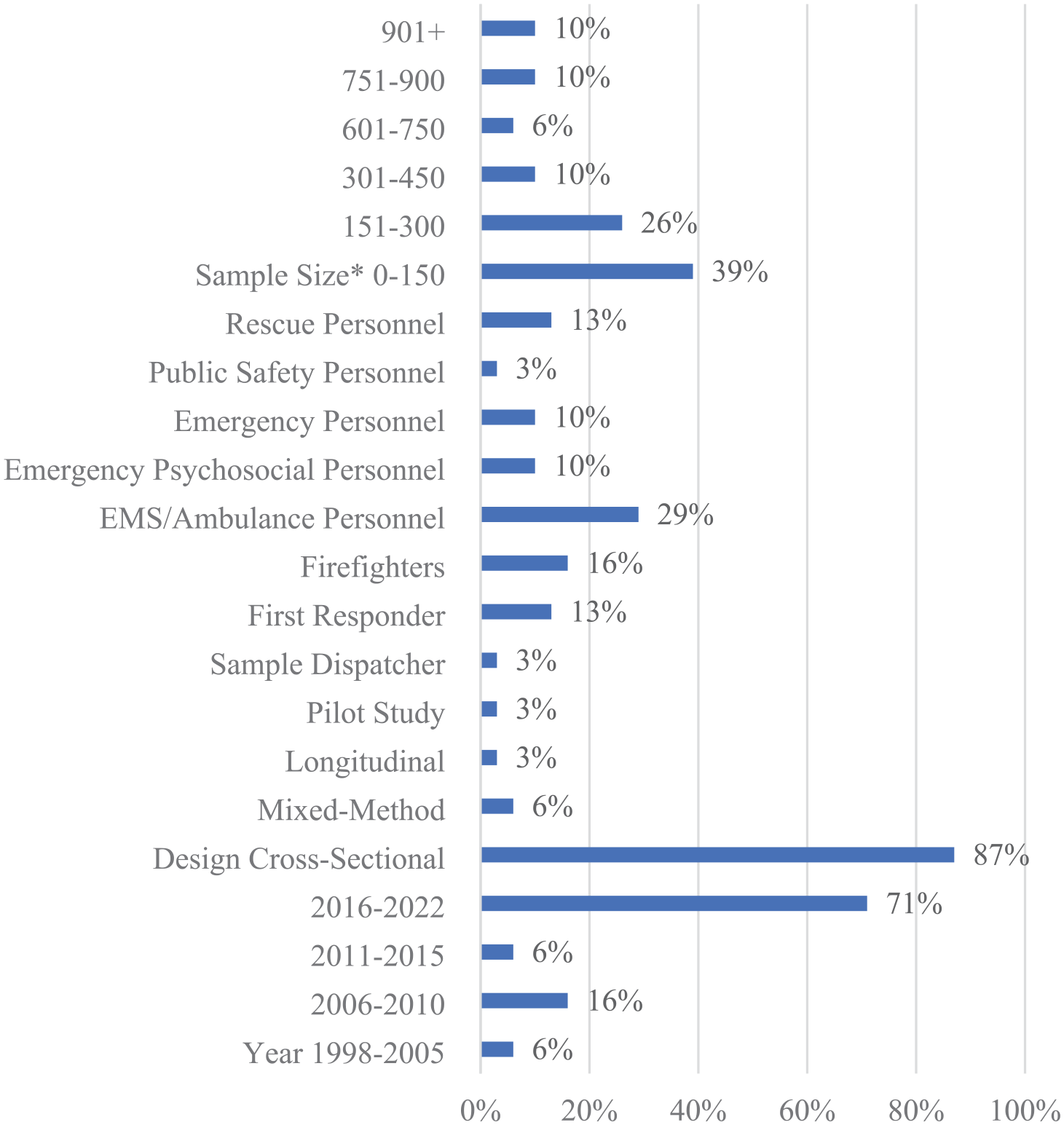
Characteristics of studies.
Summary of Studies Included.

Note. Instrument citations: Impact of Events Scale – Revised (Beck et al., 2008), Posttraumatic Stress Symptom Scale (Sahin et al., 2001), Professional Quality of Life (Stamm, 2005), PTSD Symptom Scale (Foa et al., 1993), Revised PTSD Inventory (Solomon et al., 1993), Secondary Traumatic Stress Inventory (Ogińska-Bulik et al., 2021), Secondary Traumatic Stress Scale (Bride et al., 2004), Secondary Traumatic Stress Scale – Italian Version (Setti & Argentero, 2014), Vicarious Trauma Scale (Aparicio et al., 2013). PTSD = posttraumatic stress disorder; EMS = emergency medical services; DSM-5 = Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition.
Risk of Bias
The risk of bias within studies was assessed using the JBI Critical Appraisal Checklist (Appendix B) (Joanna Briggs Institute, 2014). Overall, most of the studies had a low risk of bias based on the assessment done. Of the studies, two were at moderate risk for bias (Razakarivony et al., 2021; Stout et al., 2021), and none were at high risk of bias. Further information about the grading criteria can be found in the Checklist for Analytical Cross-Sectional Studies of the Joanna Briggs Institute (Joanna Briggs Institute, 2017a) and the Checklist for Cohort Studies of the Joanna Briggs Institute (Joanna Briggs Institute, 2017b).
Prevalence
Among the studies in this review, 11 reported levels of VT/STS, PTSD, or symptoms of these conditions among the population of interest. A total of nine different measurement tools were used: Impact of Events Scale – Revised (Beck et al., 2008), Posttraumatic Stress Symptom Scale (Sahin et al., 2001), ProQOL (Stamm, 2005), PTSD Symptom Scale (Foa et al., 1993), Revised PTSD Inventory (Solomon et al., 1993), Secondary Traumatic Stress Inventory (Ogińska-Bulik et al., 2021), STSS (Bride et al., 2004), Secondary Traumatic Stress Scale – Italian Version (Setti & Argentero, 2014), Vicarious Trauma Scale (Aparicio et al., 2013).
The findings of the 11 studies on prevalence are summarized in Table 2. Among the 11 studies that measured the prevalence of either PTSD or VT/STS, four measured the prevalence of meeting diagnostic criteria, one measured the prevalence of meeting diagnostic criteria and symptom levels, one measured symptom levels, one measured symptom levels and compared them with the experiences of other professionals, and four made comparisons of experiences between professions (details can be found in Table 2). Among the five that measured the prevalence of meeting diagnostic criteria, the prevalence ranged between 11.3% and 40% (Bastug et al., 2019; Kindermann et al., 2020; Razakarivony et al., 2021; Setti et al., 2016; Wagner et al., 1998). Among the three studies that measured symptom levels, two found that intrusion symptoms were most common ranging between 51.6% and 63.1% of participants experiencing at least one symptom (Argentero & Setti, 2011; Setti et al., 2016). The last of the three studies that measured symptom levels found that 43.3% of participants had high levels of STS symptoms (Ogińska-Bulik et al., 2021). Among three of the five studies that compared VT/STS between different professions, paramedics were found to have lower STS scores compared with doctors and/or nurses (McAleese et al., 2016; Ogińska-Bulik et al., 2021; Ondrejková & Halamová, 2022). Another study found that healthcare workers had higher levels of arousal compared to emergency workers (Vagni et al., 2020), and the final study found that volunteers presented lower levels of secondary traumatization compared with interpreters, trauma therapists, social workers, psychotherapists, and physicians working with refugees (Greinacher, Nikendei, et al., 2019).
Summary of Prevalence Findings.

Note. PTSD = posttraumatic stress disorder; STS = secondary traumatic stress.
Risk and Protective Factors
In this review, the majority (26 of 31 studies) considered a variety of different factors that may affect levels of VT/STS. They are organized into the following categories: (a) demographic differences, (b) interpersonal and community factors, (c) trauma responses, (d) work environment, and (e) fieldwork. The findings are summarized in Table 3.
Summary of Risk/Protective Factors.

Note. EMS = emergency medical services.
Demographic Differences
Of the studies in this review, 15 considered demographic differences among those with VT/STS. The items considered included gender (9 studies), age (8), relationship status (6), education level (3), drug/alcohol use (2), income/financial status (2), race (2), health/wellness (1), housing (1), medical care (1), non-work-related traumatic life events (1), number of children (1), and physical activity/stress (1). Within gender, identifying as female (the studies identified in this review considered only female and male/binary genders in their analyses) was associated with increased risk for negative outcomes compared with males in four of the nine studies (Argentero & Setti, 2011; Caricati et al., 2020; Cicognani et al., 2009; Greinacher, Nikendei, et al., 2019). One of the nine studies found a negative association between identifying as female and the outcome (Smirnova et al., 2022), and the last four studies found no association (Kindermann et al., 2020; Miller & Unruh, 2019; Miller et al., 2018; Vagni et al., 2020). Among the eight studies that considered age as a potential risk or protective factor, six studies found that it was not associated with the outcomes related to experiencing vicarious trauma (Kindermann et al., 2020; Miller & Unruh, 2019; Miller et al., 2018; Smirnova et al., 2022; Stout et al., 2021; Vagni et al., 2020), and two found that there was a negative association between age and the outcomes (Greinacher, Nikendei, et al., 2019; Pietrantoni & Prati, 2008). Of the six studies that considered relationship status, four found it to have no association (Beaton et al., 2004; Miller & Unruh, 2019; Miller et al., 2018; Smirnova et al., 2022), while one study found a negative correlation between being in a relationship and VT/STS (Kindermann et al., 2020) and another found a positive association (Argentero & Setti, 2011). Among the three studies that considered education level, all found that it had no association with symptoms of VT/STS (Kindermann et al., 2020; Miller & Unruh, 2019; Miller et al., 2018). One study found that drug/alcohol use was not associated with symptoms related to VT/STS (Chang & Taormina, 2011), while a different study found that they were positively correlated (Ericsson et al., 2021). Race was found to have no association in both studies that considered it (Miller & Unruh, 2019; Miller et al., 2018) as were income/finances (Chang & Taormina, 2011; Smirnova et al., 2022), housing (Chang & Taormina, 2011), and non-work-related potentially traumatic life events (Behnke et al., 2019). Number of children (Kindermann et al., 2020) and physical activity (Meckes et al., 2021) were both positively associated with symptoms related to vicarious trauma. Health/wellness and medical care were both inversely associated with VT/STS (Chang & Taormina, 2011).
Interpersonal and Community Factors
Interpersonal factors were considered by 10 different studies, including social support (6 studies), community (2), social exclusion (1), and social motivation (1). All the studies that considered how social support affected the symptoms of VT/STS or PTSD found an inverse relationship (Behnke et al., 2019; Chang & Taormina, 2011; Greinacher, Nikendei, et al., 2019; Setti et al., 2016; Smirnova et al., 2022; Vagni et al., 2020). Of two studies that considered the impact of a person’s community, one found that it was inversely associated with VT/STS (Chang & Taormina, 2011), while the other found that it had no association (Pietrantoni & Prati, 2008). Experiences of social exclusion (Ericsson et al., 2021) and placing importance on social motivations (Caricati et al., 2020) were each positively associated with VT/STS.
Strategies for Dealing With Trauma Responses
Of the 31 articles in this review, 12 of them considered a variety of trauma response strategies as possible risk/protective factors including mindfulness (3 studies), resiliency (2), and self-efficacy (2). An additional 25 strategies were named by one study each. Among these responses, mindfulness was found to be inversely associated with VT/STS in two studies (Greinacher, Nikendei, et al., 2019; Setti & Argentero, 2014), while having no association in another (McDonald et al., 2022). Self-efficacy had no association in one study (Caricati et al., 2020) but was inversely associated with another (Pietrantoni & Prati, 2008). Secure attachment (Kindermann et al., 2020), affective commitment (Setti et al., 2016), self-beliefs (Shiri, Wexler, Schwartz, et al., 2010), general beliefs (Shiri, Wexler, Schwartz, et al., 2010), resiliency (Miller & Unruh, 2019; Miller et al., 2018) and stopping negative thoughts (Vagni et al., 2020) were each inversely associated with symptoms of VT/STS and PTSD. Meanwhile, attachment avoidance (Greinacher, Nikendei, et al., 2019), sense of coherence (Greinacher, Nikendei, et al., 2019), depression (Kindermann et al., 2020), anxiety (Kindermann et al., 2020), greater distress tolerance (McDonald et al., 2022), avoidance coping (Prati et al., 2009), burnout (Prati et al., 2009), emotional stress (Vagni et al., 2020), cognitive stress (Vagni et al., 2020), and COVID-19 stress (Vagni et al., 2020) each had a positive association with symptoms related to VT/STS and PTSD. 1 There was no association found with moderation by inner attitude and constitution (Greinacher, Nikendei, et al., 2019), dismissive avoidant attachment (Kindermann et al., 2020), collective efficacy (Pietrantoni & Prati, 2008), emotional and support coping (Prati et al., 2009), problem-focused coping (Prati et al., 2009), cognitive restructuring coping (Prati et al., 2009), norm beliefs (Shiri, Wexler, Schwartz, et al., 2010), goal beliefs (Shiri, Wexler, Schwartz, et al., 2010), ECR-attachment avoidance (Greinacher, Nikendei, et al., 2019).
Work Environment
Risk and protective factors relating to the work environment were considered by 14 studies. The factors studied by multiple studies included years of service (5), volunteering (5), coworker support (3), work hours/shifts (3), case discussions/debriefing (3), role (3), organizational support (2), part-time (2), and work in other fields (2). An additional 14 factors were identified by one study. Those that were measured by multiple studies often had conflicting results. Work hours/shifts were measured by three studies and two found that it was not associated with VT/STS (Argentero & Setti, 2011; Caricati et al., 2020). Years of service also varied. Of the five studies, three studies found that it was not associated (Beaton et al., 2004; Miller et al., 2018; Stout et al., 2021); one found that it was positively associated (Greinacher et al., 2019), and one found that it depended on who was being measured: firefighters had a positive association and EMS had no association (Miller & Unruh, 2019). Five studies considered volunteering; four were inversely associated (Cicognani et al., 2009; Miller & Unruh, 2019; Miller et al., 2018; Setti et al., 2016), and one had no association (Razakarivony et al., 2021). Case discussion/debriefing was found to be inversely associated with VT/STS in one study (Greinacher, Nikendei, et al., 2019) and had no association in two studies (Miller & Unruh, 2019; Miller et al., 2018). The role was found to be positively associated in one study (Meckes et al., 2021) and had no association in another study (Wagner et al., 1998). Coworker support was positively associated in one study (Setti et al., 2016) and had no association in two others (Miller & Unruh, 2019; Miller et al., 2018). Organizational support was inversely associated with VT/STS in one study (Miller et al., 2018) and one found that it depended on who was being measured: inversely associated among firefighters and no association among EMS (Miller & Unruh, 2019). Working in other fields and working part-time in one study had no association (Miller et al., 2018) while another study found that it depended on the role: EMS had a positive association and firefighters had no association (Miller & Unruh, 2019). Role clarity (Argentero & Setti, 2011), understanding motives (Caricati et al., 2020), being integrated at work (Greinacher, Nikendei, et al., 2019), and perceived cohesion (Smirnova et al., 2022) were each inversely associated with VT/STS. Identifying with volunteers and self-enhancement were each positively associated with VT/STS (Caricati et al., 2020). Seniority (Argentero & Setti, 2011), predictability of the work (Argentero & Setti, 2011), view of accomplishments (Bastug et al., 2019), work protections (Caricati et al., 2020), career concerns (Caricati et al., 2020), job values (Caricati et al., 2020), type of supervision (Greinacher, Nikendei, et al., 2019), and being members of a professional organization had no association in the studies (Stout et al., 2021).
Field Work
Factors about the case while in the field were considered by five of the studies. Those that had a positive association included identifying oneself with a victim or victim’s family (Behnke et al., 2019); having a case that was extremely tragic due to the accident’s sequence of events (Behnke et al., 2019), experiencing higher levels of social emergency experiences (Ericsson et al., 2021), having a need for elder social services (Ericsson et al., 2021), job experience (Wagner et al., 1998), and the number of distressing missions (Wagner et al., 1998). There was no association between mission frequency (Argentero & Setti, 2011; Stout et al., 2021) and being on duty to go on missions (Wagner et al., 1998).
Manifestations
This review found eight articles that described the manifestations of VT/STS, defined as longer-term consequences on their work or health; see Table 4. The most common manifestation studied was burnout, which was found to be related to VT/STS or PTSD in four articles (Bastug et al., 2019; Chang & Taormina, 2011; Cicognani et al., 2009; Miller et al., 2018). Two of the articles found that compassion satisfaction was associated with experiences of vicarious trauma (Chang & Taormina, 2011; Miller et al., 2018), one study found that 85% of participants were satisfied with their work (Bastug et al., 2019), and one found that compassion fatigue was 4.6 times more likely in those with concomitant traumatic stress syndromes like VT/STS (Renkiewicz & Hubble, 2022). Depression and anxiety were found to be manifestations in one study (Kindermann et al., 2020) while a high prevalence of psychiatric symptoms including depressive mood, social dysfunction, and substance abuse were found in another (Wagner et al., 1998). Finally, one study found that IES-R scores were 11.16 points higher in the group with suicidality compared to the group without: a 60% relative difference (Renkiewicz & Hubble, 2022).
Summary of Manifestations.

Note. PTSD = posttraumatic stress disorder.
Intervention Research
Of the 31 articles that fit the criteria for this review, two articles tested interventions related to helping alleviate the impacts of vicarious trauma, see Table 5. The first article was a one-arm pilot study that focused on mindfulness to improve wellbeing and reduce distress among EMS workers at high risk for experiencing vicarious trauma (Ducar et al., 2020). The researchers used the ProQOL to measure the level of secondary traumatic stress among participants before and after the intervention (Ducar et al., 2020). The study initially enrolled 15 EMS providers, but four were lost to attrition, leaving a total sample size of 11 participants (Ducar et al., 2020). The researchers found that there was no significant change in secondary traumatic stress or perceived stress at the end of the intervention nor 6 months after completion of the intervention; however, a decrease in burnout and an increase in compassion satisfaction occurred across the sample population (Ducar et al., 2020).
Summary of VT/STS Intervention Studies.

VT = vicarious traumatization; STS = secondary traumatic stress; EMS = emergency medical services.
The second article considered the impact of training volunteers to provide psychological first aid (Greinacher et al., 2022). The study had 100 psychosocial emergency care volunteers who trained three weekends over a 6-month period (Greinacher et al., 2022). After the training, none of the volunteers had clinically relevant symptoms associated with VT/STS and they showed significantly fewer symptoms than other volunteers, trauma therapists, and refugee caregivers (Greinacher et al., 2022).
Discussion and Implications
This systematic review aimed to summarize and identify gaps in the literature concerning the epidemiology of vicarious traumatization in prehospital EMS personnel, including dispatchers, EMS, firefighters, rescuers, and others. In particular, this study looked at a group of professionals that have not been included in other systematic reviews as a whole. Recent systematic reviews have considered a broader definition of first responders (Greinacher, Nikendei, et al., 2019), child welfare workers (Molnar et al., 2020), mental health professionals (Bercier & Maynard, 2015), and others but the authors were unable to find reviews that considered this unique group of workers. These helping professionals are often overlooked in vicarious trauma-related research and interventions and yet clearly experience vicarious trauma and its potentially negative impacts as a regular occupational challenge. As magnified during the COVID-19 pandemic, helping professionals play a vital role in our society and without proper support, are at high risk for VT/STS resulting in increased turnover for their organizations. The findings of this review also shed light on inconsistencies between research studies and the need for more consistent measures and methods in studying VT/STS in this population.
The prevalence of VT/STS in EMS professionals was assessed using nine different measurement scales across the reviewed studies. The reported outcomes encompassed VT/STS, PTSD, and individual symptoms experienced by the participants. While there was variation in measurement approaches, the data consistently indicated low to moderate prevalence rates of traumatization among these professionals. However, it should be noted that the lack of consistent measures limits the certainty and comparability of these findings.
Regarding risk and protective factors, a wide range of variables were measured across the included studies. The most compelling protective factor mitigating VT/STS was social support, which was consistently shown to mitigate symptoms across all six studies. The other most examined factors were gender (in nine studies) and age (in eight studies); however, these studies often yielded conflicting findings, emphasizing the need for more comprehensive research to better understand the influence of these demographic categories on VT/STS among prehospital EMS professionals. These differences may be a result of the variety of different measures used in the studies as well as the different populations considered and the number of participants. It is important to highlight that few studies have addressed the impact of race or racism, and none have delineated the experiences of individuals who identify as part of the LGBTQIA+ community. Incorporating considerations of these intersectional identities and the corresponding social experiences that can provide their own sources of direct trauma into research on vicarious trauma and STS is crucial. Research should recognize the unique personal experiences of diverse groups and aim to understand how their work with traumatized populations may impact them. Having workplace support to retain diverse providers not only brings varied perspectives but also enhances the comfort and trust of victims by providing care from professionals who share similar backgrounds.
Among the 31 articles, there are 8 different profession categories, and 13 of the studies had less than 150 participants. These methodological aspects, along with the variety of measurement tools utilized, may have led to the discrepancies between results. There needs to be larger, more comprehensive studies to understand the risk/protective factors related to VT/STS.
The longer-term manifestation of VT/STS was explored in a smaller number of studies, with burnout being the most frequently considered factor. However, without longitudinal data, it remains unclear whether burnout is a risk factor for VT/STS, if VT/STS contributes to burnout, or if it is a bidirectional relationship. A 2014 meta-analysis examining the relationship between burnout and VT/STS found a strong association between the two but suggested that this link may stem from shared risk factors rather than a direct relationship(Cieslak et al., 2014). A 2015 study of human services workers found that job burnout contributed to participants’ risk of developing VT/STS (Shoji et al., 2015). However, neither is enough, nor with the inclusion of the articles from this review, to determine the relationship between these two constructs. Further research is needed to establish a clearer understanding of the relationship between burnout and VT/STS among these professionals, preferably longitudinal research to help understand the temporality of the relationship.
Finally, only two studies in the literature addressed interventions for VT/STS in prehospital EMS personnel, and one of them was a pilot study with a small number of participants. A scoping review of interventions for health and human services providers treating people exposed to vicarious trauma found that while interventions showed promise in reducing VT/STS, the studies lacked rigor and were generally focused on general stress management rather than specific effects of vicarious trauma (Kim et al., 2022). The scarcity of intervention studies underscores the need for more research and funding in this area to develop effective interventions for mitigating the impact of vicarious trauma in this population.
Similar problems regarding inconsistent measures and methods have been observed in other systematic reviews on VT/STS. A systematic review focused on child welfare workers identified 6 different measures used across 15 studies to assess prevalence (Molnar et al., 2020), while another systematic review on first responders found six different measures employed in 31 studies (Greinacher, Derezza-Greeven, et al., 2019). In a 2015 publication titled “Interventions for Secondary Traumatic Stress with Mental Health Workers: A Systematic Review,” the authors reviewed over 4,000 citations and found that none met the inclusion criteria for interventions to alleviate symptoms of STS among mental health workers (Bercier & Maynard, 2015). This aligns with the current study, which also identified a scarcity of intervention studies, with only two identified after the year 2015. There have also been concerns about the methodology of some studies. Small samples of workers in very specific locations are common among studies of vicarious trauma. While these studies can be helpful for the area in question, they limit generalizability to larger studies. Improving consistency and robustness across studies of VT/STS would improve the usability as well as the compatibility of the research data and thus would better support policy and organizational changes related to improving procedures and practices to support and maintain the health of not only prehospital EMS professionals but all helping professionals. While the results of these studies provide diverse insights, the lack of consistency in measures underscores the need for longitudinal research to gain a more comprehensive understanding of the impact of vicarious trauma on prehospital EMS personnel. Longitudinal studies would enable a clearer assessment of the long-term effects of VT/STS and inform the development of targeted interventions to support these professionals in their challenging roles.
The growing impacts of climate change also pose significant challenges for prehospital EMS personnel, particularly as escalating weather events increasingly affect human health (Rocque et al., 2021). As the frequency and severity of such events rise, the operational and logistical burdens on EMS are expected to intensify. A Finnish study involving participants with practical experience in EMS and emergency departments anticipates an increased workload, operational challenges such as disruptions to technical infrastructure, and complications in maintaining vital societal functions like transportation networks (Karstila et al., 2024). Similarly, research conducted in France highlights that the rising frequency and complexity of disasters will exacerbate resource limitations and disproportionately impact vulnerable populations, thereby increasing the complexity of emergency scenarios (Alreshidi et al., 2022). These findings underscore the likelihood of a growing strain on EMS systems and personnel, including a heightened risk of STS among workers, precisely at a time when their services are most critically needed. These results, along with future, more robust research around VT/STS will be able to inform interventions, training programs, and support systems at organizations/workplaces.
Because vicarious trauma is an occupational challenge, it is important for organizations to work on improving their policies, practice, procedures, and programs to ensure the support and protection of their workers, including when new challenges to the field arise. A recent study showed that organizations that were rated by their workers as highly vicarious trauma-informed were also more likely to pivot with successful COVID-19 mitigation strategies (Meeker et al., 2022). By reducing the negative impacts of vicarious trauma and promoting the positive ones, organizations can reduce turnover and improve outcomes not only among staff but also among the populations that they serve. Lower turnover rates and better mental health among helping professionals will improve their ability to be in the community and to help those in need of EMS.
Limitations
While this study followed the PRISMA-recommended methods for the search strategy, it is important to acknowledge that some eligible studies may have been missed; this limitation is common to all systematic reviews. While the 31 studies in this review considered a variety of risk/protective factors and manifestations of VT/STS, there was limited overlap among the results making it difficult to draw conclusions about the most frequent risk and protective factors and what manifestations are most common among EMS professionals. Our review found only two studies of interventions and is therefore only able to provide an extremely limited view of interventions and potential next steps for intervention development. Three other systematic reviews around vicarious trauma in other professions also found no evaluation studies of interventions related to their population of interest (Bercier & Maynard, 2015; Molnar et al., 2020; Nimmo & Huggard, 2013). These limitations are consistent with current gaps in the literature and highlight the need for further research to address them and for investment in intervention evaluation research to prevent VT/STS among emergency response medical professionals.
Conclusion
Considerable steps need to be taken to protect our EMS professionals across the globe. This study demonstrates the lack of adequate research studies as well as interventions. These professionals are key first responders that the public entrusts with their lives. Still, they are often the lowest paid among first responders and receive fewer benefits (Schafer et al., 2015). They provide crucial services to communities and in line with those services experience vicarious trauma as an occupational challenge. Workplaces and municipalities have an obligation to put into place policies and procedures to prevent and mitigate the negative outcomes of vicarious trauma among their employees while taking the opportunity to bolster vicarious resilience, PTG, and workplace relationships to create and maintain a healthier and more productive work force. Additionally, prioritizing improved access to care is essential for addressing and alleviating the impacts of VT/STS.
Longitudinal studies of the epidemiology of vicarious traumatization/secondary traumatic stress, as well as intervention evaluation research, will help organizations and workers be more healthy, guided by data from the studies in this review and future research. Evidence-based interventions will then need to be disseminated, with the goal of keeping workers healthy while doing this empathic work to care for victims of traumatic events. While vicarious trauma is an occupational challenge for prehospital emergency workers, it does not have to result in VT/STS or further manifestations of psychological, social, or occupational wellness.
Implications of the Review.

Footnotes
Appendix A – Search Terms
Appendix B
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.