
Abstract
Child victimization negatively impacts many aspects of health in children and adolescents. An increasing number of studies have examined the influence of child victimization on gaming disorder (GD), though findings have been inconclusive. To address this problem, in this meta-analytic study, we quantitatively synthesized existing empirical evidence on the associations between different types of child victimization and GD and examined whether study and participant characteristics moderate the association. Studies examining the relationship between victimization and GD published before December 8, 2023 were identified through systematic searches conducted in PubMed, CINAHL Complete, Embase, PsycINFO, and Web of Science databases. Thirty-six studies (112,057 participants) met the study selection criteria and showed a significant association between child victimization and GD, with a small effect size (r = .221; 95% confidence interval, CI [0.174, 0.268], p < .001). The pooled effect sizes for different types of victimization ranged from r = .154 to .218 (ps < .05). The overall effect size is relatively consistent, independent of age and sex of participants, study regions, study quality, and sampling methods. Study design and study samples are the only two significant moderators, with larger pooled effect sizes for cross-sectional studies (r = .245; [0.188, 0.300]) and clinical samples (r = .468; [0.328, 0.588]). Child victimization is a significant risk factor for GD, regardless of the specific type of victimization. Prevention strategies addressing multiple types of victimization are recommended.
The surge in online gaming across the globe, further accelerated by the COVID-19 pandemic (Han et al., 2022), has intensified public health concerns about maladaptive gaming behaviors among children and adolescents. Gaming disorder (GD) has first been earmarked for further research in the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5) (American Psychiatric Association, 2013). Among different technology-related disorders, it is the only one that has been included in the 11th revision of the International Classification of Diseases and Related Health Problems (ICD-11) as a formal health diagnosis (World Health Organization, 2019). GD is an addiction problem characterized by a persistent pattern of gaming behaviors and impaired control over online or offline gaming that results in functional impairment for a period of 12 months (World Health Organization, 2019). Despite its formal recognition, the diagnosis of GD remains contentious with ongoing debates surrounding various aspects, including the lack of consensus on symptomatology, concerns regarding the validity of the diagnostic assessments used, and fears of pathologizing healthy gaming behaviors that could lead to excessive diagnosis and treatment (Aarseth et al., 2017; Galanis et al., 2021; Wang et al., 2019). Nevertheless, meta-analyses indicate a global pooled prevalence estimate of 3% for GD among general population (Stevens et al., 2021), and significantly higher rates ranging from 6% to 8% among adolescents (Gao et al., 2022; Kim et al., 2022). There is also extensive literature documenting a vast array of adverse health, psychological, and social consequences associated with GD, including sleep problems, depression, anxiety, and strained parent-child relationships (e.g., Mihara & Higuchi, 2017; Paulus et al., 2018; Richard et al., 2020).
Child victimization is another crucial and prevalent public health problem. Approximately 13% to 55% of children and adolescents suffer victimizations globally, depending on the types of victimization and geographical locations (Moody et al., 2018; Smith et al., 2023; Stoltenborgh et al., 2015). Child victimization encompasses a spectrum of victimization to interpersonal violence, child abuse, and crimes, including maltreatment, peer and sibling victimization, sexual victimization, physical assault, property victimization, and witnessing/indirect victimization (Finkelhor et al., 2007). The proliferation of technology has not only given rise to GD but also a new form of victimization—cyber-victimization. Cyber-victimization can be broadly defined as an experience of intentional and repeated harm inflicted through digital means, such as computers, cell phones, and other electronic devices (Patchin & Hinduja, 2015). While some studies view cyber-victimization as a digital form of peer victimization (Miller et al., 2025; Nicolaet al., 2024), identifying cyber-perpetrators is often challenging due to their anonymity.
From a person-in-environment perspective, adolescents’ GD is likely influenced by factors related to the person as well as the social environment (Király et al., 2023). This perspective underscores the importance of expanding the research scope beyond the individual level and investigating the influences of social environment such as adolescents’ experience of victimization in their social contexts, on GD. Several theoretical perspectives suggest potential social and emotional mechanisms underlying such association. For instance, there is consistent evidence supporting the impacts of child victimization on emotional processing, such as heightened emotion reactivity and difficulties in emotion regulation (McLaughlin et al., 2020). Individuals with impairments in emotional processing, especially emotion regulation, may attempt to regulate or escape unwanted emotions through engaging in addictive behaviors such as gaming (Marchica et al., 2019). Social withdrawal may be one of the underlying social pathways through which child victimization is associated with GD. Taking peer victimization as an example, children and adolescents who are victimized at school may withdraw themselves from social interactions as a way to protect themselves from further harm (Ding & Li, 2025). They may then turn to online gaming to compensate for their unmet social needs, such as social inclusion and desire for acceptance and validation (Cheng et al., 2018). These theoretical perspectives are in alignment with the longstanding self-medication hypothesis in the addiction literature (Khantzian, 1987, 1997), which posits addictive behaviors function as a self-regulating strategy for those who have difficulties in regulating emotions and relationships.
Despite the well-established association between different types of child victimization and other addictions, such as substance use disorders (Cicchetti & Handley, 2019; Tonmyr et al., 2010), research evidence pertinent to child victimization as a risk factor for GD is mixed. Peer victimization appears to be a consistent predictor of GD, where two meta-analytic reviews (Gao et al., 2022; Ji et al., 2022) found that it was significantly associated with GD, though the effect sizes were small. On the other hand, the relationship between child maltreatment and GD is not readily discernible. Specifically, the systematic review conducted by Nielsen et al. (2020) identified one study examining the association between child maltreatment and GD, which had a significant but weak correlation. Among the three relevant studies reviewed in Schneider et al. (2017), only one reported that maltreated adolescents were more likely to have problem gaming. In a recent review, Zhuang et al. (2023) meta-analyzed three studies on the association between maltreatment and GD, which pooled a non-significant correlation. One critical limitation of the previous reviews is the dearth of studies (ranging from one to six studies) related to the study topic. A possible reason is that the objectives of the studies were to evaluate a broad range of risk factors of GD, using search terms and selection criteria not specific to victimization, which may not be able to capture all relevant articles. The small number of included studies may lead to insufficient statistical power to detect the associations in question (e.g., the association between child maltreatment and GD). An updated meta-analysis with appropriate search strategies to identify articles related to different types of child victimization and to clarify their associations with GD is needed.
A wealth of studies have emphasized the concept of poly-victimization, highlighting the need to assess multiple types of victimization within children’s interpersonal contexts simultaneously (Chan, 2019; Finkelhor et al., 2007). However, previous review studies tended to focus on specific types of child victimization, especially child maltreatment and peer victimization; the strength of the relationships between GD and other forms of child victimization, such as cyber-victimization remains unclear. A comprehensive evaluation of the strengths of the associations of different forms of child victimization will offer us valuable evidence regarding whether victimization, regardless of the specific type, is a shared factor associated with GD. Such understanding will add to the existing research that suggests victimization may be a transdiagnostic risk factor for psychopathology and mental health problems (Forbes et al., 2020; Konzok et al., 2025); and in this case GD.
Differences in the study and participant characteristics may influence the strength of the associations between victimization and GD. Specifically, the relationship between child victimization and GD may vary across regions due to the differing levels of GD preventive initiatives and intervention efforts among different nations (Thomas et al., 2024). In addition, previous research has attributed the national-level variability of addictive behaviors (e.g., social media addiction) to cultural differences, indicating collectivist cultural values (e.g., social conformity) may explain the higher prevalence of GD in Asian countries (Cheng et al., 2021). Sex is considered as another factor that may influence the relationship between victimization and GD. Males are generally found to spend more time gaming and to be more vulnerable to developing GD than females (Lopez-Fernandez, Williams, Griffiths, & Kuss, 2019; Lopez-Fernandez, Williams, & Kuss, 2019; Wittek et al., 2016). Based on studies in the field of Internet addiction, males have a higher risk for Internet addiction than females after experiencing child maltreatment, potentially owing to their less developed emotional expression and regulation skills and a higher tendency to turn to the Internet as an escape (Zhang et al., 2024). Social gender identities and expectations may also play a role in influencing girls’ perception and experience in gaming since gameplay is viewed as male-dominated (Lopez-Fernandez, Williams, Griffiths, & Kuss, 2019). In contrast, a framework was recently proposed to understand the gender-related differences in the development of GD, suggesting that females may be more likely to use gaming to alleviate psychological distress at the initial stage and to compensate for feelings of loneliness and social phobia (Dong & Potenza, 2022). Furthermore, the impacts of childhood adversities on individuals are subject to changes over time (Ran et al., 2023) and the vulnerability for addictive behaviors varies across developmental periods (Guastaferro et al., 2024). Some studies reported that GD tends to decrease with the increasing age of child (e.g., Hazar, 2019) while others did not find the effect of age on GD (Hazar & Hazar, 2018). Overall, the moderating effect of regions, gender, and age on the association between child victimization and GD warrants further exploration.
The current meta-analysis is the first to quantitatively synthesize the empirical evidence on the relationship between different types of child victimization and GD. The second aim is to identify the possible study and participant characteristics (including study regions, sex, and age) that may moderate the relationship between child victimization and GD. The results of the present study will provide more robust scientific conclusions about the relationship between child victimization and GD, thereby offering implications for holistic gaming and victimization prevention and intervention efforts.
Methods
Search Strategy
In this meta-analysis, we adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to report the findings. The protocol was registered in the PROSPERO international prospective register for review protocols (registration number CRD 20231206). In this meta-analysis, searches were conducted in PubMed, CINAHL Complete, Embase, PsycINFO, and Web of Science databases by the first author on December 8, 2023. We ran searches in the titles, abstracts, and keywords of relevant publications, using four groups of search terms developed based on previous review studies: (a) victimization, abuse, violence, maltreatment, neglect; (b) game, gaming, videogame; (c) addiction, problematic, pathological, disorder, compulsive, dependence, excessive; and (d) child, adolescent, youth, teen, student. Synonymous terms were combined with the Boolean “OR” and the four groups of keywords were combined with the Boolean “AND.” There was no restriction regarding the year of publication, geographic location (e.g., country or region), or setting (e.g., clinical, school, or community). The search strategy can be found in Supplemental Appendix 1. Reference lists in the included studies and review articles were manually searched to identify additional relevant publications; one study was identified. Grey literature was searched for in Google Scholar using a combination of the following keywords: victimization, violence, maltreatment, and gaming. The first 10 pages of the search results were reviewed, and no additional publications were identified.
Study Inclusion Criteria
Studies were included if (a) the age range of participants was 18 years or less; (b) GD was measured (including the presence or absence of GD and the severity of GD); (c) the studies dealt with any type of child victimization, including child maltreatment, peer or sibling victimization, sexual victimization, community violence, cyber-victimization, and witnessing family violence; (d) the studies were observational; (e) statistical data were available for computing effect sizes; and (f) the article was published in English.
Screening Process
All search results were first exported to EndNote, then imported into Covidence, a web-based tool for managing systematic reviews. Duplicates were identified and removed using Covidence and manually. Two independent reviewers (first and second authors) completed title and abstract screening and full-text screening to assess the articles for inclusion according to the eligibility criteria. The inter-rater agreement (Cohen’s kappa) for title and abstract screening, and full-text screening was .928 and .808, respectively, indicating substantial to almost perfect agreement. Discrepancies were resolved through discussion with a third reviewer, who is a research staff member with experience in conducting systematic reviews.
Data Extraction
A standardized coding sheet was created to extract the following information: (a) publication information, such as year of publication and country of origin; (b) study methodological characteristics, including study design, sampling method, sample size, and sample type; (c) participants’ characteristics, including age (mean and standard deviation), sex (percentage of males), parent education level, and family socioeconomic status; (d) types of measures used to assess GD and victimization; and (e) data for computing effect sizes. Effect values were extracted according to the following criteria: The correlation coefficients between victimization and GD were included in the coding. Studies that did not report the required correlation coefficient but provided other relevant data, including means and standard deviations for comparison of GD severity between victimization and non-victimization groups, percentage of GD in victimization, and non-victimization groups were also included. When a study measured GD and/or victimization at multiple time points, effect sizes with the largest temporal distance between measures were selected. As data on victimization subtypes (e.g., physical or emotional abuse, neglect) were insufficient, global measures of victimization (e.g., child maltreatment) were extracted. All studies were independently extracted by two reviewers (first and second authors). Discrepancies were resolved through consensus. Twenty-one studies did not provide sufficient data for computing effect sizes. A request was made to the study’s corresponding author via email. Six authors replied to the request, and the remaining studies (n = 15) with no additional data provided in response were excluded.
Study Quality Assessment
The 22-item Strengthening the Reporting of Observational Studies in Epidemiology checklist (Vandenbroucke et al., 2007) was used to assess the quality of the included studies. Each study was assessed by two independent reviewers (first and second authors) for quality, with each item coded as 0 (no), 0.5 (unclear), or 1 (yes) (Supplemental Appendix 2). The highest possible score was 22 for a study meeting all the checklist criteria. Intercoder agreement (Cohen’s kappa) for the study quality ratings was .75, indicating substantial agreement between the reviewers. Discrepancies were resolved through consensus.
Statistical Analysis
Three major data formats (correlation, group means and SDs, and binary 2 × 2) were available from the selected studies. Data reported in group means and SDs and binary 2 × 2 formats were first converted to a common effect size metric, that is, correlation (r) using the Comprehensive Meta-Analysis (CMA) software. To estimate an overall association between child victimization and GD, a pooled r was computed by combining the effect sizes of all selected studies. Treating multiple effect sizes from a single sample as independent units will lead to inaccurate estimates of pooled effect sizes. To address this problem, we used the “averaging effect sizes” method (Moeyaert et al., 2016). Multiple effect sizes within one study were first averaged using the CMA software, then the results across studies were combined so that each study only contributed one effect size to the analysis (Borenstein et al., 2009). Apart from the overall association between child victimization and GD, correlation estimates of the associations between different types of victimization and GD were also pooled from the studies. The effect sizes and 95% confidence intervals (CIs) in each study are presented in forest plots. Then, separate meta-analyses were conducted based on the data format. Specifically, a pooled r and a pooled odds ratio (OR) were computed from studies reporting data on correlation or group means and SDs (n = 30) and studies providing binary 2 × 2 data (n = 6), respectively. These analyses served as sensitivity analysis. Due to the heterogeneity across studies, random-effects models were used. Q and I2 statistics were calculated to assess the extent of heterogeneity among effect sizes. A significant Q value suggests significant between-study variation. The I2 statistic represents the proportions of the total variation of the included studies. Pre-planned moderator analyses were conducted to examine any significant heterogeneity due to sex (>50% vs. <50% male), study regions (Asia vs. Europe vs. America), and mean age (≤12 vs. >12 years old). Additional moderator analyses that emerged from the data analysis process include sampling methods (probability vs. non-probability), study sample (school vs. community vs. clinical), study design (cross-sectional vs. longitudinal), and study quality scores (<18 vs. ≥18; i.e., over 80% of the total score). Funnel plots and the Egger test were used to evaluate potential publication bias. As potential publication bias was detected, the Duval and Tweedie’s (2000) trim-and-fill method was used to estimate how many studies it took for the funnel to be symmetrical and to calculate the adjusted pooled effect size after imputing the missing studies. The Duval and Tweedie’s trim-and-fill method also served as a sensitivity analysis. All analyses were conducted using the CMA software.
Results
Study Selection
A PRISMA flowchart of the study selection process is presented in Figure 1. The original search resulted in a total of 1,601 publications. After removal of 588 duplicates, a title and abstract screening was conducted, which removed 921 studies. We then conducted a full-text screening on 93 potentially relevant articles, with 35 studies meeting the eligibility criteria. One additional article was identified through a review of the reference lists of the selected articles. A total of 36 articles were included in our final analysis.
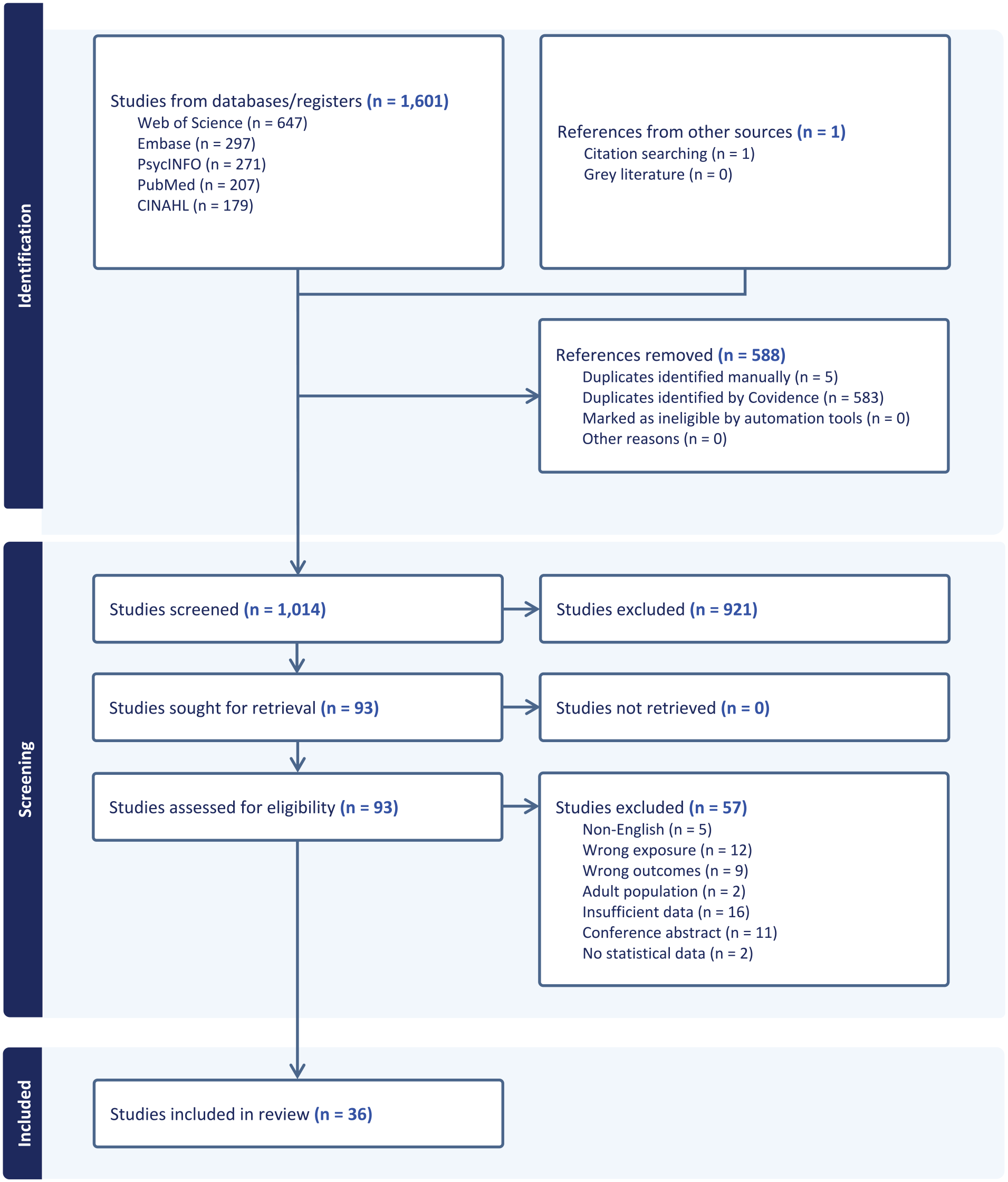
PRISMA flowchart of the study selection process.
Study Characteristics
Table 1 shows the study and participant characteristics of the 36 selected studies. The studies were published between 2013 and 2023 and involved 112,057 children and adolescents. The selected studies assessed various types of victimization, including peer victimization (n = 17), cyber-victimization (n = 15), child maltreatment (n = 10), witnessing parental conflicts (n = 2), and community violence (n = 1). The mean age ranged from 9.7 to 17.17 years. The percentage of male participants ranged from 30.61% to 100%. Most of the studies (n = 32) involved school samples, two studies had clinical samples, and two other studies had community samples. Of the selected studies, 26 adopted a cross-sectional design, while 10 were longitudinal studies. Twenty-four studies were conducted in Asian countries or regions, namely China (n = 21), Hong Kong (n = 1), Thailand (n = 1), and Vietnam (n = 1); nine studies were conducted in European countries, namely Turkey (n = 4), Germany (n = 3), Croatia (n = 1), and United Kingdom (n = 1); and two studies were conducted in North and Central America (The United States, n = 1 and Costa Rica, n = 1). The study quality scores ranged from 11.5 to 20, with an average of 16.42. All the measurements for victimization and GD used in the selected studies were self-reported. The most commonly used measurements for victimization in the selected studies included the E-Victimization Scale (Lam & Li, 2013) (n = 5), Olweus (1996) Bullying Questionnaire or an adapted version (n = 3), Delaware Bullying Victimization Scale—Student (Bear et al., 2014; Xie & Lv, 2015) (n = 3), Peer Victimization Questionnaire (Zhou et al., 2014) (n = 2), and Childhood Psychological Maltreatment Scale (Pan et al., 2010) (n = 2). GD was usually measured by the Internet Gaming Disorder Questionnaire (Gentile, 2009) or an adapted version (n = 7) and Internet Gaming Disorder Scale—Short Form (Pontes & Griffiths, 2015) (n = 5). The full list of measurements used in the selected studies can be found in Supplemental Appendix 3.
Characteristics of the Included Studies.
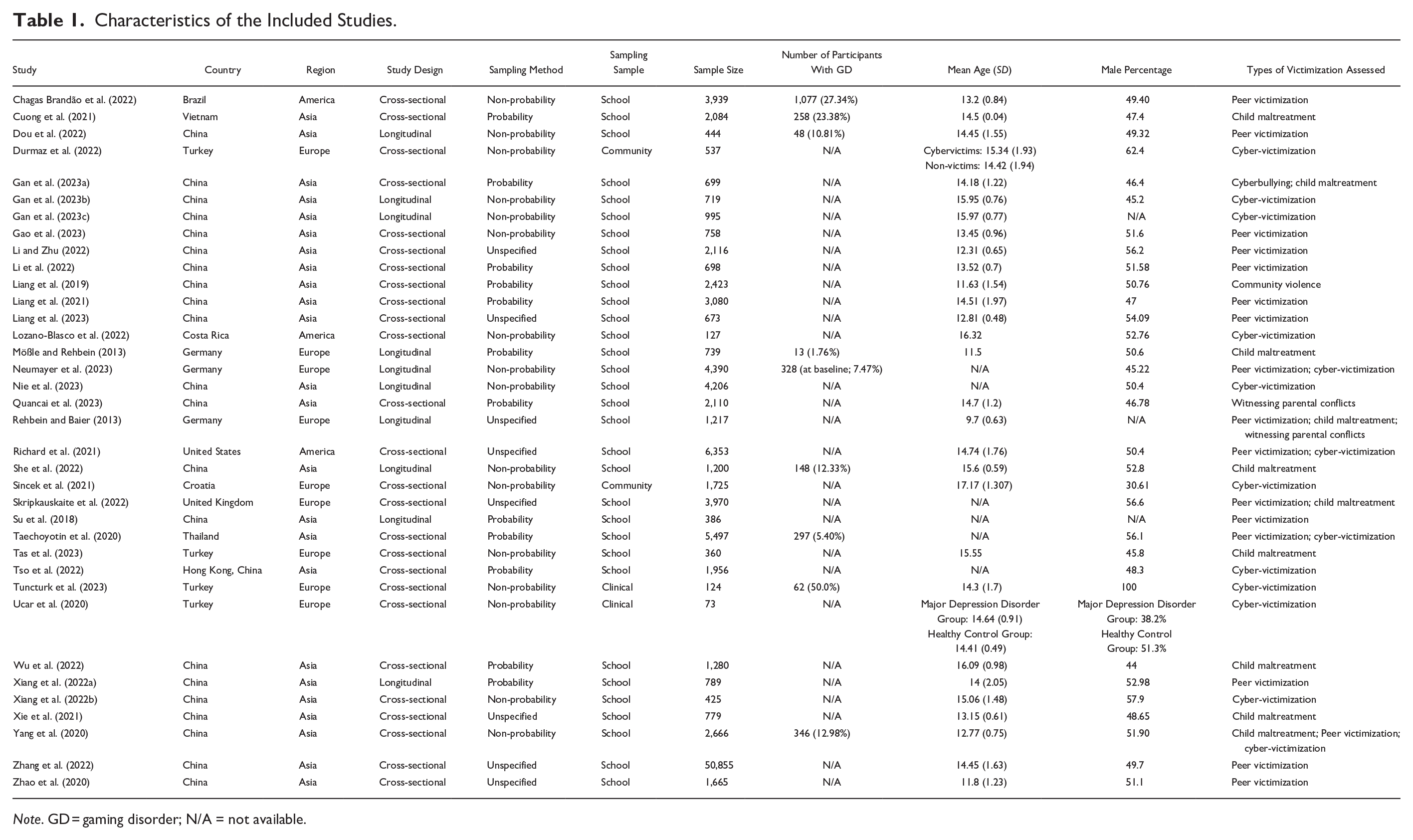
Note. GD = gaming disorder; N/A = not available.
Synthesis of Effect Sizes
The 36 included studies yielded a significant association between overall victimization and GD, with a small effect size (r = .221; 95% CI [0.174, 0.268], p < .001) (Table 2). The heterogeneity test obtained a significant result (Q = 1,499.400, df = 35, p < .001), suggesting a wide spread of variation in the selected studies. I2 statistics indicated that 97.666% of the heterogeneity could be attributed to study variation. Thirty studies reporting continuous data (i.e., correlation and group means and SDs) yielded a similar effect size (r = .224; [0.172, 0.275], p < .001). The pooled effect size based on six studies reporting categorical data (i.e., binary 2 × 2 data) was moderate (OR = 2.434; [1.871, 3.165], p < .001). The forest plots of the effect sizes can be found in Supplemental Appendix 4.
Pooled Effect Sizes of Different Types of Victimization.
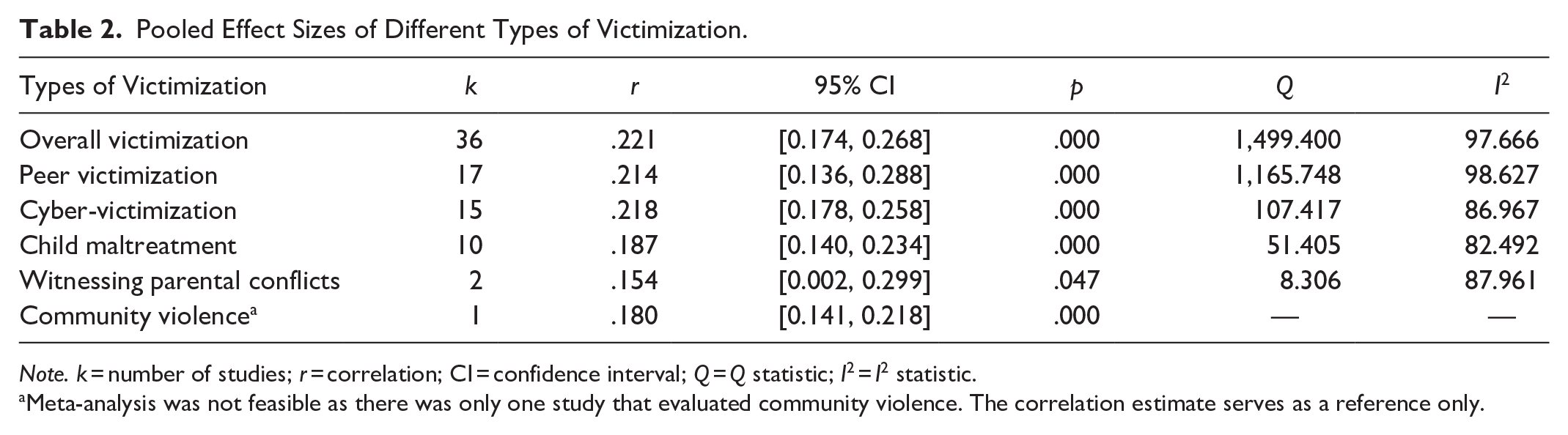
Note. k = number of studies; r = correlation; CI = confidence interval; Q = Q statistic; I2 = I2 statistic.
Meta-analysis was not feasible as there was only one study that evaluated community violence. The correlation estimate serves as a reference only.
We also computed the pooled effect sizes of different types of victimization. Seventeen studies that assessed peer victimization yielded a small effect size (r = .214; 95% CI [0.136, 0.288], p < .001). Fifteen studies examined cyber-victimization, which provided a small effect size (r = .218; [0.178, 0.258], p < .001). A small effect size was also found in the 10 studies that examined child maltreatment (r = .187; [0.140, 0.234], p < .001). The two studies that examined witnessing parental conflicts (r = .154; [0.002, 0.299], p = .047) and the study focusing on community violence (r = .180; [0.141, 0.218], p < .001) likewise yielded small effect sizes.
Moderator Analyses
Moderator analyses of factors that could influence the association between child victimization and GD were conducted. As shown in Table 3, study design (Qb = 5.584, df = 1, p = .018) was found to be a significant moderator, with a slightly larger pooled effect size for cross-sectional studies (r = .245; 95% CI [0.188, 0.300]) than longitudinal studies (r = .169; [0.142, 0.207]). Study sample (Qb = 13.246, df = 2, p = .001) also significantly moderated the relationship between child victimization and GD, in which clinical samples (r = .468; [0.328, 0.588]) yield a larger pooled effect, compared to school (r = .217; [0.167, 0.266]) and community (r = .155; [0.066, 0.241]) samples. The results on other moderators, including study region, male percentage, sampling method, participant mean age, and study quality score, were non-significant.
Moderator Analyses.
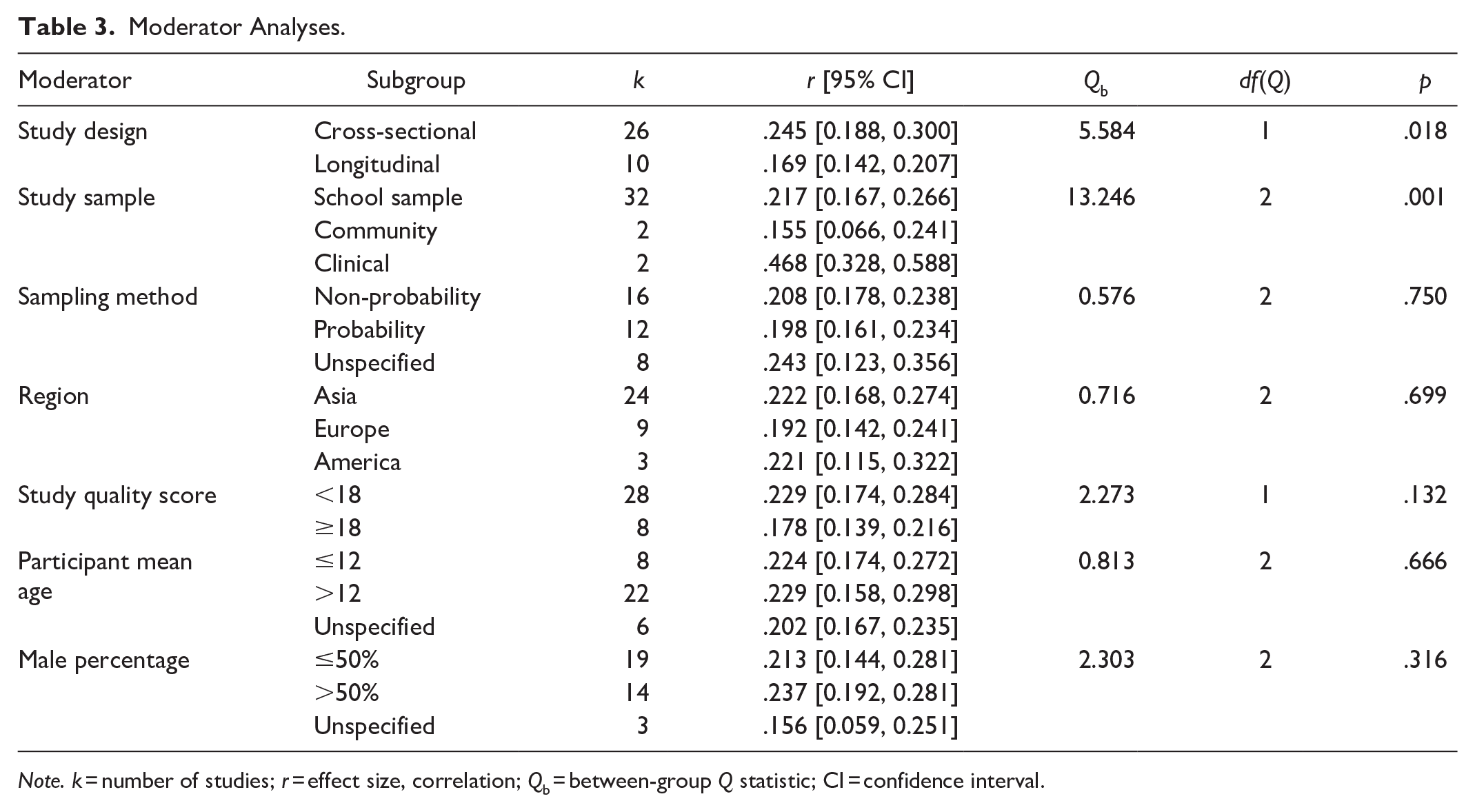
Note. k = number of studies; r = effect size, correlation; Qb = between-group Q statistic; CI = confidence interval.
Publication Bias
Potential publication bias was examined using a funnel plot and Egger’s test. Figure 2 illustrates the distribution of the effect sizes of the selected studies. The distribution of the studies was slightly asymmetrical, indicating potential publication bias. The Egger’s test was significant (p < .001), which also indicates the presence of publication bias. The Duval and Tweedie’s trim-and-fill method estimated that it took six studies for the funnel to be symmetrical. Figure 3 illustrates the funnel plot with the additional imputed studies (on the right of the plot). The adjusted pooled effect size after imputing the missing study remains significant (r = .247, 95% CI [0.206, 0.288]).
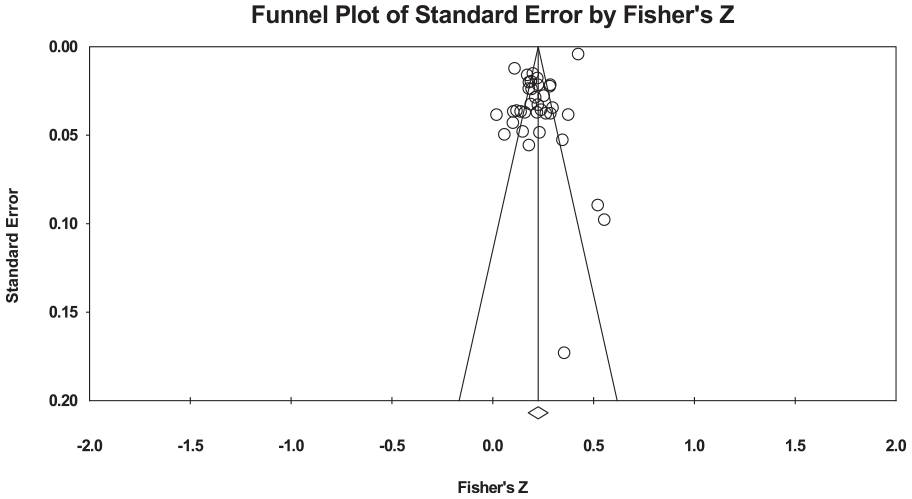
Funnel plot showing the distribution of the included studies.
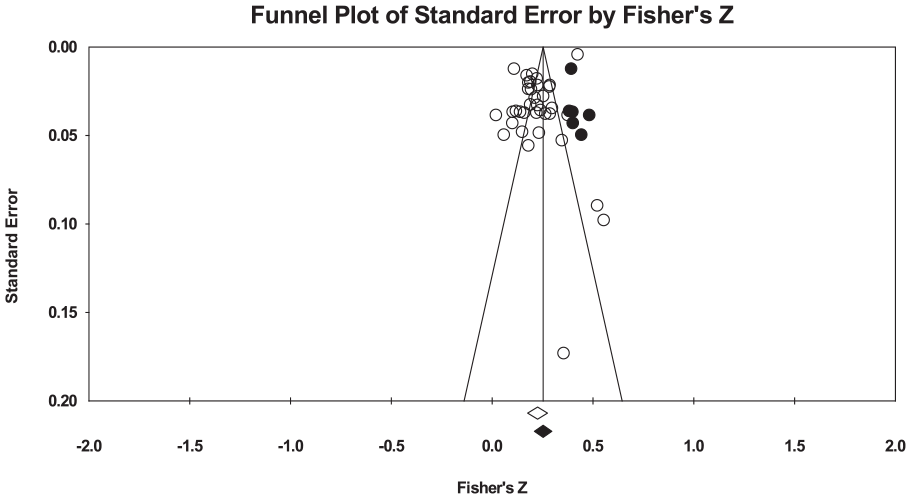
Funnel plot showing the distribution of the included studies and the imputed studies by the trim-and-fill method.
Discussion
This meta-analytic review is the first to provide a comprehensive evaluation of the associations between different types of victimization and GD in children and adolescents. A total of 36 studies met the eligibility criteria, yielding a significant positive association between overall victimization and GD with a small effect size (Table 4). When separated analyses were conducted for different data types, a larger effect size (OR = 2.434) was pooled from the studies that measured victimization and GD as dichotomous variables (i.e., measuring presence or absence of victimization and GD) than from those that employed continuous measures of victimization and GD (r = .224). To understand which type of victimization may have a larger impact on GD, we stratified the results by victimization type (peer victimization, cyber-victimization, child maltreatment, community violence, and witnessing family violence). We observed that all types of victimization were significantly associated with GD with small effect sizes. This suggests that children and adolescents who experience any form of victimization are at a higher risk for the development of GD. Contrary to our hypotheses, no significant moderating effect of study region, gender, and age was identified, implying that the strength of the relationship between child victimization and GD may be relatively stable in these variables.
Critical Findings.

Overall, the significant associations between different types of victimization and GD are consistent with findings from the existing literature, in which peer victimization, cyber-victimization, and child maltreatment are found to be positively related to other addiction problems, such as substance use (Afifi et al., 2020; Halpern et al., 2018), problem gambling (Lane et al., 2016), and Internet addiction (Zhang et al., 2024). Taken together, findings from previous studies and the current one support the Syndrome Model of Addiction (Shaffer et al., 2004), which posits that different types of addiction have common underlying etiological factors. This conceptualization also aligns with the idea that child victimization may be a transdiagnostic risk factor for addiction and other mental health problems (Forbeset al., 2020; Konzok et al., 2025). In light of the comparable effect sizes for the various types of victimization, the mechanisms underlying their associations with GD may be similar, such as engaging in the behavior as a way to self-regulate painful experiences arising from emotional and relational difficulties (Khantzian, 1987, 1997). Children and adolescents are prone to mental health symptoms, including addictive behaviors as they tend to have less developed emotion regulation capacities (Silvers, 2022). Victimization will put them at even higher risk as victimization has negative impacts on emotion regulation and processing (McLaughlin et al., 2020). Hence, the link between victimization and GD is of particular importance to this age group. Taken together, the complex interplay between victimization and GD, and the mounting psychosocial consequences associated with both issues highlight the need to reduce their prevalence and support the victims. Although the effect sizes for the relationship between victimization and GD found were small, the implications for children’s and adolescents’ health are profound and thus developing effective prevention and intervention strategies would be beneficial.
Study sample and study design were the only two significant moderators identified for the association between victimization and GD. Previous studies suggested that due to the sensitive nature of the study topic, it may be difficult to effectively measure victimization (e.g., bullying) via self-report school surveys (Schneider et al., 2017), and social desirability is a particular concern for self-report maltreatment and violence (Fitton et al., 2020), which may lead to underreporting of victimization and hence smaller effect sizes among school and community samples. Conversely, clinical samples included participants with psychiatric comorbidities such as major depressive disorder, social anxiety disorder, and attention-deficit/hyperactivity disorder, which have been consistently reported as significant risk factors for GD among adolescents (Gao et al., 2022), thereby contributing to a stronger relationship between victimization and GD. Regarding study design, we found that the pooled effect size for cross-sectional studies was slightly higher than that of longitudinal studies. It may be possible that there are factors such as brain maturation (Schettleret al., 2022) that influence GD over time in longitudinal studies, resulting in diminished effects compared to immediate associations captured in cross-sectional studies.
On the other hand, the review failed to find significant moderating effects of study quality assessment and sampling method, gender, age, and study region. While some previous meta-analytic studies found that studies with more rigorous study design and methodology tend to show larger effect sizes (e.g., Matjasko et al., 2012; Petersen-Brown et al., 2019), the current meta-analysis showed no differences in effect sizes obtained from studies with higher quality assessment scores and probability sampling. Similarly, another review study suggested that the moderating effects of the rigor and sampling method of the study may be dependent on the outcome variables (Bruner et al., 2023). As with other addictions, males are more vulnerable to developing GD than females (Lopez-Fernandez, Williams, & Kuss, 2019). Previous literature also identified gender differences in potential risk factors for the development and maintenance of GD (Dong & Potenza, 2022). Nevertheless, this gender difference did not translate to the relationship between victimization and GD, potentially suggesting that victimization may be a universal risk factor for boys and girls. Additionally, participants’ age did not moderate the association, suggesting that children and adolescents are equally affected by victimization. Lastly, although the moderating effect of study region was non-significant, it is important to note that there was an over-representation of study participants from Asian countries and regions (N = 88,503 of 112,057; 78.98%), especially from China (N = 80,922 of 112,057; 72.22%). Such imbalance of geographical distribution of studies may lead to biased results. The Chinese government’s stance on the issue of GD may explain why Chinese studies are over-represented. China is one of the first countries to have implemented regulatory measure to limit children and adolescents’ gaming duration (The State Council of the People’s Republic of China, 2021). The concerns of policymakers may have led to substantial growth of research to examine factors associated with GD to inform prevention and intervention strategies in China. From a cultural perspective, individuals’ individualism–collectivism orientation may affect their motives to engage in gaming and their presentation of GD symptoms (Cheng et al., 2018; Stavropoulos et al., 2021). More attention should be dedicated to investigating the role of culture in understanding its influence on the relationship between child victimization and GD. A culturally comparative lens may illuminate how cultural dimensions, such as collectivism versus individualism, interact with victimization and GD development, thereby addressing the contextual gaps in this evolving field of study.
Limitations of the Study
The findings of the study should be interpreted with the consideration of its limitations and the potential publication bias. First, the findings might have been impacted by the discrepancies in conceptualization and measurement of victimization and GD among the selected studies. The reference periods for victimization and GD varied between studies (e.g., past week vs. past month vs. past year vs. unspecified). It may be possible that more recent victimization will associate with GD more strongly than victimization that occurred longer time ago. However, due to the insufficient number of included studies, we were unable to conduct separate analyses for different reference periods. Relatedly, the study’s results may have been influenced by the types of data reported in the selected studies. We pooled a moderate effect size (OR = 2.434) from studies reporting categorical data (i.e., victimization or GD was dichotomized into presence or absence); and a small effect size (r = .224) from studies reporting continuous data. While there are strengths of such dichotomization, such as allowing an easy and practical interpretation of results, such approach is unable to take into consideration of the severity of victimization/GD. The pooled effect size yielded from these studies may be overestimated. Furthermore, similar to one of the limitations of current research on child victimization, the selected studies tended to focus on separate, relatively narrow categories of victimization without taking into consideration the potential contribution of other unmeasured types of victimization to GD, thus running the risk of overestimating the relationships between specific forms of victimization and GD (H. A. Turner et al., 2010). Although we attempted to provide a more comprehensive evaluation of the associations between different types of child victimization and GD in this review, the methodological limitations of the selected studies prevent the identification of the independent, unique contribution of each type of victimization to GD (Renner et al., 2020). Additionally, although this study conceptualizes victimization as a factor contributing to GD, the findings were derived from a mixture of cross-sectional and longitudinal studies, and the causal relationship between victimization and GD remains unclear. It is also possible that GD will elevate adolescents’ risk for experiencing victimization. Fifteen studies met the eligibility criteria of this review but were not included in the final analysis due to insufficient data, despite our efforts to contact the corresponding authors for the data required. It may be that the inclusion of these studies will influence the results of the analyses. Moreover, there are only a small number of studies examining children’s exposure to community violence and witnessing family violence; therefore, the effect sizes derived from the small subset of studies may be biased. Given the insufficient data on subtypes of victimization, such as child physical abuse, neglect, psychological abuse, and sexual abuse in child maltreatment, our analyses were limited to the global measures of different types of victimization. Despite these limitations, this review provides a comprehensive review and synthesis of current evidence on the topic, which serves as important reference for future research.
Implications for Research, Practice, and Policy
The findings of this meta-analysis provide important implications for future research, practice, and policy (Table 5). Previous research tended to focus on specific types of victimization without obtaining complete victimization profiles of children (Finkelhor et al., 2007). This narrow focus may exaggerate the impact of a single type of victimization to children’s outcomes, as it fails to account for the potential influence of other types of victimization in the analysis. Hence, future research should assess multiple types of victimization simultaneously to disentangle the independent contribution of different types of child victimization to the development of GD. Given the consistent dose–response relationship found in the associations between victimization and health outcomes (Evans et al., 2014; S. Turner et al., 2018), it is important to expand the scope to investigate whether GD is more impacted by multiple types of victimization, that is, child poly-victimization (Finkelhor et al., 2011) and family poly-victimization (Chan, 2017). Additionally, our findings on the study heterogeneity suggest that more studies are needed to examine how the effects of victimization on GD may vary across different developmental stages, cultures, severity and duration of violence exposure, and the co-occurrence of victimization. This nuanced understanding will help identify factors that differentiate susceptibility to GD following victimization. More importantly, the next step is to investigate the mechanisms underlying the association between victimization and GD, as well as to determine whether the mechanisms differ by types of victimization and across various study samples, to shed light on the specific pathways through which victimization influences the development and maintenance of GD. Based on the review of the study design and measurements used in the included studies, the use of consistent measurements accounting for the level of severity of victimization and GD and longitudinal designs, and the inclusion of confounding variables are recommended to fully elucidate the effects of victimization on GD. Furthermore, most of the included studies were conducted in China, and more studies from other cultural contexts are needed to verify the generalizability of the study’s findings.
Summary of Implications for Practice, Policy, and Research.
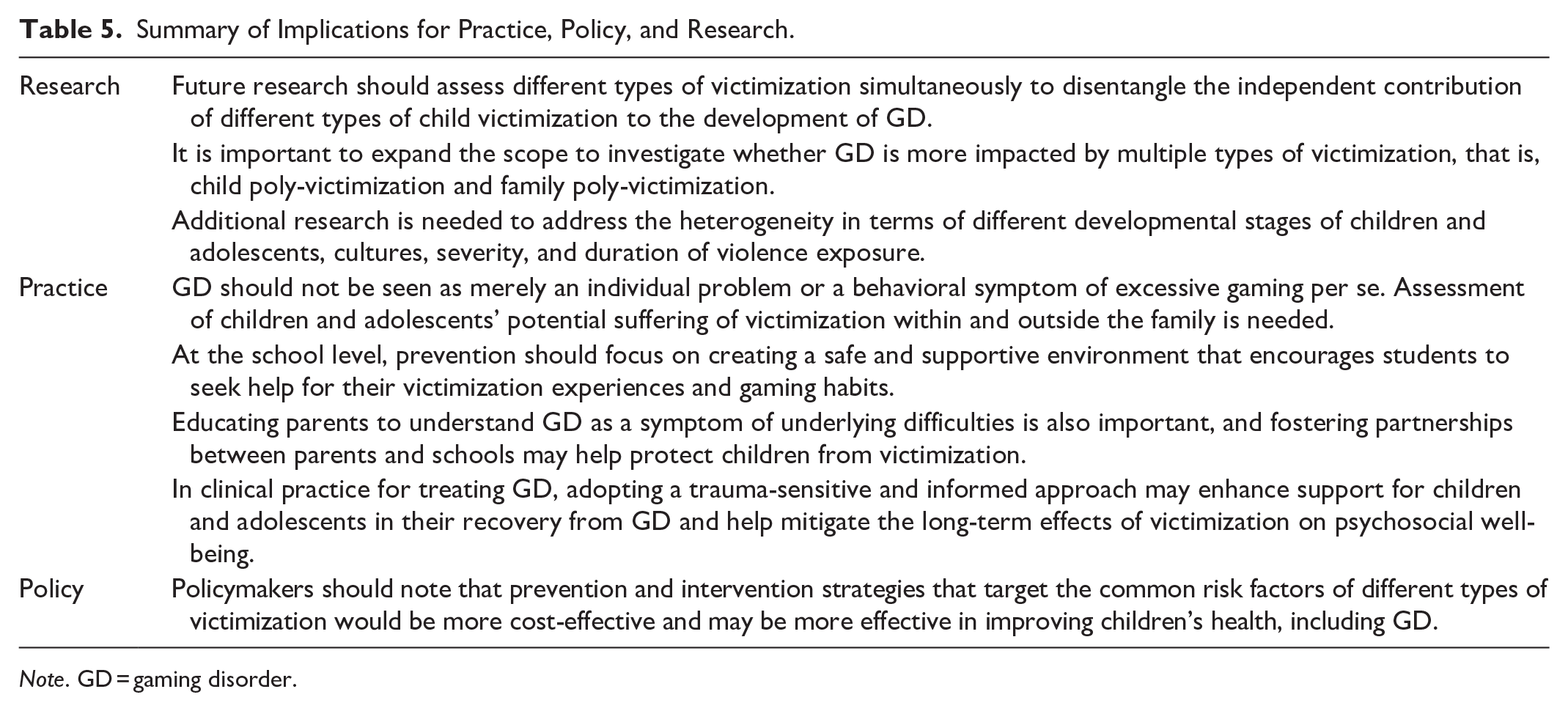
Note. GD = gaming disorder.
Existing efforts to prevent and intervene GD often focus on individuals (Lo et al., 2023), such as addressing their cognitions and emotions associated with gaming. Given the significant associations found in this study between different types of victimization and GD, preventing victimization is critical for protecting children and adolescents from GD. Therefore, in addition to recommending parents to limit their children’s gaming time, policymakers may consider expanding preventive measures to address external factors, such as victimization in different social contexts. The results of this review support an integrated preventive approach. Instead of relying on stand-alone programs that target specific types of victimization or treat different mental health problems as separate issues, policymakers should note that prevention and intervention strategies focused on common risk factors for various types of victimization may be more cost-effective and more effective in improving children’s health, including GD and potentially other types of addiction problems.
At the school level, educators and school counselors should go beyond viewing students’ symptoms of GD as merely individual problems or as behavioral symptoms of excessive gaming. It is crucial to assess whether students are experiencing victimization both within and outside their families. Prevention should focus on creating a safe and supportive environment that encourages students to seek help for their victimization experiences and gaming habits. Additionally, promoting social-emotional learning may equip students with protective factors against GD and victimization, including effective emotion regulation strategies and resilience. Educating parents to understand GD as a symptom of underlying difficulties is also important, and fostering partnerships between parents and schools may help protect children from victimization.
In clinical practice for treating GD, adopting a trauma-sensitive and informed approach may enhance support for children and adolescents in their recovery from GD and help mitigate the long-term effects of victimization on psychosocial well-being. Since the association between victimization and GD is stronger in clinical samples, professionals working with this population should pay closer attention to adolescents’ experiences of victimization and provide additional support.
Supplemental Material
sj-docx-1-tva-10.1177_15248380251349781 – Supplemental material for Associations Between Different Types of Child Victimization and Gaming Disorder in Children and Adolescents: A Meta-Analysis
Supplemental material, sj-docx-1-tva-10.1177_15248380251349781 for Associations Between Different Types of Child Victimization and Gaming Disorder in Children and Adolescents: A Meta-Analysis by Camilla K.M. Lo, Yuet Wing Cho, Qiqi Chen and Ko Ling Chan in Trauma, Violence, & Abuse
Footnotes
Author Contributions
C.K.M.L.: conceptualization, methodology, systematic search, review of articles, writing—original draft, writing—review & editing, formal analysis, funding acquisition; Y.W.C.: review of articles, writing—original draft; writing—review & editing; Q.C.: writing—review & editing; K.L.C.: writing—review & editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work described in this paper was supported by a grant from The Hong Kong Polytechnic University.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.