
Abstract
The impact of childhood adversity on parenting has long been a subject of research interest. This systematic review aimed to synthesize literature on parental adverse childhood experiences (ACEs) and parenting outcomes, with a particular focus on parenting stress and its underlying mechanisms. Following Preferred Reporting Items for Systematic Review and Meta-Analysis guidelines, 2,693 articles were identified through Boolean searches across ProQuest, MedLine via PubMed, PsycINFO via EBSCOhost, Cochrane, and Google Scholar, and 11 studies met the inclusion criteria. The criteria were: quantitative studies, parents with ACEs, parenting stress as a primary or analyzed variable, published between 1997 and 2024, and full-text availability in English. Findings revealed strong evidence linking ACE exposure to increased parenting stress. Parenting stress functioned both as a direct outcome and as a mediator or moderator in broader parenting models, although evidence regarding these pathways was inconsistent. Diverse instruments were used to assess ACE and parenting stress, with variations in construct validity likely contributing to heterogeneity in findings. Future research should include diverse sociocultural groups, longitudinal designs, and greater inclusion of fathers. Implications for practice, research, and policy are discussed.
Keywords
Introduction
Adverse childhood experiences (ACEs) are a significant risk factor for long-term health and psychosocial difficulties across the lifespan. Traditionally, ACEs have been grouped into two categories: maltreatment, that is, physical, sexual, and emotional abuse; physical and emotional neglect, and household challenges such as parental mental illness, substance abuse, incarceration, or domestic violence (Felitti et al., 1998). More recently, expanded ACE frameworks have included community-level adversities (e.g., exposure to violence, discrimination, or poverty) and peer-related factors such as bullying or victimization (Kalmakis & Chandler, 2014; Cronholm et al., 2015; Finkelhor et al., 2015). While ACEs are potentially traumatic experiences, not all adversities meet the threshold for trauma; rather, their impact depends on frequency, severity, and developmental context (Ranjbar & Erb, 2019).
Early life stressors such as ACEs exert the greatest influence during sensitive periods of development and contribute to intergenerational cycles of adversity (Narayan et al., 2021). Exposure to such events in childhood has been associated with increased risk for mental health conditions, substance abuse, relational difficulties, and chronic disease (Hughes et al., 2007, 2019). These effects can be particularly salient during transitional periods of adulthood, including the transition to parenthood and parenting (Mathijssen et al., 2024).
Parenting, while inherently stressful at times, can become significantly more challenging for individuals who have experienced adversity in childhood (Wattanatchariya et al., 2024). Parenting stress refers to the distress experienced when the demands of parenting exceed the individual’s perceived coping resources (Abidin, 1992). High levels of parenting stress are associated with increased risk for emotional unavailability (Tasel-Gunal & Arikan, 2024) and elevated risk for negative child outcomes such as behavioral and emotional problems (Ribas et al., 2024). Given that effective parenting requires emotional regulation, secure attachment representations, and psychological resilience—faculties that may be compromised by exposure to ACEs—parents with high ACE exposure may be particularly vulnerable to elevated parenting stress (Hanifah et al., 2023; Wattanatchariya et al., 2024). This is often referred to as “trauma-related parenting,” highlighting how unresolved symptoms of childhood adversity, such as hyperarousal, avoidance, and emotional dysregulation, may interfere with caregiving behaviors (Cruz et al., 2022).
Furthermore, a growing body of research has documented the broad impact of ACEs on other aspects of parenting. Individuals exposed to childhood adversity are not only more likely to exhibit higher levels of parenting stress (Hughes & Cossar, 2016; Wattanatchariya et al., 2024), but also reduced parental sensitivity and heightened parental hostility (Weistra et al., 2024), and difficulties in forming secure attachments with their children (Cooke et al., 2019). ACEs have also been linked to increased use of harsh or inconsistent discipline strategies (Wattanatchariya et al., 2024), lower parenting self-efficacy (Jiwani et al., 2022), and greater emotional reactivity in parenting situations (Kong et al., 2021). Furthermore, trauma-related symptoms such as hyperarousal, avoidance, and emotional dysregulation may interfere with a parent’s ability to respond appropriately to a child’s needs, increasing the risk of stress and negative parenting behaviors (Wattanatchariya et al., 2024).
Despite growing scholarly attention to the link between ACEs and parenting stress, the overall results are inconsistent. These discrepancies may arise due to differences in the conceptualization and measurement of ACEs (for instance, use of cumulative scores vs. expanded ACE frameworks), variation in parenting stress measures, variation in sample characteristics (e.g., clinical vs. community populations), developmental age of children (for instance, infancy vs. adolescence), and parent gender, with fathers often underrepresented or excluded. Moreover, when mediators have been examined, results are mixed. For instance, Steele et al. (2016) found that maternal mental health and perceived social support partially explained the association, though effects were inconsistent. Similarly, Moe et al. (2018) identified maternal attachment style as a mediator, but other research on parenting outcomes following adversity (Cooke et al., 2019; Quintigliano et al., 2021) suggests that attachment-related factors alone may not fully account for this link, pointing instead to the role of additional mechanisms such as depressive symptoms. These observations highlight the need for further work to clarify how ACE exposure translates into heightened parenting stress. Nonetheless, these studies help contextualize the broader landscape and underscore the importance of synthesizing evidence specifically on ACEs and parenting stress. Clarifying these mechanisms is critical to developing trauma-informed parenting interventions and disrupting intergenerational cycles of adversity.
While a number of systematic reviews have examined the impact of childhood adversity on parenting outcomes, many have focused on interventions (e.g., Pierron et al., 2018; Pedersen et al., 2019), parental involvement in education (Musengamana, 2023), or parenting behaviors more generally (Lyu & Lu, 2023; Rowell & Neal-Barnett, 2022). As a result, a systematic synthesis on parenting stress is essential.
However, a few reviews have looked more specifically at parenting stress. For example, Hugill et al. (2017) reviewed studies linking historical childhood sexual abuse (CSA) to later parenting stress, while Lotto et al. (2023) synthesized literature on maternal ACEs and negative parenting, and Ongilio et al. (2023) examined maternal adversity and subsequent mother–child interactions in early childhood. However, these reviews were either limited to specific forms of adversity or focused exclusively on maternal stress. The current review differs by using a broader ACE framework, including diverse parenting stress outcomes, incorporating both direct and indirect pathways, and evaluating study quality using structured critical appraisal tools. As such, it provides a more comprehensive synthesis of the association between parental ACEs and parenting stress.
Moreover, most studies have been conducted in Western, high-income contexts, with limited research from low- and middle-income countries (Draper et al., 2023; Scheidecker, 2024). Cultural norms around parenting, family structure, and adversity may shape both the experience and reporting of ACEs, as well as the meaning and management of parenting stress, yet these factors remain underexplored.
Taken together, existing reviews provide important insights into specific adversities or maternal populations, but no review has comprehensively synthesized quantitative evidence on parental ACEs and parenting stress using a broad ACE framework. Moreover, inconsistencies in measurement, mediating mechanisms, and limited inclusion of fathers and diverse cultural contexts underscore the need for an updated and methodologically rigorous synthesis. The primary objective of this review, therefore, is to synthesize quantitative studies that examine the relationship between ACE exposure and parenting stress, including those where parenting stress was assessed as a primary outcome, a mediating factor, or a moderator in the analysis. The secondary objectives are as follows: (a) summarize measurement approaches used for ACEs and parenting stress/parental outcomes, (b) identify potential mediators and moderators in this association, and (c) critically evaluate the methodological quality of the included studies.
Method
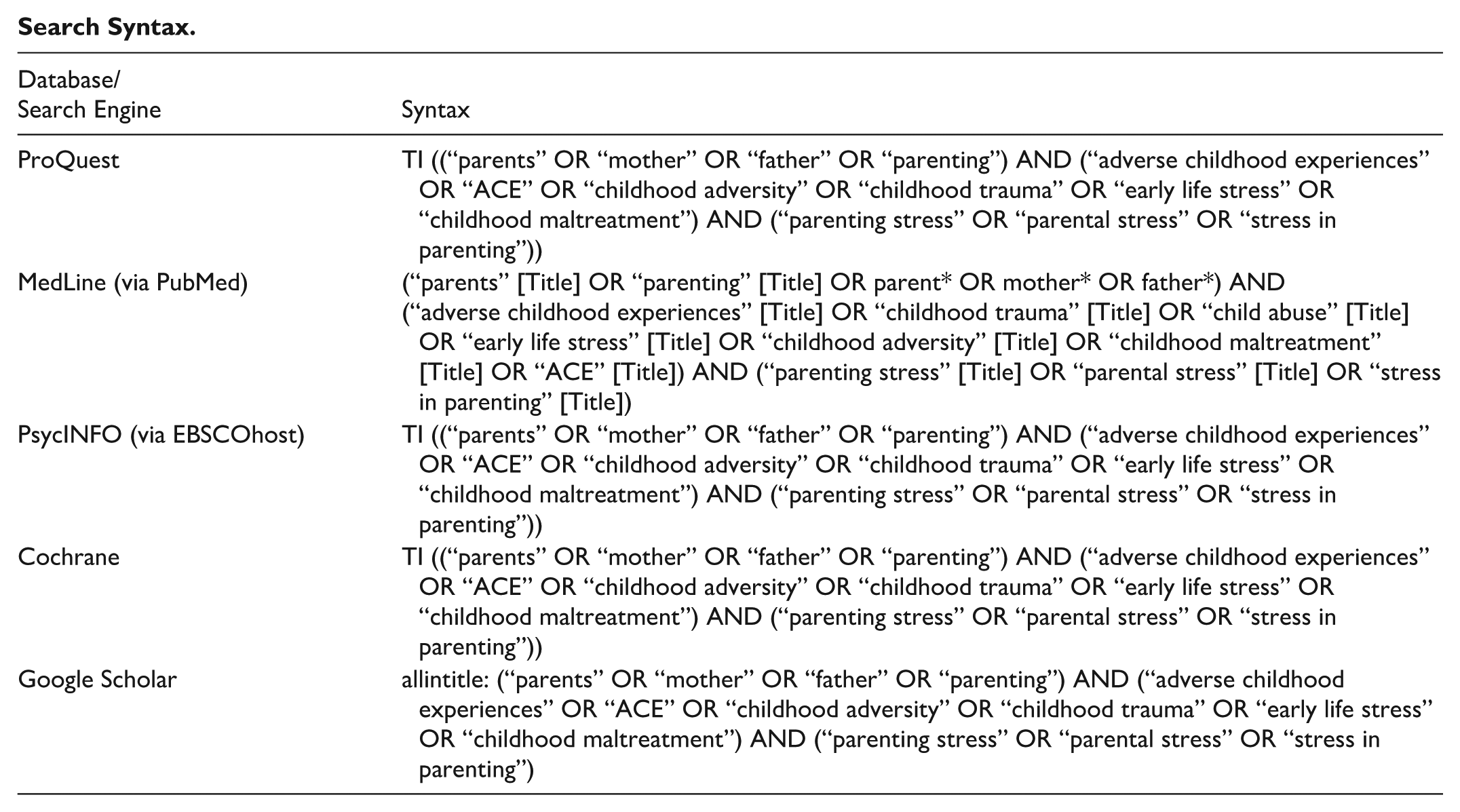
The literature search was conducted in April 2025 across five databases—ProQuest, MedLine (accessed via PubMed), PsycINFO (accessed via EBSCOhost), Cochrane, and Google Scholar—between the years 1997 and 2024. The start year, 1997, was selected as it marks the initial conceptualization of ACEs, following the seminal study by Felitti et al. (1998). Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) protocol was followed for this review (Page et al., 2021). Boolean search terms were adapted and used for each of the five databases (Appendix A). One example of a search term for title searches on PubMed was (“Parents”[Title] OR “Parenting”[Title] OR parent* OR mother* OR father*) AND (“Adverse Childhood Experiences”[Title] OR “Childhood Trauma”[Title] OR “Child Abuse”[Title] OR “Early Life Stress” [Title] OR “Childhood Adversity” [Title] OR “Childhood Maltreatment” [Title] OR “ACE” [Title]) AND (“Parenting Stress”[Title] OR “Parental Stress” [Title] OR “Stress in Parenting”[Title]). It is important to note that many different terms have been used to indicate ACEs in the extant literature. Hence, seven different terms were used in the search to identify appropriate studies and search broadly to find relevant literature.
The initial searches resulted in 2,693 articles. After removing duplicates (n = 1,097) and other records including dissertations, conference proceedings and book chapters (n = 529), 1,067 articles were identified to be screened for title and abstract. Finally, 338 articles were selected for full-text screening considering the eligibility criteria. The inclusion criteria included (a) primary studies with a quantitative design, (b) population studied must be parents (including mothers and fathers) with a history of ACEs or childhood maltreatment, (c) parenting stress must be the outcome variable or a variable in the analysis, and (d) full-text articles published in English. The quantitative studies included cross-sectional, longitudinal, and intervention designs. One randomized controlled trial (RCT) was included in this review as it reported relevant pre-intervention baseline data on ACE exposure and parenting stress, consistent with the correlational focus of this review. Studies that assessed current adversity, trauma, or stressful life events in adulthood were excluded unless they explicitly measured ACEs as a historical construct from the participant’s childhood. Studies published in languages other than English (e.g., Spanish, German, and Chinese) were excluded, given the researcher’s lack of fluency in these languages. Additionally, qualitative studies, mixed method studies and review papers, along with studies in languages other than English were also excluded. Fifteen studies for which full-text articles could not be retrieved (despite appearing in initial database searches) were excluded at the full-text screening stage (Appendix C). Out of the 338 articles, full-text screening resulted in 11 articles to be included in this study. Details of the screening process are provided in Figure 1.
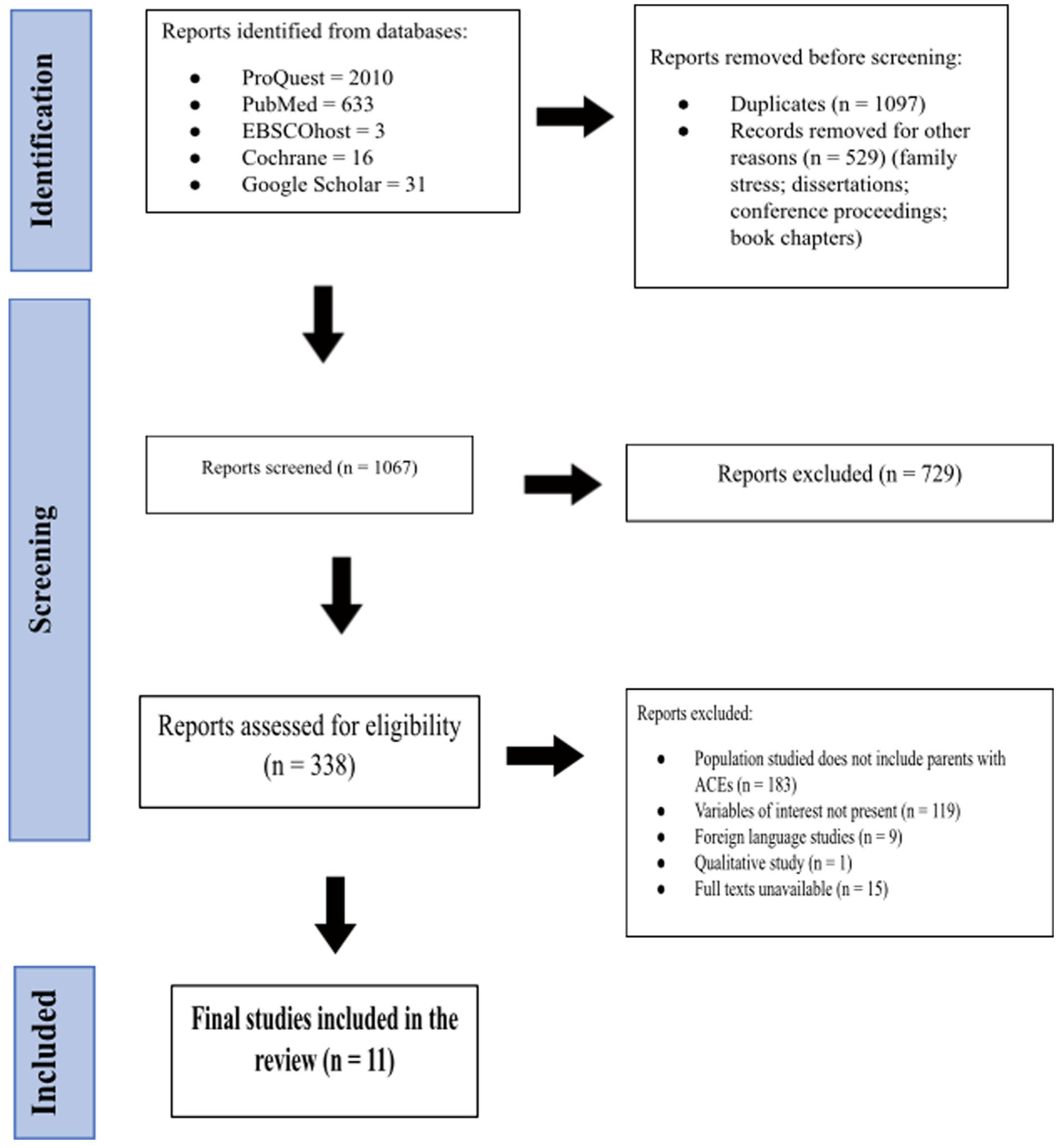
PRISMA flow diagram for article selection.
Data Extraction
Relevant data from the 11 included studies were extracted using a standardized template. This template included the following information: (a) publication details, including title, authors, source, and year of publication, (b) sample characteristics, such as population, sampling frame, gender of participating parents (mothers, fathers or mixed sample), and sample size, (c) study characteristics, including research design, inclusion and exclusion criteria, objectives, measured variables, tools used, and method of analysis, and lastly, (d) key findings and reported limitations.
Methodological Appraisal
The methodological appraisal of the included studies was conducted using design-specific tools. For the six cross-sectional studies, the Appraisal tool for Cross-Sectional Studies (AXIS; Downes et al., 2016) was applied. This 20-item tool evaluates clarity of aims, appropriateness of study design, sample size justification, reporting of non-response, suitability of measures, detail for replication, and consideration of ethical issues and funding. AXIS provides a structured assessment but does not classify studies as “good,” “fair,” or “poor”; instead, it identifies the extent to which individual criteria are met (Appendix B1).
For the four longitudinal studies, the Newcastle–Ottawa Scale (NOS; Wells et al., 2014) was used. The NOS is specifically designed for cohort and case–control studies and appraises studies across three domains: selection of participants, comparability of cohorts, and assessment of outcomes. Each study receives a star rating within these domains, allowing for evaluation of both methodological robustness and potential sources of bias, such as participant retention and follow-up completeness (Appendix B2).
Finally, the single RCT was appraised using the CONSORT 2010 checklist (Schulz et al., 2010). This checklist covers essential aspects of trial design, including randomization procedures, allocation concealment, blinding, sample size calculation, participant flow, reporting of outcomes, and disclosure of harms. Given that intervention studies carry distinct risks of bias, using CONSORT ensured an appropriate appraisal of the trial’s methodological strengths and limitations (Appendix B3).
Results
Study Characteristics
This section outlines the key characteristics of the 11 included studies, which inform the interpretation and synthesis of the overall findings. All included studies adhered to the specified inclusion criteria, focusing on quantitative studies involving a sample of parents with documented ACE-exposure and studying parenting stress as either a primary outcome variable or a variable in the analysis. A majority of the 11 included studies were conducted in the United States (n = 7), with a few studies from other geographical and sociocultural contexts—Norway (n = 1), China (n = 1), Taiwan (n = 1) and Iran (n = 1). Most studies employed cross-sectional (n = 7) or longitudinal designs (n = 4), with one study utilizing a RCT.
Sample sizes varied across the studies, ranging from 78 to 2,925 participants, reflecting a wide variation in study scope and recruitment strategy. The samples represented diverse parental populations. Most studies focused on mothers from specific contexts, such as first-time mothers or mothers from low-income backgrounds or those receiving early home visiting or behavioral health services. One study focused solely on paternal ACEs and fathering, while one other study included both mothers and fathers with ACE-exposure. This reflects a dearth of studies and a growing interest in paternal ACEs and their influence on parenting and parent-child outcomes.
The age of children in the included studies ranged from infancy to adolescence, although not all studies reported this information. Sociodemographic characteristics were variably described; several U.S.-based studies included racially and ethnically diverse, low-income parents, while other studies either focused on specific subgroups (e.g., first-time mothers) or did not report ethnicity at all. This variability limits generalizability and highlights gaps in the literature regarding underrepresented populations, particularly fathers and families from diverse cultural contexts. Characteristics of each study are highlighted in Table 1.
Methodological Characteristics of the Included Studies.
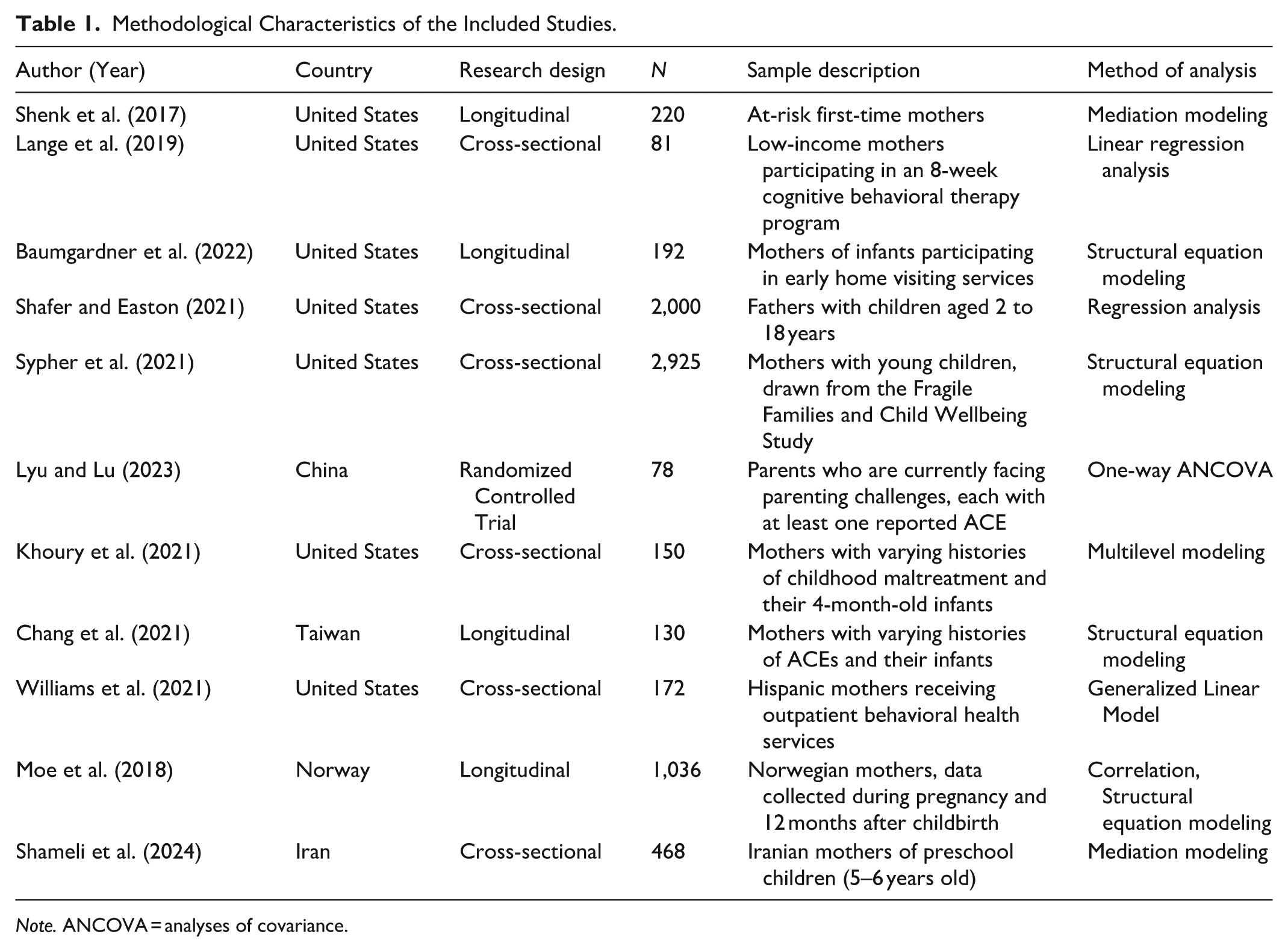
Note. ANCOVA = analyses of covariance.
Methodological Quality of Included Studies
Cross-sectional studies generally scored between 15 and 17 on the 20-item AXIS tool, indicating that while many criteria were met, gaps remained in areas such as sample size justification and reporting of non-response bias. Longitudinal studies, assessed with the NOS, were typically rated as moderate in quality, with strengths in clearly defined cohorts and valid outcome assessment, but weaknesses in participant retention and incomplete reporting of follow-up procedures. The single RCT was evaluated using the CONSORT checklist, which showed strengths in describing study aims and outcomes but shortcomings in reporting randomization, allocation concealment, and blinding. A detailed breakdown of the critical appraisal for each study is provided in Appendix B.
Across all designs, several methodological strengths were identified. Most studies presented clearly stated aims, employed appropriate designs to address their objectives, and used relevant measures of exposure (ACEs) and outcomes (parenting stress or related constructs). Analytical approaches were generally robust and well justified, with conclusions appropriately aligned to results. However, recurring limitations were also evident. A common issue was the lack of justification for sample sizes and insufficient reporting on non-responders, raising concerns about representativeness. Many studies relied heavily on retrospective self-report measures of ACEs. Finally, generalizability was limited in some cases due to the use of convenience samples or restricted populations (e.g., low-income or clinical subgroups), and fathers remained notably underrepresented across the literature.
Measurement of ACEs
A summary of the measurements of ACEs and various parenting variables, including parenting stress, has been given in Table 2. Across studies, ACE exposure was assessed using a variety of instruments, which can be grouped into two categories. First, the most frequently used tool was the original or modified ACE questionnaire, measuring domains of childhood maltreatment (emotional, physical, sexual abuse; emotional and physical neglect) and household challenges (parental mental illness, substance abuse, divorce, domestic violence). Some studies analyzed ACEs using a cumulative score, while others applied a cut-off score to classify high versus low ACE exposure. Second, other studies employed alternative instruments, including the Maltreatment and Abuse Chronology of Exposure scale, which captures peer and sibling abuse, interparental violence, and other developmental adversities, and the Child Abuse Self-Report Scale adapted for Persian-speaking populations. These instruments were sometimes culturally validated, ensuring relevance to the local context, though not all studies reported validation procedures.
Measurement of ACEs and Parenting Variables.
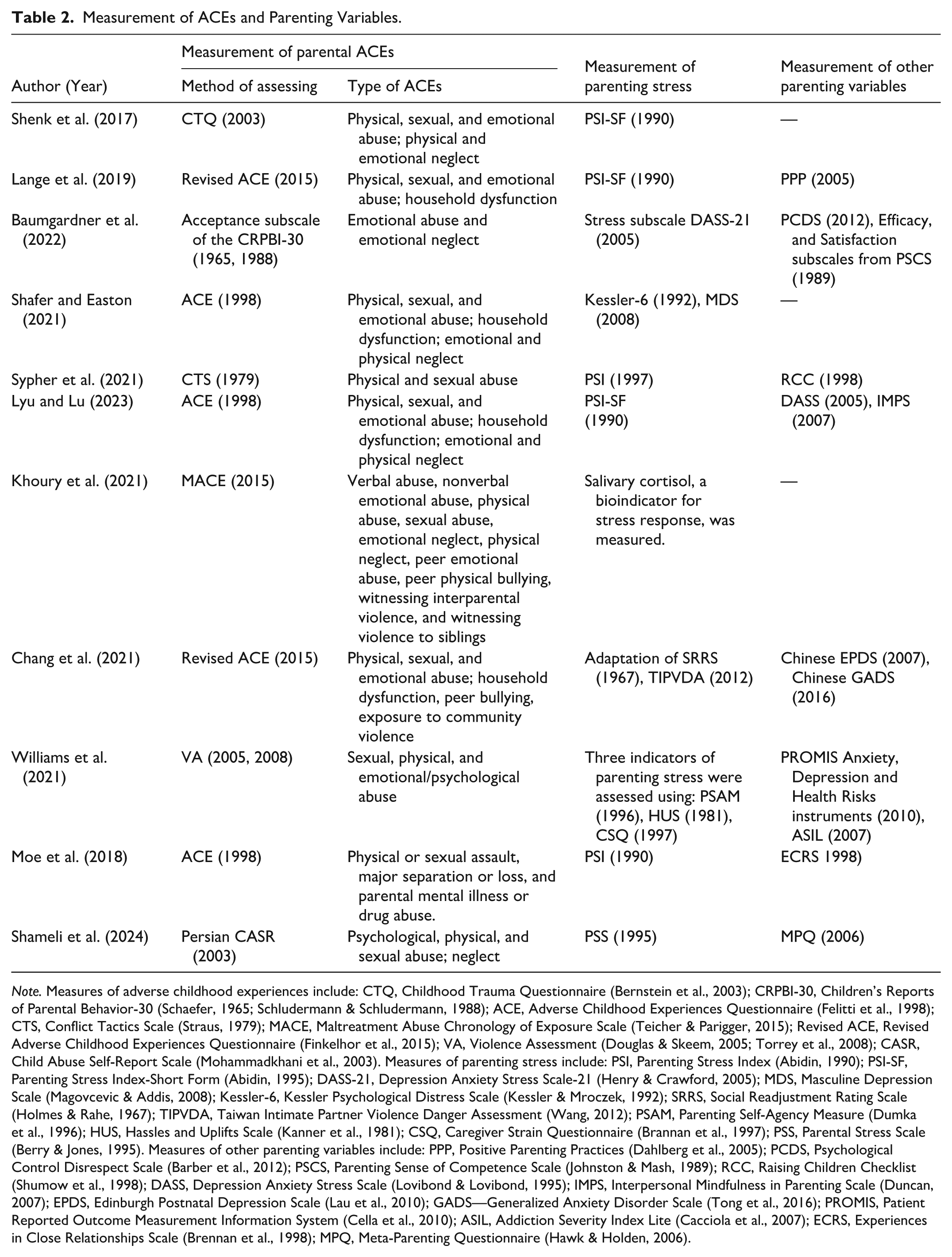
Note. Measures of adverse childhood experiences include: CTQ, Childhood Trauma Questionnaire (Bernstein et al., 2003); CRPBI-30, Children’s Reports of Parental Behavior-30 (Schaefer, 1965; Schludermann & Schludermann, 1988); ACE, Adverse Childhood Experiences Questionnaire (Felitti et al., 1998); CTS, Conflict Tactics Scale (Straus, 1979); MACE, Maltreatment Abuse Chronology of Exposure Scale (Teicher & Parigger, 2015); Revised ACE, Revised Adverse Childhood Experiences Questionnaire (Finkelhor et al., 2015); VA, Violence Assessment (Douglas & Skeem, 2005; Torrey et al., 2008); CASR, Child Abuse Self-Report Scale (Mohammadkhani et al., 2003). Measures of parenting stress include: PSI, Parenting Stress Index (Abidin, 1990); PSI-SF, Parenting Stress Index-Short Form (Abidin, 1995); DASS-21, Depression Anxiety Stress Scale-21 (Henry & Crawford, 2005); MDS, Masculine Depression Scale (Magovcevic & Addis, 2008); Kessler-6, Kessler Psychological Distress Scale (Kessler & Mroczek, 1992); SRRS, Social Readjustment Rating Scale (Holmes & Rahe, 1967); TIPVDA, Taiwan Intimate Partner Violence Danger Assessment (Wang, 2012); PSAM, Parenting Self-Agency Measure (Dumka et al., 1996); HUS, Hassles and Uplifts Scale (Kanner et al., 1981); CSQ, Caregiver Strain Questionnaire (Brannan et al., 1997); PSS, Parental Stress Scale (Berry & Jones, 1995). Measures of other parenting variables include: PPP, Positive Parenting Practices (Dahlberg et al., 2005); PCDS, Psychological Control Disrespect Scale (Barber et al., 2012); PSCS, Parenting Sense of Competence Scale (Johnston & Mash, 1989); RCC, Raising Children Checklist (Shumow et al., 1998); DASS, Depression Anxiety Stress Scale (Lovibond & Lovibond, 1995); IMPS, Interpersonal Mindfulness in Parenting Scale (Duncan, 2007); EPDS, Edinburgh Postnatal Depression Scale (Lau et al., 2010); GADS—Generalized Anxiety Disorder Scale (Tong et al., 2016); PROMIS, Patient Reported Outcome Measurement Information System (Cella et al., 2010); ASIL, Addiction Severity Index Lite (Cacciola et al., 2007); ECRS, Experiences in Close Relationships Scale (Brennan et al., 1998); MPQ, Meta-Parenting Questionnaire (Hawk & Holden, 2006).
Despite this variation in scope, ACE exposure was most often assessed retrospectively through self-report, with instruments employing dichotomous (yes/no) response options or frequency-based scales. As a result, important nuances regarding the subjective and cumulative impact of adversity may have been overlooked in these studies. These methodological limitations are common in ACE research and should be considered when interpreting patterns of association. It might also have implications for the findings of this systematic review.
Measurement of Parenting Variables
Parenting Stress
Parenting stress was mostly assessed using a range of standardized self-report instruments. The most frequently used tools were the Parenting Stress Index (PSI) and its short form (PSI-SF), which appeared in 5 of the 11 included studies. These tools evaluate both parent-related and child-related sources of stress and are widely used in both clinical and research contexts. One study employed the Parenting Stress Scale, a brief measure focused on perceived difficulties in the parenting role. Another study used the stress subscale from the Depression Anxiety Stress Scales to quantify parenting-related psychological strain. Additionally, one study utilized a composite approach, combining indicators such as parenting self-agency, child-related hassles, and caregiving load to assess overall parenting stress.
Beyond self-report, one study employed a biological marker of stress, measuring salivary cortisol levels in mothers and infants as an indicator of physiological stress. This inclusion of a bioindicator represents an important methodological strength that offers a more objective assessment of parental stress-related functioning.
While these instruments differed in theoretical orientation and operationalization of parenting stress, they were all designed to capture the psychological burden experienced by parents in the caregiving role. Moreover, in some cases, parenting stress was not examined as a primary outcome but rather as a mediator or moderator within broader models of parental functioning. This diversity in assessment approaches reflects the complexity of parenting stress and its intersections with other domains of parental functioning and wellbeing.
Other Parenting Variables
Eight of the 11 studies included measured at least one additional parenting variable alongside parenting stress. These variables provided further insight into how ACEs influence parenting, beyond stress. Parenting self-efficacy and parenting satisfaction were assessed using the Parenting Sense of Competence Scale, which measures parents’ perceived effectiveness and emotional fulfillment in their role. Parenting self-agency, which reflects initiative and control in parenting decisions, was also measured in one study using the Parenting Self-Agency Measure. Mindful parenting, operationalized as present-centered awareness, nonjudgmental acceptance, and emotional regulation in parent–child interactions, was assessed in one study using the Interpersonal Mindfulness in Parenting Scale. Similarly, meta-parenting—the cognitive process of reflecting on and planning parenting strategies—was measured in one study using the Meta-Parenting Questionnaire. Parenting behaviors, including warmth, harsh discipline, and responsiveness, were measured using the Raising Children Checklist, providing a behavioral perspective on parenting in addition to cognitive or emotional constructs.
Parental ACEs and Parenting
This section describes the core findings from the 11 studies included in this review. Studies varied in how they conceptualized and measured parenting-related outcomes, with some directly examining the link between ACE exposures and parenting stress, and others testing mediation/moderation pathways or broader parenting constructs (Table 3).
Main Findings.
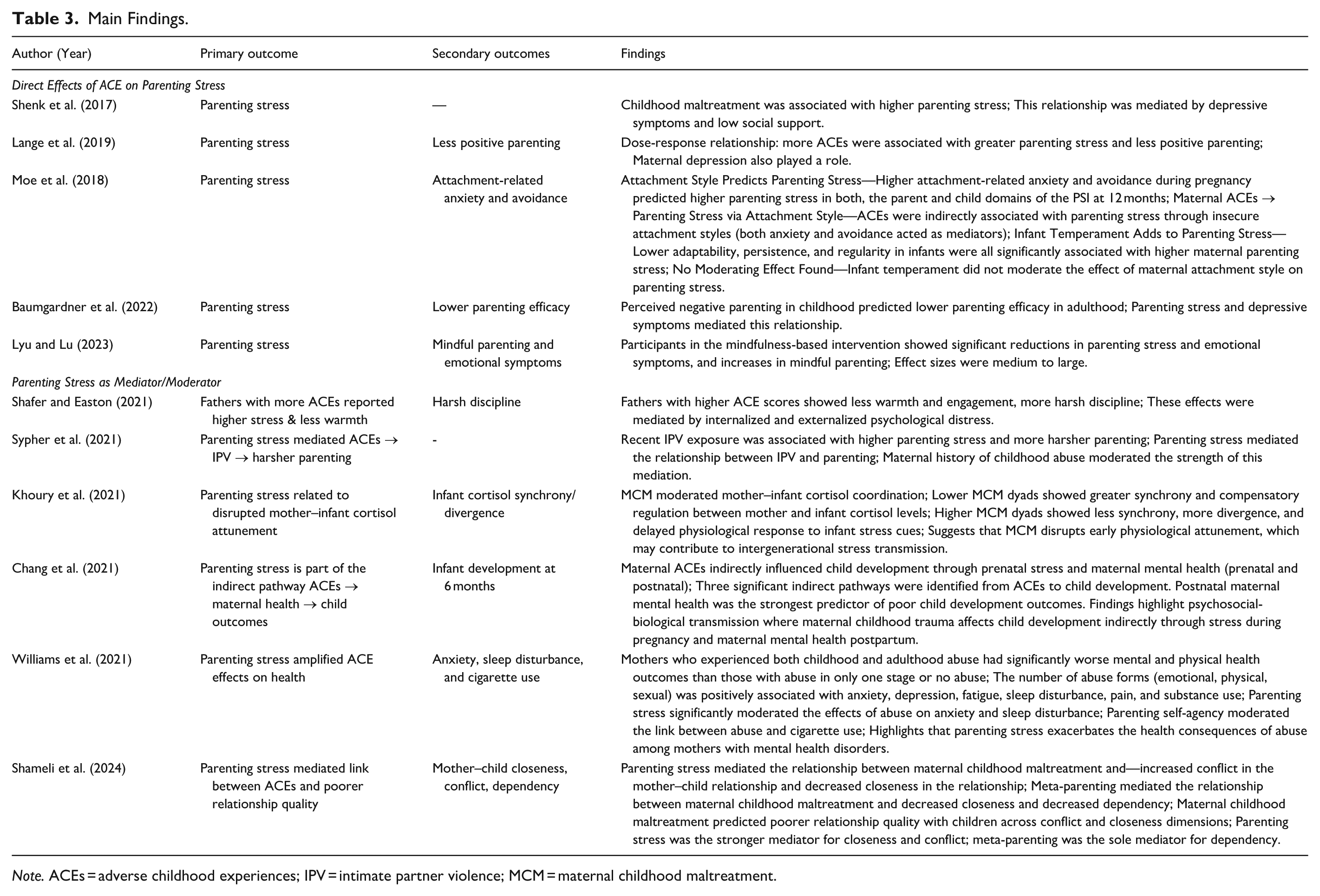
Note. ACEs = adverse childhood experiences; IPV = intimate partner violence; MCM = maternal childhood maltreatment.
Direct Association Between Parental ACEs and Parenting Stress
Across five studies that directly examined parenting stress as a primary outcome, a consistent pattern emerged—parents with higher exposure to ACEs were significantly more likely to report elevated levels of stress in their parenting roles. These studies, which included both cross-sectional and longitudinal designs, provide evidence for the psychological burden that early adversity may impose on later parenting. Two studies identified a direct dose–response relationship, between parental exposure to ACEs and parenting stress. Lange et al. (2019), for instance, found that low-income mothers with higher ACE scores experienced greater difficulty managing parenting demands, as well as reduced engagement in positive parenting practices—aligning with increased parenting stress. This finding corroborates with the results from Shenk et al. (2017), who observed that childhood maltreatment was positively associated with more parenting stress among first-time mothers as well. Further, as illustrated in Baumgardner et al. (2022), childhood emotional abuse and neglect predicted heightened parenting stress, which in turn was associated with lower confidence in the parenting role. Though these studies differ in sample characteristics, they highlight the compounding nature of early adversity on later parenting stress.
Often, early exposure to adversity may cause disruptions in key developmental processes such as attachment and emotional regulation, leading to later difficulties in the parenting role. Moe et al. (2018) found that maternal ACEs were indirectly linked to increased parenting stress at 12 months postpartum, with insecure attachment styles (both anxiety and avoidance) serving as significant mediators. This suggests that early trauma resulting from exposure to adversities may influence how parents form bonds with their own children, contributing to heightened stress during the early caregiving period. Additionally, intervention-based research offers further support for this relationship. In a RCT, Lyu and Lu (2023) found that parents with a history of ACEs reported higher initial levels of parenting stress, but also showed significant reductions in stress following a mindfulness-based intervention. This finding not only reinforces the link between ACEs and parenting stress, but also suggests that targeted interventions can mitigate its effects. While some studies incorporated additional parenting constructs, such as efficacy or satisfaction, parenting stress consistently emerged as a central and measurable outcome associated to early adversity.
Indirect Pathways Linking Parental ACEs and Parenting Stress
Mediators and moderators in the relationship between ACEs and parenting stress were examined in six of the included studies. For instance, Shenk et al. (2017) found that both depressive symptoms and low perceived social support partially explained the link between childhood maltreatment and elevated parenting stress. However, other studies focused on parenting stress itself as a mediator or moderator in broader parenting contexts. The study by Baumgardner et al. (2022), for example, reported that depressive symptoms and parenting stress jointly mediated the relationship between childhood experiences of emotional abuse/neglect and adult parenting self-efficacy. In other studies too, like Sypher et al. (2021) and Williams et al. (2021), parenting stress appeared to act as a mechanism through which the effects of early adversity and concurrent stressors are transmitted to other outcomes. Sypher et al. (2021) found that parenting stress mediated the association between recent intimate partner violence and the use of harsh parenting strategies, with maternal ACE history strengthening this link. Similarly, Williams et al. (2021) reported that parenting stress moderated the relationship between maternal abuse history and health-related outcomes such as anxiety, sleep disturbance, and substance use.
Attachment-related variables were also examined as potential mediators, particularly in the postpartum period. Moe et al. (2018) found that maternal attachment-related anxiety and avoidance mediated the association between ACEs and parenting stress 1 year after childbirth. In contrast, Cooke et al. (2019) and Quintigliano et al. (2021) reported that attachment style alone did not fully explain the effect of ACEs on parenting stress, and that depressive symptoms remained a stronger explanatory factor, suggesting that attachment may only partially mediate this link.
While these studies point to the importance of psychological and relational factors in explaining how ACEs influence parenting, the pathways tested varied widely, and no variable was found to be consistently significant.
ACEs and Complementary Parenting Variables
In addition to parenting stress, which was the central outcome of this review, several studies also examined complementary parenting variables, such as parenting self-efficacy, satisfaction, discipline strategies, mindful parenting, and meta-parenting. These variables, while not the primary focus, provide valuable insight into the broader impact of ACEs on parenting. Two studies found that childhood adversity was significantly associated with lower parenting self-efficacy and satisfaction. Baumgardner et al. (2022) reported that childhood experiences of emotional abuse and neglect predicted reduced parenting efficacy and satisfaction, particularly among mothers with high levels of depressive symptoms. Similarly, Williams et al. (2021) observed that parenting self-agency—a related construct reflecting confidence and control in the parenting role—was negatively associated with maternal abuse history.
Other studies focused on parenting behaviors and cognitive dimensions of parenting. Sypher et al. (2021) found that mothers with higher ACE exposure were more likely to engage in psychological control and harsher discipline strategies. Parenting stress emerged as a mediator in this relationship. Importantly, Shafer and Easton (2021) were the only study in the review that specifically examined a population of fathers in this context. The authors found that fathers with higher ACE exposure reported increased internalizing and externalizing symptoms, which in turn were associated with lower levels of warmth and higher levels of harsh parenting behaviors.
Cognitive regulatory processes, such as meta-parenting and mindful parenting, are also impacted by ACE exposure. Shameli et al. (2024) found that mothers with higher ACE scores reported lower levels of meta-parenting—specifically in planning, reflecting, and problem-solving—which in turn mediated the relationship between ACEs and the quality of the mother–child relationship. Similarly, Lyu and Lu (2023) observed that ACE exposure was linked to lower levels of mindful parenting. However, their intervention study also showed that participation in a mindfulness-based parenting program significantly improved mindful parenting practices and reduced the negative effects of ACEs.
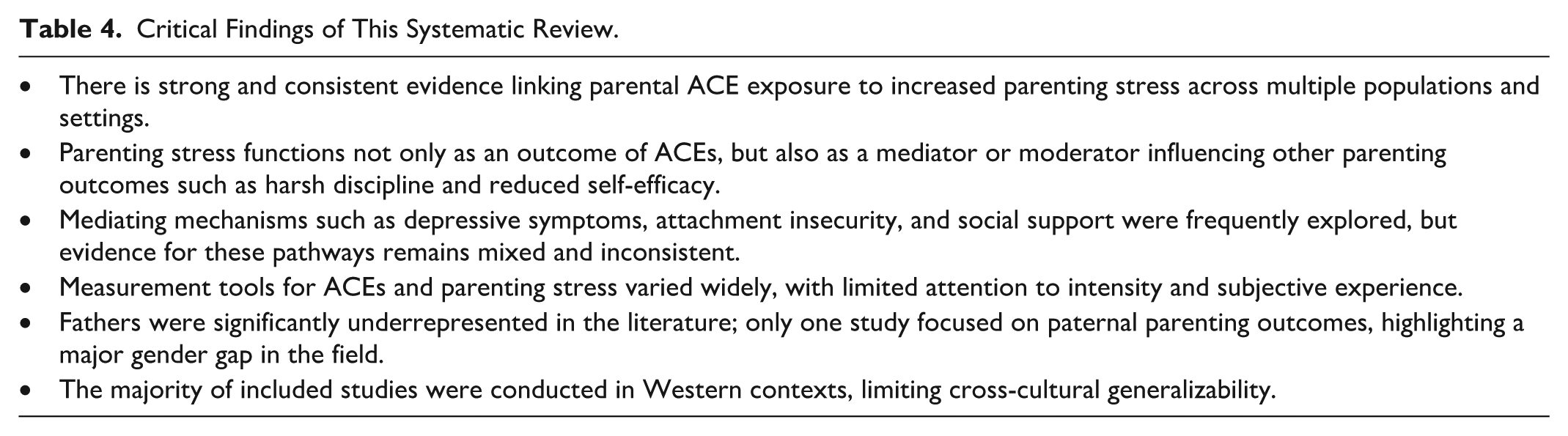
Together, these findings describe the influence of ACEs on multiple domains of parenting. While parenting stress appears to be the most consistently affected outcome in this review, the effects of early adversity extend into beliefs, behaviors, and relational patterns that are critical for effective caregiving. The critical findings of this review are summarized in Table 4.
Critical Findings of This Systematic Review.
Discussion
This systematic review aimed to synthesize quantitative studies that examine the relationship between parental exposure to ACEs and parenting stress. It also aimed to identify potential mechanisms that link ACEs and parenting stress. Given the profound impact of exposure to childhood adversity on later parenting stress, it is necessary to systematically review the findings to date. Overall, 11 articles were included in this review after a comprehensive selection process following the PRISMA protocol.
The findings of this review build upon and extend previous systematic reviews that have examined the impact of childhood adversity on parenting outcomes. For instance, Hugill et al. (2017) focused specifically on the relationship between CSA and later parenting stress, identifying predominantly indirect pathways mediated by depression and other current stressors. While their review demonstrated the relevance of early trauma in shaping later parenting experiences, it was restricted to one specific form of adversity, that is, CSA. Similarly, Lotto et al. (2023) reviewed 29 studies on the intergenerational impact of maternal ACEs on negative parenting practices, such as harsh discipline and maltreatment and Ongilio et al. (2023) reviewed maternal ACE histories in relation to mother–child interactions. Although they reported consistent associations between maternal adversity and negative parenting behaviors and mother–child interactions, and acknowledged the role of parenting stress, this variable was not the central focus of their review. In contrast, the current review systematically synthesized studies examining a broad ACE framework in relation to parenting stress specifically, both as a direct outcome and as a mediating or moderating variable. By incorporating diverse quantitative study designs, including both maternal and paternal perspectives, and highlighting key methodological patterns, this review provides a more focused and integrative understanding of how ACEs contribute to parenting stress and related outcomes.
The critical appraisal of the included studies revealed several methodological strengths and weaknesses that should inform the interpretation of this review’s findings. Most studies clearly articulated their research objectives, used appropriate statistical analyses, and employed valid and reliable tools to assess ACEs and parenting outcomes. However, a number of limitations were consistently observed across studies. These included inadequate justification for sample size, limited reporting on response rates, and overreliance on retrospective self-report measures for ACEs, which introduces recall bias. Additionally, many studies used convenience samples from clinical or high-risk populations, limiting generalizability.
Primary and Direct Effects
In our review, parenting stress was the most common variable assessed among the parenting variables. Overall, there was strong evidence for the direct effect of exposure to ACEs on parenting stress. In studies where parenting stress was the primary outcome, this relationship was observed across different populations, including first-time mothers, parents from low-income backgrounds, and participants in parenting interventions. Notably, a dose–response pattern emerged in two studies, suggesting that a higher number of ACEs is related to increased levels of stress in parenting. These findings are consistent with established models of stress and trauma, which propose that early adversity compromises emotional regulation (Chang et al., 2003) and attachment security (Doyle & Cicchetti, 2017)—both of which are processes central to the parenting role and thereby contributing to stress (Mortazavizadeh et al., 2022; Obeldobel et al., 2022; Waters et al., 2010).
Indirect and Complementary Effects
Some studies in this review extended this work by examining mediating and moderating variables in the ACE–parenting stress relationship. Maternal mental health, such as having depressive symptoms and perceived social support, emerged as prominent mediators in this relationship. Attachment-related anxiety and avoidance were also found to mediate this relationship in some studies, although the evidence for this was less consistent.
Importantly, some studies conceptualized parenting stress not only as an outcome but also as a mechanism through which ACEs influence other parenting domains. For example, Sypher et al. (2021) explained that parenting stress mediated the association between intimate partner violence and maternal use of harsh disciplinary strategies. In this model, mothers with a history of ACEs were more likely to experience heightened parenting stress when exposed to IPV, which in turn predicted harsher parenting practices. Similarly, Williams et al. (2021) reported that parenting stress moderated the impact of maternal ACE exposure on a range of maternal health outcomes, including anxiety, sleep disturbance, and cigarette use. In this context, higher levels of parenting stress amplified the negative effects of ACEs, particularly when other risk factors were present. These findings are consistent with cumulative risk and stress proliferation frameworks (Evans et al., 2013; Pearlin et al., 2005), which propose that parenting stress can exacerbate the negative effects of prior trauma when additional ecological or relational stressors are present. Taken together, these studies reflect the dual function of parenting stress—as a direct consequence of ACE exposure and as a dynamic factor that shapes how adversity influences other areas of parental functioning.
Beyond stress, ACEs were also found to affect a range of other parenting variables, including self-efficacy, satisfaction, and discipline strategies. Parents with higher ACE exposure were more likely to report lower confidence in their parenting abilities. These findings are supported by literature that suggests a mother’s lack of confidence not only affects her self-concept and physical and mental health, but may also make her less sensitive to her parental roles and damage parent–child relationships (Goto et al., 2010). This, as a result, increases their parenting stress levels (Huang et al., 2022). The review also suggested that parents with higher ACE exposure tend to use harsher and more controlling disciplinary approaches. In fact, Wattanatchariya et al. (2024) corroboratethese results in a non-Western sample of parents, indicating that those parents who had faced childhood adversity were more likely to use corporal punishment and inconsistent or harsher disciplining strategies with their own children. It is important to note that these relationships are often mediated by parenting stress itself (Freisthler et al., 2022; Kistin et al., 2014).
Parents’ cognitive and relational processes are also affected by ACE exposure. For example, ACEs were associated with lower levels of meta-parenting—the capacity to reflect on, plan, and problem solve in response to parenting challenges (Merrifield et al., 2015). These skills are particularly important for adaptive and flexible parenting, and disruptions in these processes may contribute to parental stress (Holden & Hawk, 2003). Similarly, mindful parenting—the capacity to focus awareness on one’s own thoughts, feelings and behaviours, as well as pay attention to one’s children in an intentional, present-centered, and non-judgmental manner (Cowling & Van Gordon, 2021) – was negatively associated with ACEs. Together, these findings highlight the impact of ACEs not only on stress and behavioral responses but also on deeper psychological processes that influence the quality of parent–child relationships.
Methodological Considerations
Despite the overall consistency in findings, several methodological inconsistencies were observed across studies. One key issue was the variation in how ACEs were measured. While some studies used the original ACE questionnaire, others employed expanded or culturally adapted tools, each capturing different aspects of childhood adversity. These instruments also differed in their response formats—some assessed frequency, while others relied on binary “yes/no” answers—potentially limiting the ability to capture severity or the subjective impact of the adversity. Similarly, parenting stress was measured using a range of tools, some focusing narrowly on stress and others within broader constructs such as parental mental health and parenting competence. This heterogeneity in operational definitions makes it tricky to compare results across studies. Another methodological concern was the limited attention given to the construct validation of measurement tools. Although some studies used widely accepted and standardized instruments, many did not report on psychometric properties such as reliability, validity, or cultural adaptation of the tools within the study sample.
Another limitation is the reliance on retrospective self-report, particularly in the assessment of ACEs. While this method is efficient and widely used in research, it is subject to recall bias and may be influenced by one’s current mental state. Additionally, most of the studies included in this review were cross-sectional, limiting the ability to draw conclusions about the directionality of the observed associations. Although a few longitudinal studies and one intervention study were included, follow-up periods were often short and focused primarily on early parenting, leaving gaps in our understanding of how ACEs impact parenting across different developmental stages.
Demographic and Cultural Contexts
The current evidence reflects notable gaps in population diversity. Most studies were conducted in Western, Educated, Industrialized, Rich, and Democratic (WEIRD) contexts, a limitation increasingly acknowledged in developmental science (Draper et al., 2023; Scheidecker, 2024). This restricts the cultural generalizability of findings, particularly given that parenting stress is shaped by contextual factors such as social norms, economic resources, and intergenerational caregiving practices. Furthermore, while some non-Western data exist (e.g., Wattanatchariya et al., 2024), these are limited. Culturally inclusive research, as well as adaptation and validation of parenting stress measures in non-Western contexts, remain pressing needs.
Gender diversity was also limited. Only one study (Shafer & Easton, 2021) included fathers. This lack of paternal representation leaves significant gaps, given fathers’ crucial roles in caregiving and child development. Future research must not only include fathers but also consider broader caregiver identities (e.g., grandparents, same-sex parents).
Additionally, most studies did not adequately address racial/ethnic diversity, nor did they disaggregate findings by these variables. Considering the role of structural inequalities in shaping both exposure to ACEs and parenting stress, future work should explicitly examine intersections of gender, race, and socioeconomic status.
Limitations of the Included Studies
Although all 11 studies included in this review met moderate to high methodological standards, none fulfilled all criteria on the design-appropriate appraisal tools (AXIS, NOS, or CONSORT). Common limitations included a lack of justification for sample size, insufficient reporting on response rates, and a reliance on retrospective self-report measures, particularly for assessing ACEs. These issues raise concerns about recall bias and generalizability. Additionally, very few studies employed longitudinal designs, limiting the ability to draw causal inferences or understand how ACEs influence parenting stress over time as children grow and parental responsibilities evolve. The use of diverse tools to measure both ACE exposure and parenting stress further complicated synthesis and comparison across studies. Moreover, potential confounding variables—such as partner relationship quality, current life stressors, and access to support systems, were inconsistently measured or not accounted for.
A further limitation concerns the generalizability of the findings. Most included studies recruited participants from narrow populations—such as mothers in clinical or high-risk groups—limiting the extent to which results can be applied to broader and more diverse parenting populations. Moreover, a further limitation lies in the predominance of studies conducted within WEIRD populations. This geographic and cultural concentration significantly restricts the applicability of findings to more diverse global contexts, especially given increasing recognition of the biases inherent in child development and protection research (Draper et al., 2022; Scheidecker, 2024). The lack of representation from non-Western populations limits generizability and underscores the need for culturally inclusive research to better understand how parental ACEs and parenting stress manifest across different sociocultural contexts.
Additionally, none of the studies included in this review examined child outcomes directly. While intergenerational impacts of parental ACEs are an important area of research, our review focused specifically on parenting stress as the primary outcome. Future reviews could expand this scope to include child-level outcomes in order to capture a fuller picture of how parental adversity shapes family functioning.
Strengths and Limitations of the Present Review
This review also has some limitations that warrant consideration. First, although we used a rigorous and transparent methodology guided by the PRISMA framework, we limited our inclusion to quantitative studies published in English and only from select databases. As a result, nine full-text articles published in languages such as Chinese, Spanish, and German were excluded during the screening process. This introduces the possibility of language bias and limits the inclusion of culturally relevant data from non-English-speaking contexts. Additionally, although the review covered a wide timeframe and multiple databases, the final yield was only 11 eligible studies. One reason may be overlap in database coverage, as Web of Science was not included in the search. While this may have limited the number of studies identified, key psychology, and health databases were prioritized to ensure comprehensive coverage of the relevant literature. Finally, a meta-analysis was not conducted due to heterogeneity in study designs and outcome measures, particularly in how ACEs and parenting stress were conceptualized and assessed.
Despite these limitations, the review also presents notable strengths. To our knowledge, this is the first systematic review to focus specifically on the association between parental ACE exposure and parenting stress, focusing on mothers and fathers, and including both direct and indirect pathways. By synthesizing findings across diverse populations and parenting contexts, this review provides a consolidated overview of the empirical evidence and highlights critical gaps in the literature.
Future Directions and Implications
Future research must prioritize longitudinal and mixed-methods studies that can map how ACEs influence parenting stress over time and within specific contexts. There is a clear need to include more diverse and underrepresented populations, particularly fathers, and to examine contextual factors such as socioeconomic hardship, relationship violence, and community-level adversity. Integrating protective and resilience-promoting variables, such as social support and emotion regulation strategies, into these models will also be essential to move the field toward a strengths-based, intervention-focused direction. Future reviews may also benefit from multilingual screening or collaboration to capture a more globally representative evidence base.
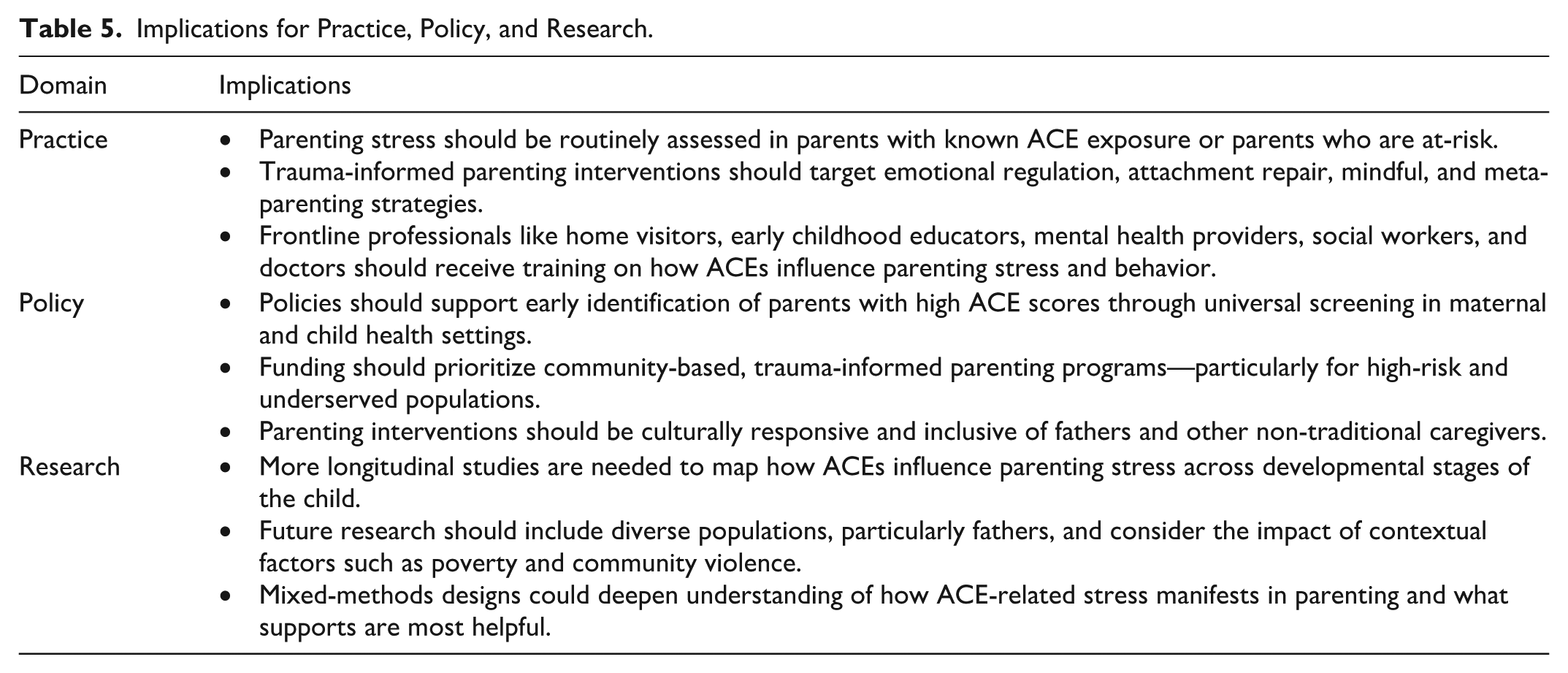
This review has several implications for practice, policy, and future research (Table 5). In clinical and community practice, parenting stress should be routinely assessed in parents with known ACE exposure or those considered at risk. Trauma-informed parenting interventions should focus on enhancing emotional regulation, repairing attachment-related disruptions, and promoting reflective functioning through strategies like meta-parenting. Furthermore, frontline professionals, including early childhood educators, health care workers, and mental health providers, should receive training on how ACEs shape parenting behavior and stress, to ensure timely identification and appropriate support. At the policy level, our findings underscore the need for early and universal screening of ACEs in maternal and child health settings. Policies should support the development of community-based, culturally responsive parenting programs, especially for underserved and high-risk groups. Importantly, interventions should be inclusive of fathers and non-traditional caregivers, who are often overlooked in parenting research and service design.
Implications for Practice, Policy, and Research.
Conclusion
Overall, the results of this review highlight a positive link between parental ACE exposure and parenting stress. Evidence for mediating or moderating variables in this link is inconsistent and scarce. However, the dual role of parenting stress as an outcome of ACEs and as a variable that mediates links between ACEs and other parental outcomes was clear. Several methodological limitations observed in the included studies were observed in this review. In particular, inconsistent measurement tools, reliance on self-reports and the predominance of cross-sectional designs limit the strength of these findings. In addition, fathers remain underrepresented in the literature, and the role of sociocultural factors remains underexplored. Understanding how ACEs influence parenting stress is essential not only for advancing theoretical models of intergenerational trauma but also for developing trauma-informed interventions. More research on diverse populations and protective factors, while considering the contextual realities of parents with histories of childhood adversity can help increase insights into the field.
Footnotes
Appendix A
Search Syntax.
| Database/ |
Syntax |
|---|---|
| ProQuest | TI ((“parents” OR “mother” OR “father” OR “parenting”) AND (“adverse childhood experiences” OR “ACE” OR “childhood adversity” OR “childhood trauma” OR “early life stress” OR “childhood maltreatment”) AND (“parenting stress” OR “parental stress” OR “stress in parenting”)) |
| MedLine (via PubMed) | (“parents” [Title] OR “parenting” [Title] OR parent* OR mother* OR father*) AND (“adverse childhood experiences” [Title] OR “childhood trauma” [Title] OR “child abuse” [Title] OR “early life stress” [Title] OR “childhood adversity” [Title] OR “childhood maltreatment” [Title] OR “ACE” [Title]) AND (“parenting stress” [Title] OR “parental stress” [Title] OR “stress in parenting” [Title]) |
| PsycINFO (via EBSCOhost) | TI ((“parents” OR “mother” OR “father” OR “parenting”) AND (“adverse childhood experiences” OR “ACE” OR “childhood adversity” OR “childhood trauma” OR “early life stress” OR “childhood maltreatment”) AND (“parenting stress” OR “parental stress” OR “stress in parenting”)) |
| Cochrane | TI ((“parents” OR “mother” OR “father” OR “parenting”) AND (“adverse childhood experiences” OR “ACE” OR “childhood adversity” OR “childhood trauma” OR “early life stress” OR “childhood maltreatment”) AND (“parenting stress” OR “parental stress” OR “stress in parenting”)) |
| Google Scholar | allintitle: (“parents” OR “mother” OR “father” OR “parenting”) AND (“adverse childhood experiences” OR “ACE” OR “childhood adversity” OR “childhood trauma” OR “early life stress” OR “childhood maltreatment”) AND (“parenting stress” OR “parental stress” OR “stress in parenting”) |
Appendix B
Critical Assessment of the Included Studies
Ethical Considerations
N/A
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
N/A