
Abstract
Reproductive coercion and abuse (RCA) refers to deliberate behaviors that undermine an individual’s reproductive decisions, such as sabotaging contraception or pressuring someone to continue or end a pregnancy. Recent legislative changes, such as the Dobbs v. Jackson Women’s Health Organization decision, highlight the timeliness of understanding how RCA manifests in the United States. We conducted a systematic review to synthesize and critically assess evidence on the prevalence of RCA and associated factors in the United States. Following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, we searched PubMed, Embase, CINAHL, PsycINFO, and Web of Science for quantitative studies published in English through April 2024. Risk of bias was assessed using Joanna Briggs Institute’s Critical Appraisal Tools. Twenty-three cross-sectional studies were included. Lifetime prevalence of RCA ranged from 7.8% to 37.8%. Prevalence of birth control sabotage ranged from 1.1% to 25.3%, while pregnancy coercion ranged from 6.4% to 19%. Most studies identified a strong association between RCA and intimate partner violence. Several studies also reported associations with age, race, ethnicity, and number of sexual partners, though findings were mixed. Evidence related to socioeconomic status, health behaviors, and partner characteristics was limited. All studies were rated as having a moderate or high risk of bias, as many failed to assess intent or use validated instruments to measure RCA. These limitations raise concerns about the trustworthiness and interpretability of findings. Future studies should examine conceptual clarity and measurement of RCA to improve data quality and inform evidence-based interventions, clinical screening practices, and policy efforts.
Background
Reproductive coercion refers to deliberate behaviors that undermine an individual’s reproductive decisions with the intent to promote or prevent pregnancy (Tarzia & Hegarty, 2021). First conceptualized by Miller et al. (2010) as a form of intimate partner violence (IPV), reproductive coercion manifests through three main forms: birth control sabotage, pregnancy coercion, and controlling the outcome of a pregnancy (Grace & Anderson, 2018; Miller et al., 2010; Tarzia & Hegarty, 2021). Birth control sabotage includes removing or damaging condoms, hiding birth control pills, and preventing access to family planning services (Miller et al., 2010). Pregnancy coercion involves threats or acts of violence to pressure someone to become pregnant (Miller et al., 2010), while controlling the outcome of a pregnancy involves coercing a partner to continue or end a pregnancy against their wishes (Grace & Anderson, 2018). While reproductive coercion may involve physical, sexual, or psychological abuse, its distinguishing feature is the intent to control reproductive outcomes (Tarzia & Hegarty, 2021).
Previous reviews have examined the conceptualization, prevalence, health outcomes, and lived experiences of reproductive coercion (Fay & Yee, 2018; Grace & Anderson, 2018; Grace & Fleming, 2016; Graham et al., 2023; Moulton et al., 2021; Rowlands & Walker, 2019; Tarzia & Hegarty, 2021). These reviews highlight the disproportionate impact of reproductive coercion among younger women, individuals in unstable relationships, and those with lower socioeconomic status (Grace & Anderson, 2018) and underscore the role of inequalities and family pressure in its perpetuation (Grace & Fleming, 2016; Graham et al., 2023; Moulton et al., 2021).
Among these reviews, Tarzia and Hegarty (2021) proposed a reconceptualization of reproductive coercion as “reproductive coercion and abuse” (RCA) to center fear, control, and intent as defining elements of the phenomenon. A key contribution of their framework is the focus on intentional behaviors that promote or prevent pregnancy, marking a shift from earlier studies that emphasized outcomes (Miller et al., 2010). This distinction is critical for measurement, as failing to assess intent can conflate RCA with other forms of abuse. Tarzia and Hegarty (2021) also emphasize the importance of measuring pregnancy-promoting and pregnancy-preventing behaviors. This reconceptualization, along with the validation of the Reproductive Coercion Scale (McCauley et al., 2017), highlights the need for an updated review. The remainder of this review will use the term RCA.
While previous reviews have included studies across global contexts (Fay & Yee, 2018; Grace & Fleming, 2016; Graham et al., 2023; Moulton et al., 2021; Rowlands & Walker, 2019), these have limited our understanding of the prevalence and factors associated with RCA in the United States. This is a critical gap in knowledge, as reproductive autonomy in the United States is increasingly constrained by legal and health system environments that differ significantly from those in other high-income countries. The U.S. reproductive health landscape is uniquely fragmented, with significant state-level variation in access to family planning services (Forouzan & Guarnieri, 2023) and long-standing racial and ethnic disparities in sexual and reproductive health outcomes (Sutton et al., 2021). Moreover, Dobbs v. Jackson Women’s Health Organization decision which removed the constitutional right to end a pregnancy, has led to a twofold increase in reports of RCA in the United States (Gerson, 2023). This stark increase highlights the timeliness of understanding the factors associated with RCA to inform research, clinical practice, and policy. Therefore, we conducted a systematic review to synthesize and critically assess existing evidence on RCA prevalence and associated factors in the United States.
Methods
This systematic review adheres to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page et al., 2021).
Data Sources and Search Strategy
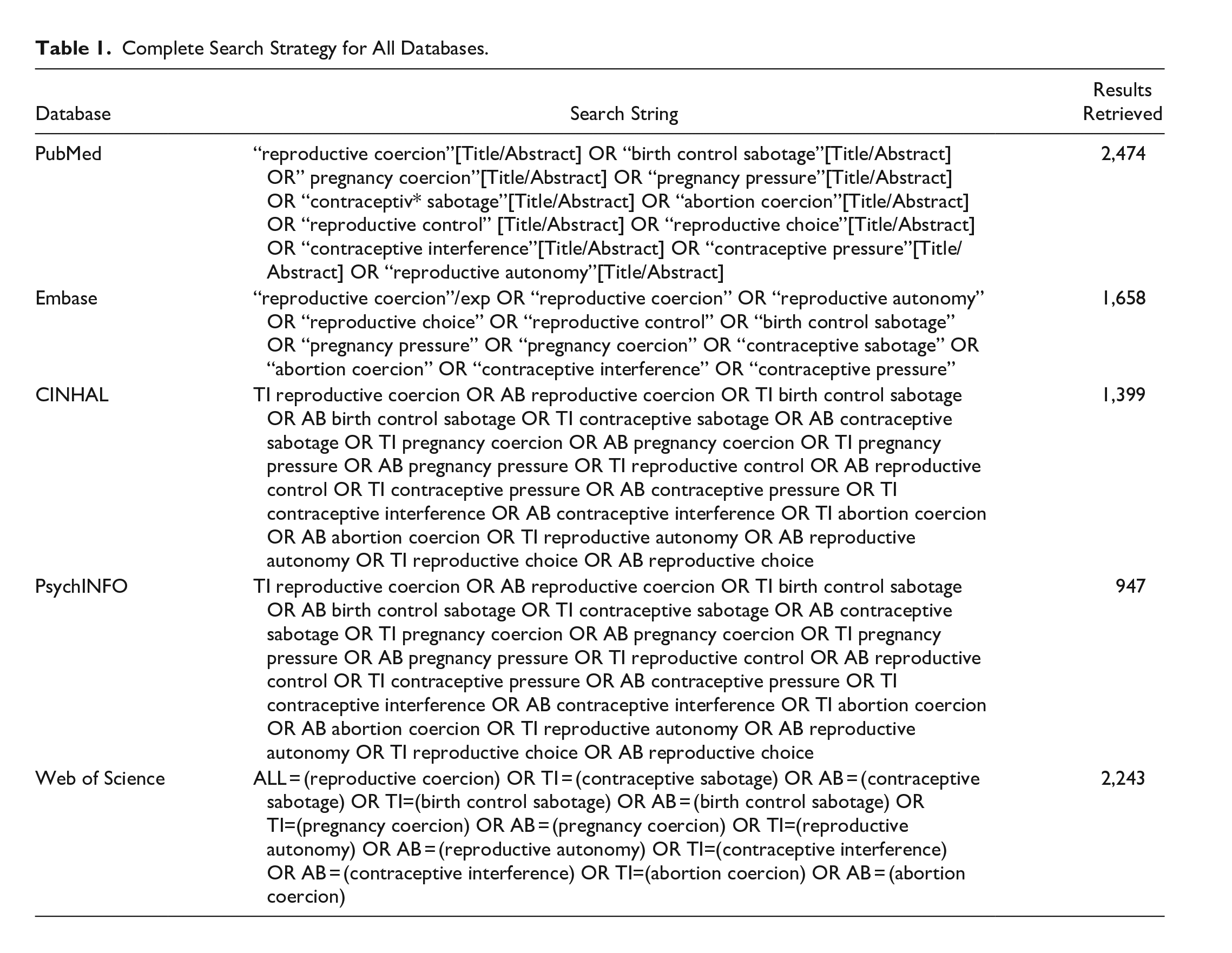
On April 4, 2024, we conducted a systematic search in five databases: PubMed, Embase, CINAHL, PsychInfo, and Web of Science. Before execution, a library information specialist reviewed the search strategy for robustness and accuracy. Our search was limited to English-language articles, with no date restrictions. Key RCA-related terms were combined using “OR” and “AND” in each database to identify relevant literature (Table 1).
Complete Search Strategy for All Databases.
Study Selection
Covidence software was used to manage study selection. Three authors (ALH, SEH, and SM) independently screened titles and abstracts against inclusion and exclusion criteria, followed by full-text review. Conflicts were discussed at weekly team meetings, and resolutions were reached by consensus. Included studies had to (a) examine RCA as an outcome, (b) assess at least one associated factor (e.g., demographics), (c) be original research in a peer-reviewed journal, (d) be published in English, and (e) be conducted in the United States. Any measure of RCA was eligible, and both nonexperimental and experimental study designs were included. Qualitative studies, clinical guidelines, protocol papers, abstracts, conference proceedings, and review articles were excluded. Given the distinct reproductive rights landscape in the United States, we excluded studies conducted elsewhere to enhance the transferability of findings to domestic research, clinical practice, and policy efforts.
Study Risk of Bias Assessment
All included studies used a cross-sectional design and were assessed using the Joanna Briggs Institute’s (JBI) Critical Appraisal Checklist for Analytical Cross-Sectional Studies (Moola et al., 2020). This eight-item checklist evaluates sampling methods, measurement of variables, handling of confounders, and statistical analyses (Moola et al., 2020). Each item was rated as “yes,” “no,” “unclear,” or “not applicable.” Although the JBI tool lacks a formal scoring system, we categorized studies as having low (6–8), moderate (4–5), or high (0–3) risk of bias based on the number of “yes” ratings.
Additional consideration was given to Items 4 and 7, which evaluated how RCA was defined and measured. For Item 4, we assessed whether each study used objective, standard criteria to define RCA, specifically, whether the measure incorporated one or more central elements such as fear, control, or intent (Tarzia & Hegarty, 2021). For item 7, we assessed whether RCA was measured using a psychometrically validated instrument. Studies were considered at an increased risk of bias if either item received a “no” or “unclear” rating. Because of their relevance to the trustworthiness of findings, these items were prioritized when determining the overall risk of bias. Three authors (ALH, SEH, and SM) independently assessed all studies, with discrepancies resolved through discussion. No studies were excluded based on the risk of bias assessment.
Data Extraction and Synthesis
Three authors (ALH, SEH, and SM) independently extracted all data, which was cross-checked for consistency. Disagreements were resolved through discussion. For each study, we extracted the author, year of publication, study design, study purpose, study setting, geographic location, sample, measurement tools, and study findings. We used Microsoft Excel to organize and summarize data in tables to identify patterns and facilitate data synthesis. A meta-analysis was not conducted due to heterogeneity in study populations and RCA measures.
Results
Search Results
Figure 1 shows the PRISMA flow diagram summarizing the study selection process. After removing duplicates, we screened 6,028 titles and abstracts and reviewed 145 full-text articles. Ultimately, 23 studies were included in the review (Alexander et al., 2021; Amos et al., 2023; Bagwell-Gray et al., 2021; Clark et al., 2014; Fay & Yee, 2020; Grace, Decker, et al., 2022, 2023; Grace, Holliday, et al., 2023; Grace, Perrin, et al., 2022; Hayes et al., 2023; Hill et al., 2019; Huslage et al., 2023; Katz & Sutherland, 2020; Katz et al., 2017; Kraft et al., 2021; Miller et al., 2010; Muñoz et al., 2023; Phillips et al., 2016; Rosenfeld et al., 2018; Samankasikorn et al., 2019; Sutherland et al., 2015; Swan et al., 2023; Willie et al., 2021).
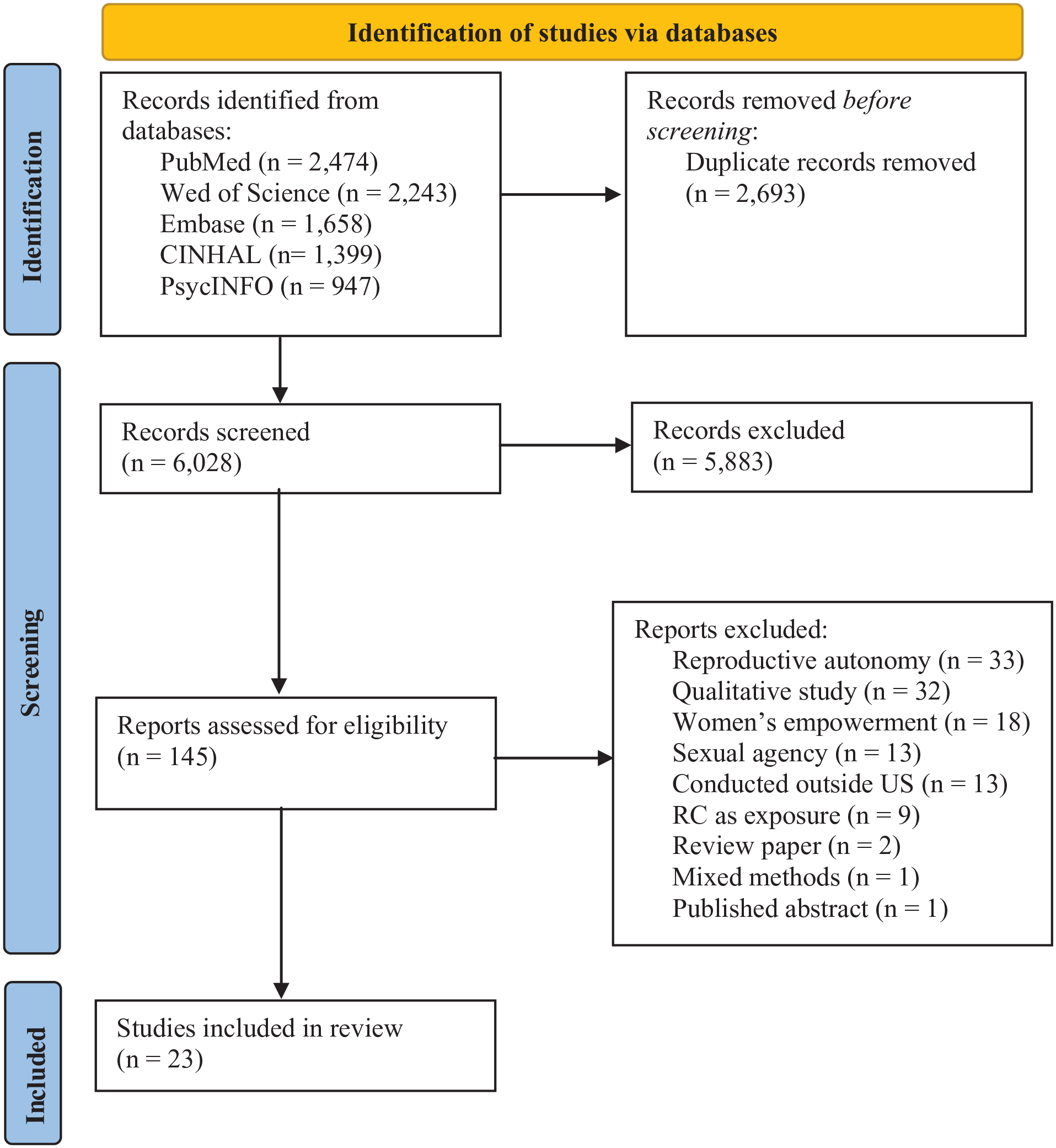
PRISMA flow diagram.
Study and Sample Characteristics
All included studies (N = 23) were cross-sectional and published between 2010 and 2023. Most participants were women, sampled from clinics (n = 7), colleges (n = 7), community settings (n = 4), high schools (n = 2), and national datasets (n = 3). Sample sizes ranged from 70 (Grace, Holliday, et al., 2023) to 20,252 participants (Samankasikorn et al., 2019), and mean participant age ranged from 17.34 years (Kraft et al., 2021) to 37 years (Bagwell-Gray et al., 2021). Additional details on each study’s purpose, geographic location, and sample demographics are presented in Tables 2 and 3.
Study Characteristics of Included Studies.
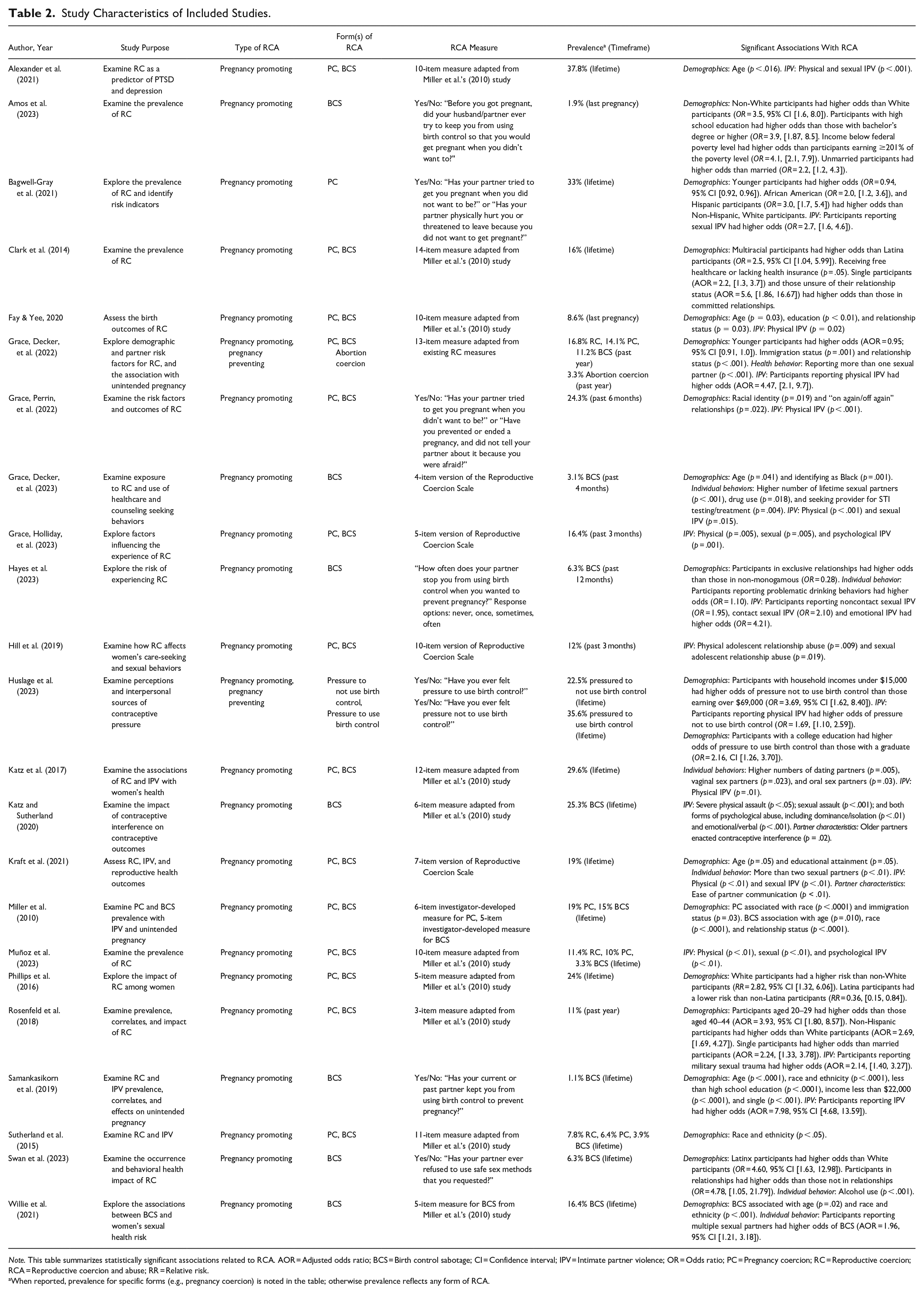
Note. This table summarizes statistically significant associations related to RCA. AOR = Adjusted odds ratio; BCS = Birth control sabotage; CI = Confidence interval; IPV = Intimate partner violence; OR = Odds ratio; PC = Pregnancy coercion; RC = Reproductive coercion; RCA = Reproductive coercion and abuse; RR = Relative risk.
When reported, prevalence for specific forms (e.g., pregnancy coercion) is noted in the table; otherwise prevalence reflects any form of RCA.
Sample Characteristics of Included Studies.
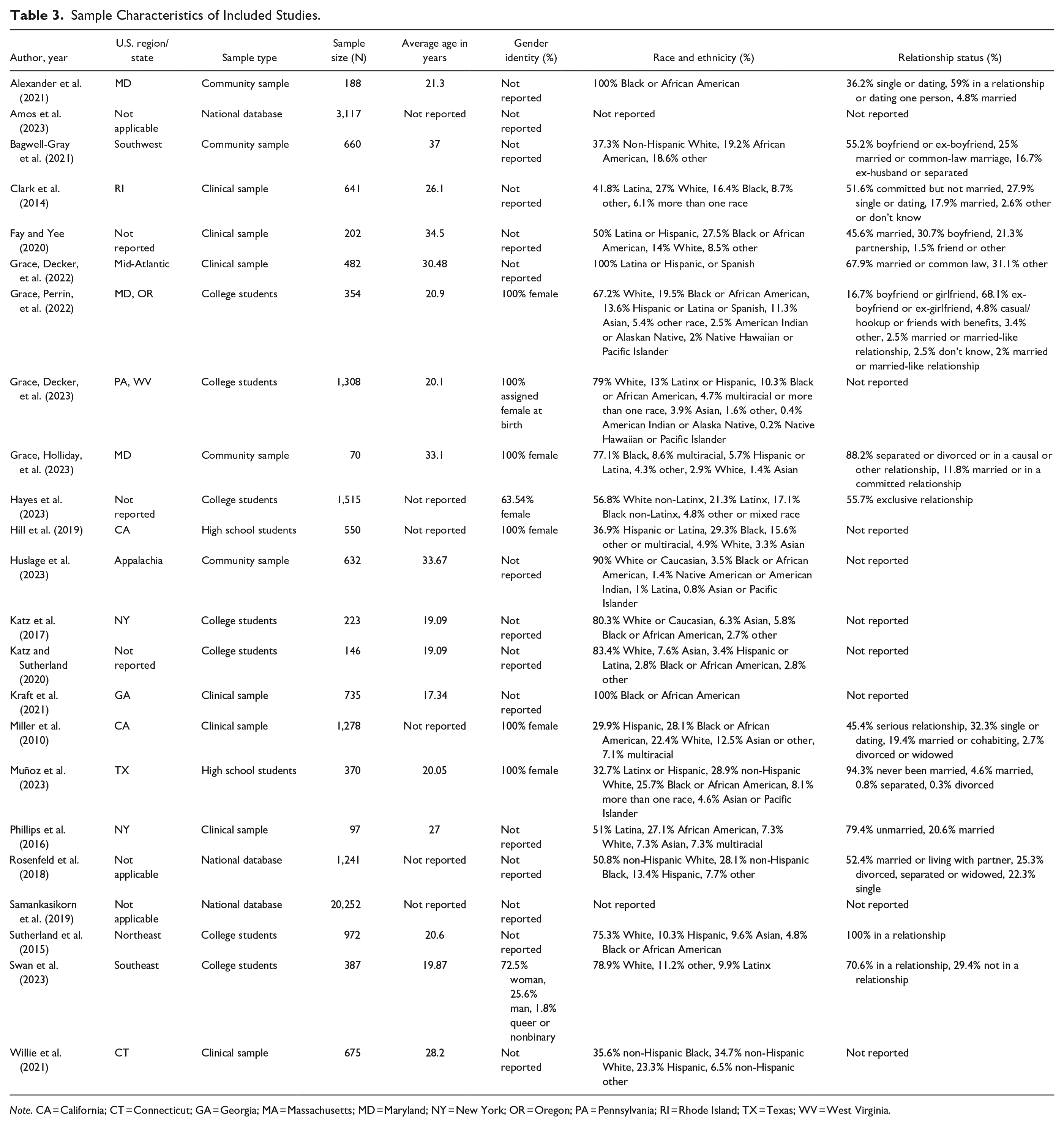
Note. CA = California; CT = Connecticut; GA = Georgia; MA = Massachusetts; MD = Maryland; NY = New York; OR = Oregon; PA = Pennsylvania; RI = Rhode Island; TX = Texas; WV = West Virginia.
Measurement of RCA
All studies included assessed pregnancy-promoting behaviors. Most measured both birth control sabotage and pregnancy coercion (n = 14), while others focused on birth control sabotage (n = 7), pregnancy coercion (n = 1), or perceived pressure to use birth control (n = 1). Only two studies additionally examined pregnancy-preventing behaviors, including abortion coercion (Grace, Decker, et al., 2022) and perceived pressure to use birth control (Huslage et al., 2023). However, many studies did not assess the underlying intent behind these behaviors, an essential feature that distinguishes RCA from sexual violence and IPV (Tarzia & Hegarty, 2021). Five studies (Fay & Yee, 2020; Grace, Decker, et al., 2022; Katz & Sutherland, 2020; Katz et al., 2017; Swan et al., 2023) did not clearly differentiate intentional pregnancy-promoting behaviors from nonconsensual condom removal, also known as “stealthing” (Davis, 2019). Moreover, four of these studies (Grace, Decker, et al., 2022; Katz & Sutherland, 2020; Katz et al., 2017; Swan et al., 2023) deliberately removed language referencing intent, such as “in order to get you pregnant.”
RCA measures also varied across studies. Eleven studies (Alexander et al., 2021; Clark et al., 2014; Fay & Yee, 2020; Grace, Decker, et al., 2022; Katz & Sutherland, 2020; Katz et al., 2017; Muñoz et al., 2023; Phillips et al., 2016; Rosenfeld et al., 2018; Sutherland et al., 2015; Willie et al., 2021) used or adapted items from the study by Miller et al. (2010), with some modifying the assessment timeframe (e.g., past 3 months vs. lifetime) or changing the number of items. The Reproductive Coercion Scale, developed by McCauley et al. (2017), was used or adapted in four studies (Grace, Decker, et al., 2023; Grace, Holliday, et al., 2023; Kraft et al., 2021; Hill et al., 2019). The remaining assessed RCA using only one or two items (Amos et al., 2023; Bagwell-Gray et al., 2021; Grace, Perrin, et al., 2022; Hayes et al., 2023; Huslage et al., 2023; Samankasikorn et al., 2019; Swan et al., 2023). Table 2 summarizes the type and form of RCA measured and the instrument or item(s) used in each study.
Prevalence of RCA
Reported RCA prevalence ranged across studies, reflecting differences in measurement instruments and timeframes. Reported lifetime prevalence of RCA ranged from 7.8% (Sutherland et al., 2015) to 37.8% (Alexander et al., 2021), while 3-month prevalence ranged from 12% (Hill et al., 2019) to 16.4% (Grace, Holliday, et al., 2023). Prevalence also differed by form of RCA. For example, studies reported lifetime prevalence of birth control sabotage from 1.1% (Samankasikorn et al., 2019) to 25.3% (Katz & Sutherland, 2020), and pregnancy coercion from 6.4% (Sutherland et al., 2015) to 19% (Miller et al., 2010). Some studies reporting the highest prevalence (e.g., Katz & Sutherland, 2020) did not distinguish between nonconsensual condom removal and pregnancy-promoting contraceptive interference, which may have contributed to variability across studies. However, we did not observe any patterns in prevalence based on whether studies assessed for intent or not. Table 2 presents RCA prevalence by study.
Risk of Bias
Of the 23 included studies, 8 studies were rated as having a moderate risk of bias (Alexander et al., 2021; Fay & Yee, 2020; Grace, Holliday, et al., 2023; Hill et al., 2019; Miller et al., 2010; Muñoz et al., 2023; Sutherland et al., 2015; Willie et al., 2021) and 15 studies were rated as having a high risk of bias (Amos et al., 2023; Bagwell-Gray et al., 2021; Clark et al., 2014; Grace, Decker, et al., 2022, 2023; Grace, Perrin, et al., 2022; Hayes et al., 2023; Huslage et al., 2023; Katz & Sutherland, 2020; Katz et al., 2017; Kraft et al., 2021; Phillips et al., 2016; Rosenfeld et al., 2018; Samankasikorn et al., 2019; Swan et al., 2023). No studies were rated as having a low risk of bias (See Table 4 for summary of risk of bias assessment).
Risk of Bias of Included Studies.
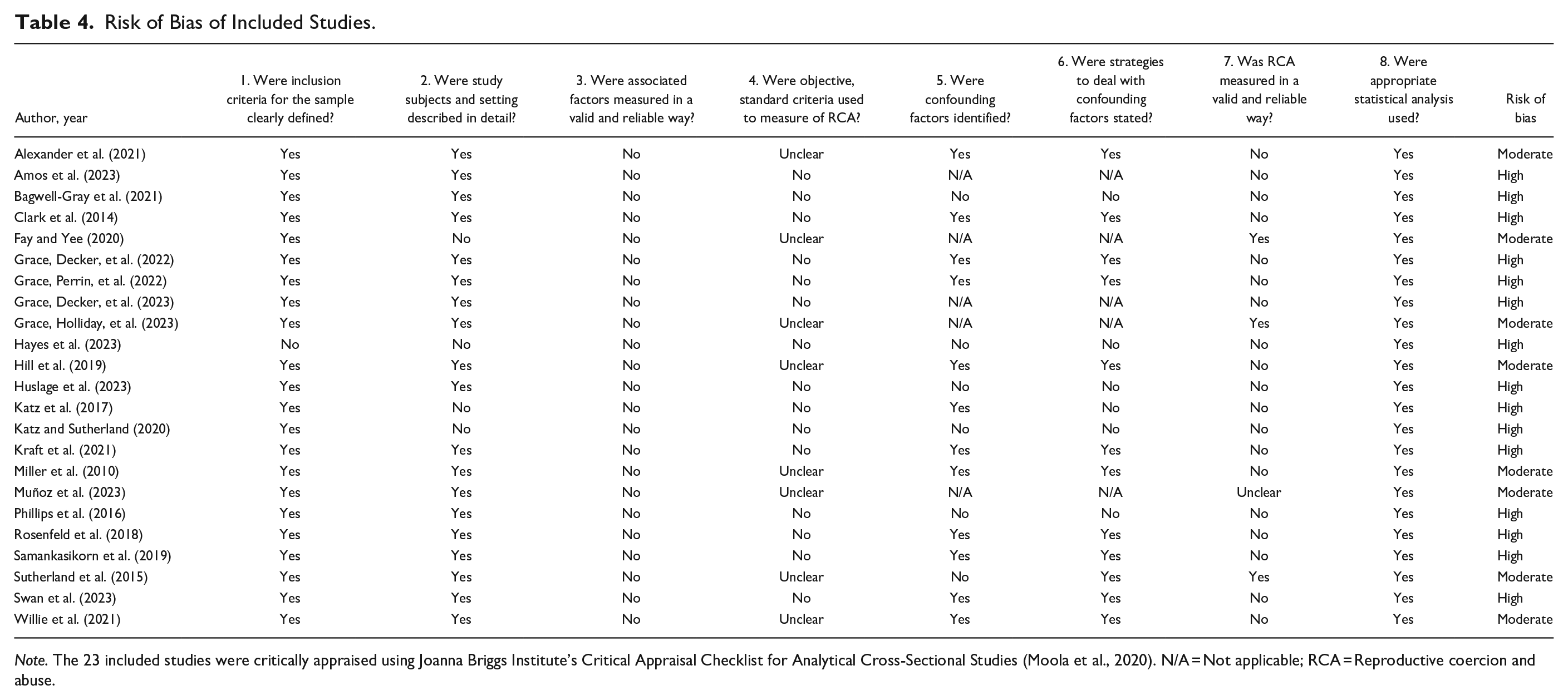
Note. The 23 included studies were critically appraised using Joanna Briggs Institute’s Critical Appraisal Checklist for Analytical Cross-Sectional Studies (Moola et al., 2020). N/A = Not applicable; RCA = Reproductive coercion and abuse.
The most frequently identified source of bias was how RCA was measured. None of the included studies conceptually defined RCA using criteria that fully incorporated its core elements, such as intent, fear, or control (Tarzia & Hegarty, 2021). We rated studies using instruments developed by Miller et al. (2010) and McCauley et al. (2017) as “unclear,” because they treated endorsement of any item as evidence of RCA, even when certain items (e.g., “told you not to use any birth control”) did not explicitly assess intent or lacked context to determine whether the behavior constituted abuse. Most studies either adapted existing RCA instruments or created new items without reporting psychometric testing. These limitations lowered our confidence in the findings and contributed to moderate and high risk of bias ratings.
Other common weaknesses included limited descriptions of confounders and inadequate strategies to address them, as well as concerns about whether associated factors, such as demographic characteristics, were measured in a valid and reliable manner. None of the studies met the criteria for valid or reliable measurement of these factors, which diminished confidence in the associations between these factors and RCA.
Factors Associated With RCA
We organized factors into four categories: (a) Demographic Characteristics (n = 19 studies); (b) Individual Behaviors (n = 10 studies); (c) Physical, Sexual, and Psychological IPV (n = 16 studies); and (d) Partner Characteristics (n = 5 studies). We only report factors with at least one statistically significant association with RCA. Significant findings are summarized in Table 2.
As mentioned, studies differed in how they conceptualized and measured RCA, which limited our ability to explore associations by specific forms of RCA and to differentiate between pregnancy-promoting and pregnancy-preventing behaviors. For example, the one study (Grace, Decker, et al., 2022) that examined abortion coercion treated RCA as a single, homogeneous construct. As a result, a synthesis of associations by RCA type or form was not possible.
Demographic Characteristics
Reported associations between RCA and demographic characteristics were mixed across included studies, as well as risk of bias rating. However, several studies reported higher RCA prevalence among younger participants (Alexander et al., 2021; Bagwell-Gray et al., 2021; Fay & Yee, 2020; Grace, Decker, et al., 2022; Rosenfeld et al., 2018; Samankasikorn et al., 2019), and among Black, Latina, and multiracial women compared to White and non-Hispanic women (Amos et al., 2023; Bagwell-Gray et al., 2021; Clark et al., 2014; Grace, Perrin, et al., 2022; Grace, Decker, et al., 2023; Miller et al., 2010; Rosenfeld et al., 2018; Samankasikorn et al., 2019; Sutherland et al., 2015; Swan et al., 2023; Willie et al., 2021). While most studies found no significant associations between RCA and socioeconomic status, those that did suggest an association were all rated as having a high risk of bias (Amos et al., 2023; Clark et al., 2014; Huslage et al., 2023; Kraft et al., 2021; Rosenfeld et al., 2018; Samankasikorn et al., 2019). One exception was Fay and Yee (2020), a moderate-risk study, which found that participants reporting RCA were less likely to have completed some college. Finally, several studies suggested that single women were more likely to experience RCA than those in relationships or married; however, most of these were rated as having a high risk of bias (Amos et al., 2023; Clark et al., 2014; Grace, Decker, et al., 2022; Grace, Perrin, et al., 2022; Hayes et al., 2023; Rosenfeld et al., 2018; Samankasikorn et al., 2019).
Individual Behaviors
Several studies found an association between having a higher number of sexual partners and RCA; however, all but one (Willie et al., 2021) were rated as having a high risk of bias (Grace, Decker, et al., 2022; Grace & Miller, 2023; Katz et al., 2017; Kraft et al., 2021). Most studies reported no association between alcohol use, binge drinking, and RCA (Grace, Decker, et al., 2022, 2023; Hayes et al., 2023); however, all received a high risk of bias rating. Findings on health-seeking behaviors and RCA were inconclusive.
Physical, Sexual, and Psychological Abuse
Studies consistently showed that RCA co-occurs with physical, sexual, and psychological forms of IPV, regardless of risk of bias rating. Thirteen studies (Alexander et al., 2021; Fay & Yee, 2020; (Grace, Decker, et al., 2022); Grace, Perrin, et al., 2022; Grace, Decker, et al., 2023; Grace, Holliday, et al., 2023; Hill et al., 2019; Huslage et al., 2023; Katz & Sutherland, 2020; Katz et al., 2017; Kraft et al., 2021; Muñoz et al., 2023; Samankasikorn et al., 2019) reported a significant association between RCA and physical IPV, defined as direct acts of physical aggression by a partner, such as hitting, slapping, punching, or kicking. Notably, the only two studies that did not find this association received high risk of bias ratings (Hayes et al., 2023; Phillips et al., 2016).
Ten studies (Alexander et al., 2021; Bagwell-Gray et al., 2021; Grace, Decker, et al., 2023; Grace, Holliday, et al., 2023; Hayes et al., 2023; Hill et al., 2019; Katz & Sutherland, 2020; Kraft et al., 2021; Muñoz et al., 2023; Rosenfeld et al., 2018) identified a significant association between RCA and sexual IPV, defined as coercing a partner into sexual activity against. Four studies (Grace, Holliday, et al., 2023; Hayes et al., 2023; Katz & Sutherland, 2020; Muñoz et al., 2023) also found psychological IPV, which encompasses emotional abuse and verbal threats, to be significantly associated with RCA; though half of these studies were rated as having a high risk of bias.
Partner Characteristics
Findings on partner characteristics were inconclusive. Two studies (Grace, Decker, et al., 2022; Grace, Perrin, et al., 2022) found no significant association between partner age and RCA, while one reported a slightly higher mean age among partners of women experiencing contraceptive interference (Katz & Sutherland, 2020). Regarding partner communication, one study (Grace, Decker, et al., 2023) found no association, while another (Kraft et al., 2021) reported that participants experiencing multiple forms of RCA had more difficult sexual health conversations with partners. However, all these studies were rated as having a high risk of bias.
Discussion
In this systematic review, we synthesized findings from 23 cross-sectional studies examining the prevalence of RCA and associated factors among U.S. populations. Several studies reported statistically significant associations between RCA and factors such as age, race and ethnicity, number of sexual partners, and physical, sexual, and psychological IPV. These findings are consistent with a prior review (Grace & Anderson, 2018), which identified RCA as disproportionately affecting younger women, individuals experiencing IPV, and Black, Latina, and multiracial women. However, we found no consistent association between RCA and socioeconomic status, and overall findings across studies were mixed (see Table 5 for a summary of key findings).
Key Findings of the Systematic Review.
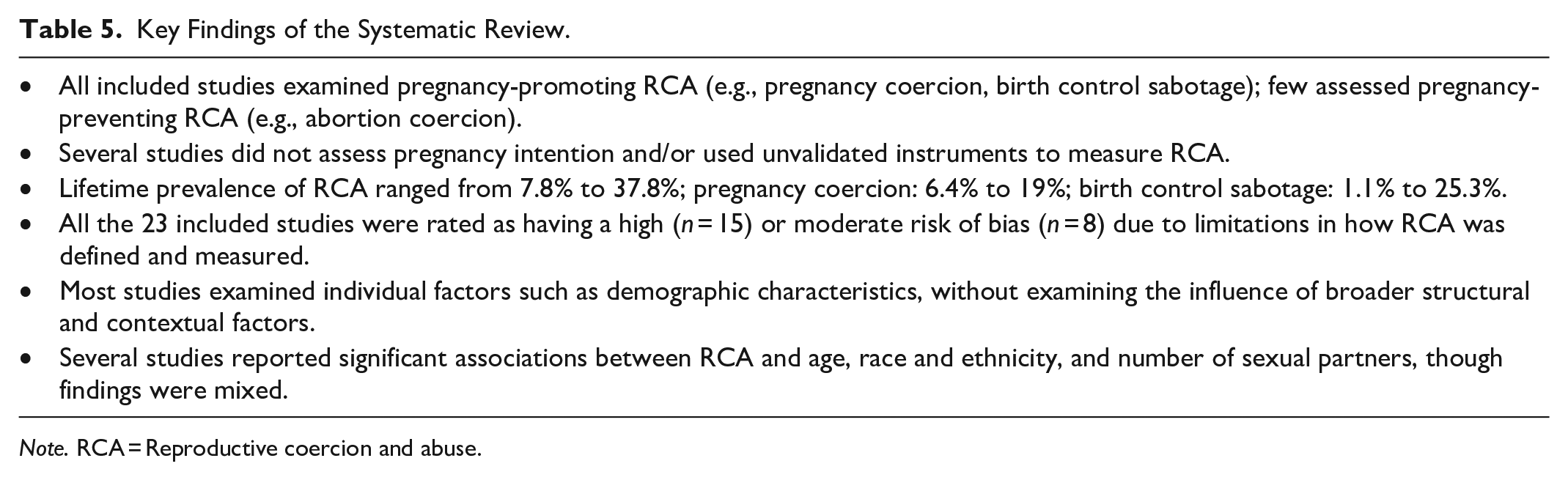
Note. RCA = Reproductive coercion and abuse.
A key contribution of our review is the inclusion of a risk of bias assessment, which previous RCA reviews did not address (Fay & Yee, 2018; Grace & Anderson, 2018; Graham et al., 2023; Rowlands & Walker, 2019). Through this assessment, we identified concerns about the trustworthiness of reported findings. All included studies were rated as having a moderate or high risk of bias, primarily due to methodological limitations in how RCA was conceptually defined and measured. These limitations raise caution about whether current evidence accurately reflects RCA prevalence or associated factors in the United States.
Foundational work has conceptualized RC as pregnancy-promoting behavior (Miller et al., 2010), while more recent frameworks (Tarzia & Hegarty, 2021) expand the construct to include both pregnancy-promoting and pregnancy-preventing behaviors, emphasizing partner intent to control reproductive outcomes. However, most studies in our review focused on pregnancy-promoting behaviors. Only two examining pregnancy-preventing forms, such as abortion coercion (Grace, Decker, et al., 2022) and perceived pressure to use birth control (Huslage et al., 2023). Although many studies predate Tarzia and Hegarty’s (2021) framework, failing to capture the full scope of RCA may distort prevalence estimates and obscure how RCA manifests across diverse populations and contexts.
In addition, several studies used RCA instruments that did not explicitly assess intent, and as a result, may have measured nonconsensual condom removal, also known as “stealthing” (Davis, 2019), rather than RCA. A recent review on stealthing found that most cases were not motivated by a desire to cause pregnancy, but rather by factors such as sexual pleasure, condom aversion, and a desire to exert dominance (Gómez-Durán & Martin-Fumadó, 2022). Only about one in ten cases were linked to pregnancy intention (Gómez-Durán & Martin-Fumadó, 2022). Even when coercive, these behaviors may reflect disregard or selfishness rather than reproductive control (Tarzia et al., 2020). While some scholars advocate removing intent from RCA instruments because all such behaviors can undermine women’s autonomy and health (Grace, Decker, et al., 2022; Grace et al., 2024; Katz & Sutherland, 2020; Katz et al., 2017), we believe research requires conceptual clarity to distinguish RCA from other forms of sexual coercion or IPV. As definitions continue to evolve, further work is needed to determine whether behaviors with and without intent have distinct health implications. Without clearer conceptual boundaries, we cannot generate high-quality data on RCA to inform evidence-based interventions, clinical practices, or policies to promote women’s sexual and reproductive health.
Beyond measurement and conceptual concerns, our review also highlights gaps in how studies examined associated factors. Most focused on individual-level factors, with limited attention to broader structural or contextual influences. For example, several studies reported higher prevalence of RCA among Black, Latina, and multiracial women (Amos et al., 2023; Bagwell-Gray et al., 2021; Grace, Perrin, et al., 2022; Grace, Decker, et al., 2023; Rosenfeld et al., 2018; Sutherland et al., 2015; Swan et al., 2023; Willie et al., 2021), but these findings must be interpreted in the context of systemic inequities. Race and ethnicity are not causal risk factors for RCA but may reflect structural conditions such as unequal access to healthcare, economic instability, housing insecurity, and discrimination (Coleman et al., 2023).
Moreover, most studies assessed demographic characteristics using single-item, self-reported measures. While this contributed to higher ratings in the risk of bias assessment, it also reflects a limitation of the JBI critical appraisal tool, which requires psychometric evidence for exposures that are widely accepted but not typically validated, such as self-reported racial identity or household income. These findings also point to a critical need to move beyond demographic proxies and examine how structural and contextual factors shape reproductive autonomy and vulnerability to RCA. Instead, structural factors such as economic instability, systemic racism, and discrimination disproportionately affect these groups, likely increasing vulnerability to RCA (Coleman et al., 2023).
Implications for Research, Practice, and Policy
In this review, we examined how RCA has been conceptually defined and measured in research, identifying an urgent need to strengthen the conceptual foundations and the instruments used in the field. Although validated instruments such as the Reproductive Coercion Scale (McCauley et al., 2017) are available, this scale only measures pregnancy-promoting behaviors, such as pregnancy coercion and condom manipulation, and does not capture the full range of RCA experiences. Few studies have examined pregnancy-preventing forms of RCA, such abortion coercion, and even fewer have done so using validated instruments. Future research should prioritize examining pregnancy-preventing forms of RCA and developing validated instruments to capture these behaviors reliably.
How RCA items are worded has important implications for both research and clinical practice. We observed that many studies used instruments that did not explicitly assess intent, which contributed to higher risk of bias ratings in our review. At the same time, we recognize that measuring intent poses challenges. Women may not always know or be able to infer the motivations behind a partner’s behavior. As definitions of RCA continue to evolve, future work must clarify whether and when intent should be incorporated into measurement.
To balance these considerations, we support the recommendation by Grace et al. (2024) to ask about behaviors and perceived intent separately. They suggest first asking whether specific behaviors occurred, followed by a question about perceived intent, such as “Do you think this person was trying to get you pregnant?” (Grace et al., 2024). Future instrument development should consider this structure and undergo rigorous psychometric testing to ensure validity, reliability, and applicability across diverse settings and populations.
Greater consistency in RCA measurement will also support clinical screening and guide policy efforts aimed at preventing RCA and promoting reproductive autonomy. Expanding the use of validated RCA instruments is essential for accurately identifying RCA and distinguishing it from other forms of IPV. Integrating RCA screening and counseling into routine clinical practice, especially in settings that already assess for IPV, can improve recognition of RCA, enhance access to appropriate support services, and reduce unintended pregnancies and prevent further abuse (Miller et al., 2017). To support these efforts, policymakers should prioritize funding for RCA research, promote the development and validation of RCA instruments, and mandate universal screening protocols in healthcare settings.
Finally, this review highlights the need to expand RCA research beyond individual-level factors to examine broader structural factors, such as healthcare access, socioeconomic inequalities, and health policy. Applying a socio-ecological framework and advanced methods like multilevel modeling can uncover how interactions across individual, interpersonal, and structural levels drive RCA disparities. Key implications are summarized in Table 6.
Implications for Research, Practice, and Policy.
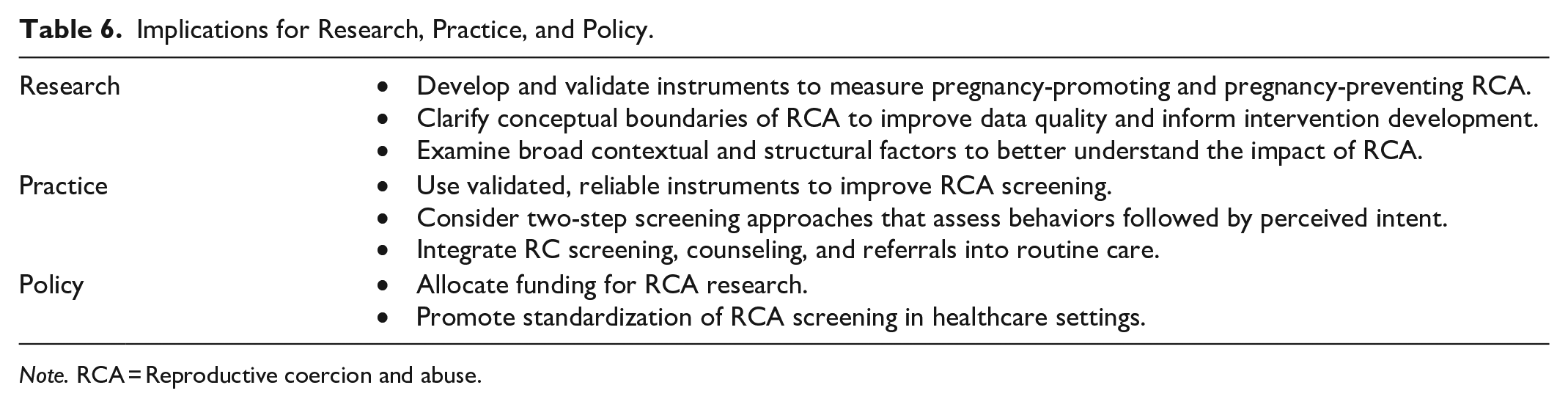
Note. RCA = Reproductive coercion and abuse.
Limitations
A key limitation of the existing literature is the considerable variability in how RCA was conceptually defined and measured across studies. These issues contributed to conceptual ambiguity, limited comparability across studies, and likely affected both prevalence estimates and the identification of associated factors. This inconsistency in RCA conceptualization and measurement also contributed to the moderate or high risk of bias ratings we assigned in this review. Additionally, most studies used cross-sectional designs and reported bivariate associations, which restricted our ability to assess causality or clarify the strength or directionality of reported associations. Finally, we restricted our review to studies conducted in the United States to inform domestic research, clinical practice, and policy developments; however, this focus limits the generalizability of our findings to global contexts.
Conclusion
In this review, we identified key limitations in the current evidence on RCA in the United States, including conceptual ambiguity, exclusion of pregnancy-preventing behaviors, and widespread use of non-validated instruments. These issues contributed to the moderate or high risk of bias ratings, limiting our confidence in the trustworthiness and interpretability of findings. We emphasize the need for validated instruments that capture the full scope of RCA and for further work to clarify how and when to assess intent. Future studies should examine conceptual clarity and measurement of RCA to improve data quality and inform evidence-based interventions, clinical screening practices, and policy efforts to safeguard reproductive autonomy.
Footnotes
Authors’ Contributions
A.L.H. conceptualization, formal analysis, writing—original draft & editing, visualization, and funding acquisition; S.E.H. formal analysis, writing—reviewing & editing; S.M. formal analysis, writing—reviewing & editing; G.W. writing—reviewing & editing; R.S. writing—reviewing & editing, and supervision.
Data Availability Statement
Data sharing is not applicable to this article, as no datasets were generated or analyzed during the current study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Nursing Research of the National Institutes of Health [F31NR021330]. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Ethical Considerations
Not applicable. There are no human participants in this article, and informed consent is not required.
Consent to Participate
Not applicable. There are no human participants in this article, and informed consent is not required.
Consent for Publication
Not applicable.